
Abstract
Childcare attendance is a recognized independent risk factor for pediatric infectious diseases due to the pathogen-sharing behaviors of young children and the crowded environments of childcare programs. The Michigan Child Care Related Infections Surveillance Program (MCRISP) is a novel online illness surveillance network used by community childcare centers to track disease incidence. It has been used to warn local public health departments about emerging outbreaks. The flow of data from MCRISP, however, remains largely unidirectional—from data reporter to public health researchers. With the intent to ultimately improve the system for users, we wanted to better understand how community illness data collected by MCRISP might best benefit childcare stakeholders themselves. Using a ground-up design approach, we conducted a series of focus groups among childcare directors participating in MCRISP. All primary data reporters from each of the 30 MCRISP-affiliated childcare centers were eligible to participate in the focus groups. A thematic assessment from the focus groups revealed that participants wanted surveillance system improvements that would (1) support subjective experiences with objective data, (2) assist with program decision making, (3) provide educational resources, and (4) prioritize the user's experience. Our findings support a framework by which community disease surveillance networks can move toward greater transparency and 2-way data flow. Ultimately, a more mutually beneficial surveillance system improves stakeholder engagement, provides opportunities for rapid mitigation strategies, and can help allocate timely resources in responding to emerging outbreaks and pandemics.
Introduction
Childcare attendance is an established independent risk factor for infectious diseases in childhood because of the pathogen-sharing behaviors of young children, naive immune systems, and crowded environments of childcare programs compared with individual households.1-4 As a result, illness surveillance has long been considered an essential component of early childcare practices—to protect both children and staff as well as limit disease transmission in the surrounding community.5,6 In the United States, childcare reporting remains largely paper based, which often results in data reporting delays and inefficiencies. Unlike the Netherlands and their comprehensive online reporting system, the United States has no online surveillance network that is dedicated to tracking and monitoring illness within childcare programs. 7 In southeast Michigan, we piloted and established the online Michigan Child Care Related Infections Surveillance Program (MCRISP) in 2013, the detailed methods of which are described elsewhere.8,9
The reporting framework of MCRISP was built following a traditional public health surveillance model. Childcare providers submit illness reports to local public health departments, which healthcare experts then use to evaluate disease incidence, transmission, and risk. However, aside from limited and often delayed public health announcements, local public health departments and medical centers rarely return timely data back to childcare stakeholders. In other words, the flow of information in MCRISP remains traditionally in one direction.
Childcare stakeholders are a unique community population that would substantially benefit from receiving disseminated illness data to improve the overall quality of childcare centers. 10 Indeed, new national consensus childcare recommendations in Caring for our Children 11 have stressed the importance of childcare providers using surveillance data to characterize daily illness patterns, identify outbreaks, and recognize effective interventions. Early studies demonstrated that MCRISP is both user-friendly and representative of real-time outbreaks. Building on these encouraging findings, our next goal was to shift the paradigm of the surveillance program toward a user-centered design that would better reflect the priorities and needs of childcare providers.8,9
To ensure that the input of childcare stakeholders was fundamentally incorporated in the redesign of MCRISP, we recruited a group of MCRISP data reporters to participate in a series of focus group discussions. Our overall aim was to answer the following question: how can a childcare illness surveillance network most optimally benefit its stakeholders? Using this ground-up design approach enabled childcare providers to shape the MCRISP redesign using their own priorities, rather than a priori assumptions from MCRISP administrators.
Methods
Participants
We recruited childcare directors from the 30 licensed childcare programs participating in MCRISP during the fall of 2019. MCRISP operates within a single southeast Michigan county and captures childcare-related illness reports from over 4,000 young children across a blend of private (70%), university-affiliated (20%), and federally supported programs such as Head Start (10%). 9 All MCRISP directors or primary data reporters from each program, were eligible to participate in the study; all were fluent in English. Our sampling goal was to recruit at least 16 directors to capture perspectives from the majority of MCRISP-affiliated centers. Participants were contacted via email during early August 2019 and given the option to attend 1 of 4 focus group dates, which were scheduled throughout August and September 2019.
Setting
We worked in close partnership with the Child Care Network (CCN), a nonprofit organization established in 1971 to improve the quality and access of childcare in southeast Michigan. 12 CCN also serves as the regional resource center for Great Start to Quality, 13 a program that assesses the quality of early childhood programs and providers in Michigan. In this role, CCN provides onsite consultants for quality improvement in local childcare programs. The CCN headquarters was familiar to MCRISP users and provided a conference room for each of our focus groups.
Data Collection
Conversations were semistructured; study moderators worked from an interview protocol but the group was free to bring up new topics and ask questions. Two members of the study team served as study moderators; the founder of MCRISP, and most familiar to the participants, was not present at any of the focus groups so as not to influence potential responses. The first 2 focus groups were attended by 2 comoderators, whereas only a single moderator attended the final 2 groups. Introductory icebreaker questions were used at the outset of each group, before transitioning to key study questions related to how an illness surveillance network best benefits childcare providers (Table 1). Because we believed that real-time, summarized MCRISP illness data would be valued by users, questions 7 and 8 requested feedback about the presentation of data that would be of best value to users. Summarized opinions of data visualization as well as the final, implemented visual manifestation on the MCRISP website are presented in Figure 1.
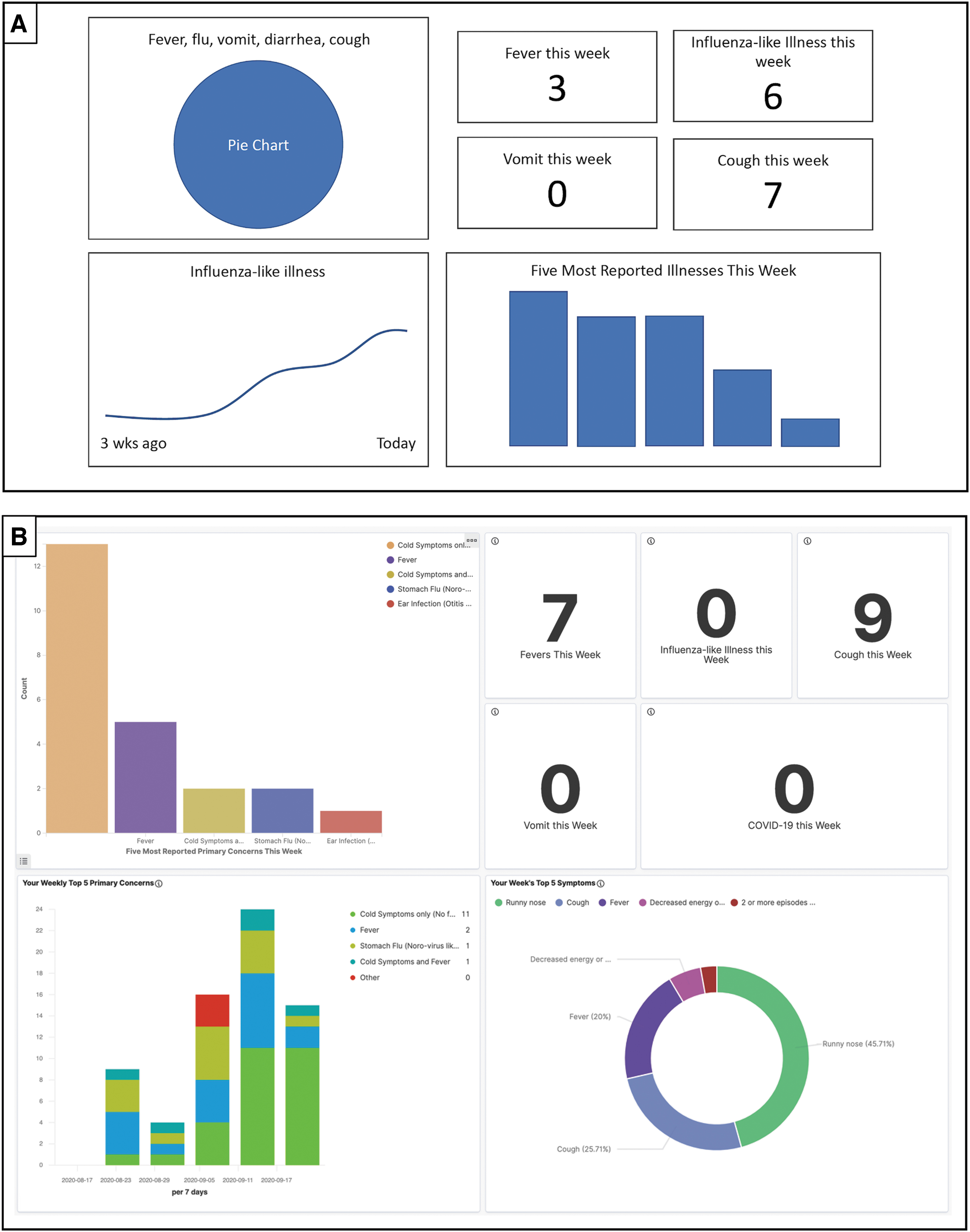
Data visualization dashboard images reflecting (A) the consolidated opinions of 12 childcare providers involved in the MCRISP focus groups and (B) the working product available to childcare providers after logging in to their respective program's home page on mcrisp.org.
Semistructured Question Guide for Focus Groups
Abbreviation: MCRISP, Michigan Child Care Related Infections Surveillance Program.
Group sessions ranged from 60 to 90 minutes in length and were audio recorded. At the end of each session, the moderator summarized the main takeaways and confirmed that participants agreed with the summary.
Ethical Approval
Although the University of Michigan Medical School Institutional Review Board deemed this study exempt from review, participants were asked to read and sign an informed consent noting the use of audio recording and that anonymous quotes may be published. Participants received food and a $50 gift card as a token of appreciation. Finally, all participants were asked to complete a short demographic questionnaire following the focus group discussion. All participants spoke English as their native language.
Data Analysis
All 4 focus group discussions were audio recorded, transcribed, and stored on a secure cloud-based server contracted with the authors' university. Participants were each assigned an alphanumeric identifier based on group number (eg, A2 corresponds to participant 2 in group A). Quotes are assigned to these identifiers throughout the transcripts. Each of the 4 transcripts was coded by one research team member. Codes were then organized into potential themes using code piles and structural maps. 14 These results were shared with 2 members of the research team and then themes were restructured based on collaboration with 3 of the other team members. Consensus themes and subthemes were defined, named, and shared with another team member who verified results of coding the manuscript after reading through all the focus group transcripts independently.
Results
A total of 12 MCRISP users participated in our focus groups, with 3 childcare data reporters per group (Table 2). Participants were all women, almost all of whom were directors of their respective programs (in cases where directors were unable to attend, the primary reporter was sent in their stead). Participants had an average of 24 years of experience working in childcare.
Characteristics of All Childcare Programs in Washtenaw County, Michigan, and Those Represented in the Study's 4 Focus Groups, Including Individual Participant Characteristics
Facility categories are approximate and not mutually exclusive as they are based on nonmandatory, self-assigned categories of licensed childcare programs in Washtenaw County, Michigan. Based on numbers from Michigan's Great Start to Quality childcare website. 13
Abbreviation: SD, standard deviation.
From the focus group audio recordings, we identified 4 major themes. Participants were looking for a surveillance system that would (1) support subjective experiences with objective data, (2) assist with program decision making, (3) provide educational resources, and (4) prioritize the user's experience. Themes and supporting quotes for each theme are detailed in the sections that follow.
Theme 1: Support Subjective Experiences with Objective Data
Knowledge of Community Illness Would Validate Experiences of the Childcare Community
All 4 focus groups supported the idea that knowledge of aggregate illness data collected by MCRISP would lead to better understanding of the current state of community childcare illnesses. In fact, childcare directors supported the idea because illness data would validate what they were experiencing and even provide a sense of solidarity among centers.
This is a community problem. Sometimes I feel like, “Oh gosh, we've caught everything.” I've washed and Cloroxed everything. Everyone's washing their hands—and obviously kids wash their hands very differently than I do—but it would be nice to know that this is not just something that's happening in our school, that we're doing enough. (D1)
Those [illnesses] are kind of just going around—just to get an idea that, like, we are not the only ones in the boat, you know? Sometimes it feels like that, for sure. (D2)
Notably, participants stated they had no issues with sharing illness information among all MCRISP centers as long as data were anonymized.
Knowledge of Community Illness Would Improve Relationships with Parents
Experience validation also seemed to be useful in conversations with parents. Participants shared a sentiment that childcare center practices or policies were often faulted for the illness of children.
I feel like we do kind of get blamed. Like, “Oh, my kid got [sick] from childcare.” (A3)
To ameliorate parental concerns, participants wanted to be able to share MCRISP illness data with parents. MCRISP data would not only corroborate the illness incidence experienced in a single center, but also assist parents in their own decision making—for instance, whether to keep a younger, immunocompromised child at home.
“It'd be nice if the system [said…,] “Hey, you know, this [illness] is running around in your area.” That would be very helpful for a lot of our families. (A1)
Theme 2: Assist with Decision Making
Decision Making for the Present
Participants noted that MCRISP could assist them during emergent community outbreaks. Not only would aggregate MCRISP illness reports bolster their understanding of the real-time community outbreak situation, but it could also provide time-sensitive, proactive advice regarding best-practice illness prevention efforts based on those outbreak data.
We […] send [outbreak information] to our custodial staff, so we can say, “Hey, we're getting notices that it's peak flu season. Can you do, what they call, a hospital clean?” So they do a deeper clean of the classrooms. (B1)
In cases of outbreaks, [we wonder] is there like a clear protocol or set of steps? “Okay, this is what you need to do.” Whatever it may be. (C1)
As an example of when enhanced MCRISP data would have been useful, participants often referred to the early fall of 2019, when southeast Michigan experienced a measles outbreak. 15 Although participants greatly appreciated the information they received from the health department, they still felt as though more educational materials specific to childcare would have helped both providers and parents.
People were talking about, “Well, anybody that enters an infant room will have to put on masks” but then, well, how effective is that? […] If there'd been a resource that you could've gone to and determine what's a reasonable step to take to not have an exposure, versus this won't make any difference at all […] that would've been something I used. (A2)
Decision Making for the Future
There was also some discussion of retrospectively using MCRISP data from their center to gauge the impact of their past interventions on historical incidence of disease.
Is there a seasonal pattern here […] and did these extra steps we decided to add for sanitation, did they make a difference? And if [they] didn't, then let's stop doing that. (A2)
Theme 3: Provide Educational Resources
Materials for Providers
Participants also hoped that a centralized surveillance site might serve as a repository for consolidated advisory materials from expert organizations, such as the American Academy of Pediatrics or the US Centers for Disease Control and Prevention.
We will invariably hear multiple things from different pediatricians coming through families […] this one will say, “Oh, it's conjunctivitis, [but] it's not contagious” but then the next doctor's like, “This is highly contagious.” […] I've been doing this for 20 some years and […] I mean none of [the opinions] ever aligned. (D1)
Not only is this information helpful to them as providers, but it also serves as a form of endorsement when speaking with parents.
[Parents] appreciate that our guidelines for exclusion are based on the American Academy of Pediatrics guidelines […] they like that it's [an] official health source […] it gives credibility then to our policies because they're based on theirs [official sources]. (A2)
We note here that childcare illnesses reported to MCRISP frequently originate from parents who let the childcare center staff know the child was sick at home, but parents do not always offer the level of illness detail requested by directors. Symptoms of home illnesses are important for childcare staff to know, however, and participants stated they could use more official MCRISP materials as a way to inquire further about the illness without being overly intrusive.
[Asking parents for illness information] feels like we're prying. We'll say “Oh, we just are part of a pilot project with this system and we just need to enter it in” […] it would be helpful to just have something to send out saying we're participating in this research. (B1)
Materials for Families
Participants also suggested the inclusion of MCRISP resources that could be used to better inform parents about common childhood illness. They noted that scientifically vetted materials should take many forms (eg, articles, videos, pamphlets) to best communicate with parents. Another participant stated that materials directed toward children were equally helpful in improving their center's health safety goals.
A curriculum about germs that's geared toward kids. We've had good success with [a specific lesson plan] and [teaching kids] how to wash their hands […] that's something I think would be helpful. (D2)
Theme 4: Prioritize the User's Experience
Operate as Simply as Possible
For MCRISP to be an effective tool, it needs to be seamlessly integrated into the daily operations of childcare centers. Participants repeatedly mentioned the frenetic nature of their jobs.
It's just an issue [in childcare] that directors are so busy and are handling so many different things in a day that finding time and ways for them to communicate […] is always a challenge. (B1)
I feel like if I don't try to report [illnesses] every day, […] it kind of falls off my radar. (A3)
Much like the desired simplicity of data visualization (Figure 1), establishing a straightforward yet comprehensive report form is crucial.
Provide Feedback to the User
Especially in light of their busy workdays, participants were frustrated that despite their reporting of illnesses on a daily basis, they received very little feedback from either MCRISP or local public health departments. Participants noted they would appreciate some form of indication that their reports were being seen and used.
If we're taking the time to enter [illness reports] in, we're getting something out of it too, you know? Like just getting updates or some kind of pop-up about an outbreak. (B1)
On the occasions they had received feedback from the health department, they perceived it to be very reassuring.
I mean, it was probably after using MCRISP for a while […] but I remember them reaching out and I was like, “Somebody's reading my stuff!” I just hit send and, yeah, I don't know if anybody's reading [the illness reports], so I found that very helpful. (B2)
Use Language and Themes Familiar to Childcare Providers
Focus groups also enabled participants to comment on strengths and challenges of the current MCRISP reporting structure. Overall, participants were generally satisfied with MCRISP's improvement over previous reporting methods.
One thing I've appreciated about this system is that it's an as-needed basis. I can go in every day. I can go in a couple of times today. If I go a whole week and nobody's sick, I don't have to do anything versus when we were recording to the health department before every Friday, I had to fill out a form and send it to them regardless of what was happening. (B2)
Still, the format of MCRISP reports fail to match a provider's experience on the ground.
I don't feel like there are enough [symptom] options for what I need. (A3)
It's not an exhaustive list [of symptoms], nor [does it have] the ability to add things that are more appropriate to what is going on. (C3)
Participants commented that reporting forms should mirror the language and experience of data reporters on the ground and reinforce the idea that user input is necessary at all points in creating a surveillance network.
Discussion
Online illness surveillance networks like MCRISP have the potential to significantly improve upon paper-based reporting methods by reducing the workload for community reporters and offering real-time information regarding local disease outbreaks. 16 The findings from our focus groups suggest that we can build upon successes of the initial MCRISP surveillance network by leveraging its efficiency and reliability to create a more mutually beneficial and user-centered reporting system. Most encouragingly, childcare providers appear eager to optimize illness surveillance data for their own uses.
We identified 4 themes resulting from the focus groups that should be used to guide improvements to illness surveillance networks like MCRISP. A beneficial system for childcare directors must (1) support subjective experiences with objective data, (2) assist with decision making, (3) provide educational resources, and (4) prioritize the user's experience. The most exciting aspect of a revamped MCRISP system for directors appeared to be the availability of aggregate illness data. These data would provide users with a meaningful feedback mechanism by enabling them to directly observe that their reports were being collated, thereby justifying their time spent entering data. Our results also suggest that sharing community data would improve program decision making, validate the subjective experiences of providers, and provide a sense of solidarity between centers. Moreover, access to community illness data has the potential to improve relationships between directors and community parents. The directors' shared sentiment of being blamed for community illness was a notable finding; it was also discouraging considering each had an average of more than 20 years of experience in dealing with common childhood disease. Unfortunately, this sentiment was also noted previously in the childcare field by providers. 17 As a solution, the rapid sharing of aggregate illness surveillance data might serve as a strategic approach for the public health and medical communities to support childcare directors who use appropriate childcare exclusion guidelines (ie, sending an ill child home from childcare or advising a parent not to bring their child to childcare).
The idea of information sharing and support for childcare programs has become more pertinent during the ongoing COVID-19 pandemic, which has underscored the essential nature of such programs in a community. The childcare industry was already struggling with financial difficulties before the pandemic18,19; however, in the process of trying to reopen (or modify practices appropriately), programs are now experiencing transmission events in the absence of appropriate public health resources and guidelines.20,21 Providing childcare experts with objective data and educational resources in an efficient manner is indispensable to further protecting the health and safety of young children and families throughout the remainder of this pandemic.
Our findings also underscore the idea that as technology advances, community surveillance systems have an opportunity to deviate from the traditional paradigm of unidirectional information flow—data from public reporters to research experts. Instead, in addition to data analysis and validity, disease surveillance systems must also strive for transparency and rapid data summarization. This idea has been raised in medical genomics, where the importance of enhancing citizen participation in surveillance research is emphasized, specifically via meaningful access to data apps and visualizations. 22 Furthermore, we suggest that shifting this paradigm is mutually beneficial. Our focus group findings demonstrate that a 2-way flow of information in community illness surveillance can immediately benefit the user and could lead to improved user buy-in and, in turn, more reporters. As a result, public health departments would receive more data regarding real-time disease circulation in childcare, which would be significant considering that children are often the first demographic subset involved in community outbreaks of disease and can serve as major propagators of localized transmission.23–25 Improved surveillance data enable public health departments to respond faster to emerging outbreaks, including devising mitigation strategies, establishing triggered alerts, and allocating resources.
We also note that improved childcare quality resulting from more 2-way, transparent illness surveillance data directly affects the wellbeing of the most at-risk families in the United States. Nearly two-thirds of all US children attend some form of nonparental childcare at some point before the age of 5 years, and high-quality childcare can serve as a vital developmental intervention for children from vulnerable, low-income households.26,27 These populations reap the highest reward as childcare quality improves.
We do note 3 limitations of our study. The first is that we had fewer childcare providers participate than the goal recruitment number of 16. The busy back-to-school and return-to-care activities of late fall may have negatively affected participation rates. Fortunately, group moderators found that the childcare providers who did attend were highly engaged, which resulted in rich conversation for focus group analysis and notable theme saturation across the 4 groups. Second, the distribution of participants from private, university-affiliated, and government-affiliated programs (75%, 17%, and 8%, respectively) was skewed toward private centers. This was not unexpected though, given the distribution of Washtenaw County childcare programs at large (81%, 3%, and 17%, respectively). However, this distribution may not be representative of other counties in Michigan or the United States where government-funded programs are more common. 12 Additionally, because no homecare programs or programs that care for a smaller number of children in a residential setting currently participate in MCRISP, no study participants were from home-based childcare programs. Finally, a system like MCRISP that is based on reliable internet access may prove challenging to implement in a more rural community. Despite these limitations, however, we feel our findings are still largely generalizable across variability in program type, enrollment size, or even method of illness reporting. The 4 broad themes identified through our focus groups would resonate with all types and sizes of childcare programs and are not necessarily specific to an online paradigm.
Future Directions
In response to focus group findings, we are updating existing MCRISP infrastructure with 2 entirely new online components. Our first addition has been to provide users with a real-time data visualization dashboard composed of aggregate community illness data (Figure 1). Our second planned addition to MCRISP will be a repository of informational resources and best practice guidelines, in response to participants' desire for accessible educational materials. These materials can be tailored to a variety of audiences, will be regularly updated to reflect current knowledge, and can be created in response to localized outbreaks or epidemiologic trends. Certainly, the ongoing COVID-19 pandemic has provided a striking use-case scenario for these materials.
Both of these additions will be assessed in a subsequent round of focus groups with MCRISP users to be held in 2021 (by video, if necessary), following sufficient time after the initial website rollout. At that time, our goal is to ascertain whether the revised 2-way system assisted providers with illness reporting, addressed the 4 themes described earlier, and helped determine how childcare protocol or policies may have changed.