
Abstract
The novel coronavirus disease 2019 (COVID-19) pandemic has exposed critical failures in global public policy preparedness and response. Despite over a decade of exposure to other epidemics and pandemics, many, if not most, nation states have failed to integrate lessons learned into their pandemic preparedness and response plans. The United Kingdom's response to COVID-19 is an archetype of how the pandemic has overwhelmed traditional public health-led approaches. In this paper, we explore the UK experience and propose that pandemics constitute multivector threats meriting attention within a health intelligence framework. They employ the processes of information management used by the intelligence sector to illustrate a procedural matrix for guiding public policy during complex health security events.
Introduction
The 2020
A recurrent feature of some of the more effective national responses to COVID-19 has been the agility of interventions and a readiness to integrate tools beyond the traditional remit of public health, some of which include established practices from the security and intelligence sectors. 3 This is contrasted against the United Kingdom's overreliance on disease modeling and slow, ad hoc scientific publication cycles, which produced a sluggish outbreak response poorly aligned with rapid response needs. From the early stages of the pandemic, the UK prioritized modeling data over the oft-quoted cornerstones of testing, contact tracing, and social isolation. 4 Public communications from government on this matter have repeatedly cited “the science” as the driving factor behind policy, however such messages have elided the complex nature of decision making in times of national crisis, presenting an overly deterministic relationship between scientific knowledge and public policy. A broader view of domestic outbreak response is necessary in order to capitalize on the array of novel techniques and perspectives that have been brought to bear on fragmented parts of the COVID-19 pandemic. The potential for a “health intelligence” approach to revolutionize the manner in which governments approach and respond to such threats is a productive focus of enquiry as COVID-19 continues to spread through global populations.
A number of issues have arisen as a result of COVID-19 that have demonstrated the impact of the disease outbreak beyond straightforward epidemiological metrics; the challenges of interstate hostilities, emergency national legislation, major economic bailouts, and social media disinformation and misinformation networks exemplify the extent to which this disease has undermined the fabric of national, regional, and global governance. These issues have repeatedly been raised within the Global Health Security Agenda (GHSA) as important factors that contribute to and exacerbate the exceptional threat posed by diseases of pandemic potential. As such the information gathering, data analysis, and data processing tools available to national governments, which are often used in other complex issues of national security, are overdue in being systematically deployed alongside regular public health practices to meet the challenge of infectious disease response. This paper argues that the consequences of threats such as COVID-19 have overwhelmed nation states' existing pandemic response capacities; in the UK, this is particularly due to the use of narrow technical framings that have relied primarily upon epidemiological modeling and the slow implementation of public health interventions. In the absence of an effective testing and sampling strategy, central methodological pillars of disease control practice, this reliance on modeling has been further called into question at national and international levels. 5
The current UK response has been fragmented and incoherent; the necessity to produce nuanced results at pace requires that innovative tools and techniques be deployed by multidisciplinary actors in a coordinated manner. We suggest that this could be achieved through the adoption of a process-driven health intelligence framework. To be effective, this framework will require the nimble integration of medical, political, economic, and social concerns into an effective structure to meet evolving nation state requirements for public policy development. Such processes are key to enabling robust connections between the scientific domain and the practical measures employed in disease response by generating a clearer locus of expertise within domestic governance structures. Consensus between domestic health and security sectors will become critical to the ongoing management of COVID-19 and future disease outbreaks.
Public Health and Intelligence: An Overview
Historically, the domains of public health and biosecurity have tended to remain technically distinct, with public health handling disease outbreaks and the day-to-day natural undulations of pathogenic reservoirs, while biosecurity has focused on biothreats, both engineered and otherwise, with an increasing attention to synthetic biology and dual-use concerns. 6 This siloing of expertise has led to critical divisions in institutional attention since at least as early as 2001, when the intentional use of anthrax as a bioweapon led to the identification of engineered biothreats as an intelligence priority by the security community.7,8 However, the GHSA has led calls for enhanced coordination between interested actors in the health and security domain, recognizing that the broader concern of “health threats” encompasses techniques and practices that can be harnessed across domains and tackled with a “health-in-all” approach.9,10 This has become clearer in recent years, where health events such as the Ebola outbreaks in West Africa and Democratic Republic of the Congo and the COVID-19 pandemic have exposed the artificial distinction between public health and biosecurity as it pertains to notions of risk and, crucially, in the deployment of mitigation and containment processes. 11 While techniques in global health have much expanded in the past decade, the cornerstone of practice remains disease surveillance. Under the International Health Regulations (2005), 12 nation states have a duty to collect relevant disease surveillance information and to deliver it to the World Health Organization (WHO). The capacity of states to generate and deliver this information has previously been noted as an important feature of good domestic health security (see the Global Health Security Index, https://www.ghsindex.org/). However, the COVID-19 pandemic raises concerns that technical capacity in health security domains, such as participation in global surveillance systems that identify spreading disease, is not in itself sufficient to protect against health threats at the domestic scale. Nor does this go far enough. Preparedness and response are as much about healthcare systems capacity, capability, and resilience, as they are about disease identification and monitoring.
Walsh 7 recently argued that “initiatives such as the [GHSA] established by the Obama Administration could provide opportunities for ‘Five Eyes’ [intelligence communities—United Kingdom, United States, Canada, New Zealand, and Australia] to increase awareness of potential biothreats and risks in addition of course to their public health capacity-building effects.” Arguably, this view is not limited to the Five Eyes community, but is part of a wider movement encompassing North Atlantic Treaty Organization countries, developing the perspective that the closer alignment of public health doctrine with some of the practices, processes, and priorities of the intelligence community is a necessary step to address the complex and political nature of contemporary health threats. Indeed, the UK's 2018 Biological Security Strategy 13 explicitly suggested a closer cross-government alignment of the intelligence and public health sectors in their “all-hazards approach” to natural, accidental, and deliberate risks. This view is likely to become more fertile now that governments are experiencing the disastrous consequences of the low priority that health threats have been afforded within security and governance matrices. This low priority is well demonstrated in the United Kingdom; a planned parliamentary inquiry into biological security was cancelled in 2019 due to government focus on Brexit and a general election, resulting in a total arrest of central planning to build on the recommendations of the Biological Security Strategy. 14
In practice, the division between the public health community and the intelligence sector has never been clearly codified. Indeed, it has been well documented that some overlap between sectors has existed across a range of portfolios.15,16 The role of medical intelligence, as it has been traditionally conceived, is defined by the US military glossary as
That category of intelligence resulting from the collection, evaluation, analysis, and interpretation of foreign medical, bio-scientific, and environmental information which is of interest to strategic planning and to military medical planning and operations for the conservation of the fighting force and formation of assessments of foreign medical capabilities in both military and civilian sectors. 17
This approach, which is pervasive across Five Eyes nations, highlights the utilization of intelligence parameters for addressing concerns as they pertain to military organizations and state capabilities. The narrowness of these concerns marks the need for a concerted shift from “medical intelligence” to a much broader concept of “health intelligence,” which accommodates the array of health risks described by the GHSA but falls well outside traditional public health/epidemiology-managed epidemics.
The further incorporation and assimilation of data from a wide variety of sources and the use of the terminology of intelligence signals a critical step in reconceptualizing the manner in which information is considered in this domain. Ostergard 11 recently provided a summary of health intelligence concepts that emphasizes the essential role of actionable information and preemptive practice regarding events of wide public health significance. Weighing and managing risk emerges as central, bringing a core focus of the intelligence method into the frame of reference. Ignoring the concept of risk, which allies “the perceived importance (saliency) associated with the risk and the likelihood of the state incurring significant losses,” 11 has been identified as a failure of the public health response to the West African Ebola outbreak (2014-2016), and can be seen lacking in many government responses to COVID-19 (eg, United States, United Kingdom). Public health organizations have previously been resistant to formally incorporating intelligence terminology; there is a persistent conceptual association between intelligence terminology and the specific intelligence techniques such as signals intelligence (SIGINT) and human intelligence (HUMINT) used by intelligence agencies. While the use of these practices in public health remains controversial from legal and ethical perspectives, it is clear from previous public health failures that the intelligence framework is at the very least applicable in these environments. It is also apparent that the possession of highly capable intelligence services does not currently translate into highly effective health intelligence practice and that this domain requires specific multidisciplinary consideration for further development as a state capability.
The UK Response to COVID-19
In the United Kingdom, the COVID-19 response has been led by the national government; the devolved administrations of Wales, Scotland, and Northern Ireland; the secretary of state for health; and the chief medical and scientific officers—with the National Health Service (NHS) acting as the primary healthcare provider. The United Kingdom's case is instructive in 2 manners. The first is the narrowness of the disciplines integrated into the government's scientific analysis, and the second is the opaque transition between scientific data and their conversion into practice.
The UK response to COVID-19 has mobilized what the government has consistently referred to as a “science-led approach.” In practice, this meant an early reliance on Professor Neil Ferguson's Imperial College London Infectious Disease Epidemiology Group to establish the underpinning assumptions guiding the national disease response. In tandem with the chief medical and scientific officers, and the government's Scientific Advisory Group for Emergencies (SAGE), the implementation of “science-led” policy has at times appeared opaque and impervious to the array of disciplinary methods available to deliver a more exacting context-led analysis of the outbreak with options derived from sources extending beyond epidemiological modeling. As preparations for the surge of infections were implemented in late March, a number of exceptional measures were undertaken within the health service: private hospitals were requisitioned, psychiatric hospitals were consolidated, hotels were converted to community hospitals, retired clinicians were recalled to the NHS, the NHS Nightingale Hospital London was constructed as a 4,000 bed intensive care unit in the ExCeL London convention center, and medical students were graduated early to supplement medical staffing.18,19 These measures were implemented parallel to the imposition of a nationwide lockdown on March 23, which required that nonessential workers stay home and for schools, universities, and 25% of businesses to shut down. 20 A persistent reluctance to reveal the underpinning assumptions of the modeling analysis behind both the government's initial approach of “herd immunity” and its subsequent reversal to the hard lockdown, 21 popularized across the rest of western Europe, has driven epidemiological methods to the forefront of public debate and generated important discussions about the appropriate matching of social measures to available information.
Much criticism has been leveled at the UK government's response, and the centrality of modeling is a focus of debate.22,23 Clare Wenham 22 recently argued in the Lancet for a greater understanding of the complexity of modeling as a pillar of public health practice, arguing that the ultimate public health shortcomings remain political in nature due to decisions taken by government. Clearly, the divergence of governments' approaches to COVID-19 reflect deeply political ruptures in regular and extraordinary governance processes. However, a recurrent issue has presented itself across affected nations, namely the translation of scientific information into effective public health practice. For governments with little experience managing domestic epidemic threats at this scale (the United Kingdom included), clear processes for the collection and management of information in this domain have been lacking. 24 This has also been evident in the siloing of what have been framed as discrete factors within this pandemic, such as the reliance on SAGE for scientific and clinical data, without elucidating the extent to which economic, logistical, social, and diplomatic factors impact the perceived risk and decision making. Concerns, too, around the transparency of decision making have rightly emerged as the membership of SAGE included controversial political advisors whose influence on public health policy remains unclear.
The territoriality of UK bureaucratic politics has been in evidence during the rollout of pandemic measures; the apparent absence of crucial specialist groups such as health security, health logistics, and emergency management professionals has been contrasted with the prominence of government-favored nonspecialist entities such as Deloitte and Serco. Obvious operational failures—such as the lack of personal protective equipment, a rapid at-source testing regime (in hospitals and care homes), and broader supply chain management problems—highlight the lack of general integration of key disciplines within a coordinated process for national outbreak management. Once leaked, SAGE membership highlighted these missing domains, which generated further questions about how scientific information is fed into the analysis and policy-making process. Political arguments over the inclusion of various individuals in SAGE and the continued lack of transparency around the newly formed Joint Biosecurity Centre and National Institute for Health Protection emphasize the continued opaque nature of information processing and delivery to relevant policy and decision makers. The Joint Biosecurity Centre is based on the Joint Terrorism Analysis Centre, supporting the government through its analytical and advisory functions and informing threat-level decision making. 25 The government's decision to replace Public Health England, an executive agency within the Department of Health, with another new entity, the National Institute for Health Protection, to which the Joint Biosecurity Centre now reports, has added further confusion to the operational and statutory mechanisms of information processing and technical management. 26 At present there remains no clear operational hub working on COVID-19 in the United Kingdom that fulfills the exacting standards of process or competency of an all sources pandemic intelligence cell. The current system fails to attend to health threats as a unique issue that is at once political and biological and also highly technical, requiring its own permanent cadre of systems, processes, and professionals at the national and regional levels.
The Merits of a Health Intelligence Framework
The COVID-19 pandemic has presented complex challenges beyond the purely biological and epidemiological. Expertise in translational practice at both ends of the knowledge–practice spectrum has been an obvious gap and reflects an underlying failure of states to recognize high-threat disease outbreaks as entities meriting significant domestic investment, in line with the provisions of the WHO International Health Regulations. 12 Distinguishing between the roles of information and intelligence is a necessary step in order to meet the challenge of transitional practice and overcome some of the data and capability gulfs in the current system.
The role of intelligence within a public health framework is contentious and reflects a number of important shifts in practice over recent years. One definition of intelligence is “the obtaining of information, [especially] of military or political value,” 27 and it is this association with military doctrine that has challenged the global public health and humanitarian communities. The well-documented issues raised by civilian and military interaction in health emergencies encourage caution when operating in settings with “blurred” boundaries. 17 Nevertheless, a much broader conception of intelligence as a practice of information processing, analysis, and dissemination can be understood as valuable in the highly complex scenarios of outbreak management and response. 18 Broadly, intelligence refers to specific information that has been collected in order to answer context-driven requirements and has been analyzed and assessed to answer these requirements. This practice is typically driven by the intelligence cycle, which describes an ongoing and circular sequence. The intelligence cycle encompasses a number of domains, starting with direction, in which the intelligence requirements or questions to be answered are enumerated and gaps in current collection are recognized; collection or the gathering of the necessary data; processing and analysis, wherein the information gathered is assessed and analyzed by specialists against the core questions in order to produce actionable answers; and dissemination, where the finalized intelligence product is provided to those who need it. 27 It is important to note that while the process is a cycle, the practice itself is sequential; to conduct each stage without first conducting the former would result in an intelligence failure.
It is this latter failure that has caused significant difficulties for the UK response. Figure 1 maps an intelligence model of the initial information management processes adopted by the UK government during the COVID-19 pandemic.

Initial UK process for information management during COVID-19. Abbreviations: CPNI, Centre for the Protection of National Infrastructure; NHS, National Health Service; SAGE, Scientific Advisory Group for Emergencies.
The United Kingdom's fractured response has been the result of its early and continued failures to utilize the intelligence cycle at 3 key points—direction, analysis, and dissemination—and its incomplete use of the collection and production phase. This, in itself, is largely the result of the initial narrow framing of the pandemic and failure to identify a series of directional requirements. Instead, the ad hoc and sometimes arbitrary assembling of separate research requirements has led to disparate data collection on the provision of health equipment, infrastructure, economic impact, and social impact. Crucially, the lack of initial intelligence requirements has led to the production of a series of separate reports and often contradictory responses from different government departments, demonstrating a fundamentally flawed conception of the cross-sectoral nature of public health and the necessities of pandemic response. Without full collection requirements, it is unlikely that the political decisions made to guide a pandemic response, which includes public health alongside economic and social measures, have been made in full understanding of the pandemic impact.
Also critical is the lack of an analysis phase. The repeated focus by the UK government on a “science-led response” fails to make clear any assessment of threat and risk, and, therefore, the generation of intelligence. While the bounded information products of SAGE, modeling, and clinical data outputs are crucial components of analysis, they have been presented to the public as a standalone justification for an array of policy decisions, some of which are highly controversial and restrictive of the public's civil liberties. These information outputs require analysis and interrogation within a multivector framework in order to produce a nuanced and weighted intelligence product for the development of public health policy that incorporates all key domains. The lack of directional requirements has led to the production of discrete reports, with no sense of the causal and consequential links between public health, economic, social, and governmental policy. As such, dissemination of these products has been impromptu and unclear.
Framework Proposal
The model of the intelligence cycle—direction, collection, processing and analysis, and dissemination—describes in clear terms a way in which information necessary to inform public practices during health crises could be managed in a highly targeted way to meet the rapidly evolving needs of stakeholders working across the health security sector before, during, and after significant outbreaks. 11 The fragmented, siloed, and opaque methods of the current information-driven response are not designed to meet the needs of complex, national security crises. A process-driven and intelligence-led framework is needed that can provide confidence to all stakeholders, including the general public. This framework is unlikely to rest with discrete bodies such as SAGE, but with the incorporation and integration of the group's contributions into a wider cross-governmental pandemic threat framework (Figure 2).
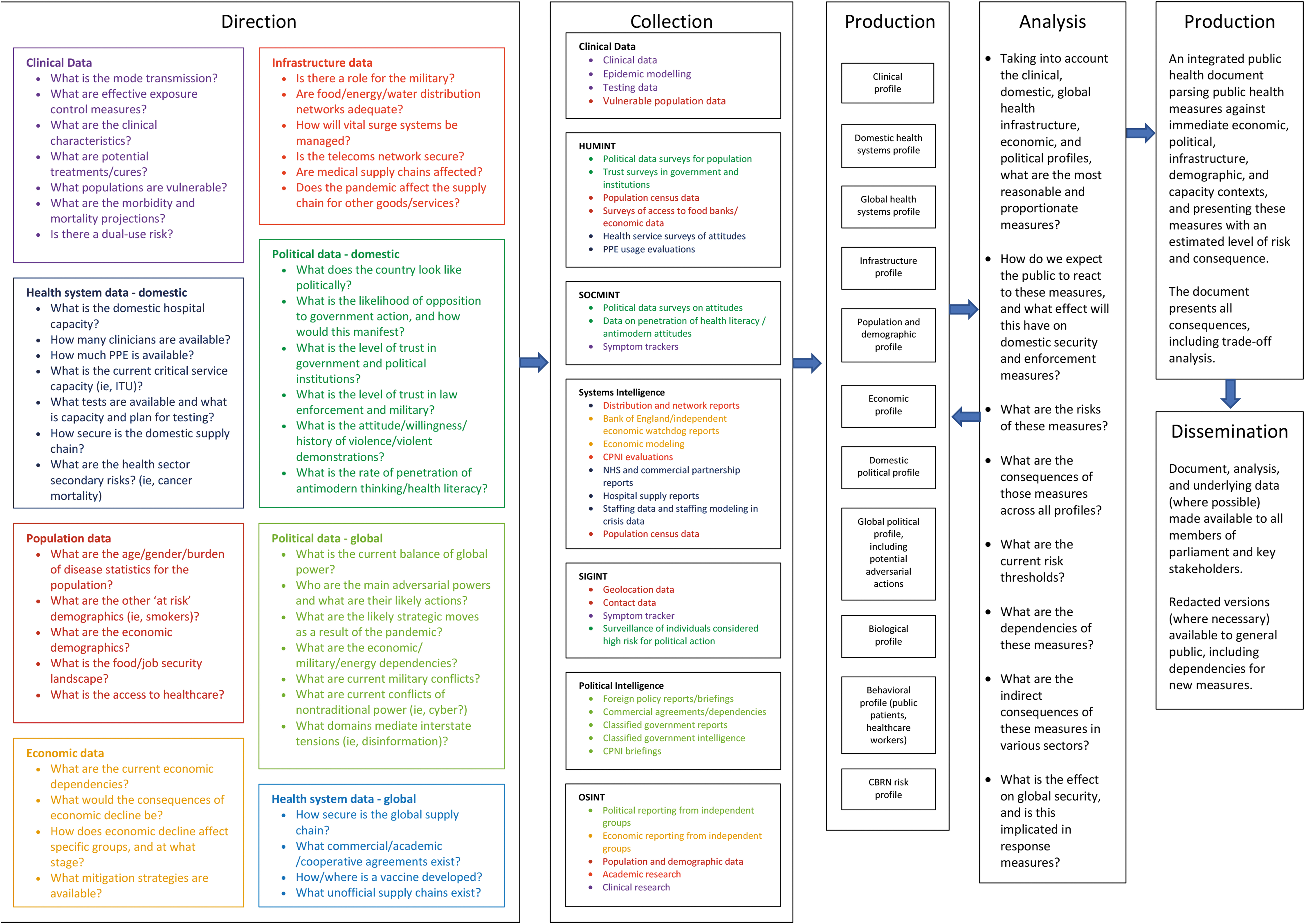
Health Intelligence Framework. Abbreviations: CBRN, chemical biological, radiological, and nuclear; CPNI, Centre for the Protection of National Infrastructure; ITU, intensive treatment unit; NHS, National Health Service; PPE, personal protective equipment; SAGE, Scientific Advisory Group for Emergencies.
Key to this framework is the sequential nature of the cycle, with clear direction that encompasses all dependencies and stakeholders within a public health crisis. This framing of intelligence requirements informs the collection, which produces a set of clear reports, allowing for targeted analysis. 28 The analysis phase demonstrates clear questions of threat and risk, with weighted judgements made across departments and sectors, rather than siloed within limited disciplinary boundaries. Finally, a single public health report is generated that can be disseminated to all key stakeholders and decision makers, allowing for a cross-government strategic, tactical, and operational response, with key decisions being taken by individuals in possession of an understanding of the wider pandemic impact. The proposed framework clarifies what a set of directional requirements might look like in the context of varied health threats and outlines the manner in which knowledge and expertise are connected with techniques and tools of intelligence to produce requirement-led, actionable intelligence products for use by governments. Such an approach connects “the science,” with crystallized processes and tools of information management, such that policy decisions can be made with the broad vision and clarity offered by this coordinated mechanism. This framework could be adapted across the broad range of health security threats, from exceptional global pandemics to localized outbreaks or engineered biothreats, bridging the gap in a regulated manner between public health practice and securitized responses.
There are several important considerations when deploying an intelligence framework; the first is the tasking and responsibility for such processes within government. Walsh 7 has advocated for a senior minister with either security or health expertise to be tasked with the health security intelligence portfolio. Such an approach has the benefit of recognizing the unique constitution of these concerns as a matter outside of the daily life of a health system, but equally unique within the security sector. In the UK context, this tasking method would ensure that this portfolio, and therefore the direction phase, is included in the business of Cabinet as a designated field of focus rather than a temporary emergency state. Placing individuals in leadership positions who possess expertise in the twin domains of public health and intelligence processes remains an area for development and capacity strengthening. What this notion opens up more broadly, however, is discussion over the manner in which governments more generally might produce institutional arrangements that attach an appropriate degree of high-level attention and procedural expertise, such that intelligence products are able to be delivered to the relevant tier of decision making in both emergency and ordinary times.
Oversight is an important dimension of intelligence, and the elevation of this specified form of health information to an intelligence product and part of due government process places it within an existing system of parliamentary oversight. Similarly, any collection techniques used in pursuit of the directional requirements would be governed by their corresponding legislation: in the United Kingdom, much sensitive collection is governed by the Regulation of Investigatory Powers Act. The trade-off between transparency and regulation in the intelligence sector has long been debated, however, the shift toward the proposed technocratic health intelligence process is likely to raise sensitive issues related to human rights and privacy due to the previously discussed association of the process of intelligence (ie, the intelligence cycle) with its techniques (eg, HUMINT, SIGINT). This framework contributes to such debates as a means of mapping potential processes of practice in order for governments to depart from the current disjointed methods of domestic health emergency management. Many of these ad hoc emergency regimes have led to the deprivation of civil liberties and enactment of exceptional states of governmental power in part due to the disarray in planning for and mitigation of the COVID-19 threat. 29 The elevation of this collection mechanism to a regulated and transparent government practice would allay some of those exceptional states of governmental power by placing it within the purview of formal parliamentary oversight. Additionally, issues around human rights and privacy could be assessed at the directional phase, in line with necessity and proportionality regulations, thus preserving due process of law in intelligence collection.
The connection between domestic and international processes for pandemic response necessitates information transfer between nation states and WHO under the requirements of the International Health Regulations (2005). The proposed health intelligence framework is designed to support state functions in compliance and, importantly, the optimization of state duties related to international law. Supporting the GHSA requires that intelligence products be shared effectively and with maximum possible levels of transparency with responsible bodies such as WHO and affected nation states. Earlier discussion on collaboration between the Five Eyes nations on health intelligence drives the need for further work on intelligence sharing and the legal, normative, and practical functions such processes entail.
Key Recommendations
A permanent cadre of health security experts be maintained by government for the prevention of, preparation for, and mitigation of health security risks. Such a cadre will consist of multidisciplinary professionals across the biomedical sciences, as well as the intelligence field.
Health intelligence exercises, including “gaming” involving policymakers, be conducted at regular intervals as part of preparedness and response.
During health security crises, the government commits to clear directional requirements and enables cross-sector collection plans.
Centralized public health crisis management should include subject matter experts able to speak to all the sectors identified in the directional requirements.
Cross-requirement analysis be conducted to produce a single public health response document/protocol, with any recommendations or findings clearly generated through a threat and risk framework.
Clear production and dissemination requirements are developed to ensure coherent cross-government practice.
A public communication in health emergencies framework to be developed and implemented.
Conclusion
The 2020 pandemic of COVID-19 has illustrated the grave risks of approaching health security crises without the policy architecture in place to support a timely and effective response. Coordination between disciplines has long been recognized as a critical dimension in outbreak response within global public health circles, 30 however, governments have tended to employ narrower policy framings of the disease threat, which has been reflected in settings such as the United Kingdom by an overreliance on particular forms of modeling rather than a preestablished coordinated response.
In the UK case, much criticism has been leveled at government for its repeated assertion that it is “following the science” with little elaboration on how scientific information is gathered, processed, and translated into policy. Groups such as SAGE are clearly pivotal hubs of expertise, however, the complexity of the COVID-19 outbreak has outpaced the current domestic mechanisms in place for managing such a comprehensive threat. The role of intelligence is to coordinate the targeted management of information in response to specified requirements. Insights from this field are fruitful for the future consideration for health risks and provide a framework for thinking and responding to the array of health security issues that challenge health systems. The health intelligence framework proposed in this paper offers a process by which to structure domestic disease response for localized outbreaks, globalized pandemics, or engineered biothreats. Greater alignment between the health security and biothreat domains highlights the common risks and shared expertise between fields. Focusing on the processes that could facilitate improved practice during health crises remains a pressing imperative for health and governance actors worldwide.
Footnotes
Acknowledgments
This work was supported by the UK Research and Innovation Global Challenges Research Fund research for health in conflict in the Middle East and North Africa (R4HC-MENA) Project; developing capability, partnerships, and research in the Middle East and North Africa ES/P010962/1.