
Abstract

New york city health + hospitals (nyc h+h), the largest public health system in the United States, delivered critical healthcare and support services to communities across New York City, the country's epicenter of the novel coronavirus 2019 (COVID-19) pandemic. The NYC H + H Community Care division was tasked with setting up isolation hotels as alternate care sites, with the goal of reducing the load of inpatient units and emergency departments in the system's 11 hospitals. Thus, the division's isolation hotel program emerged as a community-based public health intervention to mitigate current and prevent future community spread of COVID-19 in New York City. The hotel program operates on the premise that all suspected or confirmed COVID-19-positive individuals, individuals experiencing symptoms of COVID-19-like illness, or individuals vulnerable to COVID-19 require physical, emotional, social, and family support to aid their recovery. The aim of the isolation hotel program was to provide a safe and supportive environment for individuals who are homeless, living in crowded or congregate housing, or whose family and/or landlords did not want them to return home out of fear of potential exposure to COVID-19. As part of the health system's preparedness and response infrastructure, the Community Care division established the Incident Command Center, which served as a structure for making decisions and coordinating and mobilizing resources to transform more than 700 hotel rooms across 3 hotels to meet the unprecedented isolation needs of New York City residents and visitors. The isolation hotels provided 24 hours a day/7 days a week clinical monitoring and support, case management, care coordination, wrap around, and home care services. To date, the isolation hotel program has served 926 guests, 529 of whom have fully completed their isolation stays. The hotel program has since become the New York City Test & Trace Corps flagship Take Care Hotel Program.
Scouting and Selection of Hotels
Identifying and selecting hotels that would provide safe and aesthetically pleasing environments for clinical monitoring and support was paramount. We partnered with a hospitality brokerage firm and the Hotel Association of New York City to identify potential hotel sites and embarked on site visits to assess their appropriateness for the hotel program needs. We developed an environmental health and safety checklist to guide our site visits, during which we assessed floor plan, room sizes, bed capacity, and Americans with Disabilities Act compliant room capacity. 1 The ideal hotel floor plan was a straight corridor without any nooks or curves so that staff would have line of sight of all room doors at a glance. Although fire safety records were maintained by hotel management, comprehensive reviews of such records were undertaken to ensure fire and life safety systems and equipment were in place and current with inspections. If the hotels had utilities such as cooling towers and generators, preventative maintenance records were also reviewed to ensure full compliance with related regulations. Availability of cameras for all common areas and each floor was also a required security measure. The hotels were requested to address any identified environmental health and safety concerns prior to our assumption of occupancy for program implementation.
Infection Prevention and Control
Hotels as alternate care sites for individuals with suspected or confirmed COVID-19 follow the same principles and tenets of infection prevention and control (IPC) practices as other healthcare facilities.2,3 In fact, because these settings are nontraditional environments, it has been critical to ensure the hotels can support and implement all aspects of IPC practices in all aspects: engineering controls (eg, separate rooms), administrative controls (eg, plans, processes), personal protective equipment (eg, for clinical staff, wellness coordinators), physical distancing strategies, physical infrastructure (eg, storage areas, designated clean and dirty utility spaces on each floor), services (eg, food, environmental services), and care activities (eg, diagnostic and health assessments). Regular environmental assessments are performed to ensure the hotel setting is maintaining a rigorous level of IPC practices similar to traditional, healthcare environments. Appropriate signage in common areas and on every floor has also been important to reinforcing IPC training and reminding staff and guests of appropriate IPC practices.
Setting Up Alternate Care Site Transfer System
As New York City navigated the first surge of COVID-19 cases and hospitalization, there was an imminent need for a centralized transfer system to aid the efforts to relieve pressure on our hospitals. Hence, our Central Processing Unit was established to manage and effect alternate care site transfers to several temporary emergency hospitals and nursing homes within our health system. The Central Processing Unit was expanded to also manage and effect hotel transfers for individuals in need of quarantine or isolation, who are departing inpatient and emergency settings across New York City health systems; individuals from New York City Department for Homeless Services shelters and isolation hotels and New York City Emergency Management isolation and healthcare worker quarantine hotels who require clinical monitoring and support; New York City COVID-19 Hotline 4 ; and COVID-19 testing sites. We collaborated with the NYC H + H transportation team to gain access to contracted transportation resources, including ambulances, ambulettes, and taxis, to make such hotel transfers.
We developed a robust Microsoft Access data capture and tracking system to record and track all transfer referrals/requests, including referral sources, transfer outcomes, COVID-19 status, mode of transportation, turnaround times, and other important data elements. Crucial for any emergency response management, comprehensive data capture, tracking, and analytics helped drive many operational decisions for the Central Processing Unit—including staffing, training, and workflows—and positioned us to be able to identify changes and patterns in real-time and to manage staff and transportation capacity accordingly. Figure 1 is a snapshot of the dashboard (discussed in more detail later) showing that, as of July 16, 2020 at 12:48 pm, the Central Processing Unit had completed 833 transfers to isolation hotels.
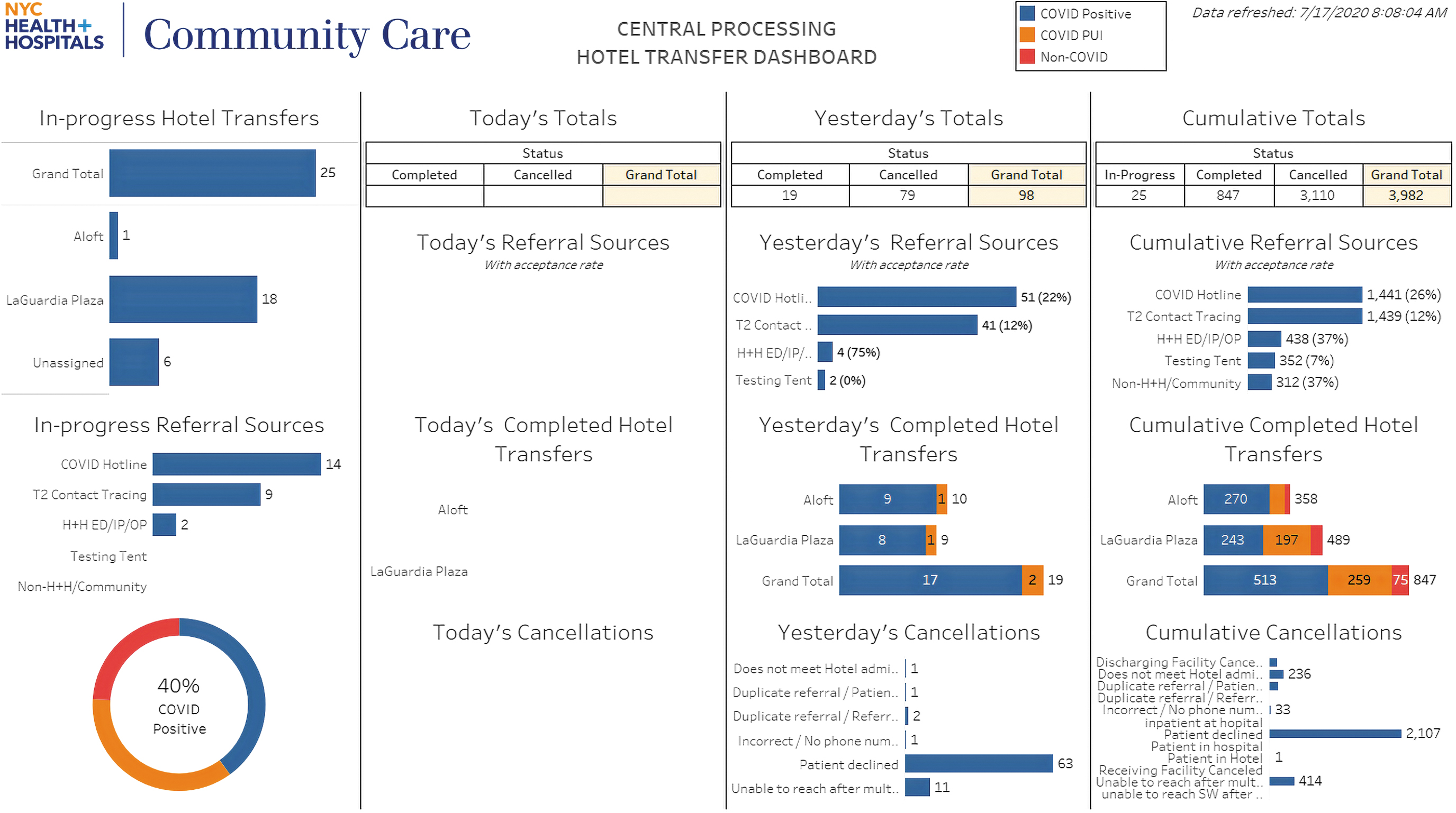
New York City Health + Hospitals Hotel Transfer Dashboard Snapshot from July 16, 2020 at 12:48 PM.
The Central Processing Unit and data management infrastructure position us to more efficiently respond to a potential second surge of COVID-19 hospitalizations. Based on lessons learned, we are seeking to implement more comprehensive and long-term transfer system solutions that will become standard tools and processes to mobilize in response to future emergencies.
Clinical screening is also integral to ensuring that the hotel setting is appropriate for a guest. The clinical screening team is comprised of registered nurses who screen potential guests for hotel placement and serve as primary liaisons to potential guests, referral sources, the logistics team attached to the Central Processing Unit, and our onsite hotel program teams. Clinical screening is conducted using a clinical review checklist developed by our nursing leadership with input from several physicians. The checklist addresses COVID-19 status, symptoms, underlying medical and behavioral health conditions, and social background. Upon completion of screening, potential guests are assigned to 1 of 3 tiers: Tier 1, requiring medical services; Tier 2, requiring behavioral health services; and Tier 3, requiring medical, behavioral health, and home care services. Upon arrival to a hotel, guests are assigned to specific floors in accordance with their designated tier and COVID-19 status.
Integration of Clinical Services
The hotel program provides low-level clinical monitoring and support of symptoms for guests who are COVID-19 positive, COVID-19 negative, have underlying chronic conditions and are vulnerable to contracting COVID-19, or are under investigation because they may be symptomatic or exposed to COVID-19 and need to isolate pending test results. We assembled a multidisciplinary team of clinicians and support staff to provide clinical monitoring and support services, which included wellness checks and onsite testing for COVID-19. This team is comprised of emergency medicine physicians, psychiatrist, social workers, registered nurses, licensed practical nurses, and care coordinators. Additionally, we partnered with community-based organizations to provide short-term case management focused on addressing priority social determinants of health—including food insecurity, housing insecurity or homelessness, cash benefits, and legal services—and integrated real-time enrollment in longitudinal Medicaid Health Home care coordination when appropriate. We developed evidenced-based, clinical escalation protocols to assist staff with identifying and escalating changes in a guest's clinical status. To ensure we are proactive in addressing guest safety issues, we developed/adopted and implemented protocols for the administration of naloxone (Narcan), 5 methadone delivery, 6 and performance of “Out-of-Hospital Cardiac Arrest: Hands only CPR.” 7 Staff were trained to apply these resources and tools using the Situation Background Assessment Recommendation 8 technique as the communication framework for the clinical team. We also implemented daily multidisciplinary team huddles and a clinical workgroup to assure a holistic approach to service delivery and to provide a forum for discussing and addressing challenges and opportunities to improve clinical monitoring and support services. This led to the implementation of the “Trauma Informed Care: Background and Resources for Hotel Staff” 9 training for the staff and telepsychiatry visits, which addressed a significant need for additional clinical support of our Tier 2 (behavioral health) guests.
Staffing and Operations
Implementing the isolation hotel program required balancing several considerations while adhering to the strictest IPC and safety standards possible in a novel environment. Access to and between hotel floors is restricted, and 1 elevator is designated for confirmed COVID-19 positive guests. Staffing is comprised of 24 hours a day/7 days a week of onsite site administrator, security, wellness coordination, nursing and nursing support, and social work coverage; 14 hours a day/7 days a week of onsite front desk coverage; 12 hours a day/7 days a week of onsite and remote provider coverage; and 8 hours a day/7 days a week of onsite care coordination and case management coverage. Guests are cohorted by floor based on COVID-19 status and underlying medical and behavioral conditions, indicative of the level of clinical monitoring and support required during their hotel stay. To the extent possible, hospital standards were emulated, including the storage and management of supplies and linen. Hotel rooms were converted to provide a clean area for donning and a soiled area for doffing personal protective equipment on each floor. Door locks were disabled to allow for quick room access, should it become necessary. To enhance security and responsiveness, wellness coordinators have been placed strategically on each floor to have complete line of sight down each hallway. Staffing ratios were established and adjusted based on volume of guests and parameters of the physical space.
Several elements were choreographed to minimize transmission, including transferring food from clean utility carts to designated stationary utility carts on each floor and door-level temperature checks using an infrared thermometer with guests required to wear masks. Food is boxed for delivery to guests who are asked to place their garbage into a plastic bag brought to their door by nursing staff. To encourage isolation, chaperoned smoking and fresh air breaks are offered. Monitoring adherence to service delivery standards and educating staff from multiple agencies who rotated thorough the program was challenging. Daily shift huddles provided opportunities to reinforce standards and to address operational concerns. An operational guide contains all of the hotel's standard work and checklists, as well as models for calculating staffing and supplies, which are crucial for estimating the needs for the ever-changing guest volume.
Financial Management
The financial management of COVID-19 isolation hotels is an ongoing coordinated effort across many departments and local government agencies. Our finance department developed models to track and calculate program expenses, leveraged NYC H + H catalogue of existing vendors, and worked to onboard new vendors to procure services needed to operationalize the hotel program, including environmental services, food, linen/laundry, supplies and equipment, personal protective equipment, and miscellaneous needs. An executive order from our health system's chief executive, Dr. Mitchell Katz, authorized expedited procurement and payment of these services, including our largest expenses: hotel rooms and agency staffing. In addition to finance operations, we worked with our central finance team to develop a budget projecting the cost of program operations and coordinated with local government agencies to track and report all expenses related to the hotel program for submission to the Federal Emergency Management Agency for reimbursement.
Data Management
The management of data—such as, room capacity, staffing needs, or incidental supplies for guests, including type and sizing of slippers and pajamas—is crucial for hotel program management. On the alternate care site transfer side, data capture, mining, and reporting is accomplished by using a Microsoft Access database and Structured Query Language (SQL). On the hotel census side, we worked with our central Epic electronic medical record team to leverage Epic bed planning and census tools to build the hotel rooms as beds in a “virtual inpatient unit.” This information was also loaded into SQL to develop a reporting suite for visualization in Tableau dashboards (Figure 2). Tableau allowed for subscriptions so that snapshots of and links to dashboards could be emailed on a schedule to various program leadership and key stakeholders. The data team also coordinated with various local government agencies including the NYC Department of Health and Mental Hygiene and the NYC Office of Emergency Management, to establish secure transfer of data to aid the automation of reporting and feeding of other dashboards and reports utilized by these agencies.

Cumulative COVID-19 Isolation Hotel Program Dashboard.
Information Technology Infrastructure
Community Care division's Information Technology (IT) department was charged with the rapid implementation of a secure and scalable IT infrastructure and a hardware plan, which were necessary for guest registration and documentation in the Epic electronic medical records. After conducting thorough assessments of all potential hotel sites, IT infrastructure plans—unique to the characteristics of each location—were devised and implemented. Hardware was procured and configured to be mobile and interchangeable. Equipment such as laptops, tablets, cell phones, printers, and fax machines were staged and set up centrally then deployed to each hotel. Equipment could be installed more densely in certain areas depending on clinical and operational needs. Account commissioning and decommissioning for over 300 staff was recorded and tracked using our system IT help desk software and managed via daily activity reports. Ensuring that all staff arrived with the appropriate types and levels of systems access needed to begin their training, as well as revocation of such assess upon termination of employment, was critical to efficient and documented delivery of services to hotel guests. In collaboration with multiple teams from our health system's central Enterprise Information Technology Services arm, we facilitated secure network communication by leveraging encrypted corporate Virtual Private Network, onsite Cisco Meraki equipment, and Remote Desktop software. This network communication approach enabled each hotel environment to quickly operationalize and modify its technological environment as needed.
Conclusion
The establishment of isolation hotels as alternate care sites and the ability to pivot quickly to address the needs of their guest populations have been essential to helping address the COVID-19 pandemic surge. Over time, the isolation hotel program evolved to serve pregnant women and infants and address guest barriers, such as need for childcare, home health aides and service animals. Evolving program operations have incorporated quality assurance and performance improvement measures, including seeking guest feedback on their hotel stay, and have improved guest experiences by including access to indoor and outdoor recreational spaces and activities; providing additional food options, including takeout; and offering additional in-room entertainment options, including premium cable TV channels. Additional clinical monitoring will include integration of pulse oximetry and harm reduction approaches to active substance and alcohol use to current protocols.