
Abstract
The COVID-19 pandemic has stretched limited public health resources beyond measures, particularly at the local level. What started as an interesting report of pneumonia of unknown etiology in late December 2019 in Wuhan, China, bloomed into an international crisis by mid-January 2020. However, it was not until late January, when the first case was reported in the United States, that a new reality took shape for US public health agencies. After all, severe acute respiratory syndrome never made it to this country, and the only 2 cases of Middle East respiratory syndrome here were imported and never spread. Local public health agencies are notoriously short-staffed and underfunded. Therefore, when a crisis looms, personnel from a multitude of areas within the agencies are called upon to help out. Under its innovative and forward-thinking leadership, the St. Louis County Department of Health internally implemented the Incident Command System, a component of the National Incident Management System. While reassignment of individuals to new responsibilities under a new and temporary reporting structure did not always go perfectly, Incident Command System kept its promise to be adaptable to a fast-evolving situation, to clearly outline needed areas of responsibility, and to provide scaffolding that kept the Department of Health functional in chaotic times. It was able to be implemented quickly within hours of the first confirmed COVID-19 case in St. Louis County and enhanced the quality and timeliness of the public health response. This experience is being shared to provide a model of how organizations with limited personnel can use the Incident Command System to reorganize and meet unexpected challenges with increased success.
Introduction
The us Department of Homeland Security first published the National Incident Management System (NIMS) in 2004, 1 as a result of Homeland Security Presidential Directive 5 following the events of 9/11. 2 NIMS is a set of best practices to enable responders from different jurisdictions, government agencies at all levels (ie, federal, state, tribal, local), the private sector, and nongovernmental organizations to work together through the 4 phases of emergency management: preparedness, mitigation, response, and recovery. 3 Federal funding for emergency management, especially preparedness, has been tied to compliance with the NIMS since 2006. Therefore, individuals playing a role in emergency management for private and public entities, including local public health agencies, participate widely in the training provided by the US Federal Agency for Emergency Management (FEMA). The Incident Command System (ICS) is one of these best practices advocated by the NIMS. ICS predates the NIMS by many years, having been adopted in the context of controlling wildfires since the 1970s. 1 It facilitates activities in 5 major areas: command, operations, logistics, planning, and finances/administration, and is both scalable and adaptable, depending on the type and complexity of an incident. 4 ICS provides clear chains of command, spans of control, and responsibilities for different functions. Despite these strengths, ICS is not an intuitive tool for individuals and entities that are not traditional emergency management agencies or personnel. There is a substantial learning curve for the vocabulary used to explain and practice the ICS. This vocabulary is quickly forgotten because it is not often practiced outside of training, since events requiring this significant shift in reporting structure and duties are fortunately rare. Most trainees are also unclear about when to apply ICS 5 and are uneasy applying it because it can be disruptive to an entity's routines and existing processes, creating new power differentials and increased workload.
Some emergencies result in activation of a local emergency operation center (EOC), 6 which then establishes its own ICS that local public health agencies will join as part of their emergency support functions. 7 However, prior to this happening and in other circumstances requiring an “all hands on deck” approach (ie, almost all divisions within a department being redirected toward a single effort), local public health agencies can use ICS internally to respond to widespread outbreaks, seasonal surges in vaccination needs, surges in opioid overdoses, and environmental events. These challenges may precede or altogether fall short of requiring EOC activation, but still overwhelm the capacity of the team within that local public health agency, which is primarily responsible for responding to these events.
With the advent of COVID-19, caused by SARS-CoV-2, the St. Louis County Department of Public Health (DPH), in Missouri, had to create its own ICS structure to provide a timely and effective response to the emerging crisis, made possible in part by the fact that our entire leadership receives advanced ICS training. As the crisis evolved, this structure morphed to be incorporated within the St. Louis County EOC ICS, but it retained a lot of its core components through the higher activation phases of the EOC. In this article, we strive to present an ICS structure for a public health department employing more than 500 people across 11 divisions, serving a population of approximately 1 million people, and with a $62 million budget for fiscal year 2020.
St. Louis Incident Command System Structure
Staff
The intent of an internal ICS is to be implemented within 72 hours of an event requiring “all hands on deck.” All positions within the ICS should have a succession plan (ie, more than 1 individual prepared to assume a set of responsibilities, either temporarily or permanently), often in the form of a supporting position. According to NIMS, the exact name for that position varies according to functions: deputy, assistant, or manager (Figure 1). In our case, the individual best suited to be the incident commander was 1 of 2 codirectors of the DPH because of her experience, qualifications, and working relationship with the government body to which the department belongs. The chief medical officer, the other codirector of the department, was ready to step into the incident commander role depending on the evolving complexity of the event and to provide additional infectious disease expertise at that level. The chief medical officer also oversaw regular DPH functions while her colleague was able to focus on ICS and the COVID response.
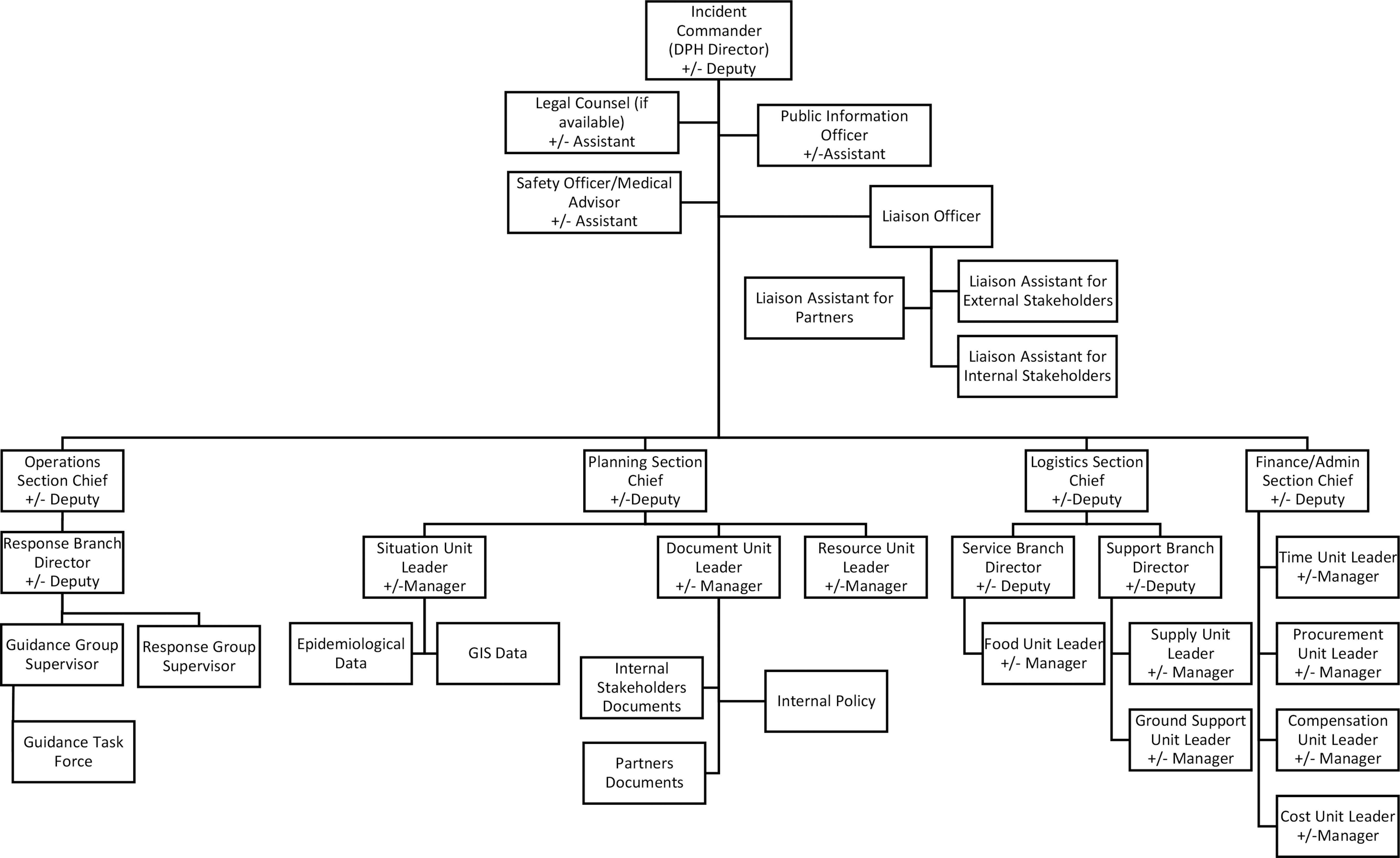
Incident Command Structure as implemented at the St. Louis County Department of Health during the COVID-19 crisis. Abbreviations: DPH, Department of Health; GIS, geographic information system.
Under the incident commander was the command staff. For our purpose, the command staff included a public information officer, a liaison officer, a dedicated legal counsel, and a safety officer/medical advisor. Content for public consumption was produced under the direction of our public health information officer, whereas content for internal and external stakeholders and partners was produced under the direction of a liaison officer, with the help of several assistants. The individual chosen for the public health information officer role had experience in several areas of the county government and could leverage existing relationships to accomplish goals. Legal counsel is not a traditional ICS position and we usually have access to the team in the county counselor's office, but having someone embedded within the DPH ensured a quick turnaround time to provide legal opinions on case investigations, contact tracing, quarantine, isolation, public health and executive orders, emergency ordinances, and to review all documents produced for various audiences as part of the COVID-19 response. If an attorney from the county's counselor's office had not been available, someone with a good understanding of DPH legal authority and processes to fulfill legislative needs could have taken on this role. A safety officer/medical advisor is typically part of ICS command staff to ensure overall incident safety. In our context, this role was taken on by our chief medical officer who was responsible for vetting medical content in all communications and published documents.
Sections
Under the incident commander and command staff were several sections to inform, enable, and carry out the work. Briefly, the Planning Section was responsible for overall situational awareness for command staff, other ICS sections, and internal and external stakeholders. The Operations Section was the implementation arm of the ICS. It provided response and guidance. The role of the Logistics Section's role was to make sure the Operations Section had what it needed to act, and the Financial and Administration Section ensured the effort was funded according to established rules.
Planning
The Planning Section should ideally be staffed with subject matter experts because it is the pivotal hub that collects and interprets facts and data to inform all decisions. The Situation Unit leader, under the Planning Section chief, was responsible for collecting this information from the liaison officer, public health information officer, and several specialty groups. The groups included an epidemiology team to gather and communicate data internally and also for public-facing dashboards. A geographic information systems (GIS) team was also there to leverage geographic and economic information important to interpret case data. GIS was used for public-facing dashboards as well. A Document Unit leader, also under the Planning Section chief, was responsible for prioritization, creation, and circulation of documents to inform decision makers, stakeholders, and partners. For example, the following internal policy documents informed and supported our workforce in these unusual circumstances: a succession plan, continuity of operations policy that addressed handling of patient health information from home or other remote locations, site-specific modified scope of services (either increased or decreased) including use of telehealth in clinical spaces and fieldwork, process for building lockdown, routing of increased phone traffic, leave and return-to-work policies for employees affected by the ongoing crisis, compensation issues for overtime and temporary assignments, and incident records. Other examples included documents to inform and coordinate efforts with other local public health agencies, nongovernmental organizations, and with other relevant branches of the county government. 8 The Document Unit also provided information about existing memorandums of understanding or contracts with call centers and providers of building security when work hours were extended. It produced daily, structured communication between itself and other sections, command staff, and major local government stakeholders, such as the Department of Corrections and the county executive's office. A final component of our Planning Section was the Resource Unit, which collected information on current human, equipment, and consumable resources.
Operations
The Operations Section implemented response activities. Under the Operations Section chief was a Response Branch director. Branches are traditionally composed of major geographical divisions and functional groups. Since DPH's purview is already a limited geographical area, DPH ICS was mostly concerned with functional groups, although it may be worthwhile to have individuals solely focused on supporting areas with particularly vulnerable populations, through engagement with community organizations and tailored messaging. We had a guidance group focused on influencing the actions of the public and external stakeholders, as requested by the public health information officer or the liaison officer, respectively. This writing was done with assistance from a guidance task force, a multidisciplinary team of subject matter and education and communication experts. We also had a response group oversee the work of technical teams on case investigations including contact tracing and monitoring, evaluations and choice of tests, personal protective equipment, training, choice of software to accomplish goals, data management, and dashboards.
Logistics
The Logistics Section coordinated supply and demand of human, equipment, facilities, and consumable resources and oversaw their sourcing, maintenance, and service needs. This section acted on information regarding existing supplies provided by the Resource Unit of the Planning Section. Within the Logistics Section, the Service Branch sourced services to support activities that were not business as usual or that constituted a surge in activities typically performed by DPH. This support helped DPH maintain its regular services, albeit in a reduced capacity, while responding to the crisis. Examples of such services may include temporary employees or volunteers (internal and external), specialty volunteers such as medical professionals who may administer medical tests or act as liaisons with school nurses or occupational health professionals of major health systems, and call centers. Part of the Service Branch would also be a Food Unit that procured food service for volunteers or employees working in alternate locations or working overtime. Alongside the Service Branch, the Support Branch sourced goods rather than services. Within the Support Branch, the Supply Unit focused on consumable supplies—such as personal protective equipment, thermometers, and test kits—to distribute within the community. Its responsibilities included testing or evaluating new sources of supplies, which could be new suppliers or donations and items coming from the Strategic National Stockpile. Finally, the Supply Unit was in charge of receiving and distributing these items. Also within the Support Branch, the Ground Support Unit sourced equipment needed to perform disaster-specific operations, such as air-conditioning or heating units for points of dispensing, laptop computers, and temporary phones for volunteers. Sourcing could take the form of donations, loans, or rentals and included considerations for maintenance or service. The Ground Support Unit received and distributed these items.
Financial and Administration
The last section was the Financial and Administration Section. Its role was to fund all the activities performed by other sections of the ICS structure. The challenge was that activities that were not business as usual or that represented surges in regular activities needed different funding strings from the baseline, either to keep track of additional expenses or to charge to a different source of funding, if one became available. Personnel time was recorded by the Time Unit leader, and cost data collected by the Cost Unit leader who also performed cost-effectiveness analyses, sought out cost estimates, and provided cost-saving recommendations. The Procurement Unit leader ensured that all sourcing was done according to DPH and county rules. Finally, the Compensation Unit leader processed claims from accidents or disease involving personnel and volunteers that were due to disaster-specific functions or presence onsite.
Challenges
Overall, our internal ICS structure has been a useful and successful tool in helping us navigate the COVID-19 crisis. We encountered several challenges, however, regarding the staffing of the ICS, communications, and public health functions other than those related to the pandemic. Additionally, some of the difficulties that we encountered highlighted needed improvement in our emergency preparedness program.
When it comes to staffing the ICS, we learned that getting the right people to the table should not be sacrificed in the name of expediency. It was tempting to prioritize subject matter expertise or individuals in the most current similar positions, but other considerations turned out to be important as well, such as personality and availability. First, each individual should have only one position within the ICS. As public health in general throughout the United States is underfunded, 8 it is not uncommon for employees to wear many hats. However, this multitasking goes against best practices for ICS, which suggests that the span of control should be 3 to 7 direct reports, with 5 being ideal. Some positions could be conflated vertically (ie, someone in a leadership position also performing a core function within the same area), but we avoided combining positions from different areas. Of note, the addition of a legal counsel in the command staff appears to increase the span of control for the incident commander to 8, but we felt that the legal counsel positions and the safety officer/medical advisor were more consultative positions in our context than positions under the incident commander. We found that the best fit for ICS positions, particularly in the lead, had the inner flexibility to assume completely different duties, deal with unstable and changing situations, rapidly expand incident response efficiency, and make decisions quickly with incomplete communications and information. Some, but not most, were already seasoned in crisis situations.
Another challenging area was communications. Fast-paced communications are built into the infrastructure and training for first responders, but this is not an area of strength for public health. One surprising aspect of the COVID-19 pandemic for DPH was the sheer number of documents that had to be generated in quick succession. The liaison officer and assistants were responsible for communications other than with the public directly. It quickly became evident that ongoing dialogue was needed with different groups to offer tailored messaging and align guidance and answers to questions. Examples of these entities included the regional healthcare coalition, residential facilities, clinical providers for medically vulnerable populations (dialysis centers), intermediate care facilities, urgent care providers, school districts, business associations, workplace occupational health departments, and faith-based organizations. Once the EOC was activated, communications with these external stakeholders were, in part, channeled through the EOC ICS, but there was a substantial period both before activation and after deactivation when these communications still needed to take place and many inquiries kept coming to DPH directly, even while the EOC was activated. This imperfect integration of DPH within EOC and coordination between them is beyond the scope of this article, but we believe it merits further study.
Just as critical was communication with internal stakeholders, including the Department of Corrections, with its vulnerable population, and with the county executive's office for frequent messaging to the St. Louis County Council. However, we found that our own DPH employees, even those who were part of the internal ICS, were sometimes left out of the loop as critical information made it to the news media before they were informed. A daily or operational period briefing works well within an EOC because people are essentially in the same room communicating with each other as needed the whole time. Within DPH and even within county government, when people had differing schedules and other ongoing commitments, we struggled to keep all but those in leadership positions informed in a timely manner. It may have been helpful to have the liaison assistant for internal stakeholders produce daily documents akin to incident status summaries and incident action plans 1 to distribute to the entire DPH.
Moving Forward
We will use this experience to improve some of activities performed by the emergency preparedness program at DPH. The Resource Unit within the Planning Section was responsible for maintaining awareness of what was on hand at all times, but we believe that more effort should be dedicated to maintaining real-time and accurate inventories on an ongoing basis, outside of crises and disasters. Examples of critical resources to track would be personal protective equipment stored at various locations including expiration dates, equipment and information technology such as laptop computers in working orders with up-to-date software, power banks, mobile WiFi, scanners and printers, fax machines, disposable phones, and clinical supplies for new onsite and field clinical work. Other items of importance to track are licenses for virtual private networks (VPN), software for contact tracing and remote patient monitoring, translation services, collaboration platforms, and conference call lines.
More time and effort should also be dedicated to practicing tabletop exercises about implementation of the ICS structure, particularly among leadership, and specifically in the context of a health department. The COVID-19 pandemic may have a lasting impact in this regard, but we need to stay comfortable interacting with one another and having effective meetings remotely, whether through WebEOC emergency management software (Juvare LLC, Atlanta, GA) or Zoom (Zoom Video Communications Inc, San Jose, CA). If we had taken meetings exclusively online almost immediately at the start of the pandemic, we would have been able to more consistently engage with subject matter experts who had to remain at home with their children due to closed schools. Business continuity absolutely requires regular practice or remote work from a variety of locations, and review and resolution of barriers to ensure that different groups can participate.
Conclusion
Although adapting the ICS structure to a new environment may seem difficult, especially in a time of crisis, the benefits are substantial in terms of providing a framework to assign new temporary responsibilities to individuals within an organization. The system minimizes gaps and duplication of efforts, which are common when staff are unsure how to help and unsure what others are working on. Most important, the ICS structure provides a model for communication flow, which is perhaps the most useful aspect in uncertain, fast-moving circumstances. However, ICS must be practiced on a regular basis to be implemented effectively when the need arises. While the FEMA trainings are necessary to introducing ICS concepts, they are not tailored to implementing ICS in environments other than first responder agencies and with individuals who still have significant other commitments, even as they participate in the response to an emergency or crisis.
Footnotes
Acknowledgments
We would like to acknowledge the hard work of all our colleagues at St. Louis County DPH, especially the public health nurses and epidemiologists.