
Abstract
The COVID-19 pandemic has generated fear, panic, distress, anxiety, and depression among many people in Bangladesh. In this cross-sectional study, we examined factors associated with different levels of psychological impact as a result of COVID-19 in Bangladesh. From April 1 to 30, 2020, we used a self-administered online questionnaire to collect data from 10,609 respondents. Using the Impact of Event Scale-Revised to assess the psychological impact of the COVID-19 pandemic on respondents, we categorized the levels of impact as normal, mild, moderate, or severe. Ordinal logistic regression was used to examine the associated factors. The prevalence of mild, moderate, and severe psychological impact was 10.2%, 4.8%, and 45.5%, respectively. Multivariate analysis revealed that the odds of reporting normal vs mild, moderate, or severe psychological impact were 5.9 times higher for people living in the Chittagong Division, 1.7 times higher for women with lower education levels, 3.0 times higher among those who were divorced or separated, 1.8 times higher for those working full time, and 2.4 times higher for those living in shared apartments. The odds of reporting a psychological impact were also higher among people who did not enforce protective measures inside the home, those in self-quarantine, those who did not wear face masks, and those who did not comply with World Health Organization precautionary measures. Increased psychological health risks due to COVID-19 were significantly higher among people who experienced chills, headache, cough, breathing difficulties, dizziness, and sore throat before data collection. Our results showed that 1 in 2 respondents experienced a significant psychological impact as a result of the COVID-19 pandemic. Public health researchers should consider these factors when targeting interventions that would have a protective effect on the individual's psychological health during a pandemic or future disease outbreak.
Introduction
SARS-COV-2,
During the lockdown period in Bangladesh, specific mitigation strategies may have had a psychosocial impact on some residents.3,10 Private and public hospitals suddenly stopped providing some services due to fears of spreading the virus,11,12 which in turn created tension among people who felt deprived of necessary treatment for conditions unrelated to COVID-19.11-13 Similarly, healthcare providers who became infected from treating COVID-19 patients were condemned and stigmatized.14-17 In addition, there were shortages of personal protective equipment for health workers and others who needed to work during the COVID-19 lockdown period. 15 For many people of different ages throughout the country, the pandemic caused fear, panic, distress, anxiety, and depression. 18 People were unable to see their loved ones or mourn the deaths of their loved ones with families and friends, and people with COVID-19 symptoms were often abandoned by their family members and some were denied burials in local graveyards; such experiences resulted in psychological trauma among family members.19-21
Daily wage earners and lower- to middle-income earners who lost their jobs or were unable to feed their families also experienced anxiety and stress, which in some cases led to suicide.22-24 Young adults reported psychosocial effects following school closures and the inability to see their classmates for a long time or be involved in physical or social activities.25-28 There were also reports of depression and anxiety among university students in Bangladesh, particularly medical students, due to educational, financial, and professional insecurity.29,30
In addition, social media speculations coupled with the spread of misinformation during the pandemic caused emotional stress in the population.19,31 There were accounts of dead bodies left unattended on the streets, and pedestrians avoiding them for fear of infection.32,33 Leading a monotonous lifestyle for an extended period also creates depression, impatience, and a level of psychological breakdown among some people.34,35 Researchers worldwide have emphasized the need to understand the psychological consequences of the pandemic, particularly in lower- and middle-income countries with limited resources,36-39 including Bangladesh.3,4,40 The effect of the COVID-19 pandemic on the mental health of people around the world, especially in higher-income countries, has been established in many studies. As a result of the inadequate healthcare infrastructure in many lower-income countries41-43 including Bangladesh,44,45 the impact of the COVID-19 pandemic may be severe, and the distress could increase with a new wave of infections.
Lower- and middle-income countries need an effective policy to minimize the psychological impact of the COVID-19 pandemic by offering appropriate services and recognizing the impact of such higher levels of stress, anxiety, and depression in the population. 46 As the people of Bangladesh become increasingly exposed to the virus, there is a need to identify who is at greater risk of COVID-19-related dysfunctional processes and maladaptive lifestyle changes, potentially leading to the onset of psychiatric conditions if left untreated.
Our study aimed to examine factors associated with the psychological impact of COVID-19 in Bangladesh. Several researchers have examined the psychological and mental health problems resulting from the COVID-19 pandemic, but no study has yet examined the severity of psychological health due to COVID-19 in Bangladesh and the factors driving these problems. In our study, we also assessed COVID-19-related stress along with other important aspects of life. Findings from this study will help identify who is at greater risk of experiencing a psychological impact from COVID-19, thereby contributing to a more sustainable health system in Bangladesh that can address the different levels of impact.
Methods
We conducted a cross-sectional self-administered survey from April 1 to 30, 2020, when mandatory lockdown was imposed in different parts of Bangladesh. A total of 10,609 respondents participated in the survey. The survey was distributed via social media platforms (eg, Facebook, Google Plus, LinkedIn, Twitter) because traditional face-to-face interviews were not possible due to the lockdown. We used a snowball sampling technique to collect information from participants who were also asked to share the Google Form link with their friends. Social media platforms enabled the target respondents living in different parts of Bangladesh to create and engage communities online.
Informed consent was obtained electronically from all participants through an online preamble that required a yes or no response to whether they voluntarily wished to take part in the study. Participants proceeded to complete the survey after providing consent. They were assured of the confidentiality of the information provided and their freedom of choice of participation. Eligibility criteria included being a resident of Bangladesh, aged 18 years or older, and able to provide consent online.
Questionnaire
To examine factors associated with the psychological impact of COVID-19, we used a 22-item questionnaire adapted from the Impact of Event Scale-Revised, 47 which has been used previously to assess the psychological impact of COVID-19. 48 The survey was administered in the English language and each question used a binary scale. A sample of the questionnaire is presented in Supplemental Table 1 (www.liebertpub.com/doi/suppl/10.1089/hs.2020.0205). The Cronbach alpha (α) coefficients measuring internal consistency among the survey item subscale score ranged from .69 to .93, indicating a satisfactory reliability level.
Univariate Analysis of Factors Associated with the Psychological Impact of COVID-19 Among Bangladesh Residents
Note: Level of statistical significance was set at P < .0001.
Abbreviations: CI, confidence intervals; HSC, Higher Secondary Certificate; SSC, Secondary School Certificate.
Dependent Variables
Responses to each item were rated from 0 for “Not at all” to 4 for “Extreme.” The total scores were grouped into 4 categories of psychological impact: normal (0 to 23), mild (24 to 32), moderate (33 to 36), and severe (above 37). For analysis purposes, normal was coded as 0, mild was coded as 1, moderate was coded as 2, and severe was coded as 3.
Independent Variables
The independent variables included demographic variables (region, age group, gender, educational status, marital status, employment status); household factors (living arrangement, number living together); COVID-19 factors (testing status for COVID-19); compliance with World Health Organization (WHO)-recommended precautionary measures (avoiding crowded gatherings, avoiding shaking hands, wearing a face mask when going out, avoiding use of public transport, advocating to others about the health risk of infection); and health symptoms (respondents were asked whether they experienced any of the following symptoms 2 weeks before data collection: fever, pain, headache, chills persistent, dizziness, breathing difficulties).
Statistical Analysis
Categorical variables are presented as frequencies and percentages. We assigned a sample weight of 1 to the variable and used survey tabulation to determine the prevalence and 95% confidence intervals (CI) for normal, mild, moderate, and severe psychological impact as a result of COVID-19. Dependent variables are classified according to their order of magnitude. Hence, univariate and multivariate ordinal logistic regression was used to determine factors associated with the psychological impact of COVID-19 in Bangladesh. Univariate ordinal logistic regression was used to assess the strength of associations of individual confounding variables. In the univariate ordinal logistic regression analysis, all confounding variables with P < .20 were retained and used to build an ordinal logistic regression model. A manual process of backward elimination was performed, and variables with P < .001 were retained in the final model due to large sample size and were considered as factors associated with the mild, moderate, and severe psychological impact of COVID-19. Data analysis was performed using Stata version 14.1 (StataCorp, College Station, TX).
To visualize the geographic distribution of the psychological impact of COVID-19 in Bangladesh, we produced a series of choropleth maps using ArcGIS version 10.6 (Esri, Redlands, CA). The map series shows 5 classes of adjusted odds ratio for mild, moderate, severe, and average levels of psychological distress across the first-level administrative unit (division) of Bangladesh. The average level of psychological distress was calculated from the means of the other 3 levels.
Results
Demographic Characteristics
Supplemental Table 2 (www.liebertpub.com/doi/suppl/10.1089/hs.2020.0205)shows the demographic characteristics of the respondents in this study (N = 10,609). The majority of respondents were women (50.4%), young adults aged 18 to 27 years (57.0%), educated with a university education or higher (58.8%), employed (56.3%), and lived in homes with their family members (80.4%). Many respondents lived in Dakar Division (49.5%), Khulna (16.8%), and Chittagong (11.3%), while very few lived in Sylhet (2.1%).
Multivariate Analysis of Factors Associated with the Psychological Impact of COVID-19 Among Bangladesh Residents
Note. The level of statistical significance was set at P < .0001. The analysis used a backward elimination model. The first model included all significant variables in the univariate analysis, whereas the final model shown in this table included only variables that were significant in the preceding model.
Definitions: intercept1 is the log of odds of normal vs. mild or moderate or severe; intercept2 is the log of odds of normal or mild vs. moderate or severe; and intercept3 is the log of odds of normal or mild or moderate vs. severe.
Abbreviations: CI, confidence interval.
COVID-19 Mitigation Measures and Symptoms
More than two-thirds (88.9%) of respondents had not been tested for COVID-19. Of those who had been tested (11%), 29.2% of which returned positive results. Although the majority of respondents (91.5%) reportedly enforced precautionary measures in their homes, many also reported not complying with the protective measures recommended by WHO and adapted by the government during the pandemic, such as avoiding large gatherings (Supplemental Table 2). About 20% of respondents reported some health symptoms in the 2 weeks before the study, including headache (26.0%) and cough or sore throat (22.4%).
Prevalence of Psychological Impact
The prevalence of normal, mild, moderate, and severe levels of psychological impact as a result of the COVID-19 pandemic are shown in Figure 1. The prevalence of severe psychological impact (45.53; 95% CI, 44.58 to 46.49) of COVID-19 was more than 4 times greater than mild psychological impact and about 10 times greater than moderate psychological impact in the study population.

Prevalence of the psychological impact of COVID-19 among Bangladesh respondents. Error bars indicate 95% confidence intervals.
Univariate Analysis of Psychological Impact
Table 1 presents the unadjusted odds ratios and the 95% CIs of factors associated with the psychological impact of COVID-19 among respondents in this study. The odds of reporting normal vs mild, moderate, and severe psychological impact was significantly associated with respondents' age. The odds were 4.28 times (95% CI, 3.88 to 4.71) and 3.38 times (95% CI, 2.66 to 4.30) greater for people aged 28 to 37 years and those aged 58 years and older, respectively, compared with younger people aged 18 to 27 years. With the exception of bachelor's degree holders, all other levels of education were significantly associated with normal vs mild, moderate, and severe psychological impact. Female respondents who were married and/or previously married (divorced, widowed), people who lived outside of Khulna Division (highest for Chittagong [OR 6.10; 95% CI, 5.23 to 7.12] and Rangpur Division [OR 5.40; 95% CI, 4.40 to 6.64]) had greater odds of normal vs mild, moderate, and severe psychological impact. Compared with respondents who lived with their family members during the pandemic, those who lived alone or in shared accommodations had 1.4 times greater odds of normal vs mild, moderate, and severe psychological impact. Noncompliance with precautionary measures and reporting of health symptoms were associated with greater odds for normal vs mild, moderate, and severe psychological impact. In addition, respondents who had undergone a COVID-19 test reported higher odds for normal vs mild, moderate, or severe psychological impact compared with those who had never been tested for COVID-19.
Factors Associated with Psychological Impact
Figure 2 shows the geographical distribution of the adjusted odds ratio by division and level of psychological impact due to COVID-19. Lighter colors represent lower impact and darker colors represent higher impact. Respondents who lived in the southern and southwestern divisions of Bangladesh had lower odds of psychological impact due to the pandemic, whereas those living in other divisions had higher odds.
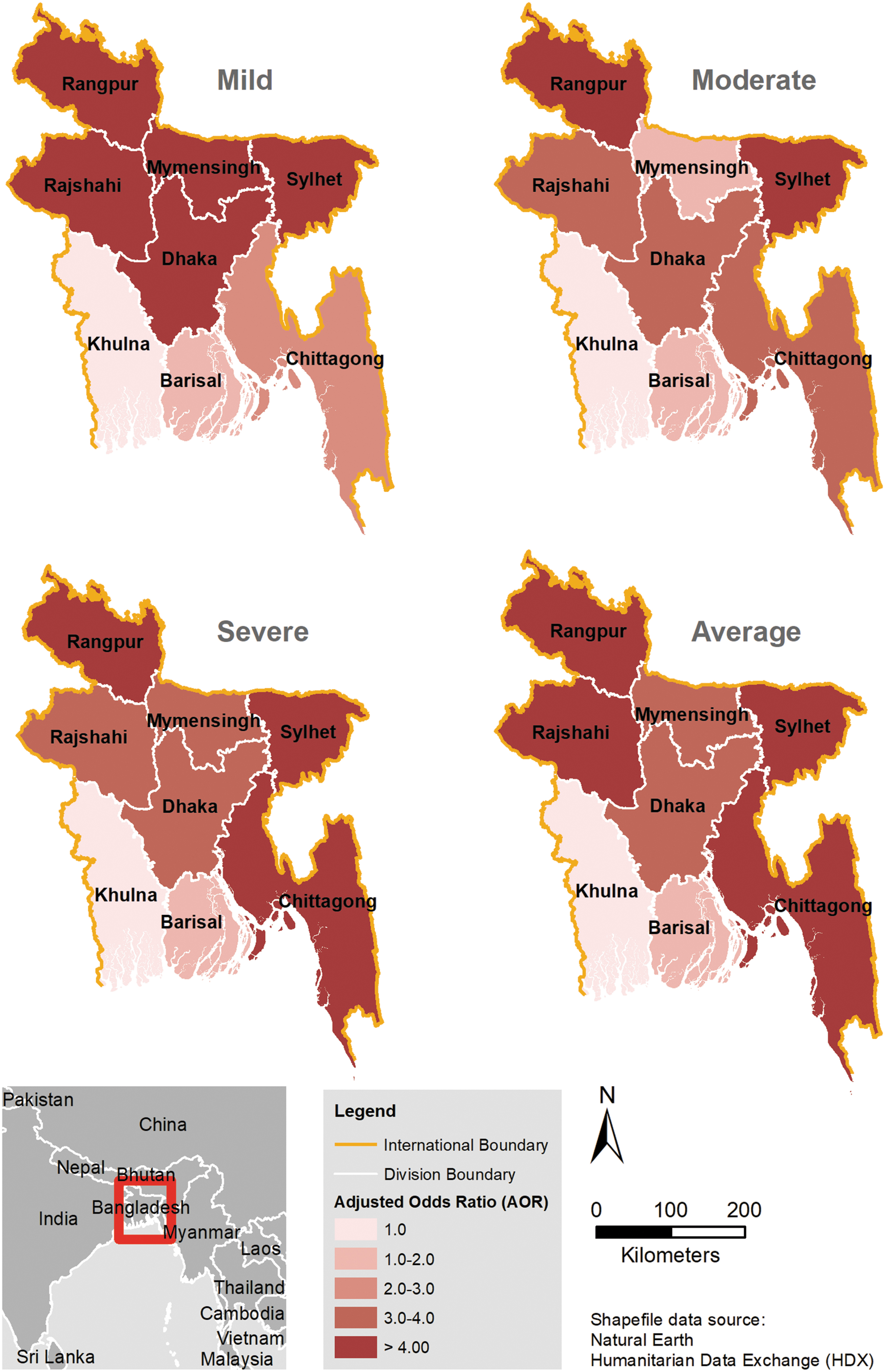
Geographical distribution of the psychological impact of COVID-19 in Bangladesh. The maps show 5 classes of adjusted odds ratio for mild, moderate, severe, and average levels of psychological distress across divisions (the first-level administrative unit) in Bangladesh. Lighter colors represent lower impact, and darker colors represent a higher impact.
Table 2 presents the results of the multivariable analysis after controlling for the variables that were significant in the first model. The table shows that the odds of reporting a psychological impact increased with lower educational status. Respondents who had completed a university education were 1.40 times (95% CI, 1.25 to 1.57) more likely to report a psychological impact due to COVID-19 compared with those who had completed a postgraduate education. Those with less than a secondary school certificate had 2.96 higher odds (95% CI, 2.35 to 3.72) of reporting a psychological impact. Female respondents who were married or previously married, adults who work, those who did not live with their families during the lockdown, and people who lived outside of Khulna Division had greater odds of reporting a normal vs mild, moderate, and severe psychological impact compared with other respondents.
Respondents who did not enforce protective measures at their homes and individuals who failed to comply with precautionary measures to mitigate the spread of infection during the pandemic were more likely to report a psychological impact as a result of the COVID-19 pandemic. Having experienced some health problems such as chills, cough, difficulty breathing, and sore throat in the week following data collection was associated with increased odds of psychological impact of COVID-19.
Discussion
This study examined the psychological impact of the COVID-19 pandemic among residents in Bangladesh in April 2020. The outcomes of psychological impact were modeled from questions designed to determine the level of depression, anxiety, perceived tension, wellbeing, and other psychological problems reported by individuals living in Bangladeshi cities during the lockdown period. 47 The study found that 1 in every 2 respondents living in cities reported a psychological impact as a result of the COVID-19 pandemic. Noncompliance with precautionary measures put in place to contain the spread of the infection and reporting of health symptoms were associated with greater odds of reporting a psychological impact. Respondents who lived in the Chittagong Division (southeastern part of Bangladesh) reported the highest psychological impact compared with those in other divisions. Female respondents who had lower levels of education, those who were either married or previously married, people who were employed at the time of this study, and those who lived alone or in shared accommodations had higher odds of reporting a psychological impact due the COVID-19 pandemic. Having been tested for COVID-19 only interacted with other variables to influence the respondents' psychological health symptoms.
The fact that Chittagong residents reported the highest odds of having a psychological impact due to the pandemic could be attributed to various factors. First, the division was home to the Rohingya refugees who lived in the camps of Cox's Bazar District, which is currently the world's biggest refugee camp.49,50 This may have increased the levels of psychological distress and anxiety among residents in this area. Second, the complex testing processes and the unwillingness of other medical centers to assign healthcare professionals to this region for fear of becoming infected may have heightened the stress experienced among people in this region, 3 which was confirmed in a WHO situation report published in August 2020. 51 The report reiterated that Chittagong Division (referred to as Chattogram in the report) was the largest single affected division in Bangladesh. Third, although the Dhaka Division had 29 ICU beds in 5 dedicated healthcare institutions for infected patients at the beginning of the outbreak, no institution outside of Dhaka had an ICU bed, 52 and those coming from the affected divisions were refused entry to Dhaka hospitals and endured neglect. These experiences may have increased their vulnerability to psychological distress.53-56
Previous studies have also found that the lockdown period was related to perceived stress and depression among people. 57 A study in China indicated that the strict lockdown measures had a severe negative psychological effect on people's psychological health during the COVID-19 outbreak. 58 In another study conducted in India, researchers found a positive effect of the lockdown on peoples' relationship with their parents, infants, partners, peers, and neighbors. This was attributed to more leisure time, reduced job burden, and the potential satisfaction from long-desired free time. 57 In the current study, people who practiced self-quarantine measures were less likely to report a psychological impact of the pandemic, which may be a causal finding. This finding is supported by another study conducted in China suggesting that the risk of mental health problems was significantly reduced among people who practiced self-quarantine measures. 59 However, it could be that compliance with the measures gave people a sense of security, or that people who were unable to follow the measures realized they were at higher risk and felt more distress because of that, or it is even possible that people who were in greater distress were less likely to follow self-quarantine measures.
We found that Bangladeshi women were more likely to report mild, moderate, and severe psychological impact than men. Although previous studies made similar suggestions, their results were inconclusive, indicating the need for further studies.60,61 The greater susceptibility of women to psychiatric conditions has been attributed to the fluctuations in their ovarian hormone levels, which were shown to be responsible for the altered exposure to emotional stimuli they experience. 62 Older people in this study experienced an elevated risk of psychological consequences due to the pandemic. Evidence on how age influences psychological problems is conflicting, but in one study, the authors found that young professionals and older adults had a higher risk of experiencing psychological distress. 63 A study conducted in China found low levels of psychological distress among young people and a comparatively low mortality rate across all ages, as well as limited susceptibility to psychological effects due to home lockdown. 64 A study in Australia found that young teenagers were more likely to experience psychological effects compared with older people during the first equine influenza pandemic in 2007. 65 This finding was attributed to a higher reliance on social media for knowledge among younger people, which may result in stress. 66
Our findings showed a higher prevalence of psychological risk due to COVID-19 among respondents with lower education, which is supported by previous findings that lower educational attainment was associated with higher psychological symptoms among residents in China, Italy, and the United States.63,67,68 Contrary to these findings, a study in China showed that people with higher education experienced more symptoms of depression than those with lower education. 69 The authors argued that the busy work life and frequent journeys made by highly educated people stopped during the pandemic, forcing them to stay home, which increased their engagement with their families. The lack of family safety, job status, and family income may have increased their worries.
Respondents in our study who were not living with their families reported higher odds of experiencing a psychological impact due to COVID-19. Previous research from China found that respondents who self-quarantined were more likely to display signs of depression and anxiety than those who did not self-quarantine. 70 Exhaustion, anxiety, irritability, insomnia, and indecisiveness were more likely to be observed among people in quarantine. 71 The largely homogeneous culture of Bangladeshis 72 means that people often travel to see their relatives and prefer to spend leisure time with friends and colleagues from outside their homes—a practice popularly known as “Bazar.” Abstaining from such activities can therefore affect people's psychology during the lockdown period. Another challenge has been the rapid spread of misleading information and misconceptions on social media.73,74 At the same time, debates on the status of the pandemic were easily accessible as they were continuously featured in electronic, print, and social media.
Those who had been tested for COVID-19 and respondents who showed signs of COVID-19 infection had higher odds of psychological distress in the unadjusted analysis. In previous studies, authors found that over 50% of patients infected by severe acute respiratory syndrome and Middle East respiratory syndrome experienced psychological distress,75, 76 suggesting that both confirmed and suspected cases of 2019-nCoV may be afraid of the effects of being infected with such a potentially lethal new virus and may feel boredom, isolated, and frustrated while in quarantine. Although the psychological impact of COVID-19 remains unclear, infected patients may experience anxiety, depression, guilt, stigma, and anger as suggested in a previous study. 77
This study had some limitations, including the use of nonprobability sampling, which is highly unrepresentative of the national population in Bangladeshi. The use of this sampling technique was unavoidable, however, due to practical considerations of the lockdown. In addition, attempts were made to increase the reach of the survey through social media channels popularly used in Bangladesh. The fact that the majority of participants in this study had at least a postgraduate education limits the generalizability of our findings, since the survey may not have captured the opinions of those with lower education levels. In addition, the predominance of a more highly educated population could be attributed to the fact that participants were likely to be those who had access to a smartphone. As noted in previous studies, younger people are more likely to use the internet and are more likely to engage in online polls as a result. 78 Earlier research, using a similar data collection approach from the same area of Bangladesh, 4 also had a disproportionate sample of more educated participants that does not represent the general Bangladeshi population. Because of the lockdown due to COVID-19 at the time of data collection, the online survey was the only viable option for obtaining opinions from a wide sample of the population. Paper-based polls would have been an alternative way to capture the opinion of those who may not have access to the internet, but this method was not feasible at the time. Further research using alternative data collection approaches such as polling services and telephone interviews are needed to further confirm the psychological impact of the pandemic in Bangladesh. Despite these limitations, these findings are necessary for the planning of effective intervention strategies in this region.
Conclusion
Our findings showed that approximately 1 in 2 respondents from Bangladesh experienced severe psychological distress as a result of the COVID-19 pandemic between April 1 and 30, 2020. Although the levels of psychological distress varied depending on geographic location, those at higher risk of experiencing psychological distress were living in the southeastern part of Bangladesh, women, older adults, and people who were less aware of the disease. Respondents who lived alone or with their families also experienced higher odds of experiencing a mild, moderate, or severe psychological impact. These findings can inform public health experts to identify target groups when designing strategies to mitigate psychological health effects from the COVID-19 pandemic and future outbreaks.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.