
Abstract
Population displacement has been embedded in Pakistan's history since its inception in 1947. The displacement of more than 3 million people from the tribal areas of the Khyber Pakhtunkhwa Province of Pakistan and their settlement in recipient areas have posed challenges to governance, service delivery, financial management, and integration of internally displaced persons (IDPs) into existing devolved district health systems. Evidence is lacking on the management of devolved health systems to respond to the public health needs of IDPs. The authors adapted qualitative methods to explore challenges faced by managers of health departments in Khyber Pakhtunkhwa Province in responding to the public health needs of IDPs and to explore policy recommendations for a devolved health system. Study findings revealed that the lack of a skilled workforce, lack of political will, financial limitations, and poor intersectoral collaboration had an impact on the humanitarian crisis response in the province. These findings suggest a dire need for overarching binding international laws and local national policies for complete protection of IDPs, particularly in regard to their health, shelter, and social security.
Introduction
Humanitarian crises due to conflicts and natural disasters have affected human existence and increased mortality and morbidity throughout history. 1 In the 50 years, disasters leading to humanitarian crisis have increased considerably all over the world. 2 In almost all complex humanitarian emergencies, forced displacement is a matter of concern—either across country borders (refugees) or within country borders (internally displaced persons, or IDPs). 3 Unlike refugees, IDPs are not entitled to special legal protection under international law; rather, IDPs remain under the jurisdiction of their own country. However, due to their status as a vulnerable group, international humanitarian agencies can provide support to IDPs on the basis of human rights and humanitarian law without replacing state authority. 4 Complex emergencies impede the functional viability of local public service systems, including healthcare services.5,6 Displaced populations, particularly in resource-limited, fragile states, place an additional strain on scarce resources. This leads to increased risk of further disasters and displacement, causing chronicity of these challenges. 7
Population displacement has been embedded in Pakistan's history since before its inception in 1947. 8 Pakistan is highly prone to both natural and manmade disasters, and the northern Khyber Pakhtunkhwa Province is the largest recipient of Afghan refugees and IDPs. 9 In the last decade or so, Pakistan has experienced large-scale involuntary displacement from all 7 agencies of the tribal areas and the Malakand Division of Khyber Pakhtunkhwa. The majority (90%) were accommodated within the host communities of adjacent areas, and the remaining (10%) were settled in camps. 10
From 2005 to 2014, armed conflicts and natural disasters led to large population displacements throughout Pakistan. The resulting IDP crisis has posed enormous challenges, causing serious disruption of society with grave economic, environmental, and health consequences. 11 Pakistan's underfunded health system, which was already functioning at suboptimal level, 12 was severely disrupted by armed conflicts. This posed serious threats to meeting IDPs' basic health needs. 11 Furthermore, the poor socioeconomic status, level of education, and living conditions of IDPs who lived in the Jalozai camp in Khyber Pakhtunkhwa Province, including women and children, put them at risk of poor health outcomes. 13 The large number of in- and off-camp displaced populations required immediate humanitarian assistance from actors with a shared operational strategy to respond to the IDPs' public health needs and to avert morbidities and mortalities. 5
According to the Internal Displacement Monitoring Centre's global risk assessment, Pakistan is among the 10 countries with the highest risk of disaster-induced displacement, with an estimated average of 240 per 100,000 people at risk to be displaced at any time, excluding preemptive evacuations. 14 Despite its prevalence, displacement within the Pakistani context is poorly understood, and no known policies are in place to address it. 15 The government of Pakistan has failed to effectively integrate crisis management into planning and policymaking so far. 9
Pakistan's health system evolved over time to comprise a mixture of public- and private-sector facilities 16 aiming to develop vigorous health programs to fulfill community health needs. However, Pakistan's health system is far from achieving this goal due to mixed health systems syndrome, 17 caused by lack of governance, poor public financing, and lack of private-sector regulation, which has led to equity, access, and quality issues.
The geostrategic position of Pakistan during the Cold War era and after September 11, 2001, affected its development, growth, and social structure. 17 In addition, Pakistan health's system was influenced by the 18th constitutional amendment, which devolved health sector authority from the federal to the provincial level.17-20 This devolution occurred on June 30, 2011 with the temporary abolishment of the Ministry of Health (which was reestablished in April 2012 as the Ministry of National Regulations and Services, and later renamed the Ministry of National Health Services Regulation and Coordination). 21 The aim of decentralization was to enhance monetary and organizational authority at provincial and district levels. However, decentralization has been a challenge since its implementation, mainly due to the lack of a national health policy and weak provincial health sector strategies. 22
The existing literature on IDPs in Pakistan focuses primarily on assessment of their public health needs, including the provision of food and shelter, as well as essential healthcare, 23 mental health, 24 mother and child health,25,26 and water and sanitation services. 27 Management of the increasing number of IDPs has remained a challenge, particularly for conflict-riddled countries, 28 including Pakistan. 9 However, there is a lack of local evidence about the management of the humanitarian crisis. The main objectives of this article are to: (1) explore the challenges that managers of provincial and district health departments faced in responding to the public health needs of IDPs living in Nowshera District of Khyber Pakhtunkhwa Province and (2) recommend policies in the context of a devolved health system.
Methods
The research presented in this article is part of a larger case study that explored and assessed the devolved local health system response to IDPs from the tribal regions of the Khyber Pakhtunkhwa Province of Pakistan. 29 We collected qualitative data from July to September 2018 through interviews with managers of public- and private-sector health departments involved in the IDP crisis.
Study Setting
We used nonprobability convenience sampling to select the study setting. Nowshera District was selected as a research case study based on the maximum number of IDPs living in the Jalozai IDP camp, as well as the favorable security situation in, and comparatively easy access to, that area. 30 The Jalozai IDP camp of Nowshera District is one of the oldest and biggest camps in Pakistan. It is situated 35 kilometers southeast of Peshawar, the provincial capital of Khyber Pakhtunkhwa Province.
Research Paradigm
Population displacement in the country and its impact on the local health system largely influenced the development of the study's conceptual framework, which is illustrated in Figure. Hence, the conceptual framework for this study not only portrays the knowledge, experiences, and opinions of public and private parties involved in the IDP crisis response, it also focuses on how and to what extent the local health systems responded to the major structural changes due to decentralization. The conceptual framework depicts that not only was the local health system influenced by population displacement, decentralization also made the situation more challenging for the local health authorities (Figure 1).
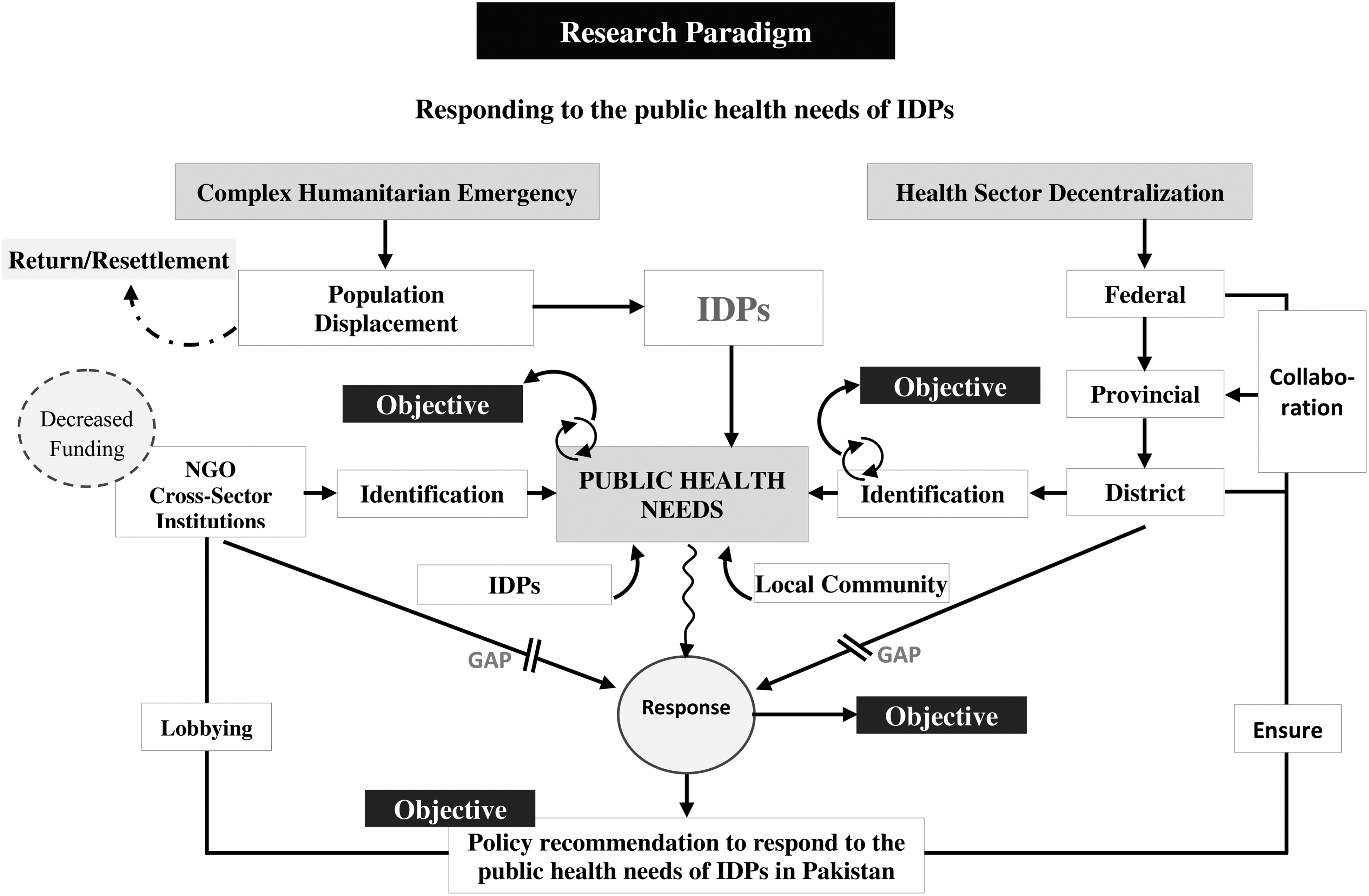
Legal framework sowing gaps between IDP health needs and services provided by the provincial health systems. “Lobbying” refers to enhancing the working relationship with the private sector for continuous support. “Ensure” refers to ensuring interdepartmental collaboration. Abbreviations: IDP, internally displaced person; NGO, nongovernmental organization.
Data Collection Procedure
The data for this article were drawn from 12 in-depth, open-ended interviews with purposefully selected managers of provincial and district health departments involved in planning and management of healthcare services for IDPs (Table 1). We developed and refined interview guides and questions to solicit the opinions and experiences of the study participants, pilot testing the questionnaire to validate the content and to identify any discrepancies in the data collection tools. Faculty members from the University of Peshawar with relevant expertise thoroughly reviewed the revised questionnaire. We then conducted interviews in the participants' offices at times that were convenient for them.
Study Interview Respondents
Data Analysis
The interviews were first recorded in Urdu and then translated and transcribed into English. The team then conducted a content-based/thematic analysis to analyze the English-language transcripts. The analysis had 3 stages. First, we used open coding to review and categorize data according to descriptions of the study participants. Second, we used axial coding to make correlations between the coded categories. Finally, we coded the data thematically based on emergent themes, subthemes, and categories without imposing a priori categories. 31
Ethical Clearance
Ethical clearance for this study was obtained from the Bioethics Committee of the Health Services Academy, Islamabad and the Provincial Disaster Management Authority of Khyber Pakhtunkhwa. We sent a formal letter and an email to each participant wherein we explained the objectives of the study and asked for an appointment to conduct the interview. Written, informed consent was obtained from all study participants prior to the interviews. We also ensured complete anonymity and confidentiality.
Results
The research team assessed the local health system response to IDPs based on themes that emerged from the in-depth interviews, which are outlined next.
Theme 1: Recipient Area Capacity to Support IDPs
From 2005 to 2014, armed conflicts and natural disasters led to large population displacements throughout Pakistan.
32
The proportion of IDPs was particularly high in the province of Khyber Pakhtunkhwa. According to the director general of the Provincial Disaster Management Authority of Khyber Pakhtunkhwa:
[T]his province is highly vulnerable to complex emergencies, including both manmade and natural hazards.
The needs of these IDPs placed immense pressure on the local health system. Many public and private organizations were involved in the early phase of relief activities. Adjusting existing health services and programs and planning new short-term interventions for IDPs were enormous challenges for the local health departments. According to a manager in the provincial health department:
At [the] start, all the available resources were mobilized to enhance the capacity of the health departments of IDPs recipient areas. The technical assistance was mainly provided by the United Nations [UN] organizations for devising short-term strategic plans.
The sudden influx of IDPs affected the routine planned activities. A substantial amount of additional work was required to respond efficiently to the situation.
Theme 2: Local Health System Challenges
Initially, UN organizations, particularly the UN High Commissioner for Refugees and World Health Organization (WHO), were mainly involved in planning health programs and health services, with the Pakistani government in a supervisory role. As the team leader of an international organization commented:
[I]t was a big challenge for all of us. The UN organizations provided technical and logistical support to the government. The WHO field guidelines in emergency situation were followed to make the short-term health plans for IDPs.
The return of IDPs from the Jalozai camp in Nowshera District to their place of origin started in 2015. Although a majority of IDPs were returned, hundreds of families continued to live in the Jalozai camp. As a result, the district health system had to extend its services and provide all basic health services to the remaining IDPs, in addition to local residents. The additional users overstretched the local health system and compromised service provision to the local community. The in-charge of a primary healthcare facility stated:
We don't have sufficient drugs and medical supplies to accommodate the IDPs.
Theme 3: Impact of Health Sector Decentralization
After decentralization of the health sector, all activities, including planning and implementation of health programs and services for IDPs and the local community, became the sole responsibility of the provincial and district health departments. A manager from the district health department pointed out:
In [the] first few years of decentralization, policy, planning, and implementation of long-term health programs was very difficult for us.
The arrival of IDPs in the district increased demand for health services and the budget required for these services. The government received financial contributions from different international donor and humanitarian agencies. The team leader of an international organization stated:
[T]he UN OCHA [Office for the Coordination of Humanitarian Affairs] was responsible to bring the humanitarian actors in Pakistan after [the] 2005 earthquake. They established [the] Pakistan Humanitarian Pooled Fund in 2010, which is still working.
Although the number of trained healthcare workers was adequate in Nowshera District, ensuring that staff had the required qualifications for scopes of work in different areas was a challenge. Another problem, alluded to by a participant, was the capability of health workers to plan and implement health programs at the local level and to translate the central government's policies into local policies. As he said:
We are lacking with the skilled workforce who can translate and apply the central-level health policies to the local situation. The health managers at district level need training and short courses to enhance their capacity in the field of policy planning.
The imbalanced distribution of health facilities in rural and urban areas of Nowshera District also greatly influenced the numbers and qualifications of the health workforce, since doctors were more interested in working in urban health facilities.
Theme 4: Interdepartmental Collaboration
In Pakistan, natural and manmade disasters have always required a national response to address the needs of local populations and to safeguard the health and wellbeing of IDPs. Since the implementation of the decentralization policy, coordination has remained an issue between provincial departments and the Ministry of National Health Services Regulations and Coordination at the federal level.
The arrival of IDPs in Nowshera District provided an opportunity to enhance coordination between health departments at district, provincial, and federal levels. A manager in the district health department pointed out:
[T]he collaboration among different sectors proved to be highly useful in terms of assigning responsibilities and to avoid the duplication of services provided by them.
Several international and domestic national nongovernmental organizations (NGOs) were involved in the provision of basic services to IDPs in the Jalozai camp. These NGOs commenced their activities in the early phase of displacement in 2009 and continued their support until the government announced the return policy for IDPs in 2015. The project manager of a local NGO stated:
[O]ur organization started to provide basic health services in Jalozai camp in 2009. We were also part of health cluster meetings, but still there was overlapping of the health programs offered by different NGOs and by the local health authorities.
The research findings highlighted that NGOs had a positive role in the provision of basic health services to IDPs until the return policy was enacted in 2015. From that point forward, the support and cooperation stopped.
Discussion
The interviews generated valuable insights from managers of public- and private-sector organizations involved in the planning and management of health programs for the IDPs living in recipient areas. The district health department made all possible efforts to provide adequate health services to both IDPs and the local community. However, as some interviewees indicated, several gaps in the existing infrastructure of the local health system compromised the health needs of IDPs. The devolution of the health sector also considerably tested the knowledge and skills of the local health management in planning and execution of health programs.
Local Health System Experience in Health Program Management
Population displacement due to complex emergencies affects the local health system of recipient areas. 33 During times of conflict, protecting healthcare systems becomes even more difficult, which influences the availability of health services to the displaced population. 34 Our research findings were consistent with findings from the wider literature that the arrival of IDPs in the Jalozai camp affected the local health system and that managing the health programs and services for IDPs was challenging for district health departments.35,36
Healthcare providers often underestimate the importance of specific needs assessments in emergencies and perpetuate the perception that there is a lack of demand for specific services from IDPs. Health departments face particular challenges in gathering relevant field information to enable better situation analysis and to manage the health programs and services properly. 37 In our research, a dearth of reliable information about health programs and services for IDPs was a critical issue. We found that no short- or medium-term health plans existed for the IDPs who refused to return to their place of origin and continued to stay in the Jalozai camp area.
Targets set at the central level for different health programs were unrealistic at the district level given the lack of health resources. The lack of technical capacity at the district level and reliance on central-level guidelines also made it difficult for district health authorities to explore local health issues and subsequently plan and execute need-based health programs and services for IDPs.
Decentralization and the Health System Response to IDPs
The decision to decentralize was made at a time when Pakistan was overwhelmed with complex emergencies. The devolution of health planning to the provinces had an impact on the local health system. 38 The local government depended on central-level policy guidelines to make their own health plans and programs, which further slowed the health decentralization progress.
Pakistan's healthcare infrastructure is spread widely throughout the country. Due to inadequate financing, structural mismanagement, and lack of resources, its utilization has remained very low. Shaikh et al 39 found that the allocated budget for the health sector in Pakistan always has been inadequate, with several weaknesses in the health financing mechanism, particularly in the devolved health system. At the time of this research, local funding for healthcare was limited.
Decentralization aims for fair, realistic, and need-based distribution of the health workforce to the districts. 40 Our study of the devolved health system in Pakistan identified several system weaknesses related to human resources, including the lack of a trained and skilled health workforce, capacity and accountability of administrators, and evidence-based policy formulation at the district level. These findings are consistent with the wider literature. 41 For example, in Sierra Leone, the majority of health workers who remained after conflict preferred to work in district hospitals rather than in primary healthcare facilities of rural areas. 42
In Pakistan's devolved health system, the provision of adequate and appropriate health services to IDPs became the responsibility of provincial and district health departments. Due to limited resources, the district health department had to integrate health programs and services for IDPs with those provided to the local community. One research study suggested adapting an “integration to outcome model” for the integration of existing health services. 43 However, the integration was not carried out in an organized or strategic way, and therefore the district health authorities were uncertain about the efficiency and effectiveness of integrated health programs and services.
Intersectoral Collaboration
The constantly changing patterns of health problems and their determinants have required consideration of health issues from a new perspective. Due to limited resources, a single sector alone cannot address the wide range of public health problems of vulnerable populations. 44 The devolution of the health sector in Pakistan was seen as an opportunity to facilitate intersectoral collaboration. A district health management team was formed to increase cooperation among multiple sectors (eg, health, education, population welfare, water and sanitation departments), which would, ideally, improve the living conditions and health status of the Pakistani people. However, the district health management team failed to achieve the desired results due to lack of cooperation between the bureaucracy and district administration, as the former considered their powers to be curtailed. 45
Many nations affected by complex emergencies have limited response capacity and need the support of the international humanitarian community. 33 The Inter-Agency Standing Committee adopted a coordinated cluster approach to humanitarian response and is recognized globally as a best mechanism to implement effective relief activities. 46 Pakistan adopted the cluster approach to respond to the humanitarian crisis that followed a massive earthquake in 2005. 47 Later, Pakistan used the same cluster approach to assist with the conflict-induced displacement in Khyber Pakhtunkhwa Province, where the government health authorities and WHO mobilized local and international humanitarian partners to assist IDPs. The response of cluster NGOs was quite noticeable in the early years of displacement. The response gradually decreased due to limited funding caused by lack of donor interest and the emergence of the Syrian humanitarian crisis. 48
Conclusion
Humanitarian crises and resultant population displacement have applied immense pressure on public services—including education, healthcare, and economic services—in IDP recipient areas in the northwestern province of Pakistan. The public health institutions of recipient areas lacked the capacity and experience to develop health programs and to provide health services to the newly arrived displaced people. The main reason for this gap in service provision was the absence of national legislation that focuses primarily on IDPs. The lack of visionary leadership, weak provincial policies, inadequate financing, and unstable health system responding to the public health needs of IDPs posed daunting challenges for both district and provincial health departments.
Organizational restructuring of federal, provincial, and district health departments due to health sector decentralization has given rise to the need to redefine the functions of health departments at all levels. We recommend that health departments collaborate with other public-sector departments and with private organizations at federal and provincial levels, as a vital strategy to improve healthcare coverage of IDPs and other vulnerable populations. Government agencies should also collaborate with international humanitarian organizations to solicit financial aid and donations for the management of IDPs.
Our study findings suggest a dire need for local governments to collaborate with UN agencies to develop overarching binding international laws and local national policies for complete protection of IDPs, particularly their health, shelter, and social security. Forced displacement is not reflected in the Sustainable Development Goals, and migration is addressed explicitly only in Goal 10. We therefore recommend that health-related Sustainable Development Goals based on a human rights framework should be applied to the situation of IDPs. This could become a key approach to improving the IDPs situation and for humanitarian actors to take increased responsibility for their health.
In the case of Pakistan, already established disaster management authorities at national, provincial, and district levels (ie, National Disaster Management Authority, Provincial Disaster Management Authority, District Disaster Management Authority) should be responsible for devising and implementing actionable strategies and tools that can be used at operational levels. There is also a dire need to establish an impact assessment monitoring system to ensure accountability. This system should have the capacity to recognize the public health needs of displaced populations, define attainable results, provide access to essential healthcare services, and monitor progress by applying key health indicators.
Finally, our research identified several gaps in the knowledge base, including gaps on livelihood, social protection, and services for IDPs. To address these gaps, we recommend further research on IDPs' public health needs, health systems, and health sector decentralization policies.