
Abstract
An international system should be established to support personal protective equipment (PPE) inventory monitoring, particularly within the healthcare industry. In this article, the authors discuss the development and 15-week deployment of a proof-of-concept prototype that included the use of a Healthcare Trust Data Platform to secure and transmit PPE-related data. Seventy-eight hospitals participated, including 66 large hospital systems, 11 medium-sized hospital systems, and a single hospital. Hospitals reported near-daily inventory information for N95 respirators, surgical masks, and face shields, ultimately providing 159 different PPE model numbers. Researchers cross-checked the data to ensure the PPE could be accurately identified. In cases where the model number was inaccurately reported, researchers corrected the numbers whenever possible. Of the PPE model numbers reported, 74.2% were verified—60.5% of N95 respirators, 40.0% of face shields, and 84.0% of surgical masks. The authors discuss the need to standardize how PPE is reported, possible aspects of a PPE data standard, and standards groups who may assist with this effort. Having such PPE data standards would enable better communication across hospital systems and assist in emergency preparedness efforts during pandemics or natural disasters.
Introduction
Healthcare is the fastest growing industry in the United States and is projected to increase from 19.8 million workers in 2020 to 23.1 million by 2030. 1 As the number of workers employed in the healthcare industry continues to increase, so will the demand for personal protective equipment (PPE) during routine workdays and even more so during public health emergencies. Within the healthcare industry, PPE is a consistent and critical component used within the hierarchy of controls. 2 During previous infectious disease outbreaks such as Ebola and influenza A, researchers examined and demonstrated the need for healthcare professionals to appropriately use PPE to reduce disease transmission.3-6 Results of these studies have provided insight into best practices for PPE compliance during public health crises; however, the disruption in PPE supply chains and subsequent surge in demand has made both compliance and implementation of best practices difficult to ascertain in terms of practicality and feasibility. For example, while preparing for the Ebola epidemic in the United States, many healthcare facilities were unable to obtain the quantity and types of PPE needed due to haphazard, large-volume ordering of PPE that caused national shortages for certain items, delays in orders, and uncertainty among product manufacturers. 7
These public health crises have demonstrated a need to establish an information technology (IT) architecture system that can be used to support nationwide PPE inventory monitoring and analysis, particularly within the healthcare industry. Although research has identified the need for national surveillance and measures for reporting PPE, 8 studies regarding the utility of such systems have not been completed. Consequently, the US healthcare industry does not have a central, neutral platform to share and exchange PPE inventory data during public health emergencies, nor does it have a standardized system for monitoring PPE inventories. Rather, these data are managed by disparate, proprietary entities that can capture and display only a small portion of the healthcare industry's data. Unfortunately, this model precludes hospitals, suppliers, stockpiles, state and local health departments, and emergency response planners from being able to collect, aggregate, and analyze data in a secure and trusted way to inform decisions. Without a standardized system for monitoring PPE inventories, the demand for PPE is likely to become further exacerbated during pandemic situations that cause panic purchasing. To this end, research, development, and even policy planning in PPE inventory monitoring and surveillance is critical.
The full benefit of a PPE inventory system to hospitals and emergency response planners will be realized only if it is automated to provide near real-time (eg, daily) data. A near real-time PPE inventory monitoring system that is used by major hospital networks, suppliers, and emergency stockpiles will enable decisionmakers to have accurate information about PPE inventories during emergencies and closely monitor their PPE use during routine clinical care. During a public health emergency, it is critical that federal, state, and local government stockpiles can help officials quickly capture the status of current inventories and potential shortages based on the quantity of PPE currently in the hospital's possession, PPE already purchased (and whether the order will be filled on time), and PPE requested but not yet fulfilled. Inaccurate reporting, however, makes it difficult to track inventory counts that are purchased, fulfilled, or unfulfilled.
In this article, we take a step back to assess the more formative issue of PPE inventory reporting in the healthcare industry to advance a valid and reliable mechanism for completing and deploying a national surveillance system that can operate during both routine and emergency responses. During the first phase of research, we conducted a proof-of-concept effort to demonstrate the feasibility of developing a scalable and automated PPE surveillance and monitoring inventory system. To initially scale and appropriately use the results of this pilot effort, participating hospital systems provided data for 3 types of PPE: N95 filtering facepiece respirators (hereafter referred to as N95 respirators), surgical masks, and face shields. The objective of this article is to assess the feasibility of automating data extraction from numerous, disparate data systems across participating hospitals where no standard nomenclatures or data reporting formats exist. Before discussing this research and development effort in more detail, we provide background information and context to better forecast the impact of this work.
Historical Background of PPE Inventory Monitoring System
In 2012, the National Personal Protective Technology Laboratory (NPPTL), a division of the National Institute for Occupational Safety and Health (NIOSH), identified the need for a PPE inventory monitoring system in healthcare and initiated formal research in this area. One effort was a contract with Vanderbilt University that culminated in the development and deployment of a PPE Preparedness, Responsiveness, and Outcomes surveillance system that was deployed with 26 hospitals.8,9 This surveillance system was initially based on a paper survey that eventually expanded to a structured electronic questionnaire for hospitals and health systems to manually self-report PPE inventory and purchase information with the manufacturer and model numbers. 9 Although this effort demonstrated that relevant supply and demand data are captured by hospitals and able to be retrieved, notable barriers were identified. For example, a hospital administrator had to coordinate across departments and systems to manually enter information in the electronic database, which required additional time and staffing, creating a barrier to real-time PPE inventory monitoring. Automation through electronic data exports from various systems also introduced new and significant concerns from hospitals, including an unwillingness to electronically export data using an information architecture that was governed and secured by the federal government.
Consequently, in 2018, NPPTL and other US Centers for Disease Control and Prevention organizational units outlined a renewed need for a near real-time PPE inventory monitoring system that could address these identified gaps in trust and automation while being able to monitor PPE use during routine clinical care and emergencies. First, perceptions and challenges related to PPE inventory monitoring were collected including: (1) unwillingness of hospital entities to electronically export data using an architecture that was overseen and secured by the federal government, demanding the need for a standard trust architecture and data use agreements; (2) difficulties in sustaining manual and accurate PPE inventory reporting to predict national and local PPE shortages, necessitating the need for automated electronic exports of data that follow a standard nomenclature; and (3) inability of small hospitals—making up about 70% of the industry—to allocate resources to daily PPE reporting and often being excluded from viable efforts. 10 These were just some issues considered when identifying potential solutions for a PPE inventory monitoring proof-of-concept prototype.
Working Toward an Automated System
NPPTL identified and initiated a contract with the Center for Medical Interoperability (C4MI) in 2019. 11 C4MI is a 501(c)(3) cooperative research and development laboratory funded by health systems to simplify and advance data sharing among medical technologies and systems using a centralized, vendor-neutral approach. A key objective of this group is to achieve an interoperable healthcare system, with approaches being informed by its hospital steering committee. The committee is staffed by representatives from member hospitals and consists of leading executives of some of the largest health systems in the United States and represents a diversity of healthcare distribution by way of more than 500 hospital sites spread across the country.
C4MI and its hospital steering committee determined that the lack of interoperability was not only a barrier to a nationwide monitoring and analysis system for critical healthcare assets but was also a significant barrier to hospital interests. Consequently, there was a shared interest between hospitals and the federal government in the need for: (1) an information architecture that promotes automation and interoperability between hospital data systems, (2) an affordable system for all hospitals, and (3) a system that meets the security and trust requirements demanded by hospitals to support the sharing and analysis of their data with third-party devices and users.
NPPTL, C4MI, and its hospital steering committee initiated a public–private partnership to pilot the design, development, and maintenance of an automated system. The steering committee determined which hospitals and systems would be best positioned to participate in this pilot effort. The committee chose a small county hospital, a midsized hospital system limited within 1 state, and a very large hospital system that spanned the United States. All of the hospitals and healthcare systems that were initially contacted by the steering committee agreed to participate in this pilot demonstration, which facilitated the development of a Healthcare Trust Data Platform (HTDP) and an app that used the platform to secure and transmit PPE inventory data for N95s, surgical masks, and face shields. C4MI obtained common data use agreements from each participating entity to allow for third-party data usage. Participating entities remained in control of their data while providing transparent accessibility and use of the data.
Healthcare Trust Data Platform
Based on input from C4MI's hospital steering committee and the healthcare information management agenda published by the Institute of Medicine and National Research Council, 12 the HTDP was designed to provide a trusted pathway for long-term, nationwide data management within and among medical devices, hospitals, and emergency response planners (Figure 1). The HTDP included a technical architecture and governance framework in which participating hospital systems entered into an agreement to securely exchange data via auditable transactions with hospital information systems and other participating systems. 11 Participating entities retained full control over permissions and visibility into data exchanges. This quick and on-demand trusted access to data (and associated information by care team members, patients, and other authorized recipients) also reduced clinician burden. A catalog of technical documents and specifications for the HTDP architecture was developed and reviewed with the hospital steering committee. Using this framework, large hospital systems may continue to work with proprietary data apps and cloud services in addition to apps provided through the HTDP, whereas smaller and more limited resource hospitals may rely on the HTDP and any apps distributed with it as their only cloud data service. With the background architecture and implementation defined, it was then necessary for the public–private partnership to establish a vision for management of user access and permissions to the HTDP apps.
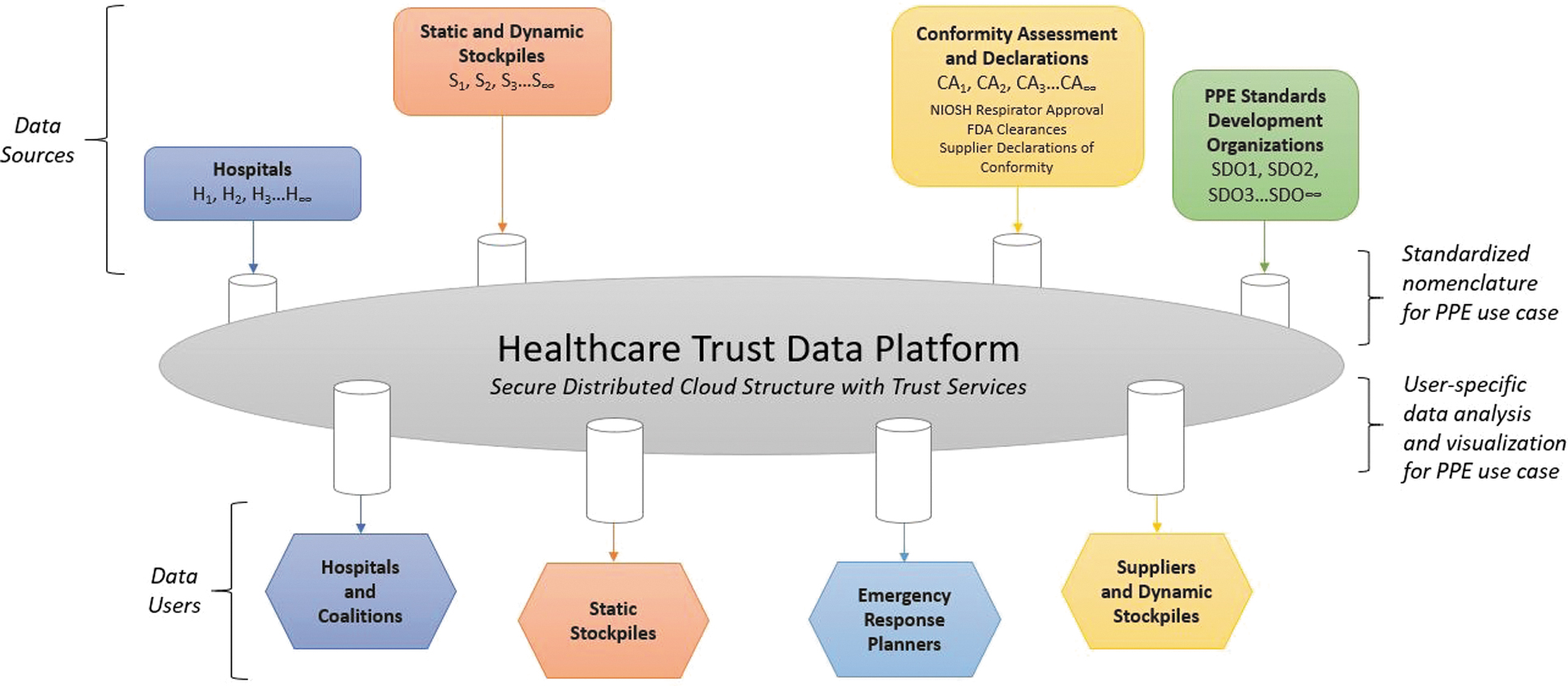
Illustration of the long-term vision of the Healthcare Trust Data Platform and its ability to support nationwide data sharing and analysis that supports medical device interoperability. The current study only evaluated the hospitals as the data source and the quality of the data that was produced. Additional information from this figure would need to be evaluated in the future. Abbreviations: CA, conformity assessment and declaration; FDA, Food and Drug Administration; H, hospitals; NIOSH, National Institute for Occupational Safety and Health; PPE, personal protective equipment; S, static and dynamic stockpiles; SD, PPE standards development organizations.
PPE Supply Management App
C4MI developed an alpha PPE Supply Management app that was deployed using the HTDP (Figure 1). The public–private partnership decided to use a mobile-friendly web app, known as the TOGETHER Portal, that would list all apps integrated through the HTDP. Because a standardized nomenclature and format for collecting PPE data did not exist, a systematic app development process was followed. Standardized datasets were created to normalize nomenclatures and formats based on desired data that were disparately named and formatted across proprietary or custom-built hospital data systems. Researchers had to establish 1 dataset for each of the 3 PPE types and then apply the provided hospital systems' data to the proprietary PPE inventory systems algorithms that were created. The app was designed to proceed through multiple development phases—the first of which is the proof-of-concept demonstration discussed in this article. This effort focused on exporting data from hospital systems that provided (1) hospital characteristics (eg, urban vs rural, US state where the hospital is located, and bed capacity) and (2) PPE inventory and purchasing data such as pending orders, delayed orders, and orders without a delivery date.
Objectives
The methods described in the following section focus on the deployment of the PPE Supply Management app and its compliance with the nomenclature and data format initially established by the research team. In this article we focus on: (1) the proof-of-concept deployment of an HTDP that addresses previously identified gaps in trust and automation; (2) lessons learned about challenges identified during the deployment; and (3) components still necessary to deploy a beta version that can collect valid and reliable PPE inventory data to inform routine preparedness and emergency response efforts.
Implementation Methods
Data Collection and Extraction Process
The alpha PPE Supply Management app was developed and deployed in 2020, and initially focused on the automated exportation of PPE data from participating hospital systems. First, a data model for inventory and purchase order information was created to standardize data collected and represented from participating hospital systems. Participating hospital systems then established daily automated reports that queried relevant hospital information systems, converted the daily reports to a common data model, and transferred results to the app, which made the data available to other participants via the HTDP. C4MI then aggregated the daily data and reported it to NIOSH weekly for each of the 3 PPE types: N95s, surgical masks, and face shields.
Hospital systems were asked to report daily, current individual hospital inventory—the quantity of PPE in their possession. These data were to be reported separately for each PPE type and disaggregated by individual units according to manufacturer and model number. Additionally, hospital systems provided their purchase orders and status updates. Using these data, C4MI developed analyses algorithms to calculate replaced individual hospital inventory and individual hospital burn rate estimates for the 3 types of PPE reported. No participating hospitals or systems dropped out or stopped providing data throughout the demonstration period. Although the details of the PPE inventory data are of interest, in this article we describe the proof-of-concept demonstration of the HTDP and app and highlight the feasibility and successes of hospital systems' willingness to share their data for third-party access.
Sample
Hospital systems entered near-daily inventory information in the alpha PPE Supply Management app from June 1 to September 10, 2020. When the alpha version deployed, 12 hospitals were participating. Ultimately, 78 hospitals participated, including a large hospital system (66 hospitals), a medium-sized hospital system (11 hospitals), and a single hospital. The single hospital and medium-sized hospital system signed data use agreements in May 2020 and was able to integrate the app into their hospital systems with relative ease. The large hospital system, comprising hospitals across the United States, took longer to onboard. Their data use agreement was signed in late June 2020 after lengthy legal reviews, and additional time was needed to work through a major system upgrade, which delayed the identification of hospitals ready to share data. Consequently, the large hospital system started sharing data during the ninth week of the 15-week demonstration. Hospitals were located in 17 states and represented 7 of the 10 US Health and Human Services regions (Table 1).
Hospital Participation by HHS Region
Abbreviation: HHS, Health and Human Services.
Upon receiving the final data from C4MI, NIOSH cleaned and subsequently recoded data variables. To inform future development of a beta app, including updates to nomenclature and format, this manuscript discusses the PPE data validation process.
PPE Data Validation
Researchers relied on information about respirators from trusted sources such as an NPPTL webpage containing information about NIOSH-approved N95s organized by model number, manufacturer, and, if applicable, NIOSH approval number. 13 Additionally, the webpage noted which surgical N95 respirators were also cleared by the US Food and Drug Administration (FDA). For a majority of the N95s reported, researchers used the NPPTL webpage to verify the model numbers.
For surgical masks, researchers used the FDA 510(k) Premarket Notification website 14 to cross-check model numbers and manufacturers. However, this website contained information for only a handful of surgical masks reported. Consequently, researchers used standard internet search engines and typed in the model numbers and manufacturers provided by participants to verify the data reported. In most cases, if the correct model was provided or even a corresponding stock-keeping unit (SKU) or vendor number, researchers were able to locate the surgical mask and, if needed, update the model number. When the distributor was incorrectly reported instead of the manufacturer, researchers used the same validation process to identify the correct manufacturer. While researchers searched for and verified surgical mask model numbers, they also reviewed the product manufacturer pages, specifically, to determine whether surgical masks were approved by ASTM International (formerly the American Society for Testing and Materials). 15 Most major manufacturers provided documentation if they claimed a surgical mask was certified by ASTM at levels 1, 2, or 3.
The same process was used to verify face shields. Researchers started with the FDA 510(k) Premarket Notification website 14 but quickly moved to internet search engines. Because fewer standards exist for face shields, researchers only made note of whether the face shields were half- or full-face and whether they were reusable or disposable. Table 2 shows an excerpted example of raw data provided by participating hospitals, and Table 3 shows the same data with the updated, verified model numbers and manufacturers. These tables show example data for N95s only, but we used the same validation process to accurately update surgical mask and face shield model numbers as well. This example demonstrates how small nuances in the way PPE model numbers are reported affects whether the model appears unique within an automated system, thereby highlighting the importance of small errors, such as spacing when entering a number.
Example of Raw Data Provided by Participating Hospitals
Abbreviations: CIHI, current individual hospital inventory; FFR, filtering facepiece respirator; PPE, personal protective equipment.
Revised Data Provided by Participating Hospitals After Verification a
Changes made to the original data are shown in bold italics.
Abbreviations: CIHI, current individual hospital inventory; FFR, filtering facepiece respirator; PPE, personal protective equipment.
Among the 3 PPE types, participating hospitals provided 159 model numbers, which researchers verified and corrected using the steps outlined above, resulting in updated model numbers and manufacturers. The results of this effort are described below.
Results
Table 4 shows that of the 159 PPE models initially reported, 118 (74.2%) were verified, which represents the final sample of 118 PPE model numbers.
PPE Reporting and Verification
Abbreviation: PPE, personal protective equipment.
N95 Respirator Reporting
The 78 participating hospitals reported a total of 38 different model numbers for N95 respirators and surgical N95 respirators, of which 35 (92.1%) were verified. The 3 that could not be verified came from a hospital among the group of medium-sized hospital systems. This hospital's level of reporting was minimal in that the 3 incorrect model numbers reported only occurred over a few days during the demonstration period rather than daily over the 15-week demonstration period. The number of individual units the hospital reported was also low. For the 3 model numbers that could not be verified, the hospital instead provided international testing standards or a generic name for the respirators. For example, 96 units were simply reported as “KN95” but without a model number, and therefore could not be traced. Similarly, 2,496 units were reported as “Donation N95.” Of the 35 verified N95s from all participating hospitals, 9 (25.7%) were reported inaccurately using either the vendor number, FDA model number, UPC bar code, or adding “mask” after the model number. After reassigning inaccurate model numbers with the correct ones, the final sample included 23 different models supported by 17 unique NIOSH N95 approval numbers. Additionally, 16 of the 23 N95s were approved by NIOSH and cleared by FDA as surgical N95 respirators. Figure 2 shows a detailed breakdown and visualization of results.
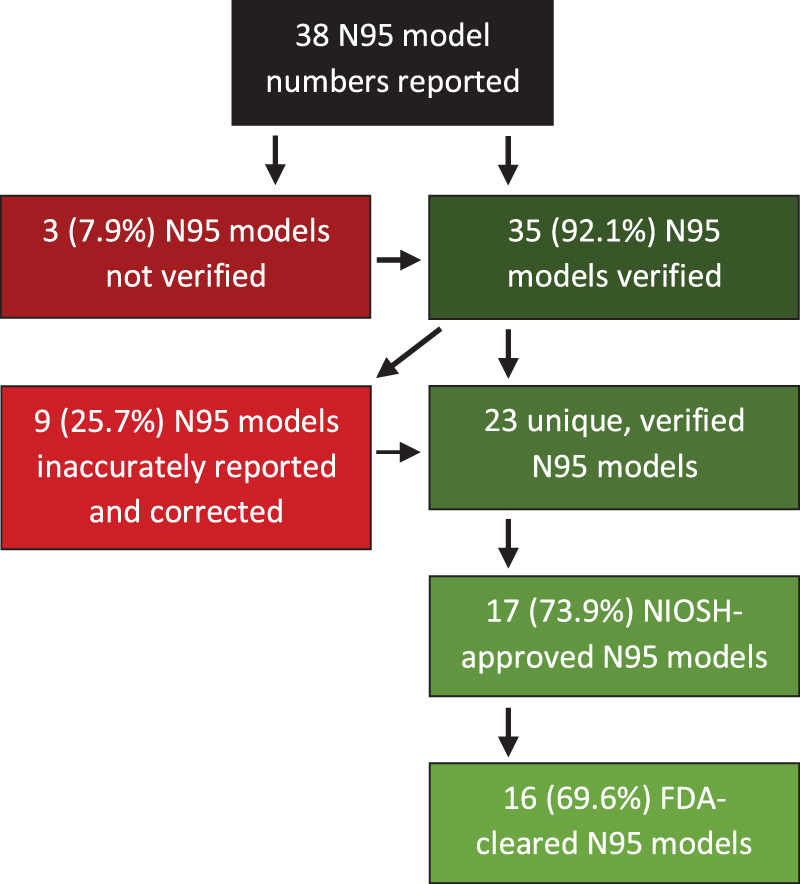
Illustration of N95 filtering facepiece respirator verification results. Abbreviations: FDA, Food and Drug Administration; NIOSH, National Institute for Occupational Safety and Health.
Participating hospitals reported 22 N95 manufacturers; however, there were only 5 unique manufacturers with the remaining being the private label distributor of the product. Private labels are used when a manufacturer enters into an agreement to have its respirators sold by another company. For example, 3M's 1860 was often inaccurately recorded, with 10 private labels listed as the manufacturer. Inaccurate reporting of the manufacturer was isolated to 1 hospital within the medium-sized system and not a trend throughout the sample.
Face Shield Reporting
Participating hospitals reported a total of 15 face shield models; however, 1 was a surgical mask, and subsequently added to the surgical mask dataset, and 1 was a powered air-purifying respirator hood, and therefore was removed from the dataset. Of the 13 remaining models, 2 were labeled as “DonationShield” and “FaceShield,” and 2 numbers reported were SKUs and, with no other model or manufacturer information available, it was not possible to verify these 4 face shields. Consequently, the majority (n = 9, 60%) of model numbers were verified. Four models were inaccurately reported and could be corrected, 1 was unique, and 3 were variations of another model number (see Figure 3 for results). A total of 9 unique manufacturers were reported, with 3 reported inaccurately using the distributor or private business name.
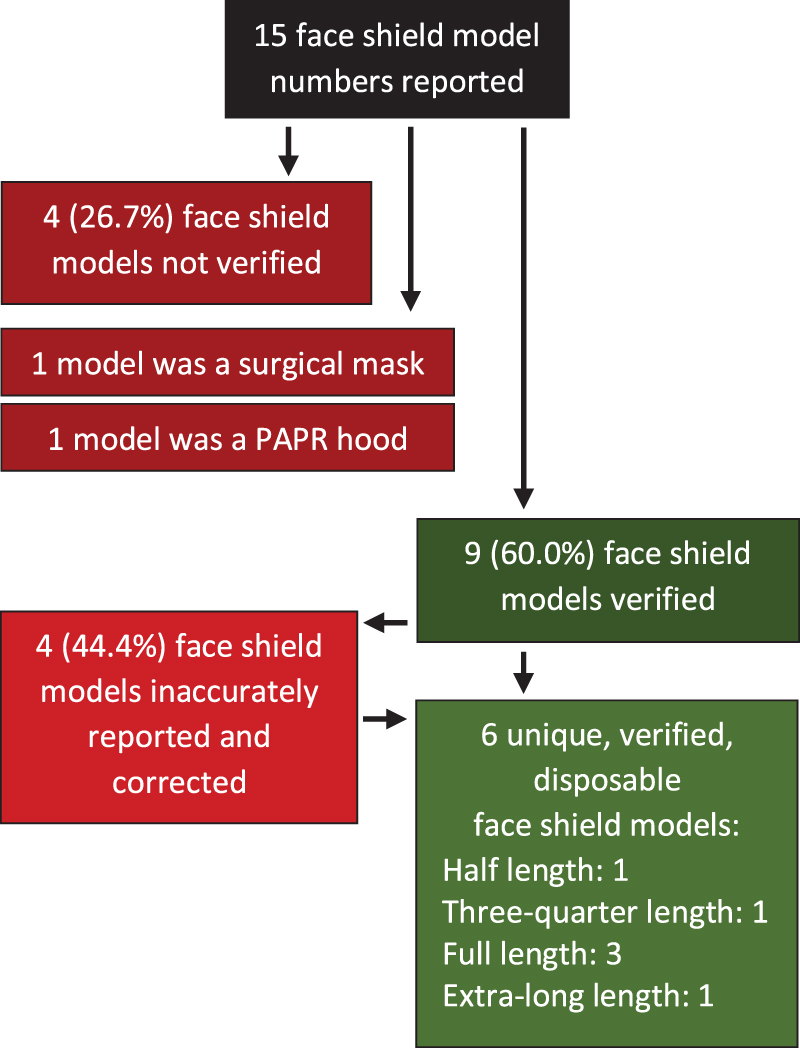
Illustration of face shield verification results. Abbreviation: PAPR, powered air-purifying respirator.
Surgical Mask Reporting
Initially, 106 surgical mask model numbers were reported. However, 1 reported model number under “Face Shield” was a surgical mask, bringing the total to 107. Of these models, 95.3% (n = 102) were verified; the models that could not be verified were reported as, “Mask,” “Masks,” “MLS-2,” and “ORSM-Mask.” Of the 102 that were verified, 21.6% (n = 22) were reported inaccurately using the vendor number, UPC bar code, or distributor number, and subsequently corrected. Another common occurrence was reporting the order number, which changes slightly when the same surgical mask is ordered in different quantities. For example, 47500 and 47500Z refer to the same product but are ordered in either 50 or 300 quantities. Thirteen surgical masks belonged to validated model numbers already reported in the data, while the remaining 9 were unique. After assigning the 13 inaccurate numbers with the correct model, the final sample of validated surgical masks was 89. Among these 89 surgical masks, 53.9% (n = 48) claimed to meet the ASTM standards. Specifically, 52.1% (n = 25) claimed to meet ASTM Level 1 standards, 6.2% (n = 3) ASTM Level 2 standards, and 41.7% (n = 20) ASTM Level 3 standards. For the remaining 41 surgical masks, researchers were unable to identify a specific ASTM level claim, although several often claimed to meet 1 or more of the 5 ASTM 2100 testing criteria. Figure 4 presents a breakdown of results, showing how the final sample of surgical masks ended up being 89. Hospitals reported 17 different manufacturers, 8 (47.0%) of which were manufacturers, whereas the remaining 9 (53.0%) were product distributors or website retailers.
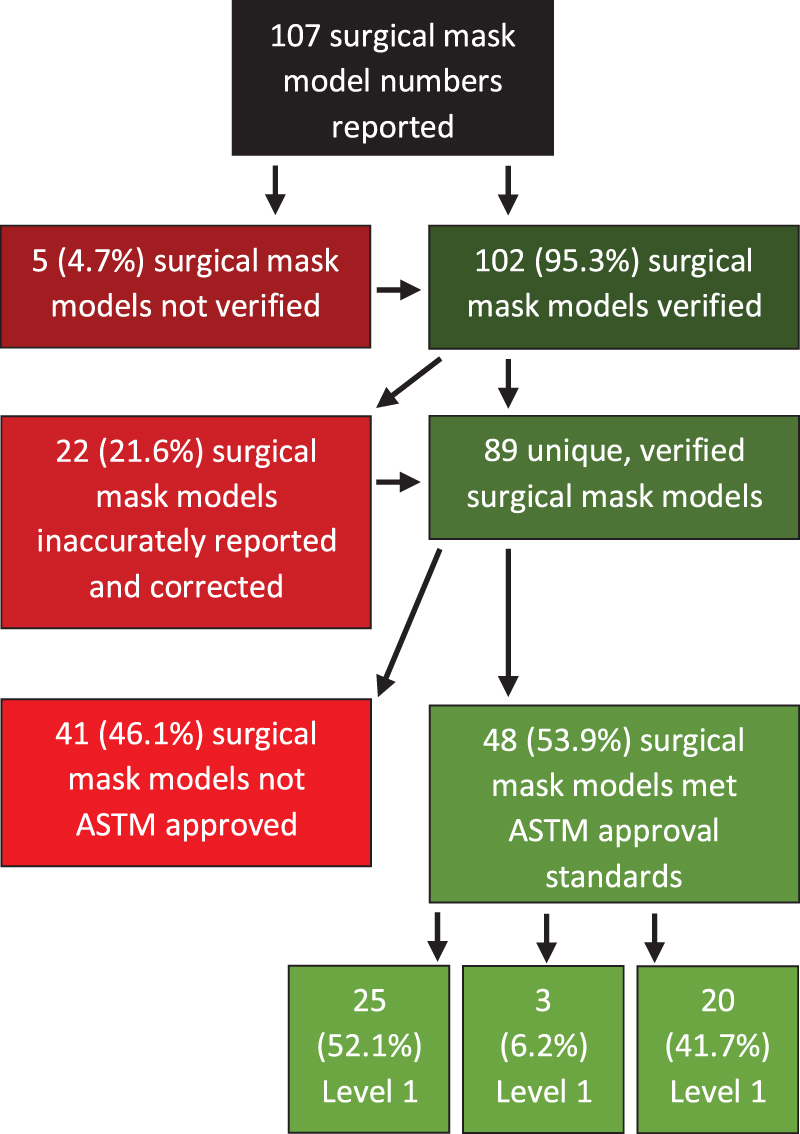
Illustration of surgical mask verification results.
Discussion
Proof-of-Concept PPE Inventory Monitoring System Successes
It is noteworthy that 3 different entities (ie, large hospital system, medium-sized hospital system, single hospital) signed agreements to participate and permit the blinded sharing of their PPE inventory data via the HTDP. This demonstrates that an overarching IT architecture can be devised for the voluntary and trusted sharing of critical PPE supply chain data. The willingness of hospital systems to sign agreements and allow the exchange of data with third parties such as state and local health departments and the US Centers for Disease Control and Prevention has historically been a significant hurdle to successfully deploying a trusted and secure data exchange. This willingness shows the interest and utility of a PPE inventory monitoring system at the hospital level. However, considering that the large hospital system took roughly 8 additional weeks to onboard (4 weeks to navigate legal reviews and another 4 to integrate the hospital systems using the proof-of-concept PPE app and inventory monitoring system), it is worth noting that different-sized healthcare systems will encounter their own unique challenges during such a process.
The initial PPE nomenclature and format developed was able to extract a highly accurate amount of PPE data and provides a solid base to continue building upon for future standards. We anticipate that such standards could inform more sophisticated data platforms to help optimize PPE inventories based on hospital characteristics, allow hospital systems and coalitions to standardize PPE for sharing, and enable PPE inventory comparisons with others that have similar characteristics to self-assess preparedness levels. Another encouraging aspect is that inaccurate reporting of models and manufacturers were primarily isolated to a few hospitals. Future analyses and publications by the authors hope to explore the variability in hospital and hospital system reporting to identify barriers to data accuracy. Identifying data validity issues within these specific hospitals will likely inform and advance considerations for a future nomenclature in this area.
Proof-of-Concept PPE Inventory Monitoring System Challenges
Using the proof-of-concept PPE inventory monitoring prototype overcame significant hurdles related to the logistics and feasibility of an automated system, but it also revealed challenges related to data validation. As described earlier, the data cleaning process involved standardizing different naming conventions for the exact same product depending on the manufacturer (and its various private label arrangements), distributor, and group purchasing organization. The lack of standardization led to a laborious and inefficient process of aggregating and analyzing PPE data across hospitals. To illustrate this challenge, 37 manufacturer names were initially reported across all participating hospitals for the 3 types of PPE, but ultimately there were only 14 unique companies. Those that were inaccurately reported as manufacturers were private label holders or distributors who market or resell the products. Not knowing the manufacturer of current PPE inventory poses challenges in predicting shortages across a state, region, or country during times of domestic PPE shortages. In addition, concerns about counterfeit and substandard respirators highlight the need to monitor PPE inventory and ensure that manufacturers and model numbers are accurately recorded for quick identification and notification in the event that equipment puts healthcare personnel at risk.
In this study, we drafted and applied a standard nomenclature and format for PPE inventory reporting for numerous and disparate hospital data systems that were not designed for this framework. Accuracy of the data reported in this study was high, but some reporting challenges still demonstrate the need for a data standard with agreed-upon nomenclature and format. Developing such a standard should be achievable, but the subsequent challenge will be for hospitals to request, require, and use appropriate software that meets this standard.
Improving PPE Inventory Monitoring and Surveillance
Establishing a global PPE standard nomenclature is critical to the success of future PPE inventory monitoring and surveillance efforts. For example, the data format assigned for NIOSH-approved respirators is different from the format used by other respirators certified to international standards, which led to difficulties in verifying international respirator models. It was also problematic to decipher between manufacturers, private labels, distributors, and the different labeling used for quantities purchased. A global PPE standard should ensure that private labels and distributors are not used interchangeably with manufacturers and should help determine how to handle different quantities purchased.
When considering relevant groups to pursue in developing standardized nomenclatures and data formats for PPE, several options exist. One option includes working with appropriate sector groups for healthcare, such as Health Level Seven (HL7), who was initially consulted on this effort. HL7 is a member group that provides international standards that offer guidance in transferring and sharing data among healthcare entities. HL7 recently published the Situational Awareness for Novel Epidemic Response (SANER) open-sourced initiative. 16 SANER aims to streamline and accelerate the real-time transmission of deidentified data from healthcare facilities that can be used during public health emergencies and disasters. 16 Although SANER is not a standards development project, aligning with HL7 could help deploy or implement some of the outcomes of proposed data standardization efforts.
Additionally, related to healthcare, the Association for Health Care Resource and Materials Management (AHRMM) 17 of the American Hospital Association leads issues related to healthcare supply chains. AHRMM acknowledges the importance of healthcare supply chain data standards and has facilitated and promoted widespread use of other unique PPE identifiers including Global Location Numbers (GLN) and Global Trade Identification Numbers (GTIN). Further, AHRMM recently posted a white paper on their website that discussed the need to work with providers, suppliers, distributors, technology partners, and providers to build a more resilient PPE supply chain. 18
Because PPE is produced for and used by more than 1 industry, it is worth considering additional standards groups so that all PPE nomenclature can be standardized moving forward. For example, the maritime industry is considered extremely hazardous, with PPE use and management among the most influential factors in preventing injury, 19 potentially making such transportation industries that relate to supply chain issues important to consider. Inclusive occupational safety and health standards groups may also be willing to work on PPE data standards that can accommodate supply chain issues or international respirators during surge events, such as the American National Standards Institute and the International Safety Equipment Association, which oversee standards and conformity assessment activities.20,21 ASTM is another important group that oversees standards, conformity assessments, and labeling, which may be useful when trying to merge new data elements into a larger data bank. 15 Including appropriate groups in efforts to standardize PPE nomenclature is important for several reasons; for example, after initial standards are developed that focus on respiratory protection, standards groups can assist with developing nomenclature for other types of PPE to improve surveillance in various occupational sectors.
Adopting a standard PPE nomenclature poses some challenges, however. The data cleaning effort in the current study's proof-of-concept demonstration would have been minimized if participating hospitals had included identifiers from existing nomenclatures such as GTIN 19 for specific models or UNSPC 22 for PPE categories. Most hospitals did not have access to these identifiers in their information systems, either because the information system vendor did not support it or because the data were not populated by manufacturers or distributors. Hospitals could manually add these identifiers themselves, but that would shift the data cleaning burden onto providers. The only way to extract clean data using an automated system is to set standards for validating data from the start, including the development of a common nomenclature, to be wholly adopted by all stakeholders including hospitals, inventory management system vendors, distributors, and manufacturers. This effort is likely challenging, but doable with the right collaborations in place.
Conclusion
The purpose of this article was to assess the feasibility of automating data extraction from numerous, disparate data systems across participating hospitals where no standard PPE nomenclatures or data formats exist, such as non-NIOSH-approved PPE. The proof-of-concept deployment demonstrated the HTDP's architecture and its ability to secure and transmit PPE-related data from inventories provided by US hospitals. Notably, hospitals signed data use agreements and remained in control of their data while providing transparent accessibility and use of the data. Lessons learned from this effort inform considerations for a future beta version and standard PPE nomenclature. The current design was limited to exporting PPE inventory data from any off-the-shelf inventory management system, whereas a future beta model must be able to handle more nuanced data by integrating updated algorithms developed during the proof-of-concept effort. A next step would be to integrate these algorithms at hospitals and other entities, such as group purchasing organizations and stockpiles, to help learn about emergency response planning. Future deployments at a beta level would render PPE inventory data that would be more easily and accurately interpreted for immediate stakeholder use.
In 2011, the Institute of Medicine indicated that standardization of PPE terms and nomenclature would enhance government and manufacturer accountability. 23 The results of our proof-of-concept study support this argument. Although NIOSH NPPTL's respirator certification program provides standardized nomenclature for N95 FFRs and surgical N95 respirators in the United States, the use of this nomenclature is not part of a domestic PPE data standard. Results from the current study show that additional, standardized nomenclature is needed at the international level to ensure an accurate representation of PPE availability and stockpiled supply. An international, widely used PPE inventory data standard would also support notification efforts when counterfeit or substandard equipment is identified. Finally, having such PPE data standards would allow for communication across hospital systems and assist in emergency preparedness efforts during pandemics or natural disasters.
Footnotes
Acknowledgments
This research received funding support from the US Centers for Disease Control and Prevention Influenza Coordination Unit within the National Center for Immunization and Respiratory Diseases. The findings and conclusions in this paper are those of the author(s) and do not necessarily represent the official position of the US Centers for Disease Control and Prevention National Institute for Occupational Safety and Health.