
Abstract
Bangladesh faces distinct challenges as a resource-poor country due to the combined effects of the COVID-19 pandemic and simultaneous dengue outbreaks. Older adults are particularly vulnerable to infection and death from COVID-19. While overall health and life expectancy in the general population have improved substantially in Bangladesh, health services for older adults are still lacking. No specialized geriatric units have been established in hospitals, and no home care programs have been established for older adults. COVID-19 mortality rates were highest among older adults ages 61 to 70 years (35%), and 71 to 80 years (20%) in 2022. Although the country's average COVID-19 mortality rate was low at 1.76%, in older adults, it was much higher (55%), accounting for 14,797 deaths, despite that most cases (55%) were recorded in young adults. During the COVID-19 pandemic, Bangladesh also experienced a dengue epidemic. Around 21,193 dengue patients were admitted to hospitals between January 1 and October 8, 2022. Without a well-established and all-encompassing social care program, the indirect socioeconomic burden of COVID-19 continues to fall on older adults. There is an immediate need for robust healthcare and support services, especially for older adults in Bangladesh, which are particularly susceptible to the dual threats posed by the COVID-19 pandemic and the dengue epidemic. Recommendations are made to protect older adults from the devastating effects of the 2 simultaneous epidemics.
Introduction
COVID-19 was initially reported in December 2019 in Wuhan, the capital of China's Hubei Province, and was traced back to SARS-CoV-2.1,2 Due to the high concomitant and rapid transmission of COVID-19, the World Health Organization declared a global pandemic on March 11, 2020. 3 As of September 7, 2023, over 215 countries and territories have been affected by COVID-19 since its discovery in 2019, with over 770,437,327 confirmed cases and 6,956,900 deaths. 4 *
COVID-19 is one of the foremost worldwide health concerns, especially for older adults, who account for a disproportionate percentage of mortality and morbidity. 5 In low- and middle-income countries located in tropical and subtropical climates, the COVID-19 pandemic has worsened already challenging situations where endemic diseases, such as dengue fever, already plague populations. 6 The combined effects of COVID-19 and dengue, 7 for example, pose an even greater threat to older adults because of their weakened immune systems and potential preexisting conditions, such as high blood pressure, diabetes, cardiovascular disease, and respiratory ailments. 8
In Bangladesh, May through September are peak transmission months for mosquito-borne diseases like dengue, chikungunya, and malaria. 9 The country faces distinct challenges as a low-income country with limited resources due to the combined catastrophic effects of COVID-19 and dengue. During the COVID-19 pandemic, the simultaneous dengue epidemic added extra pressure on Bangladesh's already overwhelmed health systems.
The worldwide annual number of dengue cases is estimated to be around 100 million, with Southeast Asia and Latin America bearing the heaviest burden.10,11 Accordingly, the combined impact of dengue and COVID-19 epidemics could have devastating consequences in tropical and subtropical cities.10-12
The total population of Bangladesh is 170 million, including 13 million older adults (ages 61 years and older) and 46 million youth (ages 15 to 29 years). Life expectancy for men and women reached 71 and 74 years, respectively, in 2018. 13 Although overall health quality and life expectancy in the general population have improved substantially in Bangladesh, health services for older adults are still lacking. No specialized geriatric units have been established in health centers, and no home care programs for older adults have been established. 14 While the country has not introduced any comprehensive social security legislation addressing the needs of older people, it has implemented numerous programs to assist older people, including pension plans, health insurance, and other aspects of the social security network including the old age allowance, freedom fighter payment, widow and abandoned women's allowance, and vulnerable group feeding. 15 Only the government pension and other insurance programs for public sector workers have focused on the needs of older adults; however, most older people, especially those who work in agriculture and manufacturing, do not benefit from these initiatives. There is a lack of attention to geriatric care because neither public and private hospitals nor nursing homes have established policies or monitoring mechanisms. 16
Family dependence, low socioeconomic status, low literacy, limited access to health services, comorbidities, and a lack of adequate social security programs all contribute to the stigmatization of older people in Bangladesh. Their lower levels of awareness and access to information regarding COVID-19 also make them more susceptible to infection. 9 Most older adults who cannot read or write think that religious people are immune to the coronavirus because of their belief system. They believe that no matter what happens, God will protect them. As a result, over 100,000 people did not follow social norms such as wearing masks and observing official restrictions at burial rites. 17 In addition, older people in rural areas may have trouble getting referred to healthcare facilities due to geographical and administrative barriers or fear of social stigma.
Older adults, especially women, have reduced exposure to mass media and awareness activities, making it more difficult for them to access information about COVID-19. 18 The simultaneous dengue epidemic had additional implications for the vulnerability of older adults in Bangladesh. For example, COVID-19 patients occupied almost all of the 16,472 hospital beds and 1,300 intensive care unit (ICU) beds, 19 making it harder for those with severe dengue to be admitted to a hospital. These numbers illustrate the underprovision of healthcare services and facilities for over 170 million people. A lack of ICUs causes many people who require urgent treatment for acute diseases, such as severe dengue patients and older adults, to delay treatment due to COVID-19. The health crisis will worsen and give rise to new health emergencies if dengue fever persists among older adults during the COVID-19 outbreak.
COVID-19 Among Older Adults in Bangladesh
According to the Institute of Epidemiology, Disease Control and Research, the first 3 confirmed COVID-19 cases were recorded in Bangladesh in early March 2020, and by October 9, 2022, there had been documented 2,029,314 confirmed cases and 29,380 deaths (Figures 1 and 2). 20
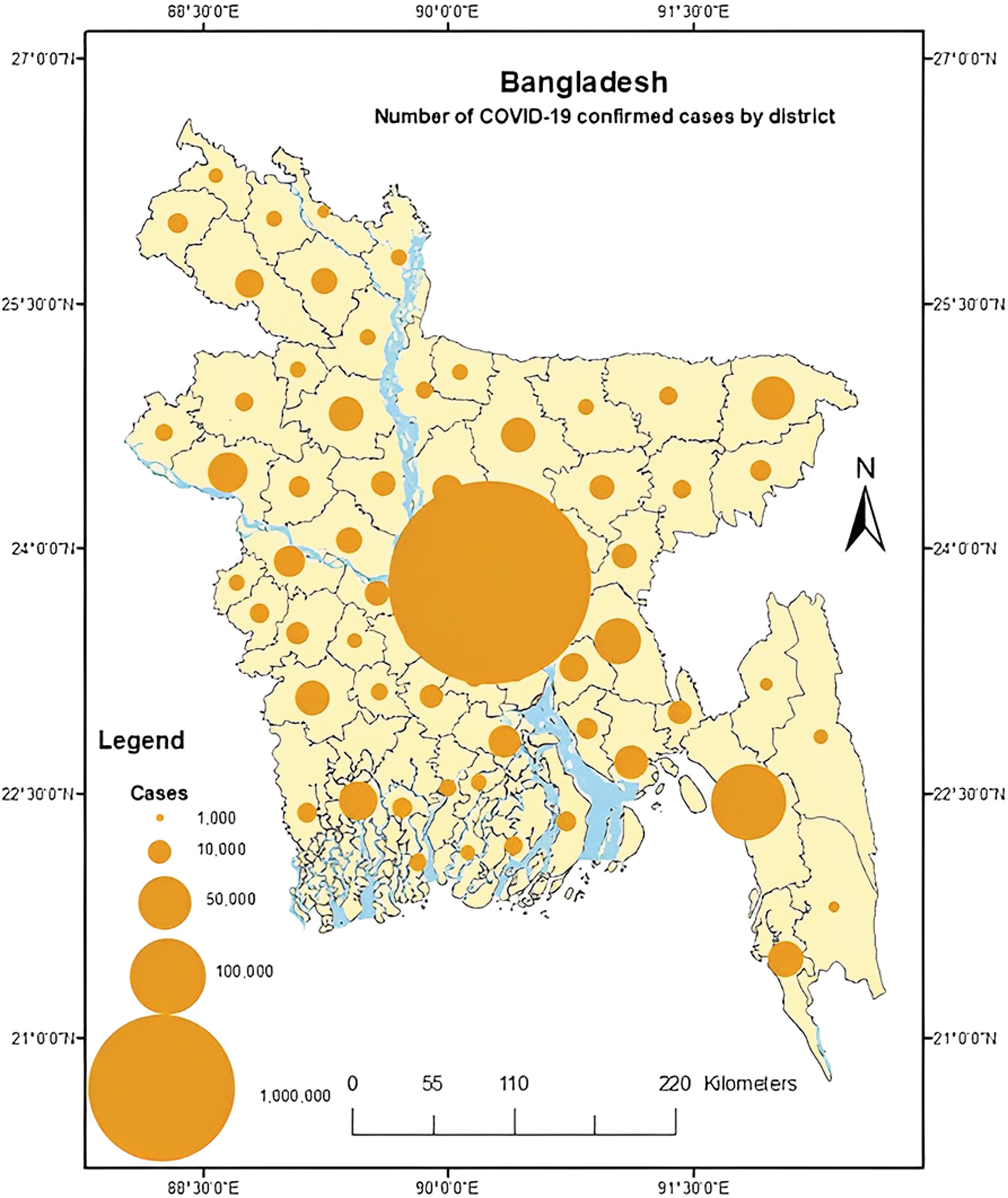
Number of confirmed cases distribution by district as of October 9, 2022.
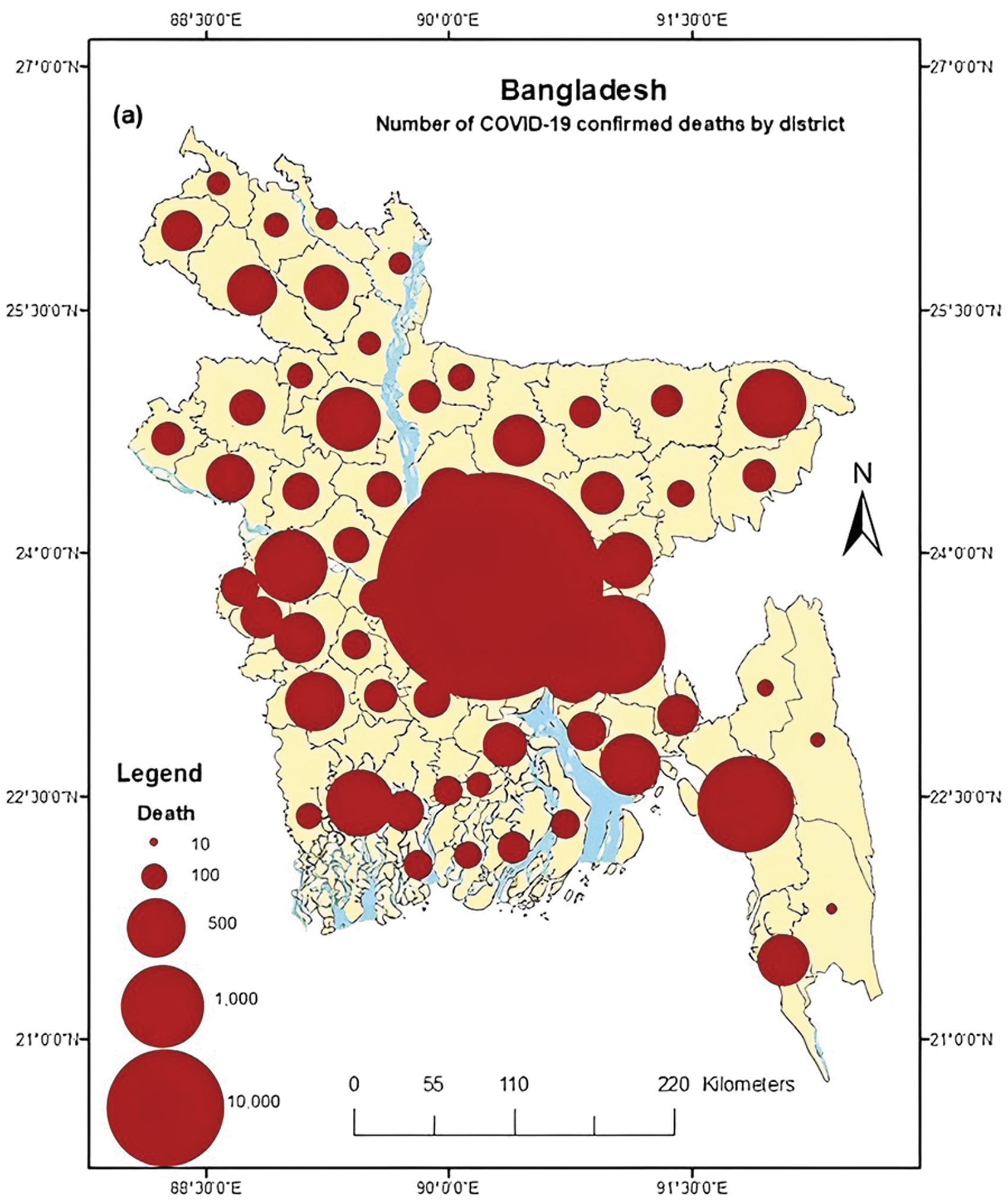
Number of deaths distributed by district as of October 9, 2022.
As of October 9, 2022, the average mortality rate was low at 1.76%; however, the mortality rate was high among older adults (55%), accounting for 14,797 deaths, despite that most cases (55%) were recorded in young adults. 21 COVID-19 mortality rates were highest among older adults ages 61 to 70 (35%) and 71 to 80 (20%). Daily transmission had decreased from approximately 30% to 10%, with an average infection rate of about 16%. As of the end of July 2022, over 100 deaths from COVID-19 had been continuously recorded daily, with older adults having the highest mortality. 19 According to the age distribution of confirmed cases and fatalities in Bangladesh, COVID-19 is especially dangerous for older adults (Figure 3).

Confirmed cases and deaths of COVID-19 by age group as of October 9, 2022.
The government of Bangladesh took every measure necessary to stop the spread of COVID-19, including canceling international flights, using thermal scanners to screen passengers, closing educational institutions and borders, and extending lockdowns across the country several times. In addition, the government allocated a small amount of financial help to vulnerable social groups, including older people and adults; however, the allocation was minimal. 2 As part of preparedness efforts, the government published national guidelines on the clinical management of older COVID-19 patients. 22
Dengue Outbreak During COVID-19 Pandemic
During the COVID-19 pandemic, Bangladesh was threatened with an epidemic of dengue fever, an endemic disease. The sudden surge in dengue cases placed tremendous stress on the healthcare system in the resource-limited country, which was already overwhelmed by the growing coronavirus outbreak.9,19 Dengue fever is a mosquito-borne virus prevalent in urban and semiurban areas in tropical and subtropical climates, including Bangladesh. Due to the temperate, humidity, and monsoon climate, Bangladesh is an ideal breeding ground for Aedes egypti, the mosquito vector for dengue. Dengue virus has 4 types, each of which is called a serotype. While recovery from 1 serotype confers lifetime immunity against that serotype, further infection with other serotypes significantly raises the risk of developing severe dengue. 23
Since October 8, 2022, the number of dengue patients has increased significantly. 19 During the first 5 months of 2022, only 100 patients were infected with dengue, and since June, the number of dengue patients continues growing. Since the end of July, more than 100 dengue-infected patients have been observed daily. According to the Directorate General of Health Service, 12,434 dengue patients have been admitted to both government and private hospitals, and more than 52 dengue patients died between the end of July and September 9, 2022, a substantial portion of whom were older adults (Figure 4). 19

Dengue cases and deaths by age group, January to September 2023. Data is presented here as of September 30, 2023. 19
An additional complicating factor is that dengue fever and COVID-19 have similar symptoms, which makes it more challenging to distinguish them and could result in increased misdiagnoses. 23 In 2022, COVID-19 patients occupied almost all hospital beds and ICUs, making it hard for those with severe dengue to be admitted to a hospital. In addition, entire medical teams were managing COVID-19 patients, whereas other severely ill patients, such as those with dengue, received less attention. 24
Dengue fever epidemics occur yearly in Bangladesh during the monsoon season because of the country's high population density, unplanned urbanization, hot and humid climate, heavy rains during monsoon season, environmental degradation, and inadequate sanitation facilities. 9
The dengue outbreak first emerged in Bangladesh in 2000, claiming 93 deaths. The virus was better controlled after that, although it grew endemic. The number of fatalities declined to nearly zero before skyrocketing in 2018, resulting in 10,148 cases and 26 deaths. A severe dengue epidemic erupted the following year, with 101,000 cases and over 179 deaths. In 2022, a total of 62,382 people were hospitalized due to dengue and 281 people lost their lives to the disease 19 (Table 1).
Number of Dengue Cases and Deaths Reported Hospitals Monthly Between 2010 and 2022
Data available up to December 31, 2022. 19
Since 2000, when the government first began tracking dengue-related hospitalizations and deaths, 2022 was the third consecutive year in which the number of dengue patients admitted to hospitals exceeded 20,000. More than 63% of hospitalizations in 2022 occurred in Dhaka's metropolitan area, with 39,220 patients being reported. 19 Bangladesh's capital, Dhaka, is rated one of the worst cities on the livability index. 25 Aedes mosquitoes thrive in the dirty urban environments that are common in the surrounding areas of most buildings in Dhaka city. The Aedes mosquitoes took advantage of Dhaka's tropical climate and dirty urban settings and made the city a new hub for mosquito reproduction. Consequently, the country could pay a high cost if the spread of dengue is not controlled promptly.
When the 2022 monsoon season in Bangladesh began with heavy rainfall, the dengue outbreak pattern was expected to be similar to 2019. Simultaneously, the number of reported cases of COVID-19 across the country rose steadily. As of October 8, 2022, dengue cases were higher (712) than COVID-19 cases (549). Their close temporal proximity suggests that dengue and COVID-19 were concurrent epidemics in Bangladesh. 26
Past outbreaks of DEN-1 and DEN-2 variants occurred in Bangladesh, but DEN-3 was more frequent in 2022. In 2022, numerous dengue patients in Bangladesh were infected by the dengue variant DEN-3, increasing the death risk. There is a strong association between DEN-3 and DEN-4 serotypes, plasma leakage, and respiratory and organ damage.19,23 However, the first case of COVID-19 and dengue coinfection in Bangladesh was recorded on May 15, 2020, in a 53-year-old man. It has been shown that COVID-19 and dengue coinfection has significantly increased patient morbidity and mortality. 23
As a low-income country with high population density, Bangladesh's older adults are the most vulnerable social group during the pandemic due to fragile health systems, socioeconomic conditions, family dependency, low literacy, natural disasters, religious and cultural faith, personal hygiene practice, attitudes toward COVID-19, comorbidities, limited access to health services, and lack of proper social security programs. 9 Moreover, sudden dengue surges increased the vulnerability of older adults during the COVID-19 pandemic. Socioeconomic issues such as unemployment and poverty worsened during the pandemic, negatively influencing older adults. Older adults continue to bear the indirect socioeconomic burden of COVID-19 without an established and comprehensive social care program. 9 The country is also in danger of increasing death rates from COVID-19 due to noncommunicable diseases among adults ages 60 years and older. 27 Nearly half of the mortality rate amounted to 522,300 deaths from noncommunicable diseases in 2012. 8 Preexisting comorbidities may also increase the vulnerability of older adults during the concurrent epidemics of COVID-19 and dengue. Older adults sometimes experience physical and logistical obstacles or fear of social stigma that prevent them from accessing healthcare centers. Older people are less informed about infectious diseases such as COVID-19 and dengue due to limited exposure to mass media and awareness-raising activities. 9 It can be difficult to convince older adults in Bangladesh about the importance of nonpharmaceutical interventions (eg, frequent handwashing, mask use, staying home, social distancing).
Challenges for Mitigating COVID-19 With Dengue Coinfection
Dengue and COVID-19 initially present with similar clinical and laboratory features, making diagnosis challenging. Both conditions manifest initially as a fever with no other distinguishing features; common laboratory abnormalities include leukopenia, thrombocytopenia, and elevated transaminases.28,29 Initially diagnosed with dengue in Singapore, patients were later infected with COVID-19 due to a false-positive dengue rapid serological test. If COVID-19 patients are misdiagnosed as having dengue and not isolated, the disease will spread throughout healthcare facilities and the wider community. A priority for healthcare systems in the tropics and subtropics should be raising awareness of dengue and using virological tests to distinguish dengue from COVID-19. 12 Although COVID-19 affects older people, dengue can become a substantial cause of morbidity and mortality in older people in a densely populated country like Bangladesh.
Coinfection with dengue and COVID-19 has been reported in several countries, including Bangladesh. 30 Two people in Bangladesh were diagnosed with coinfection in 2020; unfortunately, 1 passed away.30,31 In 2021, 11 patients were coinfected with dengue and COVID-19 in Bangladesh; 3 were older adults (Table 2). In addition, coinfected older adults' conditions were severe. 32
Dengue and COVID-19 Coinfected Patients: Demographics and Clinical Characteristics
Note: Cases described in Hannan TB et al. 32
Abbreviations: BP, blood pressure; PV, per-vaginal; RR, respiratory rate.
Bangladesh is particularly vulnerable to the COVID-19 pandemic and dengue outbreak because of the country's weak healthcare infrastructure, poor economy, frequent natural disasters, growing population of older adults, increasing number of refugees, and overcrowded urban centers. 31 Bangladesh's doctor–patient ratio of 5.81 per capita is the second lowest in South Asia. One regular hospital bed is allotted to 1,196 patients and 1 isolation bed is allotted to 23,185 patients for COVID-19. Presently, only 1,300 ICU beds are available for COVID-19 patients, whereas the ideal ratio is 1 ICU unit for every 10 regular hospital beds. These statistics reflect the minimal healthcare facilities for populations exceeding 166 million. Due to the severe lack of ICUs, many patients in critical condition, particularly older adults, must delay treatment during the COVID-19 pandemic. 2 In addition, there is a misdistribution of healthcare workers, with 78% of the population living in rural areas of Bangladesh and 70% of healthcare workers assigned to urban areas. As of August 13, 2020, there were only 3,037 members of the COVID-19 medical team, including 992 physicians and 825 nurses. 22 In addition, during the early stages of the pandemic, the government had a single laboratory dedicated to analyzing COVID-19 samples. 21 There are now 137 COVID-19 testing laboratories in Bangladesh's major urban hubs. Notably, while 66 laboratories are located within Dhaka city (59%), another 46 are outside Dhaka (41%), where more than 80% of the population resides. 14
Dengue is the most dangerous arboviral disease globally due to its high morbidity and mortality rates. 33 The lack of an effective treatment for dengue fever is a significant problem. In addition, lack of awareness is the main challenge to controlling dengue fever. 2 Supportive care is necessary for patients with severe conditions, and ICU assistance is necessary for the most critical cases. Similarly, ICU care is essential for patients with severe COVID-19. Having the dengue epidemic and COVID-19 outbreaks occur simultaneously can therefore negatively impact the outcome of both infections by decreasing access to healthcare. 33
Mitigation Measures to Curb COVID-19 and Dengue
Bangladesh has taken all possible initiatives to mitigate the adverse effects of the COVID-19 pandemic and the dengue outbreak. From April to June 2021, a nationwide lockdown was in effect (with fewer business hours and public transportation options) to control the outbreak. The government enacted the strictest lockdown (all offices and transportation were shut down) on July 1, 2021. It is worth noting that unlike in higher-income countries, lockdowns were not enforced in Bangladesh due to a lack of public support and knowledge about the benefits of such measures. Because of this, all ICUs in hospitals nationwide, especially in Dhaka, were full of COVID-19 patients in July 2021. 34 On the other hand, the country's vaccination campaign was well into its middle stages as of October 9, 2022, with 73% of the population having received the second dose of the vaccine. 22
Bangladesh's government took many initiatives to mitigate dengue during the COVID-19 pandemic. Most initiatives operated in the city corporation areas such as Dhaka, Rajshahi, and Chottogram. The primary initiatives in Bangladesh to eradicate dengue included awareness building, cleaning campaigns, monetary penalties through mobile courts after finding a favorable environment for Aedes mosquito breeding, and destroying Aedes mosquito larva breeding spots. However, most of the initiatives were insufficient for a densely populated country like Bangladesh.
A 2022 survey by the health services directorate general found an increase in the population density of Aedes mosquitoes in Dhaka, the epicenter of the dengue outbreak. Of the 3,149 households in Dhaka included in the survey, 392 had larvae. 36 This result represents a prevalence rate of 12.44%. According to the survey, the number of mosquitoes in Dhaka was twice as high as before the start of the monsoon. In the meantime, it has been reported that the government could use Wolbachia bacteria to combat Aedes mosquitoes. When Wolbachia is widely disseminated, Aedes mosquitoes will no longer transmit dengue to humans. 37 Dhaka's city administration has spent much money trying different strategies to reduce mosquito populations. The northern city government invested in drones to spray insecticide, while the southern city government opted to farm guppies, frogs, tilapia, and ducks. However, it seems like we have exhausted all of our options. The authorities have not been spraying larvicide once a week and adulticide daily on open areas, wetlands, drains, roadside spaces, lakes, and buildings to combat mosquitoes, although spraying is a proven scientific method.
Recommendations
Adequate steps to protect older adults from the concurrent COVID-19 pandemic and dengue epidemic are urgently required. Direct, immediate health consequences, mortality risk, and unintended indirect impacts disproportionately affect older adults due to COVID-19. Older adults in Bangladesh have challenges accessing their health facilities, and the resources available manage the healthcare needs of older adults are inadequate. Such gaps in geriatric healthcare during the COVID-19 pandemic and dengue epidemic may lead to many deaths and severe illnesses. Hence, to protect older people's health and wellbeing, less expensive, accessible, and adequately controlled geriatric healthcare should be developed, emphasizing health promotion, income-generating activities, and rehabilitation.
Furthermore, policymakers and stakeholders should promptly prepare for managing post-COVID-19 adverse effects on older adults. The integration of awareness messages regarding preventing and managing dengue and COVID-19 should be adequately disseminated to older adults. We highly recommend offering dengue testing free of cost for all older patients suspected of having COVID-19 symptoms and setting up a small dengue section in all hospitals to prioritize older dengue patients and minimize causalities for this vulnerable population.
Finally, we propose the following recommendations for national and regional policymakers in Bangladesh to control the dengue outbreak and protect older adults from the combined threats of COVID-19 and dengue:
Establish separate geriatric units in public and private hospitals nationally and locally to provide rapid medical assistance to older adults. Introduce mass media programs such as radio broadcasts, television broadcasts, newspaper articles, and online activities to promote awareness and knowledge in geriatric healthcare, Improve the national combined dengue and COVID-19 preparedness program focuses on older adults. Prepare special isolation housing for older adults in flood and hurricane-prone areas, and provide dedicated ambulance and boat services to transport patients with suspected or confirmed COVID-19 or dengue fever to the nearest health centers during pandemics and disasters. Engage young student volunteers to expand older adults' knowledge and hygiene practices related to COVID-19 and dengue. Adopt guidelines and instructions for caring for older adults in hospitals, clinics, retirement homes, and shelters during coexisting COVID-19 outbreaks and the dengue epidemic. Increase the level of community participation in mosquito control efforts. Prioritize public health education for dengue and COVID-19 prevention initiatives focusing on older adults. The government must regularly spray effective larvicides and adulticides and keep public areas, buildings, and shops clean.