
Abstract
Children and youth with special healthcare needs are at risk for severe consequences during infectious disease emergencies. Messages for parents and caregivers from trusted sources, via preferred channels, that contain the information they need, may improve health outcomes for this population. In this mixed methods study, we conducted a survey (N = 297) and 80 semistructured interviews, with 70 caregivers of children and youth and 10 young adults with special healthcare needs, between April 2018 and June 2019 in Pennsylvania. The survey presented 3 scenarios (ie, storm, disease outbreak, radiation event); the interviews included questions about storms and an outbreak. This article addresses only the disease outbreak data from each set. Participants were recruited through convenience samples from an urban tertiary care children's hospital and practices in a statewide medical home network. In this article, we summarize the preferred information sources, channels, and content needs of caregivers of children and youth with special healthcare needs during an infectious disease emergency. Nearly 84% of caregivers reported that they believe their child's doctor is the best source of information. Other preferred sources include medical experts (31%); the US Centers for Disease Control and Prevention (30%); friends, family, and neighbors (21%); and local or state health and emergency management (17%). Pediatric healthcare providers play an important role in providing information to parents and caregivers of children and youth with special healthcare needs during an infectious disease emergency. Public health agencies can establish health communication plans that integrate medical practices and other reliable sources to promote the dissemination of accurate information from trusted messengers.
Introduction
Nearly 20%
Methods
We used a convergent mixed methods design 19 in which both quantitative and qualitative data were collected during the same timeframe or study phase, then analyzed concurrently and compared to provide a more complete understanding of the information preferences of this population. The survey was intended to identify major trends in information-seeking preferences and practices. Interviews were conducted to further characterize the attitudes, beliefs, facilitators, and barriers that inform these preferences and practices. The research team created a survey and an interview guide in 2017 to collect information from parents and caregivers (also referred to as caregivers) of CYSHCN, and directly from young adults with special healthcare needs. Surveys and semistructured interviews were completed between April 2018 and June 2019. Respondents for each method were not mutually exclusive: interviewees may have also completed the survey, generally several weeks before the extended interview. The study was conducted in Pennsylvania and the Philadelphia metropolitan area, where the researchers are based.
The study was informed by the extended parallel process model, 20 which posits that the perception of the threat and personal sense of efficacy for recommended behaviors will drive protective action. Additionally, the crisis and emergency risk communication model reinforced the need to study caregivers with CYSHCN as an exigent population, at high risk for severe outcomes, and with different communication needs based on the stage of the event (eg, precrisis, initial response, recovery). 21 Finally, the World Health Organization's risk communication and community engagement framework supported the utility of exploring the information source and content needs of this vulnerable population for different emergency scenarios, including the potential role of the child's doctor as the preferred source. 22 We used these frameworks to create a conceptual model for disaster communications with CYSHCN caregivers (Figure 1) in which medical practices and trusted intermediaries provide information to CYSHCN caregivers during different emergency scenarios, through a variety of channels.
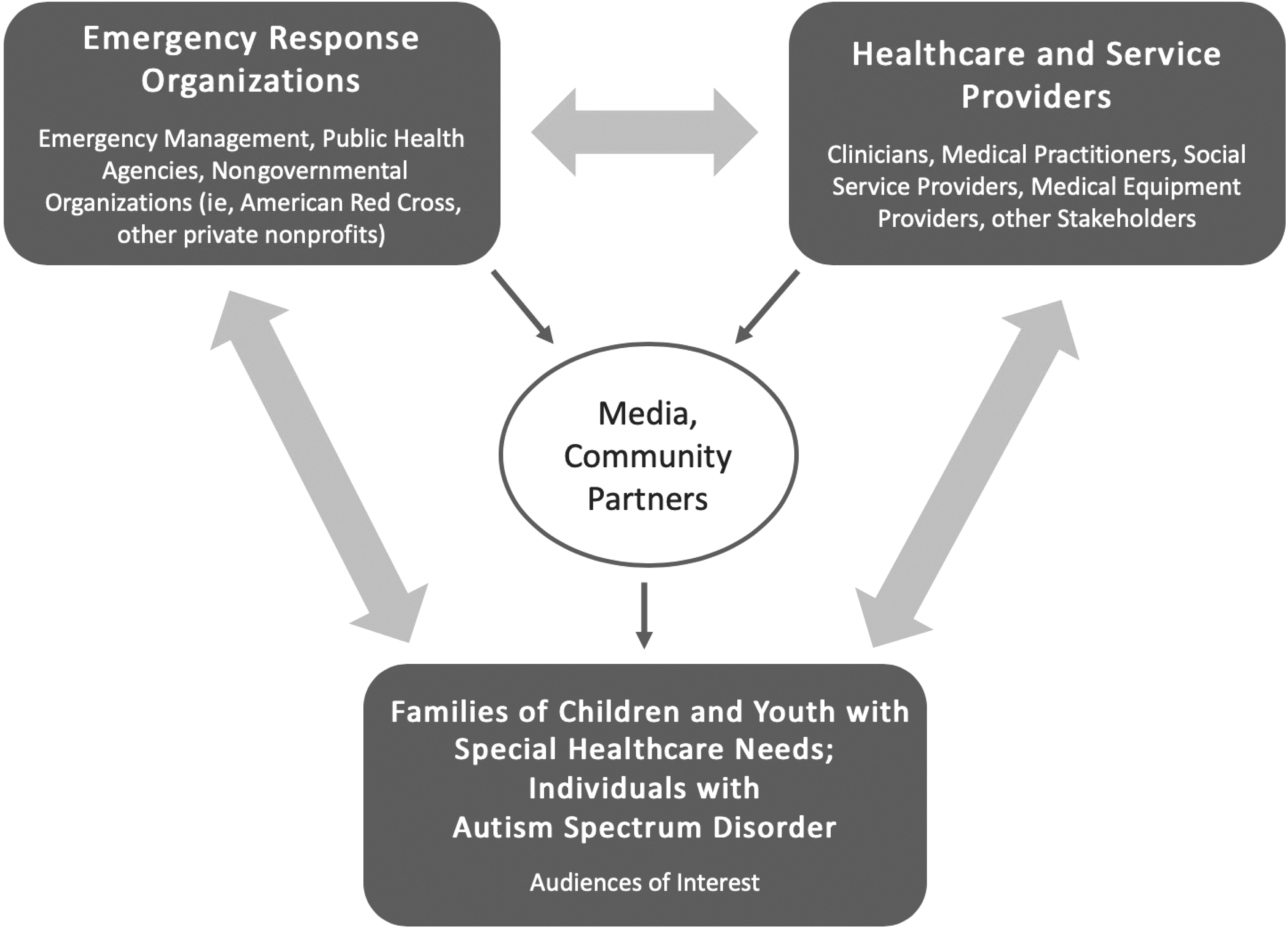
Conceptual model for disaster communications with caregivers of children and youth with special healthcare needs.
Survey
The survey contained questions on caregivers' sociodemographic characteristics, family preparedness for emergencies, practices for obtaining health information and information during potential emergencies, and communication preferences and needs during 3 different scenarios: severe storm, infectious disease outbreak, and a radiological event. These scenarios were chosen because they were either common events in the study location (ie, storm, outbreak) or rare radiological events (ie, accident, terrorism) that are relevant to residents of Pennsylvania, which is home to 5 reactors. Respondents were presented with questions containing between 6 and 14 options related to preferred sources, channels, and desired content, and asked to select their top 3 choices. A Likert scale was used to determine agreement with statements on risk perception and efficacy for specific threats. Data were stored in a Qualtrics (SAP, Provo, UT) database and analyzed using IBM SPSS Statistics version 24 (IBM Corp., Armonk, NY) for descriptive statistics and chi-square tests. Selected survey questions pertaining to information-seeking preferences, preparedness behavior, and perceived risk and efficacy were adapted from the National Survey of Disaster Experiences and Preparedness. 23 The survey was also reviewed by experts in risk communication and child health inside or outside of the US Centers for Disease Control and Prevention (CDC) (Vincent Covello, personal communication, May 6, 2017). It was piloted with 6 individuals, including 3 caregivers of CYSHCN who were not included in the final sample.
Interviews
The interview guide contained questions related to the sociodemographic characteristics of the caregiver as well as open-ended questions regarding family emergency preparedness and caregiver information-seeking behaviors related to disasters generally and for specific scenarios, focusing on the reasons for communication preferences and information needs. The guide also contained questions regarding the interviewee's use of social media and experiences in prior emergencies. Each interview covered at least 2 scenarios: a severe storm, and an infectious disease outbreak and/or a radiation emergency (ie, nuclear power plant accident). Of the 80 interviews, 77 addressed an infectious disease outbreak. Interviews lasted 45 to 60 minutes and were transcribed and analyzed using NVivo version 12 (QSR International, Burlington, MA). The research team developed a codebook corresponding to sections of the interview guide to capture emergent themes related to preferred content, channels, and sources for preparedness information and during a disaster, including specific concerns regarding an infectious disease threat and information needs pertaining to medical countermeasures. Five reviewers independently applied the codebook to a sample of 5 transcripts to ensure intercoder reliability (Cronbach alpha = .825), then coded the remaining transcripts.
Participants and Data Collection
Quantitative
We distributed the web-based survey via email to caregivers of CYSHCN receiving medical care from providers affiliated with the AJ Drexel Autism Institute in Philadelphia, Pennsylvania, and the Pennsylvania Medical Home Program (MHP) of the Pennsylvania Chapter, American Academy of Pediatrics. The MHP is a statewide practice network using the medical home model for pediatric care to serve CYSHCN and includes the Center for Children and Youth with Special Healthcare Needs at St. Christopher's Hospital for Children. We also distributed the web-based survey through listservs of caregiver organizations based in Pennsylvania. In addition, a convenience sample of caregivers completed hard copies of the survey during medical encounters for their children or during parent conferences held by MHP practices. Surveys were available in English and Spanish, the 2 most common languages spoken in the sample catchment area. A total of 297 people completed the survey.
Qualitative
A total of 80 people were recruited for interviews. These included 70 adults from the same convenience sample of parents and caregivers from MHP practices. Interviews were conducted separately, at a different time from the survey, either in person or via telephone, according to caregiver preference. The remaining 10 were young adults (ages 19 to 27 years) with special healthcare needs that we recruited to interview directly (ie, without caregivers), for the purpose of exploring the communication preferences of young adults who receive emergency information directly from sources. These interviewees were recruited from the AJ Drexel Autism Institute and the MHP practices. Eight of the 10 young adults had autism spectrum disorders (ASD) and attended school or worked outside the home but lived with parents. Two additional young adult interviewees had chronic medical conditions unrelated to ASD.
The interview sample was recruited to include a minimum of 20 caregivers of children with physical disabilities or reliance on assistive technology (including hearing and visual impairment), 20 caregivers of children with chronic medical conditions, and 40 caregivers of children with intellectual and/or developmental disabilities (10 minimum) and ASD specifically (30 minimum); the latter group was oversampled to optimize our ability to describe the information preferences of young adults with cognitive and communication challenges. The diagnostic categories were not mutually exclusive; children had multiple conditions in different categories. To complete analyses that we believed were most relevant for emergency planning for CYSHCN, we dichotomized these categories into 2 overarching, mutually exclusive groups: (1) physical disabilities and chronic illness and (2) intellectual/developmental disabilities and/or ASD.
The 10 young adults were included in these same diagnostic categories based on their medical conditions. Each interviewee (70 caregivers and 10 young adults) received a US$25 gift card. Six caregiver interviews were conducted in Spanish, transcribed into English, then reviewed again by a Spanish speaker to ensure transcript accuracy. Two caregiver interviews were conducted in Haitian Creole using a certified interpreter and transcribed into English; these were not reviewed again.
Ethical Considerations
The CDC sponsored this study. It was reviewed and approved by the Drexel University Institutional Review Board, Protocol Number 1705005423-R002. The CDC was not engaged in human subjects' research and relied on Drexel University's Institutional Review Board approval. All of the young adults were able to consent to interviews and their parents and caregivers consented to their participation.
Results
This article presents findings for an infectious disease scenario only. Responses for the storm and radiation scenarios focused on concerns regarding utility disruptions and general emergency preparedness and will be described in future articles.
Sample Demographics
Sociodemographic characteristics of people who participated in the survey and interviews are summarized in Table 1, with their child's or their own disability characterization. A total of 297 caregivers completed the survey: 113 (38%) of whom completed online surveys (the estimated response rate for online distribution was 6%, based on approximately 2,000 recipients combined) and 184 (62%) of whom were recruited by providers and completed paper surveys. Caregivers identified 19 different medical conditions that affect their children, which were mapped to the 2 overarching categories previously described. (See the footnotes in Table 1 for a list of reported conditions and how they were categorized.) Over half (56%) of the survey sample cared for children with both physical disabilities, or reliance on assistive technology, and intellectual/developmental disabilities. The mean age of the 10 young adult interviewees was 21.8 years (range 19 to 27 years).
Demographic Characteristics of Caregivers: Survey and Interviews
Survey respondents did not complete every question, so unique n values are provided for each item. Only caregivers completed survey.
Interview sample included 10 young adults; demographic data in this table includes these subjects, except for income categorization, which reflects household income.
Some families had more than 1 child with special health needs. Interview sample includes 10 adolescents/young adults who were interviewed directly.
Category includes: cerebral palsy, mobility challenges, respiratory disease (eg, bronchopulmonary dysplasia, any condition requiring supplemental oxygen), nutritional support needs (eg, feeding tubes), hearing impairment, and visual impairment.
Category includes: asthma, severe allergies, diabetes, epilepsy or seizures, sickle cell disease, any condition requiring daily medication for more than 6 months.
Category includes: intellectual or developmental disabilities, behavioral disorders (eg, attention deficit hyperactivity disorder), psychiatric conditions (eg, depression, anxiety, obsessive compulsive disorder), fragile x syndrome, Tourette's syndrome or tics, learning disability, speech or communication disability. Category was not mutually exclusive from autism spectrum disorders; caregivers could select both options.
Abbreviation: GED, general education development.
Parent and Caregiver Concerns
Nearly 55% of survey respondents strongly agreed or agreed that “a dangerous form of the flu that could lead to […] breathing problems” was likely to happen in their community within the next 5 years, and 79% of the respondents either strongly agreed or agreed that this scenario would be dangerous for their child. Only 36% (11.6% strongly agreed, 24.4% agreed) of respondents reported that their family was prepared for an event like this (Table 2). These answers did not differ significantly across disability categories.
Perceived Risk and Efficacy for an Infectious Disease Emergency, by Child's Medical Condition (N = 275)
Note: Respondents were presented with the hypothetical scenario: “There is an outbreak of infectious disease, such as a dangerous form of flu that could lead to pneumonia and breathing problems” and given 5 options: strongly agree, agree, neutral, disagree, strongly disagree. Strongly agree/agree and strongly disagree/disagree responses are combined in this table.
In interviews, many caregivers conveyed that an infectious disease event could exacerbate their child's vulnerability:
I think that probably scares me more than [a] storm […] my son has always had a very, very […] compromised immune system. I mean if you stare at him long enough, he will catch a cold.
My nightmare. […] She could die. I mean, it could take her from us. It's the most devastating problem.
Several caregivers expressed concerns about visitors to their home and indicated they would keep their child home during an infectious disease emergency, including avoiding their doctor's office:
So, he has respiratory issues, so that would obviously be our greatest concern. I think we would hunker down in the house and not let anybody in.
When it's virus season or flu season, I try not to make any appointments for her at all, because we have to go all the way over to the hospital. So, if it's an appointment that can wait until spring, I make it wait until spring, because I'd rather not expose her to anything.
Information Source and Channel Preferences
Survey participants were asked to select the sources they would trust most to provide them with information, as presented in Figure 2. Sixteen options were presented; nearly 84% of caregivers indicated that they would prefer to receive information from their child's physician during an infectious disease emergency. This preference was consistent across race/ethnicity, education level, income, English proficiency, and child's disability. Non-Hispanic White respondents were more likely than non-Hispanic Black or Hispanic respondents to identify CDC as a preferred source (38% vs 26% and 20%, respectively, P = .007) and English speakers were more likely than Spanish speakers to identify CDC as a preferred information source (31% vs 12%, P = .048). More non-Hispanic Black respondents listed family and friends as a preferred information source than Hispanic and non-Hispanic White respondents (32.7% vs 20% and 14.5%, respectively, P = .031). Caregivers with high school education or less were also more likely than those with higher education to seek information from family and friends (27% vs 16%, P = .026). Neither income nor disability type were associated with source preference.
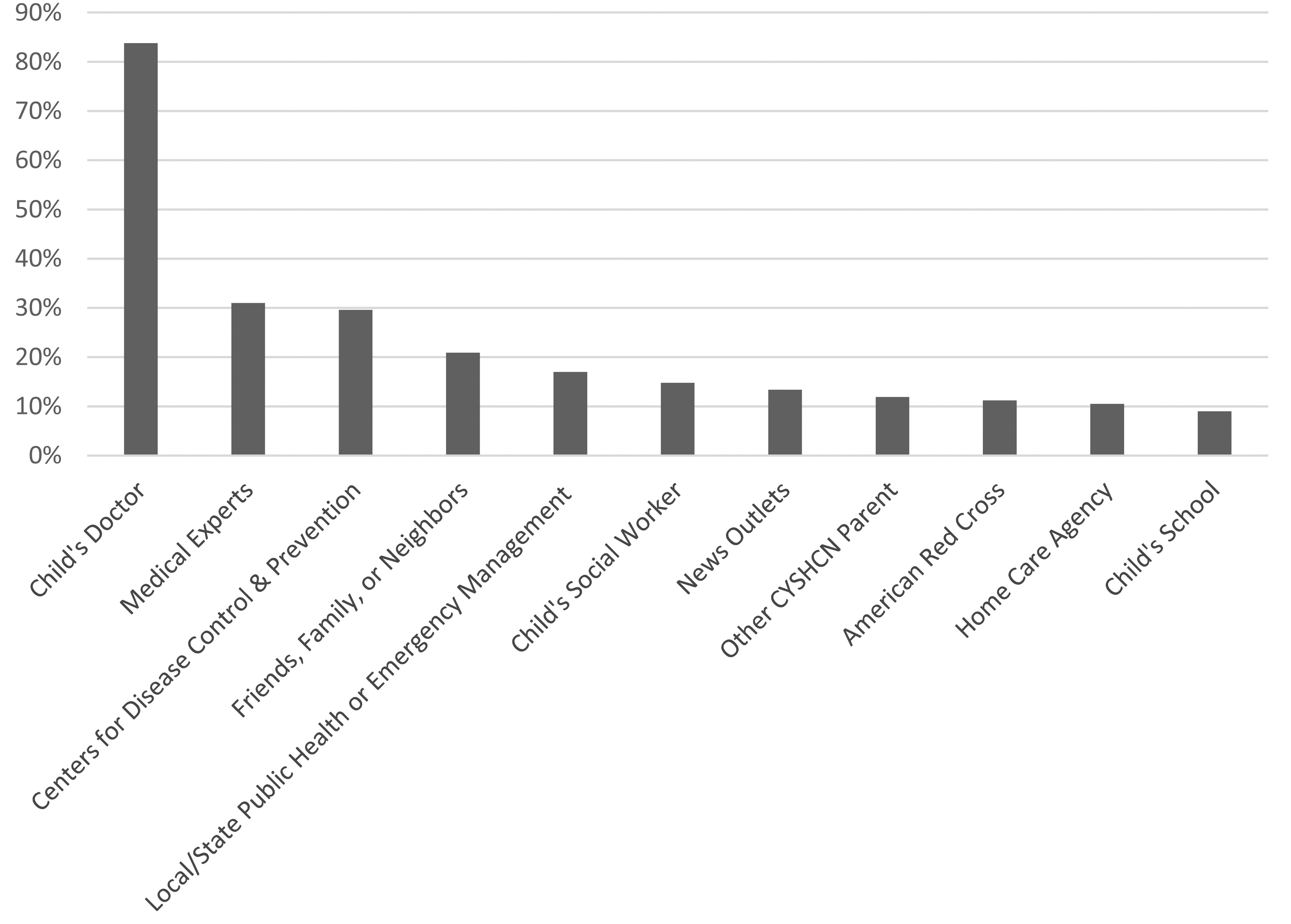
Preferred information sources in an infectious disease emergency for caregivers with children with special healthcare needs. “Who would you trust most to provide you with information about protecting the health of your child with special healthcare needs?” Percentage of caregivers who selected each source. The 277 respondents were presented with a total of 16 choices. The most frequently selected choices are presented in this figure. Additional available choices not depicted above that were selected by 5% or fewer of respondents include: child's emergency equipment provider, Federal Emergency Management Agency, place of worship, other, and autism advocacy organizations. Abbreviation: CYSHCN, children and youth with special healthcare needs.
Nearly all the caregivers interviewed reported their child's healthcare provider was their preferred information source. The primary reason was their familiarity with their child:
Definitely my healthcare team. […] I think that when you have a child or family member that has specific healthcare needs, you want to hear specifically how it will affect that person as opposed to the general population.
Several interviewees discussed how the desperation for information sometimes supersedes the importance of the source:
Well, in an emergency, I wouldn't care who it's from. The first one who gives me information, I'd look for it.
[I would want to get my information] probably from anybody. I don't have a specific person. […] Word travels very fast. So, if it's a professional that's one. But just regular people will share. They will do that.
The survey did not contain questions about communication channels used specifically in an infectious disease event. Survey respondents indicated they would use many different channels to obtain information during any emergency, including television (79%), radio (60%), websites via phone (57%), or websites via computer (41%). The majority (82%) used social media generally but less than half would use it during an emergency (46% use Facebook, 8% use Twitter).
In interviews, caregivers reported using multiple platforms concurrently to obtain information, including traditional media (eg, local news) and websites of the CDC, healthcare organizations, and professional societies. Social media was not frequently mentioned as a preferred way to obtain information in an infectious disease emergency, although several interviewees noted they use it in general to share information with their social networks.
My community has its own actual web pages on Facebook. They have their own community. I do go into that a lot as well, because word-of-mouth is very quick to let you know what's going on.
The caregivers emphasized their desire to speak directly with their child's healthcare provider via telephone, in person, or less frequently, through the patient portal in the electronic health record. Some interviewees expressed concerns regarding their ability to reach their doctor:
My hope would be that they would push information to us because it's not easy to call here. It's not easy to call our pediatrician at [medical institution], either. And I know that they would be busy, so I would hope that they would communicate it with us in some way.
The 10 young adults who were interviewed voiced similar communication preferences to adult caregivers, including their desire to communicate directly with their doctor or someone from their medical practice. They often relied on parents to share information (“My mom would be the first to know”), a finding especially common among the interviewees with ASD. Most used social media in general and thought it would be useful during emergencies but were unaware of government health accounts.
Content Needs
A total of 271 survey respondents answered the question: “What would you most want to know about a new medication to feel comfortable giving it to their child during an infectious disease emergency?” They indicated that they would want to know if their child's physician recommended it (69.7%), whether it was safe (69.0%), whether it was effective (54.6%), and if use of the medication would differ for children with health conditions compared with healthy children (30.3%). English-speaking caregivers were more likely than non-English speakers to want information about a drug's safety (72.0% vs 42.0%, P = .003). These preferences did not differ statistically by education, income strata, or child's disability category.
The majority of caregivers interviewed expressed concerns about their child's unique vulnerability during an infectious disease emergency, particularly children with physical disabilities and chronic medical conditions. They wanted information about specific protective measures for their child, what to do if they become ill, and guidance on when to keep their child home or seek care. All wanted information about risks and benefits of medications, side effects, contraindications, medication interactions, and how it helps their child. Three of the 80 interviewees expressed concern about vaccine safety; all were parents of children with ASD. The main interview themes are summarized in Table 3. Caregivers consistently cited the need for as much information as possible, and for information directly relevant to their child's medical needs. Non-English speakers expressed concerns that all the available information would not be translated into their preferred language.
Top Concerns of Caregivers With CYSHCN During Infectious Disease Emergencies – Interview Themes
Discussion
We believe this is the first study to explore communication preferences of parents and caregivers with CYSHCN related to an infectious disease outbreak. This study was completed 6 months before the global emergence of COVID-19. During the COVID-19 pandemic, families with CYSHCN expressed the need for better information, but there were few evidence-based practices to guide effective communication.18,24,25 The pandemic also disrupted healthcare access, education programs, and supportive services, creating additional challenges for CYSHCN.26-28
In this theoretical infectious disease emergency, caregivers and young adults with CYSHCN strongly preferred to receive information from their child's physician or medical practice compared with government agencies, medical experts, friends, or family. They used multiple communication channels concurrently to obtain information and used social media to exchange information with friends and family, including other parents with CYSHCN, consistent with prior research. 29 Earlier studies in this population, including during the 2009 H1N1 influenza pandemic, highlighted the importance of conveying tailored information for families with CYSHCN and their unique vulnerabilities, and the important role of the pediatric practice to assist with community planning, share public health recommendations, and communicate with patients.3-5,30-32
Our findings also align with a prior review of successful risk communication during disasters, which identified the importance of risk perception, targeted messages for vulnerable populations, and community engagement. 33 Most caregivers in this study believed a major infectious disease outbreak was likely to happen in their community, it would be dangerous for their child, and they did not feel prepared if such an event were to occur. Moreover, caregivers expressed that they would want to know more about physician endorsement and safety and effectiveness before administering a new medical intervention to their child. They wanted information specific to their child's condition. Caregivers also expressed a reluctance to seek nonessential medical care and services. This concern became evident during the COVID-19 pandemic, when routine childhood vaccination rates and medical visits declined for all children.
Our study population overall was racially and ethnically diverse, with Hispanic and Black populations proportionally overrepresented compared with the overall US population, but similar to the demographics of CYSHCN. The sample reflects the large proportion of study participants from the area of Philadelphia near St. Christopher's Hospital for Children, which has a high proportion of Black and Hispanic individuals, and where 40% of children live in poverty. In this study, non-Hispanic White individuals were more likely to prefer to receive information from the CDC, while non-Hispanic Black individuals were more likely to prefer information from friends and family. Our findings are consistent with other studies of effective risk communication involving vulnerable populations, which have identified the importance of clear communications from trusted sources, 34 and the value of community relationships in both effective communication and preparedness, particularly among low-income or ethnic communities with limited English proficiency.35-38 Others have identified a potential role for technology to support effective risk communication with culturally and linguistically diverse communities in disaster response, focusing on appropriate communication that addresses trust and message tailoring, which may explain our findings as well. 39
Prior studies of disaster vulnerability among children with disabilities have highlighted the contribution of social vulnerability to disaster risk, and the importance of the complex intersections of social characteristics, physical vulnerabilities, and psychological vulnerabilities that augment this risk.40-42 Children with disabilities are more likely to live in poverty and to live in lower-quality housing that is more vulnerable to disasters. Their physical and cognitive impairments require more timely warnings to take health protective measures, and inclusion in emergency preparedness planning to ensure that their disability-related needs are met during a disaster response.43,44 CYSHCN have inequities in health and healthcare access, especially children with medical complexity, although this is associated primarily with their significant medical needs as opposed to income status and race/ethnicity. 45 Additional research is needed on larger populations of CYSHCN across the complexity spectrum to examine the influences of social factors and underlying medical conditions on information needs and preferences. In the United States, Hispanic, non-Hispanic Black, non-Hispanic American Indian and Alaskan Native, and socially disadvantaged children have had the highest burden of pediatric COVID-19 infection, including severe disease and death.46-49 This disproportionate impact reinforces the need to engage all communities effectively during infectious disease emergencies to mitigate risk, improve health outcomes, and promote health equity. 50
Our study had several limitations. The online survey had a low response rate; two-thirds of the respondents were a convenience sample of caregivers who completed the survey during healthcare encounters or forums for parents. They were highly engaged in healthcare and perhaps especially concerned about an emergency's impact on their child. Over half of our survey respondents and 30% of interviewees had children with both physical and intellectual disabilities. They had more medical conditions than a recent national cross-section of CYSHCN in which 11% of caregivers reported their child had 2 or more functional difficulties.
51
Our samples were more representative of children with medical complexity, a recognized subset of CYSHCN with multiple substantial chronic health problems affecting multiple organ systems, resulting in functional limitations and high healthcare utilization.
52
This medical complexity may explain the reliance on physicians for health information. Because most caregivers in our sample had children with multiple coexisting conditions, we had limited ability to identify differences in caregiver communication needs based on a child's disability, such as children with ASD. Additionally, both the survey and interview guide were used for the first time in this study and were not well validated. However, few instruments exist for studying disaster communication needs of this specific population. Our study objectives were to provide an initial description of the information-seeking behaviors and preferences of this understudied population and to provide both tools and data for future studies. Findings from this study are relevant for health communications during any infectious disease outbreak, including emergent infectious diseases, and support the following actions:
Medical practices can prepare to share information early in an emergency, explain information disseminated from other sources, and address misinformation. This is especially important because providers were the most trusted information source in this study and have a unique role in communicating with families. Medical practices can provide caregivers of CYSHCN with information tailored for their child's specific health conditions. Practices should prepare families before emergencies and plan effective processes for communication to reach them early and rapidly. Young adults, especially those with intellectual disabilities, rely on parents and caregivers for medical information but also prefer to receive direct messaging from their providers. Practices can communicate with parents about when to keep their child home and when to seek medical care. Fears of contagion may result in missed appointments and less utilization of home health support or routine health services, including immunizations. Community engagement with friends and family members of CYSHCN is important when communicating public health emergency information to historically marginalized groups, specifically racial and ethnic minorities. Risk communication researchers and government agencies such as the CDC should study ways to increase confidence among these groups when delivering health messages.
Conclusion
Pediatricians and other professionals in pediatric practices are an important source of information for families with CYSHCN during an infectious disease emergency. Public health agencies can establish health communication plans that integrate medical practices and other reliable sources to promote the dissemination of accurate information from trusted messengers.
Footnotes
Acknowledgments
This study was supported by CDC contract #200-2016-92427. We are grateful to the families and providers of the Pennsylvania Medical Home Project of the PA Chapter, American Academy of Pediatrics, for sharing their time and their perspectives. We thank Ms. Eileen Thompson, director of the Medical Home Program, and Ms. Suzanne Yunghans for their guidance in conceptualizing this project and recruiting focus group participants, and Dr. Jennifer Plumb and Gabriella Grimaldi for their assistance with data collection and analysis. The findings and conclusions in this article are those of the authors and do not necessarily represent the official position of the CDC. Use of trade names and commercial sources is for identification only and does not imply endorsement by CDC, the US Public Health Service, or the US Department of Health and Human Services.