
Abstract
Early in the COVID-19 pandemic, substantial disruptions in personal protective equipment (PPE) supply chains forced healthcare systems to become resourceful to ensure PPE availability for healthcare workers. Most worrisome was the global shortage of N95 respirators. In response, a collaboration between the Department of Infection Control and Healthcare Epidemiology and the Department of Biosafety at the University of Texas Medical Branch developed a PPE recycling program guaranteeing an adequate supply of respirators for frontline staff. The team successfully developed and implemented a novel workflow that included validated decontamination procedures, education, and training programs as well as transportation, labeling, and storage logistics. In total, 15,995 respirators of various types and sizes were received for recycling. Of these, 12,752 (80%) were recycled. Following the program's implementation, we surveyed 134 frontline healthcare workers who overwhelmingly graded our institution's culture of safety positively. Overall impressions of the N95 respirator recycling program were mixed, although interpretation of those results was limited by a lower survey response rate. In an era of increasing health security threats, innovative recycling programs like this one may serve as a model for other health systems to respond to future PPE supply chain disruptions.
Introduction
COVID-19, first identified in December 2019 and declared a pandemic in March 2020, is classically characterized by fever, chills, cough, and shortness of breath. 1 In some, the disease progresses to profound hypoxia and a hyperinflammatory respiratory distress syndrome requiring respiratory support. 2 Despite impressive scientific advancements in diagnostics, therapeutics, and vaccine development, the COVID-19 pandemic continues as the emergence of more contagious variants, such as Delta and Omicron, propagate the spread of the disease. 3
SARS-CoV-2, the betacoronavirus that causes COVID-19, is primarily transmitted via respiratory droplets and aerosols. N95 respirators are thus essential personal protective equipment (PPE) for healthcare workers (HCWs) caring for COVID-19 patients. N95 respirators are designed to filter at least 95% of non-oil aerosolized particulates, typically those less than 5 μm in diameter. These aerosols can remain suspended in the air for extended periods of time, allowing them to disperse further distances than respiratory droplets. 4 In the United States, like other countries across the world, SARS-CoV-2 put an unprecedented strain on healthcare systems and medical supply chains. Early in the pandemic, many suppliers could not meet the demand for N95 respirators, leading healthcare institutions to consider innovative ways to safely reuse PPE.
At the University of Texas Medical Branch (UTMB), PPE acquisition discussions began before the first diagnosed COVID-19 case. As cases increased, however, our supply chain became severely restricted. With limited possibilities to procure new PPE, additional sources included our institution's personal stock of pandemic PPE supplies and the Strategic National Stockpile. N95 respirators in our pandemic supply were minimal and nearing expiration and the Strategic National Stockpile was limited due to many healthcare institutions requesting PPE distributions simultaneously. Given the limited product availability, the UTMB supply chain reached out to the Department of Infection Control and Healthcare Epidemiology (ICHE), who in return collaborated with the Department of Biosafety (DOB) and Occupational Safety to review PPE purchases before distribution throughout the healthcare system. We received several types of respirators that required frequent up-to-date fit testing of staff, which further strained operations. To lessen this stress and maintain supply, ICHE and DOB began to investigate novel and safe ways to recycle eye protection (not described in this article) and N95 respirators. 5
UTMB is a large academic tertiary healthcare system and research enterprise composed of 959 inpatient beds, 88 ambulatory clinics, and 275 research laboratories. 6 The institution has a close relationship with a high and maximum containment infectious diseases research facility funded by the National Institute of Allergy and Infectious Diseases. Because of this, we have expert knowledge in various decontamination and sterilization methods. Through innovative collaboration between the infection control and biosafety departments, our institution bridged its clinical and research enterprises to create a successful N95 respirator recycling program. The common goals of each department in reducing occupational exposures and infections enabled a quick and effective partnership to form. By combining resources, we were able to respond to one of the worst PPE crises of our time and deliver safe and uninterrupted patient care. Herein we describe our program including the strengths and challenges faced, the decontamination process, and responses from HCWs who used recycled respirators.
Methods
N95 Decontamination Studies
To determine decontamination methods for validation, DOB staff acquired a sample of each respirator model currently in use by HCWs. The 3M 1860/1860S, 3M VFlex 1805/1805S, Prestige Ameritech RP88020, and 3M 1870/1870+ were identified as low stock but high-use respirators. Two different decontamination methods were tested for each respirator model: vapor-phase hydrogen peroxide (VPHP) and moist heat. All validation testing and decontamination cycles were performed in-house by DOB staff.
For each study, the respirators were subjected to multiple decontamination cycles of a single method and assessed for point-of-failure, if reached. The following methods were used to assess respirator integrity and overall fit for reuse of each respirator model: biological spores, chemical integrators, filtration efficiency, breathability, fit testing, and strap integrity testing.
Biological and Chemical Validation
The decontamination systems were validated using both Geobacillus stearothermophilus biological spore indicators (BI) (3M and Mesa Labs) and Comply SteriGage Steam Chemical Integrators (CI) (3M).

N95 decontamination validation studies. (A) Penetrations were made within the material layers of the N95, and a biological indicator was placed between the different material layers to demonstrate penetration of the vapor-phase hydrogen peroxide through the layers. (B) The arrows demonstrate where the biological indicators are placed. The penetration on the front of the N95 was closed after biological indicator placement to ensure the vapor-phase hydrogen peroxide penetrated through the material. (C) Initial vapor-phase hydrogen peroxide cycles were validated using a sealed testing chamber. (D) Chemical integrators were placed within the N95 folds, singly bagged (in either Steriking or Kraft pouches/bags), and placed in the autoclave with an 3M Attest Super Rapid 5 Steam-Plus Challenge Pack. Autoclave bins were used to contain and keep the bags upright during the autoclaving cycle.
Fit Testing
Quantitative fit testing was performed using volunteers from the recycling team using a PortaCount Respirator Fit Tester 8030 (TSI) following established fit-testing methods outlined by the National Institute for Occupational Safety and Health (NIOSH). 7 A fit factor of at least 100 was a passing result. More than 1 individual participated in the fit testing to account for variance between individuals. All respirator models outlined in the decontamination studies were subject to fit-testing postdecontamination procedures. Each respirator model was tested in triplicate by decontamination method and fit testing.
Filtration Efficiency
Particle counting was conducted using an AeroTrak Portable Particle Counter 9110 (TSI Incorporated, Shoreview, MN) with an attached customized flange setup. Depending on the respirator model, either 1 (folded respirator) or 2 (molded respirator) sites were measured on the respirators to acquire particle count readings compared with unprocessed respirator controls as previously described. 8
Strap Integrity Testing
Respirator strap elasticity and integrity was assessed by physically pulling the strap and evaluating its ability to recoil after each decontamination cycle. These assessments were considered in each validation study. Although it has been reported that respirators may be able to sustain over 50 VPHP decontamination cycles successfully, we observed structural integrity issues and decided to be conservative with our approach; therefore, a maximum of 10 decontamination VPHP cycles was selected.8,9
Clinical Setting Logistics
Healthcare Worker Education and Training
After specific respirator models were identified for recycling, ICHE and DOB developed materials focused on HCW education and logistics for staff performing reprocessing. Process flows were established for clinical staff, Environmental Services, couriers, and Occupational Safety. Together, these materials discussed safe doffing of PPE, packaging of used respirators, transporting bins of used respirators to a central location for processing, and labeling the recycled respirators for redistribution. These materials together with the decontamination processes previously discussed created the N95 recycling program.
ICHE and DOB staff trained all HCWs in proper donning, doffing, and point-of-use collection for PPE recycling. Signage and a training video detailing the recycling process educated additional staff quickly and reinforced the education provided during in-person trainings, such as during daily nursing huddles. 10 The workflow for HCWs was mapped out to achieve optimal recycling of respirators at the end of patient care.
PPE Doffing Stations
Collection bins were placed at point-of-use stations within medical units caring for COVID-19 patients. Signage was placed inside and outside of patient rooms for HCWs to correctly don and doff PPE (Figures 2A and 2B). After completing patient care, HCWs removed used PPE and placed the items into corresponding bins for respirators, eye protection, and trash (Figures 2C and 2D).

Personal protective equipment and doffing station signage. (A, B) Visual donning and doffing instructions were created and posted in each patient room. (C, D) Doffing stations located in common areas outside of the patient rooms. Modular signage was created to enable flexibility in the recycling program and effective communication to healthcare workers. The signage displayed which N95 models were being collected for recycling and which models should be discarded in the waste bin. This enabled us to adjust our recycling efforts based on institutional needs throughout the pandemic.
Solid, nonporous plastic 5-gallon collection bins were used to enable safe and easy transport and disinfection at the decontamination site. In addition to proper PPE donning and doffing, HCWs assigned a point person to track PPE usage on the unit and ensure trash was not placed in either the respirator or eye protection bins. Additionally, the point person was instructed to contact Environmental Services for early pickup if a bin was full before its designated pickup time.
Courier Logistics
Inpatient Unit and Ambulatory Clinic Locations
Environmental Services gathered used inpatient respirator bins daily and delivered them to a central location for processing. Once the bins were brought to the central processing location, used respirators were placed in 30-gallon drums labeled for recycling. In the ambulatory locations, the same collection bins were used. The sealed bins were placed in the soiled utility room until pickup. The health system courier gathered the bins and delivered them to the fleet area for pickup. The courier staff would also deliver clean 5-gallon bins to the ambulatory sites to replace the used collection bins.
Transport Logistics to the High-Containment Facility
Environmental Protection Management, a department that handles hazardous waste on campus, collected the used respirators from both the inpatient and ambulatory clinic drop-off locations and delivered them to the high-containment facility weekly, or more often depending on the amount of recycled PPE. Clearly labeled areas were created for used respirator drop-off and recycled respirator pickup for redistribution in the high-containment facility dock.
Decontamination Logistics
N95 Respirator Prepping
DOB staff transported the used respirator drums (Figure 3A) to a biosafety level 3 laboratory for sorting and decontamination. A biosafety level 3 laboratory was used because of the VPHP decontamination process. For sorting and decontamination, DOB staff wore facility-dedicated scrubs and shoes, gowns, double gloves, and powered air-purifying respirators.

Decontamination preparation and setup. (A) Used N95 drums were delivered in clearly labeled and sealed 30-gallon drums. (B) An example of a damaged Prestige Ameritech N95 that is not suitable for decontamination. Red arrows indicate areas of compromised seams on the N95 after healthcare worker use. (C) A makeup-soiled N95 example; this category of soiled N95s was segregated from the other N95s during the decontamination process and recorded separately on the inventory management sheet to assist with retraining of healthcare workers. (D, E) Example of a vapor-phase hydrogen peroxide setup, in which a large room was outfitted with large storage racks; clips or hooks were used to hang the N95s for decontamination or placed flat on a nonsolid surface to enable air circulation around the N95. (F) N95s decontaminated using moist-heat autoclaving were sorted and bagged in the biosafety level 3 room and then processed in the facility-dedicated autoclave.
Used respirators were sorted by model and size. Respirators soiled with anything other than makeup, or those torn, damaged, with a distinct loss in elasticity, or unable to hold form (molded respirators) were considered unsuitable for decontamination and discarded (Figures 3B and 3C). Details of all respirators received for processing were recorded and shared in real time with ICHE and the institution's internal supply chain.
Decontamination Setup
For VPHP, used respirators were carefully hung on stainless steel racks using metal clips or hooks. The respirators were hung or placed flat on a nonsolid surface in a manner as to not overlap to ensure the VPHP could circulate around each respirator (Figures 3D and 3E). For moist heat, used respirators were packaged individually and autoclaved using the autoclave cycle processes previously described (Figure 3E). 8
Repackaging, Labeling, and Inventory Management
After PPE was decontaminated and the room was considered safe for entry (less than 1 ppm hydrogen peroxide), each recycled respirator was marked with a dot to track the number of times it was decontaminated (Figures 4A and 4B). The respirators were again sorted by model and size and repackaged in the same quantity as the original manufacturer. This packaging process was intentional to make it easy for the supply chain to fill purchasing orders without changing how the inventory is accounted for in the system.
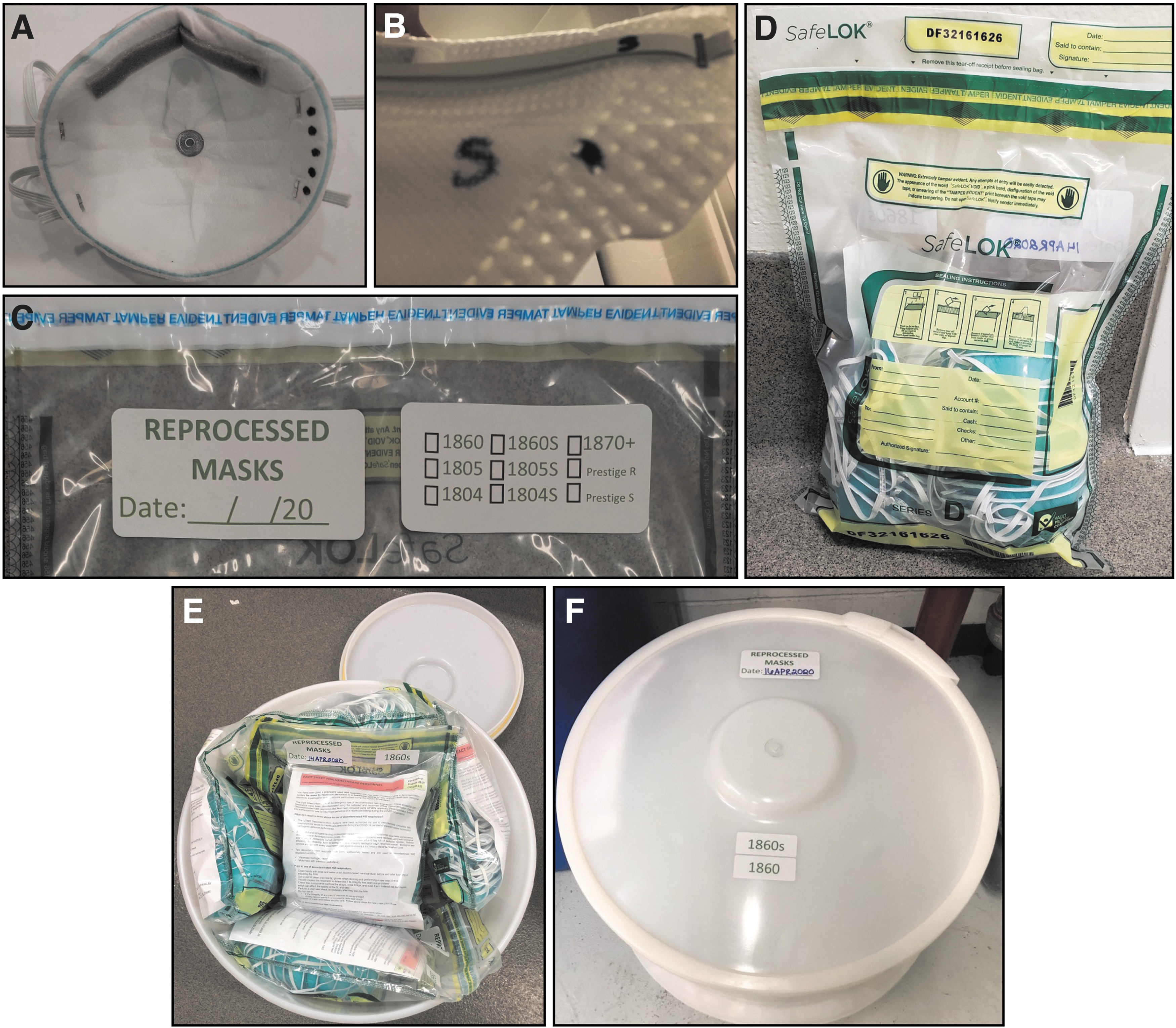
Marking, packaging, and labeling. (A) After each decontamination cycle, N95s were marked with a dot to track the number of times an N95 was decontaminated. (B) For N95s (eg, 3M 1805/1805S) that experienced fading of sizing information (for models that have different sizes), the size was marked on both the bill and strap to ensure the healthcare worker could confirm the size of the N95. (C) Decontaminated N95s were sorted by model and size and packaged within tamperproof sealed bags. (D, E, F) Sealed bags were labeled, packed into white drums, and transported to the supply chain warehouse.
Recycled respirators were repackaged in clear, tamperproof deposit bags (SafeLOK, Wigan, UK) with a fact sheet informing HCWs about the reuse of respirators, how the decontamination process was performed using an institution-approved process, and that the respirators were authorized for use by HCWs in a healthcare setting during the COVID-19 pandemic. This document also provided instructions on how to inspect and use the recycled respirator. A label was created to document the date of decontamination and mark the respective respirator model and size on each packaged bag of recycled respirators (Figures 4C, 4D, and 4E). Finally, the repackaged respirators were placed in clean drums of a different size and color than those containing used respirators, then sealed and labeled to indicate that recycled respirators were inside (Figure 4F). These drums were picked up by high-containment facility staff and delivered to the supply chain warehouse for redistribution within the healthcare system. On average, once the respirators were sorted and set up for decontamination, the average turnaround time for repackaging for VPHP was 24 hours given off-gassing and less than 12 hours for moist heat. Our team tracked the process using a shared database that included tracking times, effort spent recycling, and the number of respirators discarded or found unsuitable for recycling. The database also aided in prioritizing recycling efforts based on available respirator models and sizes. This helped direct DOB and Occupational Safety on which employees needed to be fit tested for a different respirator model when inventory volumes were low.
Healthcare Worker Survey Evaluating Perceptions of the Recycling Program
We developed a simple survey tool using an ordinal scale to gauge frontline HCW perceptions of the recycling program. A frontline HCW was defined as any person with direct patient care responsibilities. Survey categories of HCWs included physicians, nurses, and allied health professionals. The physician category included residents, fellows, and faculty members. “Allied health professionals” included fields such as physical therapists, occupational therapists, respiratory therapists, and patient care technicians. The survey evaluated 4 domains: training and education, safety, logistics, and healthcare worker emotional response. Nonbinary responses were graded on an ordinal scale from 1 (lowest) to 5 (highest), then divided into “lower” (1 and 2) and “higher” (3 to 5) categories. All responses were anonymous. Nonordinal scale, open-ended comment options were used for the emotional category. Comment areas were also available in each category to provide greater detail about respondent experiences. This study was approved by the University of Texas Medical Branch Institutional Review Board (approval IRB#21-0205).
Results
N95 Recycling Program
Between April and September 2020, 15,995 N95 respirators were collected via the recycling program. The program successfully recycled 12,752 (80%) respirators, deeming 3,243 (20%) unfit for recycling. A breakdown of our recycling program efforts by respirator model and size can be found in Table 1.
Total Number of N95s Received and Decontaminated for Reuse
Our decontamination processes (moist heat and VPHP) successfully demonstrated the respirators met acceptable performance standards even after multiple decontamination cycles both in our studies and as previously published.8,9 For VPHP, although it has been reported that respirators may be able to sustain over 50 VPHP decontamination cycles successfully, we observed structural integrity issues and decided to be conservative with our approach; therefore, a maximum of 10 VPHP decontamination cycles was selected for our recycling program. 9 Overall, all respirator models tested tolerated VPHP decontamination and were ultimately validated for up to 10 decontamination cycles at our institution.
For moist heat, our validation studies concluded that the molded style respirators (eg, 3M 1860/1860S) do not withstand this decontamination process. However, the folded style respirators (eg, 3M VFlex 1805, 3M 1870/1870+) can withstand moist heat decontamination for up to 3 decontamination cycles before performance standards are affected. 8
A large majority of the nonrecycled respirators discarded after 1 use were inventory stocks that had been in our institution's emergency pandemic supplies the longest. Foam degradation after single use of the 3M 1860/1860S models accounted for most of this model's inability to withstand recycling, thus these respirators were also excluded from recycling. In addition, while we were able to successfully validate the decontamination processes on the Prestige Ameritech respirators, issues with predecontamination strap integrity led us to abort efforts on recycling these respirators (Figure 3B1).
Healthcare Worker Survey Evaluating Perceptions of the Recycling Program
A total of 185 frontline HCWs responded to the survey, 134 (72%) of whom reported their occupation and that they had direct patient care responsibilities. Over half (n = 70, 52%) of those respondents were nurses. Overall, most (n = 117, 87%) respondents felt they were provided the resources they needed to safely perform their job duties. They also endorsed a high sense of institutional dedication to their safety, with 85% (n = 114) responding “expected” or greater. These findings correlate well with HCW impressions of PPE adequacy, with 86% (n = 116) responding with “expected” or greater. Importantly, an overwhelming majority of HCWs (n = 123, 92%) felt there was high-level institutional commitment to patient safety as well. Safety results are summarized in Table 2.
Rating of Safety in the Hospital
A total of 134 respondents reported their occupation and indicated that they had direct patient care responsibilities. The percentages in the occupation columns are calculated using the occupation denominator.
General impressions of the recycling program were mixed (Figure 5). Of the 134 respondents who responded to a question about the program's existence, a slight majority (n = 69, 52%) reported being unaware of the program's existence, with the lowest awareness (n = 16, 12%) among physicians. Among the health professions, nurses were most likely to be aware of the program (n = 39, 29%) followed by allied health professionals (n = 16, 12%). Only 49% (n = 65) of HCWs rated their confidence in the recycling program (Figure 6). Of those, about half (n = 34, 52%) reported lower confidence, with the lowest confidence reported among nurses (n = 24, 37%). Allied health professionals had the highest reporting of confidence (n = 10, 15%), followed by physicians (n = 6, 9%).
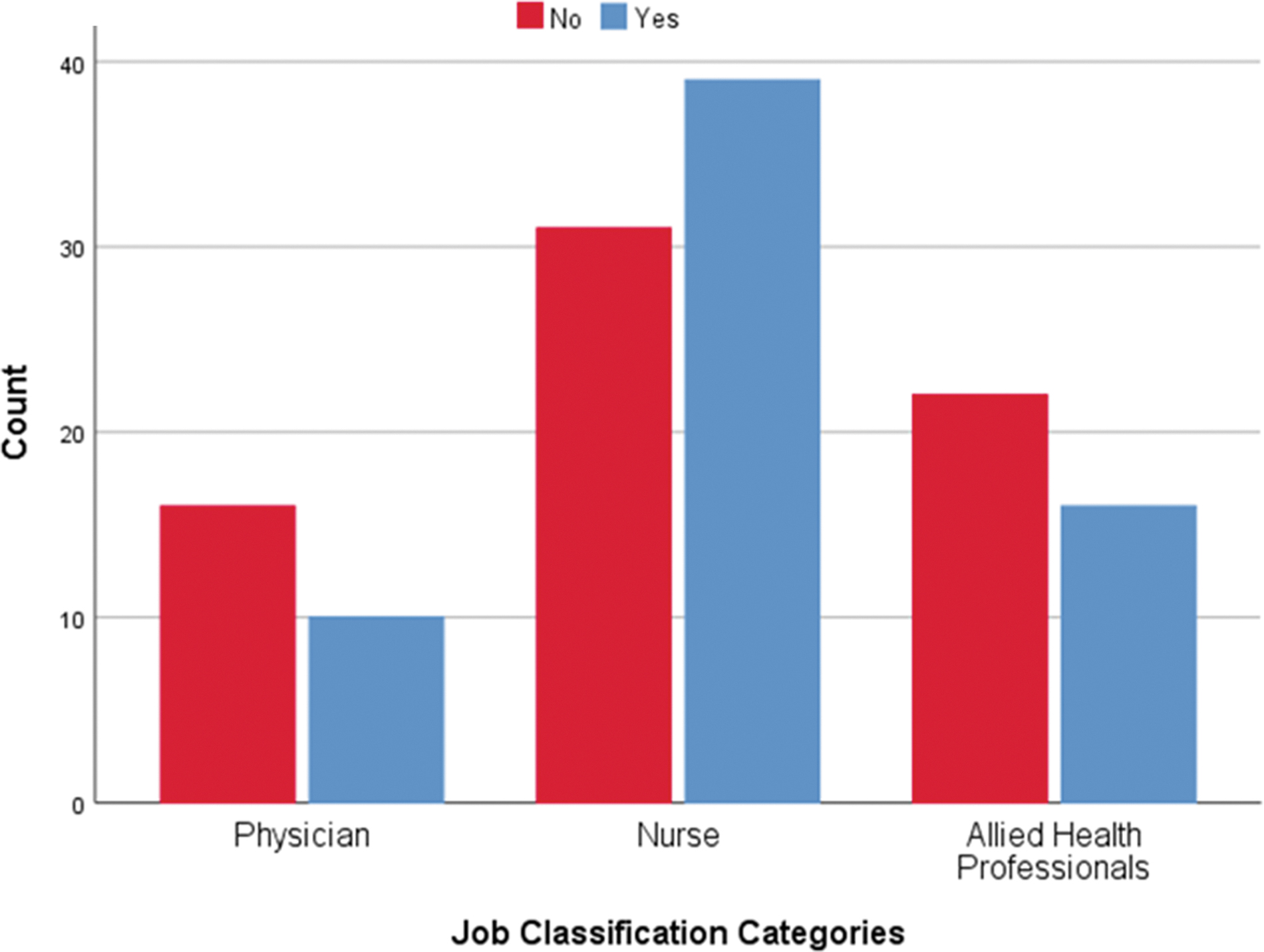
Awareness of N95 recycling program by profession.
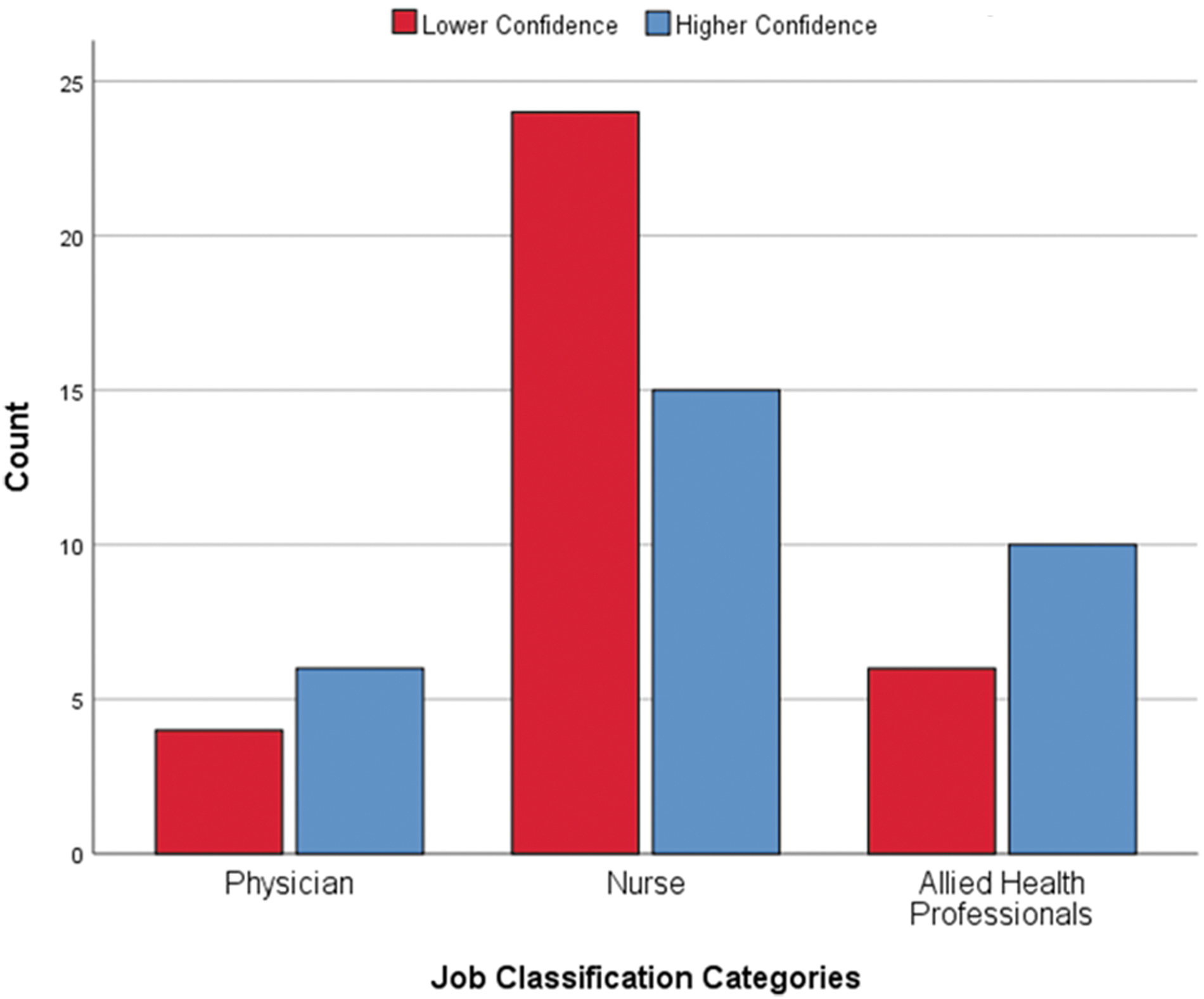
Confidence in N95 recycling program by profession.
Informal feedback from HCWs was solicited at DOB unit rounds, during which HCWs expressed appreciation for the implementation of tamperproof bags, fact sheets, and the labeling system. They also appreciated the chain of custody procedures, which offered a way to confirm that the recycled respirators had not been tampered with between the decontamination and redistribution processes.
Discussion
Our institution responded to an extraordinary PPE shortage by successfully designing and implementing an efficient, high-throughput, high-quality N95 respirator recycling program. This program enabled the institution to address supply chain issues in an efficient manner without sacrificing HCW safety. Our program also created a platform for new forms of interdepartmental collaboration. This project brought our institution's infection control and biosafety teams together to form an interprofessional Infection Control and Biosafety Team. This highly collaborative and action-oriented team has already begun to develop policies, procedures, and training materials that will help our institution prepare for future emerging or special pathogen outbreaks that may lie ahead. The decontamination process and logistical implementation of the program provided many opportunities for adaptive learning, the details of which are explored as follows.
First, decontamination methods were chosen based on ease of operation and systems available. While VPHP requires specialized equipment, expertise, and training, we selected a second method that could easily be deployed to any healthcare setting that had moist heat autoclaves available if the DOB staff were unable to keep up with recycling demand. A 3-person DOB team was dedicated to the recycling program. While it may have been more challenging performing 2 different decontamination methods, both decontaminations were performed in the same biocontainment facility, which greatly reduced DOB staff burden. Further, operating the decontamination methods simultaneously increased efficiency and turnover of recycled respirators back in circulation for HCWs.
Our methods for validating 2 decontamination systems with both a BI (demonstrates a 6-log kill of bacterial spores) and CI (class 5) was to ensure that both methods were capable of inactivating not only SARS-CoV-2 but any normal bacterial flora that could pose hygiene concerns between wearers. This was important in our validation studies because all recycled respirators were deposited into the main inventory circulation and were not returned to the original wearer.
Additionally, during the recycling efforts DOB staff were able to communicate in real time with ICHE about any issues that arose, which enabled targeted retraining. Because the bins were labeled with campus origin, targeted communication was possible. Feedback was provided by ICHE to the HCWs of respirators successfully recycled, as well as areas needing improvement in collection (eg, trash in collection bins dedicated to respirators). In addition to unit point persons, ICHE conducted frequent PPE rounds to monitor each unit's PPE recycling processes.
We made several changes to our processes as we learned in real time and received HCW feedback on the overall recycling program. Almost immediately after launching the program, we switched the types of bags used for autoclaving from kraft paper bags to open Steriking bags. The paper bags were too cumbersome for HCWs to package, fold, and place in the recycling bins. Therefore, to make the process easier, HCWs were instructed to deposit their respirators directly into the recycling bins and then DOB staff would prepare the respirators for autoclaving. This change in process enabled DOB to inspect the respirators before recycling to ensure damaged respirators were not placed back into circulation and prevented overuse of resources on damaged respirators.
One of our biggest challenges, and targeted areas for retraining, was the soiling of used respirators due to makeup. ICHE used different methods of communication to target HCWs regarding the use of makeup while wearing respirators. Over time, the number of soiled respirators declined as communications were reinforced during shift huddles and systemwide emails.
Through trial and error, we learned that certain marker colors used for our “dot” tracking—to track the number of times respirators were decontaminated—faded more easily than others. Blue pigment markers were the least reliable. Fading occurred for a variety of reasons including autoclaving or wearer perspiration. We also had the additional challenge of high-heat autoclave cycles, which severely faded the manufacturer information printed on the respirators (eg, size, make, model). To compensate for the fading, we used black pigment markers to notate the respirator size on both the strap and front of the respirator (Figure 4B). We recognize writing on respirator material is not recommended by the NIOSH National Personal Protective Technology Laboratory; however, given the circumstances we chose to do so to ensure we could track the reuse times.
Survey results from frontline HCWs demonstrated that our institution successfully created a culture of safety during a time of extreme stress and uncertainty. Commitment to both HCWs and patient safety were perceived favorably, with high levels of confidence in the quality of PPE. While the performance characteristics of the recycling program were excellent, feedback was mixed. Despite a comprehensive internal and external communication strategy, many frontline HCWs were not aware of the program. Some HCWs, especially nurses, expressed lower levels of confidence in the recycled PPE. Physicians and allied health professionals, while generally less aware of the program, reported higher confidence in the recycled products.
Given the relatively small number of respondents, it is difficult to draw concrete conclusions from the survey data. However, several lessons can be learned. First, HCWs must be made aware of the benefits of a recycling program and the quality of the recycled materials. Second, hospital leadership must mainstream communications in a manner that inspires confidence in the program. Third, to improve perceptions of a recycling program, institutions should consider the feasibility of tracking the PPE usage of each HCW and returning recycled PPE back to the individual user. Finally, continued quality improvement and feedback from HCWs should be solicited on a regular basis to ensure confidence and comfort with using recycled PPE.
Institutions were granted the ability to establish recycling programs for certain PPE under an Emergency Use Authorization issued by the US Food and Drug Administration in March 2020. 11 These measures were only sought due to the critical shortages of PPE. Routine, noncrisis contingency recycling of PPE is not recommended due to safety concerns for HCWs and patients. Further, it should be noted that decontamination and reuse void the NIOSH approval of respirators. 5 Thankfully, by September of 2020, ICHE was able to discontinue the recycling program, as a steady supply of respirators were maintained. In June 2021, the US Food and Drug Administration revoked their decontamination and bioburden reduction system Emergency Use Authorizations since the national supply of NIOSH-approved respirators was maintained. 11 Guaranteeing an adequate supply of PPE prevented the implementation of other creative interventions, such as donning surgical masks over respirators or reuse without decontamination. It also prevented the worst-case scenario: that our institution would run out of inventory and thus be unable to meet respirator demand for frontline workers and ultimately limit patient care.
Conclusion
The ability to implement recycling programs can be essential to healthcare enterprise functions, as was proven at UTMB early during the COVID-19 pandemic. Such a program would be vital for future infectious pandemics, which could again stress supply chains that may struggle to meet the demands of a rapidly growing and evolving part of the public sector.
COVID-19 represents the latest in an era of increasing health security threats. As healthcare institutions begin focusing on preparing for future infectious disease pandemics or global outbreaks, such as monkeypox, innovative recycling programs such as this one may be used as a model to anticipate and prepare for potential PPE supply chain disruptions.
Footnotes
Acknowledgments
The authors would like to acknowledge the Galveston National Laboratory/Keiller Biocontainment and Research Team who coauthored the pilot decontamination validation studies and their continued support throughout the recycling program. We would also like to thank the ICHE, Environmental Health & Safety, and the following people for their support in the recycling program: Dr. Janak Patel, Michelle Guigneaux, Jennifer Bledsoe, Dean Leathers, and Nicolette Ward from UTMB. The authors would also like to acknowledge the support of the N95 decontamination operations by the Office of the Provost, UTMB, and the National Institutes of Health, National Institute of Allergy & Infectious Disease National Biocontainment Laboratories (NBLs) Operations Support (UC7 grant).