
Abstract
From the Field
is a semiregular column that provides insight into the experiences of local, county, or state health professionals on the frontlines of health emergencies. National Association of County and City Health Officials members share the challenges faced and the solutions developed as they prepared for and responded to disasters, epidemics, and other major health issues. The aim of sharing these practical experiences is to provide other public health champions with the information and tools they need to help keep their communities safe even in extreme situations.
The COVID-19 pandemic created an extraordinarily high demand for personal protective equipment (PPE). Acute need and supply chain disruptions made hospitals, emergency medical services, and other critical care agencies particularly vulnerable to PPE shortages. In March 2020, King County, Washington, developed computational tools, operating procedures, and data visualizations to fulfill its responsibilities to prioritize, allocate, and distribute scarce PPE equitably and efficiently during a public health emergency. King County distributed over 1.6 million gowns, 22 million gloves, 3.9 million surgical masks, and 1.5 million N95 respirators (among other items) during its PPE distribution mission. An algorithm processed resource requests from the community, with respect to available inventory, emergency allocation policies, prioritization constraints, estimated PPE use rates, agency-specific needs, and other parameters. With these inputs and constraints, the requests were translated into instructions for fulfillment and delivery and several tabular and graphical data visualizations were produced for quality assurance and transparency. Access to timely, relevant, and stable data was a constant challenge, and constraints invariably changed as the emergency response unfolded. King County's PPE distribution mission provides a useful case study in how to develop a scalable and data-driven approach to resource allocation and distribution under emergency response conditions.
Introduction
King County is a large metropolitan county in the state of Washington, with about 2.2 million residents, and is a major part of the greater Seattle area. In early 2020, King County was among the first areas in the United States impacted by the COVID-19 pandemic. The first diagnosed COVID-19 case in the United States was confirmed in February 2020 in the state of Washington, with the person coming through an international airport in King County. 1 The first reported COVID-19-related death in the United States was a King County resident 2 and the first identified COVID-19 institutional outbreak at a long-term care facility occurred in King County. 3 These events and the broader pandemic response created an extraordinarily high demand for personal protective equipment (PPE) in early 2020. This acute demand made PPE difficult to procure across the state, nationally, and internationally. Global supply chain disruptions constricted local and domestic inventories and led to major PPE shortages across the United States, putting additional stress and strain on the healthcare system and providers. 4 Emergency medical services (EMS), hospitals, health agencies, long-term care facilities (LTCFs—in King County these consist of adult family homes, assisted living facilities, and skilled nursing facilities) and other clinical settings were affected by PPE shortages in King County, leading to rationing and conservation measures for equipment and potentially compromising the health and safety of healthcare workers, first responders, and patients. Smaller facilities, such as adult family homes with 6 or fewer residents, without established relationships to vendors and other organizations with fewer financial resources were particularly vulnerable to PPE shortages, leading to further inequities.
To meet this unprecedented demand for emergency medical supplies, King County developed and invested in new approaches to purchase, receive, and redistribute PPE to healthcare networks and external partners. The need for a flexible and scalable system to manage the high volume of resource requests and handle distribution in an equitable, COVID-19 case-driven manner led to the creation of a data-driven process for PPE allocation.
Process Overview
In early March 2020, King County developed a novel, data-driven PPE allocation process to fulfill its responsibilities to prioritize, allocate, and distribute scarce medical supplies equitably and efficiently. This weekly approach used available data from facilities and epidemiological databases to algorithmically distribute resources under policy constraints and shifting inventory levels in 3 primary steps: (1) data ingestion and standardization, (2) algorithmic allocation, and (3) quality review and implementation.
Data Ingestion and Standardization
Under the incident command system (ICS) framework, the resource request form (RR 213) is often the standard approach to request resources during an emergency response. It is general enough to encompass a wide variety of materials and resources but lacks specificity (a byproduct of its generality), requires significant manual attention, and can be delivered in several ways (eg, fax, photocopy, email). Parsing these requests was cumbersome and required substantial staff time.
In response to this burden, King County developed a standardized form for PPE supply requests, which could be either submitted as an Microsoft Excel form by email or as an online form on the King County Office of Emergency Management website (online form no longer available; Figure 1: Receive orders). The new customized form limited incoming requests to items expected in inventory, emphasized general item types rather than brands, and standardized the item unit (eg, box, individual item, gallon). With these adjustments at intake, it was possible to implement new automated data standardization routines, which drastically reduced the amount of person-time required to handle incoming requests.

Flow chart of the King County prioritization, allocation, and distribution process for personal protective equipment. Abbreviations: EMS, emergency medical services; LTCF, long-term care facility; PPE, personal protective equipment.
Algorithmic Allocation
At the center of the PPE allocation process was an algorithm that combined incoming resource requests with situational intelligence on the burden of COVID-19 by facility type to inform the allocation of available PPE inventory.
First, all requests were screened for validity and eligibility according to the Washington Department of Health (DOH) Prioritization Guidelines for Allocation of Personal Protective Equipment 5 (Figure 1: Prepare orders). The prioritization guidelines were based on the type of requesting facility or organization, and requests were fulfilled by classifying facility types into tiers. Entities in direct, unavoidable contact with COVID-19 patients (eg, hospitals, EMS, LTCFs) were considered Tier 1, while other entities serving vulnerable populations in healthcare (eg, community health clinics, congregate settings) were considered Tier 2. Other selected entities, such as behavioral health clinics, social services, and childcare providers, were Tier 3. A fourth tier was added to include additional agencies not classified in other tiers. As the situation evolved, providers in certain facility types experienced different levels of COVID-19 exposure, and were therefore prioritized or deprioritized based on their relative risks according to changes in tiering guidance and epidemiological information. Prioritization changes also included loosening of item-based restrictions. For example, N95s were initially reserved for certain Tier 1 facilities, but as exposure patterns changed, N95s were distributed to an increasing variety of requesters.
Second, the requests were stratified by tier and item type (eg, surgical masks, N95s, gowns). For each set of Tier 1 requests, prioritization weights were generated from the amount allocated to each request as a function of estimated burn rate by facility type and case burden per facility (Figure 1: Tier 1 allocation). Burn rate estimates for some facility types, such as EMS, were taken directly from operational data streams that recorded the amount of PPE being used by the facility type, while estimates for other facility types were inferred from reported case load and subject matter expert assessments of how many daily PPE changes were required while caring for patients in that setting (Figure 1: Tier 1 prioritization inputs). Specifically, the PPE changes per case values for LTCFs, isolation and quarantine facilities, and hospitals were derived from guidance from hospital administrators, emergency services staff, and other subject matter experts. As additional data streams became available we updated the calculation of prioritization weights to reduce reliance per updated guidance. For example, as hospitals began reporting PPE supplies (late April/May 2020) these data were included as way to prioritize requests within the sector.
The following formula describes how a request (r) from a Tier 1 facility for an item (i) is addressed:
Where:
R is the list of requests in the tier for the same item i burn rate is the estimated amount of PPE per day (based on expert judgement and case counts) a facility requesting i is using. Burn rate calculations for the following facility types include: Hospitals: burn rate = 20 x number of cases at facility LTCFs: burn rate = 10 x number of cases at facility Isolation and quarantine facilities: burn rate = 20 x number of cases at facility EMS: reported weekly Public health response: reported weekly burden is a facility type-specific metric of population at risk. Estimates of burden for the following facility types include: Hospitals: number of COVID-19 patients at the facility Isolation and quarantine facilities: number of clients staying at the facility LTCFs: number of licensed beds at the facility EMS: resources divided among component entities Public health response: resources divided among component entities inventoryi is the amount of item i available for distribution x
For tiers 2 to 4, facility types were categorized into several ranked priority levels and any available inventory was allocated iteratively down the priority hierarchy (Figure 1: Tier 2-4 allocation). Unlike Tier 1 requests, there was no weighting or prioritization between similar facility types, resulting in an equal distribution of items up to the amount requested.
If the amount allocated to a given facility (
At the end of a weekly cycle, all open requests were closed, and facilities received an update on how much their requests had been filled as well as a target delivery time. If a request received no allocation (
Although some parts of the algorithm, such as the estimated number of PPE changes per patient by facility type, remained mostly constant over time, most other measures (eg, case burden) changed over time, usually weekly. By incorporating near real-time data streams, the algorithm adapted to shifting patterns of need, cases, and available inventory within the county.
Quality Review and Implementation
After each request was processed, the results were converted into several data products (Figure 1: Validate allocations and create picklists). Operationally, the most important product was the picklists, which provided the warehouse with instructions for what and how much PPE to send to a given requester. These were sorted and grouped by ZIP code to facilitate speedier delivery. To validate the results of the algorithm and provide a final quality assurance check, several documents and visualizations were also created. These included an interactive map showing the type of PPE and amount being sent to facilities by region and facility type, as well as a series of data dashboards that made it easy to manually identify outlier requests for quality control.
Other Strategies Used to Support PPE Distribution
King County implemented several other strategies to better meet the PPE needs of the community and supplement the regular PPE allocation process. An early example occurred in June 2020 when King County distributed 20 million surgical masks and 5 million cloth masks to libraries, cities, chambers of commerce, transit agencies, grocery stores, and hundreds of other local organizations for distribution to King County residents, with a special focus on those living in lower-income communities.
During emergency situations such as COVID-19 outbreaks at LTCFs or shelters, an urgent request process triggered by Public Health – Seattle & King County investigators was developed to provide expedited PPE shipments to facilities. As PPE supply and procurement became more reliable, staff conducted outreach to priority stakeholder groups, such as community health clinics, childcare providers, and other community-based organizations to increase awareness for the program and process for requesting emergency PPE.
King County surge strategies during the initial Omicron wave resulted in the delivery of more than 1 million KN90 respirators to King County community and faith-based organizations through a courier service and distribution events for community-based organizations and other groups to pick up PPE supplies. King County also provided PPE care packages to approximately 1,000 adult family homes in King County for outbreak prevention.
An overarching consideration of employing these different strategies to provide PPE was to try to address existing inequities in the community and make PPE available through other distribution opportunities, ultimately working toward more equitable health outcomes.
Outcomes
During King County's PPE distribution mission (April 2020 to June 2022), agencies and facilities submitted more than 60,000 requests for items, with some agencies submitting multiple requests, and over 70% were at least partially fulfilled. N95s, surgical masks, gloves, and gowns were the most requested items and represented about half of all requests.
King County distributed over 1.5 million N95s (68% of requested amount), 3.9 million surgical masks (83% of requested amount), 22 million gloves (85% of requested amount), and 1.6 million gowns (59% of requested amount) using the allocation algorithm—among millions of other items throughout the course of the pandemic.
LTCFs received most of the PPE distributed—as measured by N95, surgical mask, glove, and gown disbursement—at 17.7 million items (about 60%). This is partially a reflection of Public Health – Seattle & King County's efforts to supply adult family homes, which are smaller LTCFs and often owned or operated by Black, Indigenous, and people of color members or communities; and as smaller entities, they were also more likely to be impacted by supply chain shifts. Figure 2 shows how King County's distribution amounts changed over time, with the peaks usually corresponding to new waves of COVID-19 transmission and/or the changing availability of inventory. Figure 3 provides a further breakdown, showing a visualization of the weekly percentage of requests fulfilled for selected facility types and item types. These figures show how the combined effects of available inventory, prioritization guidelines, and competing requests affected fulfillment patterns. For example, health clinics routinely had their mask/respirator requests fulfilled at high levels but did not receive N95s until the summer of 2021 because of a change in the policy guidance. Conversely, community health clinics began receiving N95s, when available, in mid-2020 due to specific King County policy and strategy. LTCFs saw middling levels of N95 fulfillment until spring of 2021 when policy changes, an influx in inventory, and an improved supply chain facilitated higher fulfillment levels.
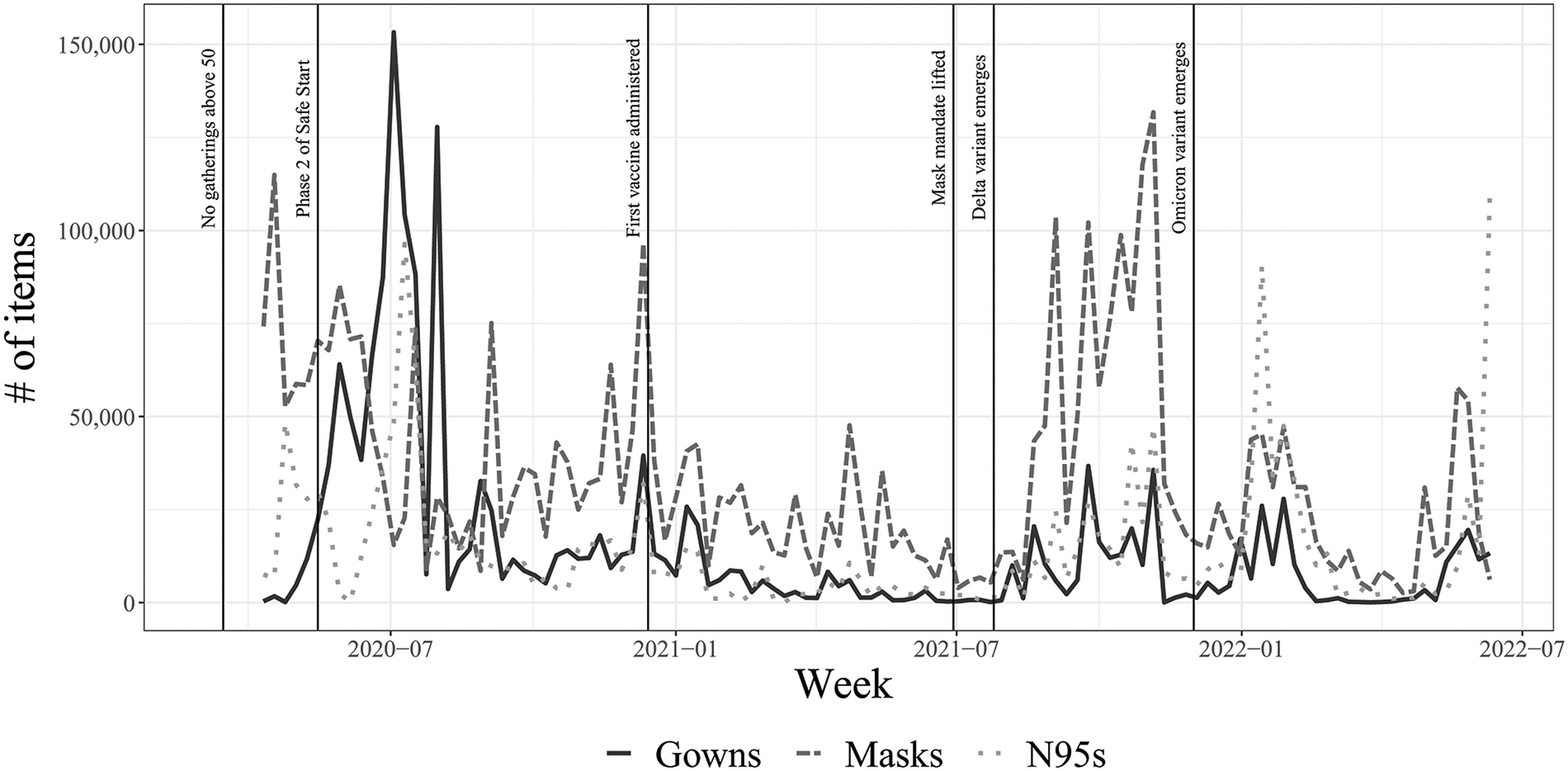
Timeline of gown, surgical mask, and N95 distribution by King County through the weekly allocation process.
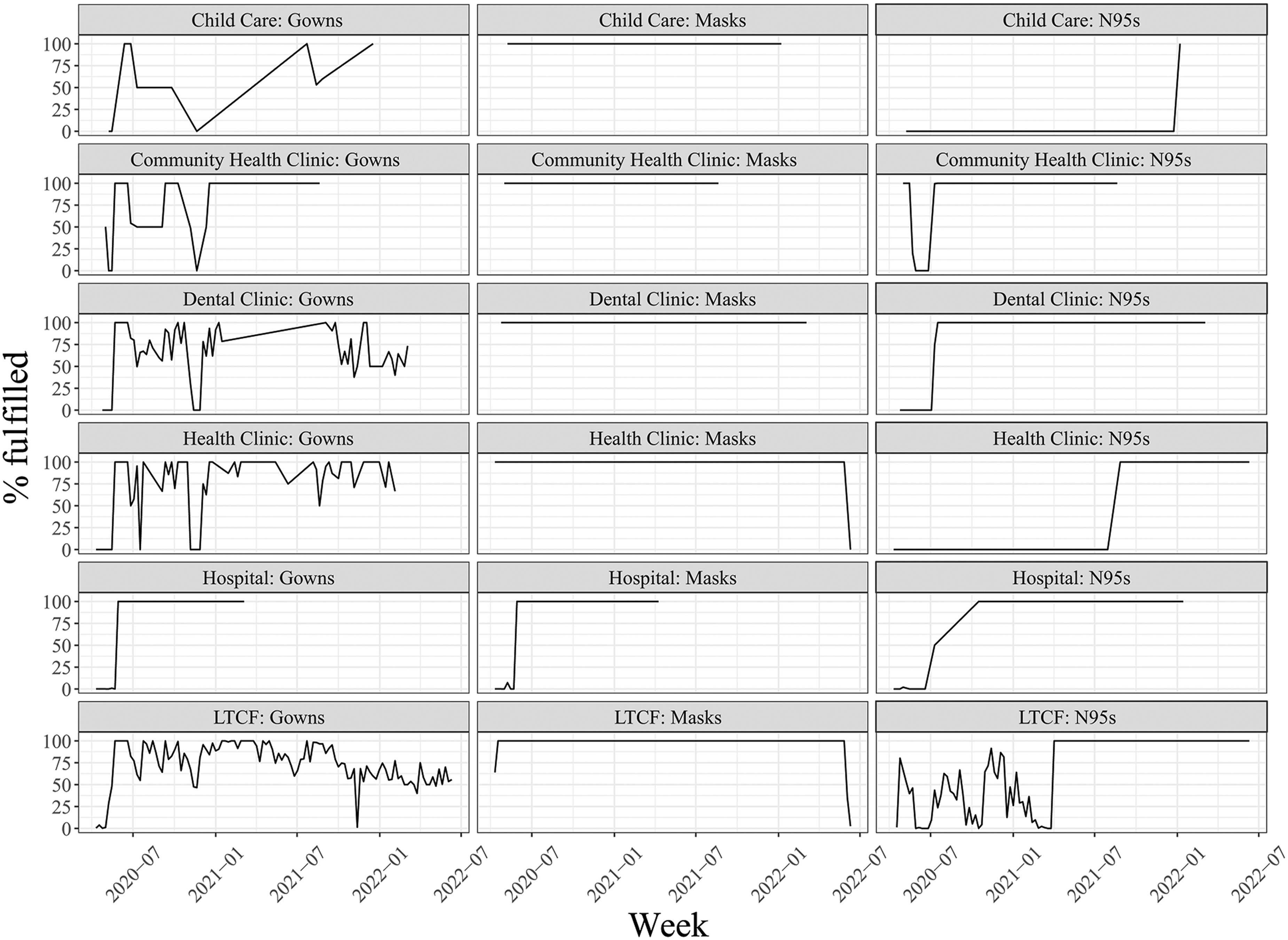
Percentage of personal protective equipment requests fulfilled by facility type and item type by week, April 2020 to July 2022. Abbreviations: LTCF, long-term care facility.
Of all PPE items requested, gowns were the most subject to inventory swings, as evidenced by the changing fulfillment percentages, especially for LTCF requests.
Throughout the pandemic, a monthly PPE fact sheet describing the PPE tiers, allocation strategy, and monthly allocations was posted online to provide greater transparency and accountability for the distribution process.
The implementation of the algorithm and associated process improvements noticeably reduced the time and labor required to execute the weekly cycle. At the beginning of the PPE distribution mission, the algorithm allocation step required at least 2 full-time employees working overtime as the algorithm was being developed and used simultaneously. By the end of the mission, staff levels for this step dropped to 1 half-time role. Additionally, close collaboration between the algorithm team and the warehouse team reduced delivery time from about 2 to 1.5 weeks. This reduction allowed the warehouse to deliver items sooner while also eliminating most weekend work. Other improvements by the warehouse team dropped the required labor resources by half.
With the substantial investment made in establishing a system to procure, store, allocate, and distribute PPE throughout the pandemic, King County is working on a sustainable plan to retain a 30-day supply of PPE that could be used for future emergencies.
In developing and implementing this process for PPE allocation, King County established stronger working relationships with external partners. These key relationships and the associated infrastructure helped build trust and contributed to success in other COVID-19 mitigation strategies such as supporting community vaccination events and distributing COVID-19 test kits.
Lessons Learned
During the development and implementation of the PPE allocation and distribution process, we identified areas for improvement and clarified the limitations of our approach.
Areas for Improvement
System Interoperability
We quickly discovered that various software systems within King County did not communicate with each other effectively. Although we connected some of the data silos, gaps remain. Getting data silos to interact with each other without manual input continues to be a challenge.
Modular Practices
While the philosophy and methods we used to allocate PPE within King County can be expanded to other resource-constrained situations, the technical implementation was specific to PPE and King County. Ideally, the design would be more transferable for other scenarios and settings.
Outreach
Many of the important community connections for PPE distribution developed during the emergency response were created in the moment. The groundwork to identify sectors requiring PPE could have been more explicitly laid before the emergency began.
Algorithms
The algorithm was designed to focus primarily on filling requests in a controlled way, with limited concern for how the orders would be physically packaged and shipped. Changing the algorithm design to identify warehouse-friendly solutions by rounding up orders and other optimizations could have further reduced the amount of work (eg, minimizing pallet repacking) required to deliver PPE.
Communication
A customer relationship management tool for handling bulk email would have reduced time spent by our logistics team to notify requesters of their order status.
Limitations of Our Approach
Despite the overall success of the approach to PPE allocation, there were some limitations. Automation and data analysis requires specialized skills and technological sophistication that were not always readily available. In addition, we still received reports of unmet needs, particularly during earlier periods of the pandemic when demand outpaced available supply. Some organizations may have given up on requesting supplies from the county after not receiving any due to low supply and/or not meeting the prioritization criteria at the time of their initial requests. Inability to fulfill requests at times of high need may have led to issues of diminished trust and impressions of low reliability from requesting organizations. Insufficient staff and time resources limited outreach and engagement, including language access and other accommodations. Language access support was an important part of outreach strategies for other parts of King County's response, but we were unable to provide language support or translated forms for this process.
Recommendations
King County's commitment to developing a data-driven approach to PPE allocation early on facilitated efforts to distribute necessary PPE to the community in a scalable way that could meet the changing demands of the COVID-19 pandemic. Successful implementation of the allocation algorithm required an initial investment in updating the resource management process by standardizing data inputs, introducing automation, and establishing data linkages. The underlying technological and process improvements were supported by partnerships with key stakeholders in King County, public health leadership, and WADOH. We believe this data-driven and scalable approach to resource management could provide a useful framework for other jurisdictions during public health emergencies, with the additional benefit of extending it to other components of emergency response. We provide the following recommendations for other public health jurisdictions to inform future response efforts.
Data and Software
Invest in software, smart data processes, and trained staff to ensure quality control and efficiency.
Smart Practices
Incorporate smart practices into processes to reduce staff time while ensuring thoughtful and high-quality review.
Conclusion
The collection of tools, visualizations, and processes described in this article improved the efficiency, transparency, and scalability of King County's PPE distribution mission. This data-driven and scalable approach to resource management provides a useful model for other jurisdictions during emergency responses.
Footnotes
Acknowledgments
We are tremendously grateful to staff from across Public Health – Seattle & King County and other King County departments, our partners, and the community, all of whom contributed their time and expertise to the COVID-19 response. We would especially like to acknowledge all of the teams and individuals that contributed to successfully implementing the PPE triage process in King County including Michael Croasdill, Staci Knutson, Sandra Davidson, and the 1st Ave Warehouse Team; Philip Sylling and the King County Information Technology Team; Sam Barbour, Juanita Cordova, Marianne Javillonar, Ted Toet, Jason Shirron, and the King County Office of Emergency Management; Alison Levy, Lisa Pan, Mashea Adams, Nick Solari, and the Public Health – Seattle & King County COVID-19 Operations Coordination Team.