
Abstract
Stanford Vax Crew, one of the largest medical-student-led vaccination programs in the United States, serves as a case study of a successful community–university partnership that adapted its existing operations to enable COVID-19 vaccine distribution. It offers a model for agile, community-centered vaccination campaigns that harness diverse stakeholder strengths to promote vaccine access and uptake in underserved communities. This case study aims to outline the history and structure of the community–university partnership model developed through Stanford Vax Crew, describe key observations of factors that contributed to the scalability of the model, and provide experience-based recommendations for future community–university collaborations.
Introduction
Over 676 million COVID-19 vaccine doses have been administered in the United States since vaccine distribution began. 1 Multistakeholder partnerships have formed and adapted to advance this monumental effort, highlighting the need to identify how such collaborations can promote effective, equitable strategies in the continued effort to address COVID-19 and in preparation for future public health emergencies.
Community–university partnerships have offered a model for delivering public health interventions for decades. Past studies have elucidated evidence-based strategies for successfully using these partnerships to achieve a shared public health goal. 2 For instance, Noel et al 3 described successful community–university partnership guidelines for cancer-prevention efforts. Similarly, Fields et al 4 and Kaur et al 5 outlined community–university partnership models to increase health literacy rates and reduce health disparities during the COVID-19 pandemic. Notably, most research has examined the initial development of new collaborations; however, there remains a need to examine the factors that enable preexisting community–university partnerships to adapt and expand in response to a novel public health emergency. Stanford Vax Crew, one of the nation's largest medical student-led vaccination programs, serves as a case study of a successful community–university partnership that expanded its operations to enable COVID-19 vaccine distribution in medically underserved communities. 6 This case study aims to outline the history and structure of the community–university partnership model developed through Stanford Vax Crew and provide experience-based recommendations for future collaborations.
Background
Stanford Vax Crew Structure
Stanford Vax Crew is a multidisciplinary team of healthcare students, physicians, and undergraduate students from Stanford University that has partnered with local community organizations to host free influenza vaccine clinics throughout California for 22 years as well as COVID-19 vaccine clinics since 2021. 7
Stanford Vax Crew, originally called Stanford Flu Crew, was founded in 2001 by Dr. Walt Newman with the mission of advancing health equity by increasing access to vaccines in medically underserved communities in California. In its first year of operations, Stanford Flu Crew administered 20 free influenza vaccines to farmworkers in the Salinas Valley. By 2019, the program was administering hundreds of influenza vaccines annually to students, community members, and farmworkers in the San Francisco Bay Area. 6 In total, Stanford Vax Crew has administered tens of thousands of free vaccines in the past 22 years.
To organize its operations, Stanford Vax Crew uses a 3-pronged leadership approach that consists of faculty physician supervisors, a healthcare student leadership team, and an undergraduate leadership team, as depicted in Figure 1.

Stanford Vax Crew leadership structure.
The faculty physician supervisors serve as advisors to the student leaders who organize events. They are also responsible for receiving, distributing, and documenting the influenza and COVID-19 vaccines that the organization uses, as well as supervising the student vaccinators. To receive institutional approval for events, the faculty liaises with the risk management department at the Stanford School of Medicine prior to each clinic.
The healthcare student leadership team consists of medical and physician assistant students from the School of Medicine who partner with the Stanford University Occupational Health Center and community-based organizations to organize vaccine clinics on and off campus, respectively. They also recruit physician supervisors and healthcare student vaccinators, coordinate event logistics, and collaborate with preclerkship course directors to develop and implement mandatory intramuscular injection training in the first month of the medical school curriculum. In accordance with policies outlined by the California Department of Public Health, medical student volunteers are allowed to administer vaccines as part of their course of study under the supervision of medical faculty. 8 Finally, undergraduate leaders recruit and train undergraduate volunteers to support nonclinical roles, such as registration, vaccine documentation, and community engagement.
The organization's operational costs are low given that it receives free vaccines from the county and federal governments and relies on volunteers. It has a budget of a few thousand dollars a year from the Stanford Medical Student Association to cover the cost of transportation and refreshments for volunteers at events, personal protective equipment, coolers for vaccine storage, and other necessary supplies.
Stanford Vax Crew Community Partnerships
Stanford Vax Crew includes the Stanford team and an extensive network of over 30 community partners—including community-based organizations, churches, and workplaces in Northern and Central California—who work together to provide both influenza and COVID-19 vaccines at free clinics. The collaboration represents an expansion of Stanford Flu Crew, which disseminated influenza vaccines prior to the COVID-19 pandemic.
Stanford Flu Crew established its first partnership in 2001 with the United Farm Workers, the nation's first and largest farmworkers' union. The organization represents thousands of vegetable, fruit, wine, and dairy workers in California, many of whom are recent or undocumented immigrants, and sponsors legislation to protect farmworkers and promote immigration reform. 9 Stanford Flu Crew has hosted dozens of free vaccine clinics at farms in the California Central Valley in partnership with the United Farm Workers in the past 22 years. During the pandemic, Stanford Vax Crew also began partnering with the UFW Foundation, a 501(c)(3) nonprofit sister organization of the United Farm Workers, founded in 2006, that advocates nationally for farmworkers' rights and provides critical services and community outreach in rural communities. 10
Other longstanding partners include the Salvation Army, the Roots Community Health Center in Oakland, and San Mateo County public libraries. The populations served by these organizations—including people experiencing homelessness; Black, Indigenous, and people of color communities; and individuals of low socioeconomic status—often face systemic barriers, such as lack of insurance, language barriers, and lack of access to healthcare. The Stanford Flu Crew network has played an essential role in providing community members with access to free influenza vaccines for decades, and the importance of these partnerships was magnified during the COVID-19 pandemic when racial and ethnic minorities faced disproportionately high rates of infection, hospitalization, and mortality.11,12 Collaboration between the medical school and community-based organizations offered an avenue for building trust in the healthcare system and reaching vulnerable populations with the vaccine.
Stanford Vax Crew partnerships are formed in 2 ways: (1) Stanford Vax Crew leaders conduct outreach to local community organizations to assess their interest in partnering, or (2) community organizations contact Stanford Vax Crew to inquire about partnership. Once the partnership is established, community partners provide an informal assessment of community needs to ensure goal alignment. Vaccination events are coordinated through meetings with all stakeholders. When setting up vaccination events, community partners and the Stanford Vax Crew leadership team work together to establish a clear workflow, plan for data collection to meet documentation requirements, and discuss effective community engagement strategies. After the vaccination event is complete, partners meet to debrief on ways to improve future events. Finally, the partnership is maintained through frequent communication about community needs and Stanford Vax Crew's capacity (Figure 2).

Stanford Vax Crew collaborative model.
The model used by Stanford Vax Crew provides an example of a successful community–university partnership that grew out of a community need—a need for free, accessible vaccines. The model leverages the strengths of the community partner and the university organization to promote vaccine uptake.
Discussion
In 2021, as COVID-19 rates spiked in California and the vaccine was authorized as the best tool for stopping its spread, Stanford Vax Crew, formerly Stanford Flu Crew, joined the national vaccination effort and began administering COVID-19 vaccines in addition to annual influenza vaccines.13,14 The team more than doubled the number of vaccination events it planned and implemented with support from both existing and new stakeholders. In the 2021-2022 academic year, Stanford Vax Crew organized dozens of vaccination events, administering over 1,000 influenza and COVID-19 vaccines. This represented a tremendous expansion of operations from previous academic years, such as 2018-2019, when the focus was on influenza vaccination events and fewer partners were involved (Table 1).
Expansion of Stanford Vax Crew Operations, 2018-2022
Note: Data are from the Stanford Vax Crew archives.
Intervening years were omitted to clearly distinguish prepandemic and postpandemic trends.
Some partners hosted multiple events, which is reflected in the lower number of partners than the total number of vaccination events organized.
Through all this change, Stanford Vax Crew has thrived and developed a system that both accommodates rapid expansion and responds to the dynamic nature of the pandemic. By laying out key observations from the collaborative, we hope to shed light on the factors that contribute to the scalability and adaptability of new and existing community–university partnerships during public health emergencies.
Observation 1: Strong Operational and Relational Foundations
Prior decades spent developing vaccination infrastructure and fostering trusting partnerships during nonemergencies provided strong operational and relational foundations that could be rapidly adapted and scaled up.
Operational Foundation
Unlike many other coalitions that formed in response to the pandemic,4,5,15 Stanford Flu Crew already existed when the COVID-19 vaccine was authorized, but it had to adapt its program to meet considerations specific to the new vaccine (Figure 3). These modifications were made by closely following public health recommendations, organizing weekly meetings among the Stanford Vax Crew leadership, and finalizing decisions via frequent calls with community partners.

Stanford Vax Crew operational adaptations to the COVID-19 pandemic.
To scale up, Stanford Vax Crew extended its annual timeline from a 2- to 3-month program that targeted influenza season to a yearlong operation, given the staggered eligibility requirements for the primary COVID-19 vaccine and subsequent boosters. The yearlong commitment posed challenges for the recruitment of student volunteers, including low staffing availability during vacations and exams; thus, a dedicated and prepared student leadership team was often required to operationalize events. Additionally, the organization had to supplement its operational budget by applying for state public health grants to support the increased number of events, which required more provisions and personal protective equipment for volunteers.
The team had to adjust its model for administering influenza vaccines—most notably by obtaining COVID-19 vaccines from a new source, the federal government, and adapting the workflow at events. However, its decades of experience training students to administer vaccines and its well-established administrative housing within the School of Medicine (which provided volunteers and insurance for the program) offered a strong operational foundation for partnering with community-based organizations to successfully distribute COVID-19 vaccines.
Relational Foundation
The critical work of building trust, both between partners and with community members, had been in progress with Stanford Flu Crew and its smaller network of community-based organizations for decades prior to the COVID-19 pandemic. The trust determination model of communication identifies 4 sets of factors essential for creating trust: (1) dedication and commitment, (2) competence and expertise, (3) caring and empathy, and (4) honesty and openness—all of which have been identified as critical for pandemic response.16-19 In the case of Stanford Vax Crew, stakeholders had already demonstrated (1) dedication and commitment by hosting vaccine clinics in the 20 years preceding the pandemic; (2) competence and expertise through their well-established operational model; (3) caring and empathy in their personal relationships with each other, such as at team dinners; and (4) honesty and openness through frequent planning meetings with all stakeholders. Thus, during the pandemic, preexisting relationships enabled interpersonal trust between partners, who could rely on the shared model to disseminate the new vaccine, and institutional trust from community members, who were already familiar with Stanford Flu Crew.
While Stanford Vax Crew had a relational foundation to provide COVID-19 vaccines to existing partners, they also used publicly available data to guide outreach to new groups according to need. For instance, in response to low pediatric vaccination rates, the group formed new partnerships with a children's musical company and a children's museum in San Jose to host pediatric-themed clinics. To build relationships from scratch, Vax Crew hosted meetings with new stakeholders prior to events to exchange organizational ideas and goals, conducted site visits to plan the clinic workflow, and debriefed via follow-up by email or phone after events. Throughout this process, members of the Vax Crew leadership team spoke with local county COVID-19 response team members as well as community partners to ensure events were targeting underserved populations without redundancy from services provided by other emergency response actors.
Observation 2: Clear Alignment of Goals
The clear alignment of goals enabled stakeholders to overcome historically distinct incentive structures. Historically, community–university partnerships have faced challenges due in part to differences in incentive structures: while community partners are rewarded through local recognition and improved community wellness, academics are incentivized to produce publishable findings that promote good among a broad audience. 20 This can lead to confusion in operations and breaks of trust. Strategies for overcoming these differences include the identification of common goals, the promotion of ongoing structured dialogue as priorities evolve, and the horizontal exchange of resources, the last of which will be discussed in Observation 3.20-22
Stanford Vax Crew is effective because its main goal is simple and long established for all partners—to disseminate vaccines broadly across Northern and Central California, with a focus on reaching medically underserved communities. All partners benefit from downstream consequences of the program: the university and hospital system support the education of future healthcare professionals and decrease emergency costs by enhancing preventive care; the public sector reduces its own administrative costs associated with vaccine delivery; the community-based organizations enhance the type and quality of services they can offer community members; and employers support the health of their workers. Thus, a mutually beneficial reward system shaped the initial development of Stanford Flu Crew, and this system has been reinforced throughout the COVID-19 pandemic.
Observation 3: Equitable Sharing of Resources
A commitment to providing and sharing resources equitably among partners structured horizontal collaboration where all stakeholders were necessary and valued.
Many of the coalitions that thrived in vaccine delivery during the COVID-19 pandemic did so by equitably sharing resources.4,23 This practice enables each stakeholder to contribute to the production of results that would be impossible to achieve in isolation and demonstrates each group's commitment to the other, contributing to interpersonal trust.
Stanford Vax Crew reinforced this concept through its own practice of sharing resources (Table 2). Each stakeholder recognized that resources for its own operations could only be provided by others, which helped to mitigate inequitable power dynamics that sometimes exist in community–university partnerships, as the value of each partner was visible and appreciated at every event. Additionally, each partner provided human resources. While Stanford had volunteers trained in vaccination techniques, community partners offered rich experiences of providing social support to community members and sharing promotional materials, such as flyers in English and Spanish, to increase attendance at events. This created an environment where both clinical and social skills were valued, which the program hopes will prepare future generations of healthcare and social service workers to partner to address the intersecting needs facing many patients.
Stanford Vax Crew Resource-Sharing Structure
Recommendations for Strategic Community–University Partnerships
Promoting strategic community–university partnerships is in the interest of government public health agencies, academic institutions, and community organizations because these partnerships are essential for building the community trust and resilience necessary for pandemic preparedness. Recommendations for how specific institutions can promote the formation and maintenance of strategic community–university partnerships are outlined in Table 3.
Institution-Specific Recommendations for Fostering Community–University Partnerships
While this case study outlines observations of a COVID-19 vaccine delivery team born from a preexisting influenza vaccine operation, the experiences of Stanford Vax Crew in establishing its initial influenza vaccine program, building new partnerships during the COVID-19 pandemic, and advising other universities can be used to synthesize recommendations for academic institutions and community partners who seek to build collaborations de novo. Figure 4 offers on-ramps for both universities and community partners who aim to initiate partnerships to build similar vaccine delivery programs.
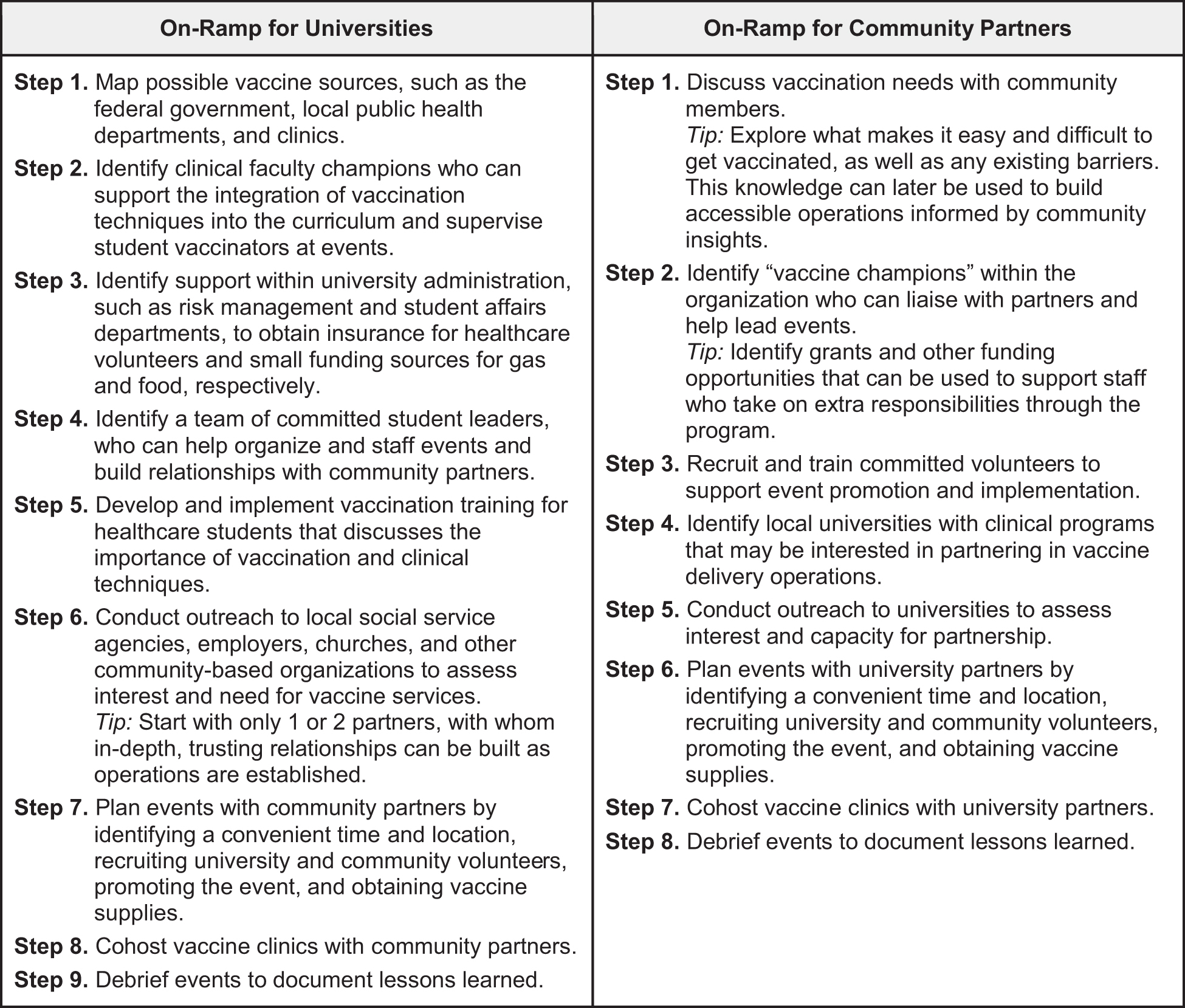
Steps for universities and community partners to build partnerships de novo in the community–university vaccine delivery model.
Limitations and Generalizability of the Model
Community–university partnerships can supplement, but should not replace, the role of the public sector in ensuring access to healthcare for all people. While Stanford Vax Crew and other grassroots initiatives have been responsible for the vaccination of thousands of individuals, given their small budgets, these organizations would be unable to operate if forced to purchase vaccines at prices set by pharmaceutical companies if the federal supply expires without further action. Therefore, this case study emphasizes the utility of government provision of free vaccines and the importance of collaboration between the public, private, and nonprofit sectors in promoting vaccine equity.
The Stanford Vax Crew model itself has limitations due to its reliance on medical students in their preclinical years, who phase out as they progress through the curriculum. The high turnover rate of personnel creates challenges in maintaining institutional memory, sustaining long-term initiatives, and maintaining partnerships as the continuation of the program depends on the commitment of future leadership teams. Stanford Vax Crew has implemented strategies to facilitate knowledge transfer by holding transition meetings at the start of the year and documenting institutional knowledge, but more work remains to be done. Thus, community–university partnerships that rely on student volunteers should acknowledge these limitations and likewise develop protocols that promote sustainability.
Finally, it is important to acknowledge the components of the community–university partnership model used by Stanford Vax Crew that contribute to and detract from its generalizability to other universities. The low cost of the program, which relies on volunteers and budgets less than US$200 per event for transportation and food, enhances its feasibility across institutions with varying amounts of resources, including universities that are both small and large, public and private. However, given the essential role of the academic institution in providing volunteer vaccinators, this model requires the involvement of trainees in fields such as medicine and nursing as well as faculty committed to teaching; thus, it is not applicable to institutions without clinical programs. The availability of undergraduate students also affects generalizability; in a clinical training program without an affiliated undergraduate university, this model would rely more heavily on community partners or clinical volunteers to fill roles such as registration and community engagement at events. Finally, this partnership model is generalizable only to universities with access to a vaccine source; thus, academic institutions seeking to replicate this model must identify a partner, such as a federally qualified health center, local clinic, or public health department, with vaccines to disseminate.
Conclusion
While community–university partnerships are not the ultimate solution to the larger structural issues that underlie the inequities of the healthcare system, they do offer a meaningful way to respond to public health emergencies, alleviate health disparities, and build trust between public health institutions and communities on a local scale. Stanford Vax Crew provides a model for community–university partnerships seeking to adapt and respond to evolving public health priorities.
Footnotes
Acknowledgments
We gratefully acknowledge the support of the Stanford Vax Crew's medical faculty supervisors, Dr. Walt Newman, Dr. Patricia Fast, and Dr. Judith Sanchez. We would also like to acknowledge the Stanford Vax Crew's community partners for sharing their knowledge, enthusiasm, and dedication to community health.
It is with deep sadness and gratitude that we acknowledge Dr. Walt Newman, who passed away before the publication of this manuscript. He was the heart and soul of the Stanford Flu Crew, later known as Stanford Vax Crew; the collaborative model discussed in this manuscript would not exist without him as he was a champion of community partnerships. He was a passionate family medicine physician and an incredible community advocate who practiced the art of medicine with unbridled dedication and joy. In addition to being a wonderful healer, he was also a patient mentor and innovative collaborator. He leaves behind a generation of healthcare professionals, students, and community partners dedicated to continuing his work promoting equitable, community-centered healthcare. While his work touched thousands if not millions of lives, his true legacy lies in the individual friendships that he cultivated with everyone he interacted with. To quote one of his favorites, William Shakespeare, “I can no other answer make, but thanks, and thanks, and ever thanks.” Thank you, Walt, we are all better because of you. May this manuscript serve as a testament to your incredible work.