
Abstract
An organizational culture of biosafety and biosecurity is critical for effective management of transboundary animal diseases. One essential aspect of this work is keeping important pathogens studied in veterinary laboratories under control. Türkiye is among the countries that are both endemic and disease-free for foot-and-mouth disease (FMD) virus, and it has a unique institute dedicated to FMD diagnosis, control, and vaccine production. To build an organizational safety culture within this institute and strengthen awareness of the importance of safe and secure handling of FMD, 4 staff members previously trained in biorisk management developed and provided trainings to all institute staff. The institute's 173 personnel were divided into 3 groups by job description based on direct or indirect work with FMD virus. All 3 groups received training that addressed biosecurity, biosafety, biorisk awareness, and insider threat; the trainings varied in length by group. Three-quarters (n=130, 75%) of all institute staff completed their training and were asked to complete knowledge surveys using a Likert scale survey before and after their training. A majority (n=104, 80%) of those participants completed both the pretraining and posttraining surveys. All 3 training groups' posttraining surveys showed improved awareness above baseline scores, and all 3 groups scores reached the targeted threshold goal. Group 2 demonstrated a realization that some of the knowledge and habits they had acquired through experience were incorrect. Scores for several individual questions decreased at posttraining, and these results will need further evaluation. The overall training results prompted the institute to provide periodic updates to employees to sustain the organizational safety culture. With this study, the institute now has a dedicated group of biorisk management representatives. This work serves as a wake-up call for established institutions that rely on staff experience to foster an organizational culture of biosafety and biosecurity.
Introduction
A
Biorisk issues are critical when working with microorganisms that potentially pose a biological danger. Both the World Health Organization (WHO) and the World Organisation for Animal Health (WOAH) define biorisk management (BRM) as having 2 major components. The first is biosafety risk, which is the possibility of unintentional infection. The second is biosecurity risk, defined as risk of unauthorized access, loss, theft, misuse, diversion, or deliberate release.2,3 Furthermore, according to WHO, there is a third component of BRM, which is the oversight of dual-use research. This refers to research that can reasonably be expected to produce knowledge, products, or technology that others could directly misapply to damage public health and safety, agricultural crops and other plants, animals, or the environment. 4 To keep the environment, society, and employees safe and secure, high attention should be given to all 3 components of BRM and to measures for their recognition, evaluation, and mitigation.
Although foot-and-mouth disease (FMD) is not considered a biorisk in countries where the disease is endemic, the absence of cross-protection across serotypes in this virus means there is high risk of introduction of a novel serotype into a new endemic location. One example is the A/G-VII epidemic of 2015 in the Anatolian part of Türkiye, which had dire repercussions and an economic impact of approximately US$230 million, according to the Ministry of Agriculture and Forestry's 2015 national risk-based strategic plan for FMD. 5 Losses from FMD outbreaks can result in even more severe economic losses in disease-free countries; for example, during the 2001 outbreak in the United Kingdom, £39 million (US$53.5 million) and £1.34 billion (US$1.83 billion) were allocated for business recovery and farmer compensation, respectively.6,7
FMD is an acute, highly contagious viral disease of cloven-hoofed animals that has significant potential for use as a bioweapon in an agroterrorism assault. Biosecurity precautions for FMD are always on governments' agendas, even though a biological attack using the FMD virus (FMDV) would have no direct impact on human health and many animals affected by FMD recover.8-10 Nevertheless, the US government has developed a program to perform frequent evaluations of government-funded or government-conducted research involving 15 high-consequence infectious agents and toxins, including FMDV, for their potential to be dual-use research of concern and to mitigate the risks when possible. The fundamental purpose of this monitoring is to safeguard the benefits of biosciences research while reducing the possibility of abuse. 11
FMD causes severe losses in the production of meat and milk, with significant impacts on a country's livestock due to factors such as restrictions on animal movement, including the export of animal products, the burdens of compensation to farmers, and the intensification of veterinary services. In addition, people in disease-free areas that choose to treat FMD by stamping it out may be unable to benefit from the nutritive advantages of animal food. These effects also have the potential to diminish a country's tourism earnings. 6 Due to the importance of the potential and actual effects of FMD, it is critical to build an organizational safety culture in places working with the active virus, such as the ŞAP (Foot and Mouth Disease) Institute, which acts as the national reference laboratory and vaccine manufacturing facility for FMD in Türkiye.
The ŞAP Institute produced an average of over 139.5 million monovalent vaccine doses between 2020 and 2022, which includes exports to Azerbaijan. In addition to vaccine production, another main responsibility of the institute is tracking FMDV serotypes and lineages in the field and sharing them either for research projects or upon demand to the World Reference Laboratory for Foot-and-Mouth Disease and the European Union Reference Laboratory for Foot-and-Mouth Disease. Given factors such as the lack of comprehensive BRM training at the institute, as well as disparities in knowledge levels among employees (such as those with PhDs, good manufacturing practice auditors, recent graduates, and staff with no previous laboratory experience), it became necessary to provide basic BRM training to new institute personnel and to augment BRM knowledge among existing personnel. These were the motivations for efforts to create a proactive BRM culture, which would in turn necessitate a driving force that extends beyond adhering to external supervision. 12
The purpose of the institute's BRM initiative was to assess the staff's awareness of biorisk at the institute, enhance their knowledge of biosafety and biosecurity through BRM training, and evaluate their internal threat perceptions and responses to potentially unfavorable scenarios. Staff knowledge levels were measured using pretraining and posttraining surveys.
Methods
Institute Demographics
During the study, the institute had 177 personnel, of which 53 were female and 124 were male. The distribution by age range was 29% (n=52) for ages 25 to 35 years, 29% (n=52) for ages 36 to 45 years, 30% (n=53) for ages 46 to 55 years, and 11% (n=20) for ages 56 years and older. The distribution by years of experience in the institute was 5% (n=8) with 1 to 4 years of employment, 54% (n=95) with 5 to 10 years, 16% (n=29) with 11 to 15 years, and 25% (n=45) with more than 15 years. Among these staff members were 10 good manufacturing practice auditors and 4 veterinarians; of the veterinarians, 2 held PhD degrees, with 1 having obtained the International Federation of Biorisk Associations' Professional Certification in Biorisk Management, and the other 2 held bachelor of science degrees. All 4 veterinarians had received training in BRM from Sandia National Laboratories and were part of the instructor team for the study: the 4 instructors were not included as part of the study population.
Training Groups and Final Study Population
The training was extended to all staff members at the institute, as it represented the first comprehensive biorisk training provided and was therefore mandatory.
The 173 staff members requested to attend training were grouped into 3 sections for the training based on their level of interaction with the virus. Group 1 (n=94) consisted of veterinarians, biologists, chemists, and laboratory staff who worked directly with the FMDV. Mechanics, drivers, and cleaners had the possibility of contact with the virus during precleaning, driving, engineering, or preparation, and were placed in Group 2 (n=19). Finally, office workers, security guards, and other professionals who did not have contact with the virus were placed in Group 3 (n=60). Groups 1 and 3 were made up of employees with varying levels of expertise, while all members of Group 2 had more than 10 years of experience at the institute. Details about the training groups are shown in Table 1. Except for the instructor team, none of the staff had received any training in BRM before.
Training Groups, Attendance, and Pretraining and Posttraining Survey Completion
The institute had 177 staff members, but the 4 who acted as instructors were not counted as part of any training group, leaving 173 to be trained. Of the 130 staff who attended their training, 104 completed both pretraining and posttraining surveys. bThe final study population. cTwo separate full-day training sessions were conducted with identical content to manage the crowd and enhance the efficiency of the training.
Abbreviations: GMP, good manufacturing practice.
Due to production demands, diagnostic activities, or health issues, 43 staff members could not attend the training. Of the remaining 130 employees, 75% (n=70 out of 94) of Group 1, 84% (n=16 out of 19) of Group 2, and 73% (n=44 out of 60) of Group 3 participated in the training sessions. However, 26 participants did not complete the pretraining and posttraining surveys, resulting in a final study population of 104 respondents: 55 (53%) in Group 1, 12 (11%) in Group 2, and 37 (36%) in Group 3.
Training
Held December 17 to 20, 2019, the training addressed 4 main topics: biosecurity, biosafety, biorisk awareness, and insider threat. For detailed examination, each topic was divided into subtopics. In addition, training content was tailored to each group's level of interaction with the virus (Table 2). For instance, measures to prevent illegal entry and theft or release of biological materials or organisms were discussed under the “physical security measures” subtopic. On the other hand, proper usage of gloves, laboratory coats, face shields, goggles, footwear, and gowns, and methods to reduce the risk of exposure, were covered under the “use of personal protective equipment (PPE)” subtopic. The contents of all training topics and subtopics are provided in the Supplemental Information (www.liebertpub.com/doi/suppl/10.1089/hs.2023.0044).
Training Topics and Subtopics by Training Group
Note. √, topic included in the training; x, topic not included in the training.
Based on the number of training topics and the amount of content identified for each group, Group 1 received a full-day training and groups 2 and 3 each had a half-day in-person training. The instructor team used training materials from the Sandia National Laboratories Global Biorisk Management Curriculum library, along with the additional documents cited here.13-16
Pretraining and Posttraining Surveys
The pretraining and posttraining surveys used a 5-point Likert scale (strongly disagree, disagree, neutral, agree, strongly agree). The study team established a score of 4.0 as a threshold level required for either the overall average score, the score on specific topics, or for individual items, in order to deem participants as having satisfactory awareness and understanding of the principles targeted in the study. Groups were given varying numbers of questions or statements in their survey depending on their jobs/roles and the technical content of their training: Group 1's survey had 69 items, while groups 2 and 3 had 46 and 36 items, respectively. For example, in the PPE-related section of the survey, Group 1 was asked to respond to the statement “I wash my hands after working in the laboratory,” whereas Group 2, given their responsibility for collecting biological waste, was additionally asked to respond to “I always use the necessary PPE when collecting biological waste.” Conversely, since Group 3 was less likely to interact with the virus, their sole statement to respond to was “I know what type of PPE I should use if I have to go to the lab.” Two identical written questions (eg, give 5 examples of biosafety, give 5 examples of biosecurity) were included for all groups at the end of the survey to determine if trainees could distinguish the difference between biosafety and biosecurity.
All staff who completed the pretraining survey were invited to complete a posttraining survey again 1 month after the training. The posttraining survey responses were examined to evaluate the retention of the information provided during training and to gauge the increase in trainees' perception of their BRM knowledge.
Data Analysis
Overall survey scores were calculated by taking the average of the item scores, and a Wilcoxon signed ranks test was used to determine the significance between pretraining and posttraining survey results. Statistical analyses were performed using jamovi software version 2.3 (the jamovi project, Sydney, Australia). We calculated the percentages of trainees who gave 5 correct examples for both written questions.
Results
In all groups, average posttraining scores increased over the threshold level of 4.0 (Figure 1). When the significance in the score changes between pretraining and posttraining surveys was analyzed, Group 1 showed a 5.68% increase, Group 2 had a 0.75% increase, and Group 3 had the highest percentage increase, at 12% (P<.05). Figure 2 shows the overall increase in scores by training topic for each of the 3 training groups. Biosafety and biosecurity scores rose significantly in Group 1, while Group 3 showed a substantial increase in scores for all topics (P<.05). On the other hand, there was no difference detected in Group 2 (P>.05). Figure 3 shows improvement in trainees' ability to list in writing 5 individual examples of biosafety and biosecurity, by training group. Each group showed improvement, with scores increasing by 12% for Group 1, 80% for Group 2, and 19% for Group 3.

Average pretraining and posttraining survey scores for the 3 training groups. The threshold level was set at 4.0.
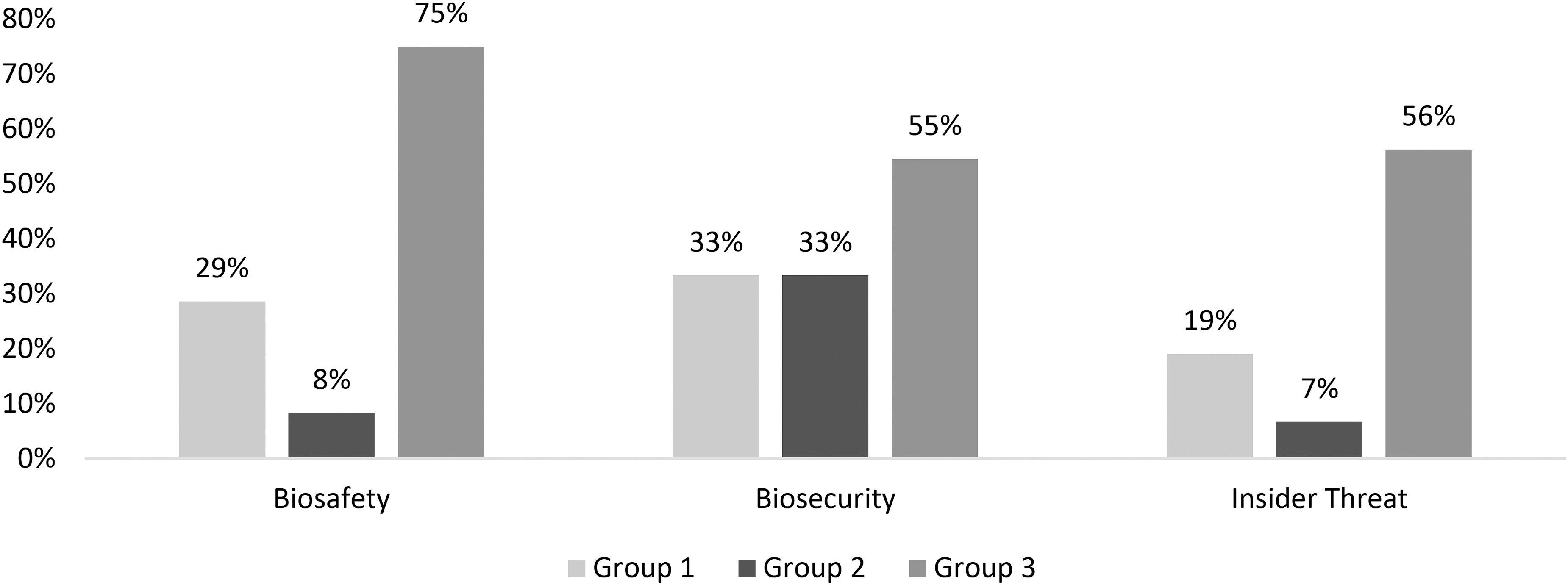
Percentage of questions with scores that increased between pretraining and posttraining, by main training topic and training group.

Percentage of participants who correctly answered the 2 written questions (5 examples each of biosafety and biosecurity), by training group.
Tables 3, 4, and 5 break down the pretraining and posttraining survey responses for each group by key biorisk topic presented during their training. As noted in Figure 1, each group increased their average scores from the results of the pretraining survey to the posttraining survey completed 1 month after the training, and the average threshold score was also above 4.0, our targeted goal going into the sessions. However, we did see lower posttraining than pretraining scores in some topics and subtopics for Group 2 (Table 4). When examining the group responses in detail according to training subtopics:
Survey Results for Training Group 1, by Topic and Subtopic (n=55)
Survey Results for Training Group 2, by Topic and Subtopic (n=12)
Group 1 (laboratory staff) recorded increases in posttraining results from 3.87 to 4.09, but did not achieve the 4.0 threshold for the following 6 subtopics: inventory (3.70), security measures for visitors (3.97), waste management (3.57), sterilization (3.70), security measures for insider threats (3.44), and teamwork (3.70) (Table 3).
Group 2 (mechanics, drivers, and cleaners) responses demonstrate where the institute needs to focus most attention. Though this group showed a very slight increase in general knowledge when all topics were combined (4.00 to 4.03), it was also the only group to show posttraining decreases in some of the training topics, with slight decreases in both biosafety (4.08 to 4.05) and insider threat (4.01 to 3.94) topics (Table 4). Group 2 also did not achieve the 4.0 threshold for 7 subtopics: security measures for visitors, hygiene, use of PPE, sterilization, awareness of biorisk, security measures for insider threats, and teamwork. Additionally, Group 2 exhibited decreases in scores for 5 subtopics, as shown in Table 4.
In Group 3 (office workers), apart from security measures for insider threats and teamwork, the posttraining scores for other subtopics exceeded the 4.0 threshold, with the total score changing from 3.74 to 4.20 (Table 5).
Survey Results for Training Group 3, by Topic and Subtopic (n=37)
Discussion
During World War II, various countries independently conducted incredibly ambitious biological warfare research programs, and FMDV was one of the agents studied. 17 Besides the possibility of agents being used as biological weapons, there is always the possibility that an agent could accidentally escape from the laboratory. One of the more noteworthy biorisk incidents in recent decades was the accidental release of an FMDV laboratory strain from a laboratory in UK, which contaminated nearby areas and caused more than £100 million (US$192.5 million) in financial damage in 2007. 18
As the largest manufacturer of FMD vaccine in Türkiye, the ŞAP Institute places a high priority on biorisk. Across the country, attempts are being taken to foster a “organizational culture of biosafety and biosecurity,” the significance of which is becoming clearer day by day. First and foremost, training is the top-ranked mitigation measure of proactive BRM. The ŞAP Institute training was planned based on the need to establish an organizational culture of safety not only among laboratory staff handling the virus on a daily basis, but also among all employees at the institution, including office personnel, whether they have access to biohazards or not. In addition to creating this culture, the aim was to ensure that all employees act consciously while supporting each other in practice.
When these trainings were initially planned, the institution had 177 personnel, 4 of whom were trainers. However, due to ongoing FMD diagnostic and vaccine production activities, along with unforeseen health issues, only 130 employees were able to participate in the training, and of these, 104 completed both the pretraining and posttraining surveys. According to the overall scores, Group 3 had the most substantial improvement (12%) in their posttraining biorisk scores across all topics, followed by Group 1 (5.68%) (Figure 1). This was to be expected, as Group 3 employees are unlikely to interact with the virus and had no prior experience with biorisk issues. For all 3 groups, the biosecurity questions improved the most consistently after training (Figure 2). Groups 1 and 2 both increased their biosecurity knowledge by the same percentage (33%), while Group 3 had the highest proportional increase in biosecurity knowledge (55%). The project was initiated with a focus on biosecurity and insider threat, as compared with biosafety topics, these were topics that had not been given significant attention previously. Insider threat appears to be one of the areas to review in depth, as compared with other the topics, the posttraining results showed lower scores among the groups with direct access to pathogens (4.04 and 3.94 for groups 1 and 2, respectively). Also, the biorisk topic (3.81) had an even lower posttraining score than insider threat (3.94) in Group 2.
Group 2 exhibited the least increase (0.03) in overall knowledge following training, and was the only group to show lower posttraining scores than pretraining scores for some of the questions. Moreover, none of the participants in Group 2 were able to list any biosafety or biosecurity examples on the pretraining survey. The percentage answering these questions fully and correctly increased by 80% following the training (Figure 3). This was expected, however, because Group 2 had not been previously trained in the relevant topics. In fact, the improvement in scores for Group 2 after the training was remarkable and will serve as a focus for review by the training team with an eye to updating our training in the future. As this group does have possible direct access to pathogens, we plan to determine how we can increase awareness of all aspects of BRM in the future for the cleaners and technicians in Group 2. This will involve adding more information on these topics to their introductory trainings as well as to the refresher training that we are formulating. Additionally, we believe it would be beneficial to divide this group's training into smaller, face-to-face informational sessions.
During our detailed examination of subtopic knowledge, we did see an increase in insider threat awareness among Group 1 and Group 3, although not in Group 2. With this awareness, the staff made a different evaluation 1 month following the training. However, the survey results for security measures for insider threats and teamwork remained below the threshold value in all groups (Tables 3, 4, and 5). While scores did not improve in subtopics such as teamwork, which is a situation that would take a long time to rectify, positive changes were observed in the 3 subtopics of awareness (awareness of biosecurity, biorisk, and insider threat), which are subjects that can be covered more rapidly in practice, and scores improved in a short time. After the trainings, the survey results were reported to the institute's administration for the purpose of increasing precautions, and it was decided to give priority to these issues in the next training. We will need to focus more time on the insider threat topic during training, especially for Group 2, as this was identified as one of our most important training goals during development of our training materials. We need to improve our messaging, but we must also balance the amount of potentially sensitive information provided.
Two factors could have skewed the data. First was the significant percentage of staff that had some prior knowledge about most of the topics before completing the training, especially the good manufacturing practice auditors and laboratory staff in Group 1. Second was the length of time between the training and the distribution of the posttraining survey. For those without prior BRM training—and many were receiving information on insider threat awareness for the very first time—assessing awareness of BRM principles 1 month after training would be a challenge. Based on this, we have tried to determine what to improve for future trainings.
Lessons Learned and Recommendations
While planning for future training, the following data will guide the instructor team. For laboratory staff in Group 1, failing to achieve the 4.0 threshold in 6 of the subtopics is the main area for improvement in the review and update of our training. These topics are essential to have an increased level of understanding and awareness. Furthermore, the waste management topic, which is below threshold, has been directly associated with devastating outbreaks in the past (eg, the 2007 FMD outbreak in the United Kingdom 19 ). Meanwhile, the slight score decrease in the insider threat topic among mechanics, drivers, and cleaners in Group 2 brought the posttraining score to below the 4.0 threshold, which reinforces the need to review and update how information on this topic is presented.
Group 2 was the only group to show posttraining decreases in biosafety subtopics. We grouped mechanics, drivers, and cleaners together due to their potential for access to the virus, but this group had varied levels of education. When we examined the survey responses in detail, we noticed that the cleaners' responses differed significantly from others' responses. We believe that some of these results can be explained by the conscious competence matrix. 20 It has 4 stages, covering the phases between not realizing how much we still need to learn and realizing what we do not know. In Stage 1 (unconscious incompetence), a person has a complete lack of knowledge and skills in a specific area, and is unaware of this. In Stage 2 (conscious incompetence), a person has discovered that they need to learn new skills. Training becomes important to avoid wrong decisions. In Stage 3 (conscious competence), a person is skilled but is not performing activities as an automatic response. At this point, it is necessary for them to update their information periodically to ensure that these skills are not diminished. In Stage 4 (unconscious competence), a person is performing their tasks without thinking, like an innate talent. 20
The mechanics, drivers, and cleaners in Group 2 were receiving BRM training for the very first time, and we believe that the differences in their results can be explained by this conscious competence matrix. All had worked for the institute for more than 10 years, and their knowledge from experience was why they achieved high scores in both surveys, without prior training. However, following the training, they began to question their ingrained knowledge and while they corrected their knowledge on some topics they also lost their confidence on others. After the evaluation of the scores, instructors realized they were at the second stage of the matrix. It became apparent that continuous training would be needed for them to transition to the following stages. Although there were no significant differences between the group's pretraining and posttraining scores, the very slight increase in overall scores, and the increased scores in most of the topics, led us to believe that the education was still effective at improving this group's BRM and biosecurity knowledge.
Numerous studies have demonstrated the value of education in promoting awareness in the biorisk field.21-25 Our institute's leadership believed that it was especially important that all staff receive more advanced training according to their work area. We divided the staff into groups based on direct handling of, potential access to, or no access to the virus, and we will retain the groups for future training sessions. We also gained invaluable insight with this educational initiative that we will incorporate in our next round of BRM training, especially for the 43 staff who could not participate in the initial training, for new personnel coming into the institute, and for Group 2 staff, who had the least amount of improvement overall. This group included the least educated staff members, and all were receiving BRM and biosecurity information for the first time at our training. We also provided a lot of information to this group in a short time by trusting their experience. For future trainings, we have decided to break down our training information for Group 2 into smaller informational sessions and to build in repetition to help reinforce critical concepts.
The data we gathered from this study gave us the idea to construct face-to-face training for Group 2 and for new employees who require more specific training.20-22 For employees with an intense schedule due to vaccine production and an appropriate degree of competence, reminder trainings can be planned virtually, especially for those who do not have time to attend on the scheduled date and time of the face-to-face training.23,24 Both face-to-face and virtual approaches, each with their own advantages and disadvantages, might be chosen according to the predetermined level of knowledge of the personnel.
Overall, BRM and biosecurity knowledge increased for all our training groups, and the posttraining survey, sent a full month after the training, demonstrated that we were successful in raising awareness about how to act against insider threats. Furthermore, the institute has since made many developments, starting from the topics where trainees did not exceed the threshold level on the posttraining survey. These developments can be listed as follows:
For implementing proactive BRM, the administration recognizes the importance of education. Training that could not be held immediately due to the COVID-19 pandemic is being planned now. Moreover, the pretraining and posttraining surveys identified people's knowledge gaps. The instructor team now has valuable outcomes gathered from these surveys that will help them prepare further educational materials, including on topics that should be emphasized, participant profiles, training formats (face-to-face or online), and training durations. For both outsider and insider threats, the administration has increased precautions since 2020, such as placing cameras at strategic locations. All areas are monitored and recorded using nearly 100 cameras. Within the scope of biosecurity measures, the number of security guards has increased, and they have been qualified through training. As biosecurity measures, all precautions are being taken with visual, auditory, and motion-sensitive sensors. Also for biosafety and biosecurity purposes, the personnel transition system has been updated. With this system, transitions are kept under control by monitoring personnel movements to isolate infected areas and clean area workers for biosafety requirements. In terms of biosecurity, both employees and visitors are recorded in accordance with the Personal Data Protection Law.
26
The significance of inventory has been recognized since the training. An intranet system for the storehouse to track consumables was developed and has been used for almost 2 years. The intranet system enables staff to follow all processes applied within the institution for vaccine production, control, and also diagnosis. In this way, all processes involved in the flow and disposal of dangerous goods are easily monitored and managed in a controlled manner. In addition to monitoring vaccine production, shipping can be followed throughout the country. Another software system is under development for pathogen archives, where access-restricted computers may contain storage information of the live viruses. For waste management and PPE, the importance of using appropriate waste containers was recognized, and sharps boxes were distributed to all laboratories. Insufficient PPE were detected, after which PPE was provided, and warning signs for both PPE and hygiene were hung on the walls. In addition, the personnel in charge of controlling and promoting the use of PPE were identified and described. For hygiene and sterilization, a waste management standard operating procedure has been written following the template of Sandia National Laboratories.
Besides the improvements mentioned above, the most important finding of this study is that having an experienced staff such as those in Group 2 is not enough for an effective organizational culture of biosafety and biosecurity. Management should ensure that all staff continue their education with the appropriate type of education for each group profile.
Footnotes
Acknowledgments
The authors are grateful to Sandia National Laboratories, DTRA Biological Threat Reduction Program, US Department of State, Biosecurity Engagement Program, and Republic of Türkiye Ministry of Agriculture and Forestry. We are especially grateful to Eric Cook, William Pinard, all other Sandia National Laboratories staff, and all managers and all staff of the ŞAP Institute.