
Abstract
National public health emergency operations centers (PHEOCs) serve as hubs for coordinating information and resources for effective emergency management. In the International Health Regulations (IHR 2005) Monitoring and Evaluation Framework, a simulation exercise is 1 of 4 components that can be used to test the functionality of a country’s emergency response capabilities in a simulated situation. To test the functionality of PHEOCs in World Health Organization African Region member states, a regional functional exercise simulating an Ebola virus disease outbreak was conducted. The public health actions taken in response to the simulated outbreak were evaluated against the exercise objectives. Thematic analysis was conducted to summarize key strengths and areas for improvement. From December 6 to 7, 2022, more than 1,000 representatives from 36 of the 47 African Region member states participated in the exercise from their respective PHEOCs. Approximately 95% of the 461 participants polled agreed with the positive responses to the postexercise survey. More than half of the PHEOC participants were able to test their existing emergency preparedness and response plans and became familiar with the expected roles to be fulfilled during an event. Of the participants who responded to the survey, over 90% reported that the exercise helped them understand their roles during emergency management. The exercise met its objectives and provided an opportunity to test the functionality of PHEOCs using realistic scenarios, and it helped participants understand existing response systems and procedures. However, the exercise also revealed areas for improvement in terms of the timing and preparation of participants. We recommend conducting functional exercises at the regional and national levels at least once a year, early or midyear, to allow many stakeholders to take part in the exercise. Moreover, there is a need to train country-level evaluators and controllers in designing and conducting functional exercises.
Introduction
M
After the 2014-2016 EVD outbreak, member states and relevant stakeholders stepped up measures to strengthen emergency preparedness and response capabilities, including the establishment of public health emergency operations centers (PHEOCs) as part of their emergency management program. WHO AFRO, in collaboration with the Africa Centres for Disease Control and Prevention (Africa CDC) and other partner organizations, supported the initiatives in various ways, for example, by providing guidance through the Framework for a Public Health Emergency Operations Centre in 2015. 3 In the same year, WHO AFRO officially launched a regional emergency operations center network (AFR-EOCNET) to collaborate with member states and key partners to assist countries in establishing PHEOCs and to promote the exchange of best practices. 4
A PHEOC is a hub for the effective coordination of information and resources during the management of public health emergencies. It employs an incident management system (IMS)—an emergency management structure with sets of standardized procedures, protocols, and skilled human resources—to provide a coordinated response approach for all types of public health emergencies.3,5 An established PHEOC is one of the requirements member states should implement to fulfill International Health Regulations (IHR 2005) 6 requirements to effectively prepare and respond to public health emergencies.
WHO recommends a training and exercise program as part of the PHEOC to regularly test functionality of plans, procedures, and systems, and to develop skills. A simulation exercise is 1 of 4 components in the IHR Monitoring and Evaluation Framework 7 that can assess the functionality of a country’s emergency preparedness and response in a real or simulated situation. “A simulation exercise is a form of practice, training, monitoring or evaluation of capabilities, involving the description or simulation of an emergency to which a described or simulated response is made.” 7 Any actions taken as part of a public health response must be reviewed and assessed to capitalize on best practices and identify areas and actions for improvement. 8
A functional exercise is intended to create a situation as close to an actual event as possible and that engages players and helps test available plans and procedures, tools, technologies, and interoperability as if it were a real event at the designated facility without involving the actual deployment of resources to the field.9,10
During regional PHEOC meetings in 2017 and subsequent meetings, member states recommended that WHO and other partners conduct regional functional simulation exercises to assess the functionality of PHEOCs as well as test communication, coordination, and information sharing among national PHEOCs. As a result, 2 regional functional simulation exercises were conducted in 2018 and 2019; however, implementation was interrupted in 2021 and 2022 due to the COVID-19 pandemic. WHO AFRO, in collaboration with Africa CDC, the West African Health Organization, the US Centers for Disease Prevention and Control (US CDC), the UK Health Security Agency, and the Robert Koch Institute, conducted a third regional functional simulation exercise from December 6 to 7, 2022, to test PHEOCs’ functionality in member states in WHO AFRO. All national PHEOCs of the 47 member states in the region were invited; of these, 36 member states confirmed their participation in the exercise.
This article aims to document the key strengths, areas for improvement, and recommendations from the third regional functional exercise, in order to contribute to improving future exercises and strengthening emergency response capability in the region.
Management and Conduct of the Exercise
Exercise Objectives
The functional simulation exercise took place on December 6 and 7, 2022. Evaluation of the response actions undertaken by participating PHEOCs during the exercise were an integral part of the planning process to identify strengths and areas for improvement in future exercises. Twenty-two “injects” (scenario events) were developed to initiate specific responses by the participating PHEOCs against the simulated EVD (Sudan-type) outbreak scenario.
Exercise objectives were developed based on the 4 core components of a PHEOC including (1) the legal framework, plans, and procedures; (2) skilled human resources; (3) information systems and data standards; and (4) communication technology and physical infrastructure.
11
The objectives of the exercise were to:
Test the existence of legal instruments to enable the PHEOC to operate Assess the operationalization of plans and procedures including the implementation of an IMS in participating member state PHEOCs Familiarize staff with PHEOC technologies (telecommunication and information systems) and test them under realistic operational conditions Test information management (both event-specific and operational information) capability for decisionmaking Test the capabilities and capacities of the PHEOC to coordinate and collaborate with other responders to health events Define and document response linkages with national emergency management authorities and other sectors Test the capability of cross-border communication and information-sharing between PHEOCs in the event of a public health emergency
Exercise Management
A team representing key partners supporting PHEOC implementation in the African Region was established to manage the exercise, and a simulation exercise coordination cell (SimCell) was physically set up at the WHO AFRO Strategic Health Operations Centre in Brazzaville, Republic of the Congo.
A master scenario events list and the EVD (Sudan-type) outbreak scenario were developed to direct the exercise’s timeline of events. The master scenario events list, participant and evaluator guides, and comprehensive injects were developed in English and translated into French and Portuguese. Preexercise virtual briefing sessions in English and French were provided to the country-level controllers and evaluators drawn from WHO country offices, Africa CDC, West African Health Organization, Regional Center for Surveillance and Disease Control, UK Health Security Agency, US CDC, Robert Koch Institute, and African Field Epidemiology Network. In addition, the preexercise virtual briefing sessions focused on participant expectations and roles, which participants received on December 5, 2022, in English and French.
For the duration of the simulation exercises, an exercise controller was appointed to each national PHEOC, in addition to physical and virtual evaluators who were appointed to each member state to record actions taken. All exercise-related email communication between SimCell and participating PHEOCs was managed through a single point of contact via email. A SimCell WhatsApp group was also used to communicate between SimCell and exercise controllers and to distribute the exercise injects. A recurring Zoom call was established between the in-person and virtual exercise management teams.
Methods
Exercise Coordination and Communication
An exercise management team was established to lead the exercise (Figure), consisting of a lead controller, a SimCell, regional-level evaluators and controllers, and national-level evaluators and controllers. A physical SimCell was set up in a room at the WHO AFRO Strategic Health Operations Centre in Brazzaville, Republic of the Congo, with team members from WHO headquarters, Africa CDC headquarters, UK Health Security Agency, and Robert Koch Institute participating virtually.
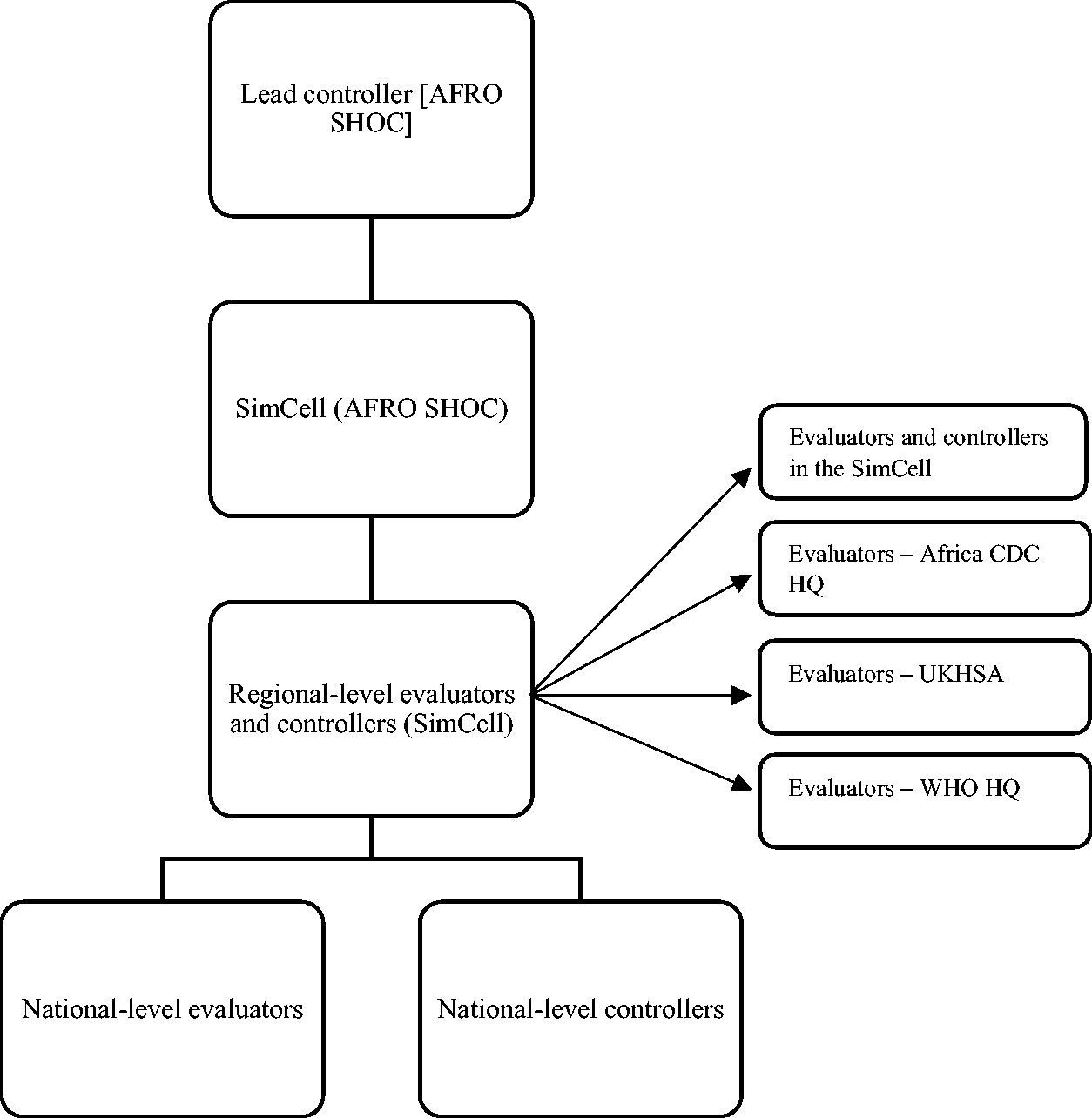
Simulation exercise management team. Abbreviations: AFRO, Regional Office for Africa; Africa CDC, Africa Centres for Disease Control and Prevention; HQ, headquarters; SHOC, Strategic Health Operations Centre; SimCell, simulation exercise coordination cell; UKHSA, UK Health Security Agency; WHO, World Health Organization.
Country Evaluator and Participant Participation
Of the 47 WHO AFRO member states, evaluators from 36 (77%) countries participated in the exercise. Of those 36 countries, evaluators from only 30 countries completed the required evaluation checklists and reports. More than 1,000 participants with various professional backgrounds from diverse government sectors and ministries, nongovernment sectors, and partners joined the exercise including experts from ministries of health, disaster management agencies, ministries of agriculture, ministries of environment, ministries of defense, and key partners involved in emergency management (eg, WHO, Africa CDC). Of those participants, 461 completed a postexercise survey.
Data Collection Process
Country Evaluator Feedback
A checklist of key parameters for measuring achievement of the exercise objectives was developed and shared with country-level evaluators who used it to assess actions taken in response to the injects and then compiled a report with their feedback. Evaluators shared their reports and completed checklists with the regional exercise management team.
Participant Feedback
A participant postexercise survey was administered online in both English and French (see Supplementary Table S1, www.liebertpub.com/doi/suppl/10.1089/hs.2023.0104). Participants were asked to provide open-ended feedback on strengths, areas for improvement, and recommendations to address the gaps.
In addition, participants were asked to rate the following 7 statements (on a Likert scale of 1 to 5, with 1 being “strongly disagree” and 5 “strongly agree”):
The exercise was well structured and organized. The scenario was realistic. The briefing before the exercise was useful and prepared me for the exercise. The exercise allowed us to test our response plans and systems. The exercise improved my understanding of my role and function during an emergency response. The exercise helped me to identify some of my strengths as well as some of the gaps in my understanding of response systems, plans, and procedures. At the end of the exercise, I think we are better prepared for a health emergency.
Debriefing Session
At the end of the exercise, each participating country conducted a hot-wash briefing/debriefing facilitated by the in-country evaluators and controllers to review the participants’ feedback. Evaluators collated the feedback in their report and submitted it to the regional exercise management team. In addition, the exercise management team conducted virtual debriefings with participants, evaluators, and controllers to discuss their perspectives on the exercise. The debriefings reflected on the exercise outcome and drew out strengths, areas for improvement, and recommendations to improve future exercises.
Data Analysis
Descriptive analysis was conducted to summarize quantitative data, and thematic analysis was used to describe the strengths, areas for improvement, and recommendations drawn from the exercise.
Ethics Statement
Because this review did not involve research with patients or individuals, it did not require institutional ethical review approval. Data were anonymized and no personal information was included.
Results
Country Evaluations
Of the 36 countries that took part in the exercise, 30 (83%) completed evaluation checklists and reports, which they shared with the regional exercise management team. The evaluation reports focused on key actions taken in response to exercise injects, which are summarized below by thematic area.
Legal Framework for the PHEOC
PHEOCs received an inject in the form of a request from a health sector minister to test the presence of a legal framework. A legal framework is critical because it provides a PHEOC with an official mandate that defines roles and responsibilities, objectives, authority, and process for timely decisionmaking and availing resources throughout the emergency management. The inject took into consideration the declaration of an EVD outbreak as a public health emergency of international concern, which urges multisectoral coordination and communication at all levels. Feedback from evaluators showed that 17 (57%) PHEOCs demonstrated the existence of a legal framework that defines mandates and responsibilities for all relevant stakeholders, while 7 PHEOCs acknowledged the partial existence of a legal framework that provides limited mandates for its operationalization.
Operationalization of Plans and Procedures
Plans and procedures are key components of a PHEOC, and many different types are included under an overarching national health emergency response plan. These plans describe PHEOC operations and management, response coordination systems, activation processes, information management, communication, and so on.
As depicted in Table 1, of the 30 countries that provided feedback, 21 (70%) reported that their PHEOC was in watch mode to monitor public health risks. An event monitoring or event-based surveillance system was intensified in 20 (67%) PHEOCs when the EVD outbreak spread across countries in the region. In addition, 14 (47%) PHEOCs disseminated spot reports (SPOTREPs) to brief the leadership and relevant stakeholders on potential risks that might require activation and coordinated response. Based on the risk assessment findings, 14 (47%) PHEOCs were able to move to an alert mode as the subsequent mode of operation and implemented activation procedures, activation authority, and activation levels. In terms of IHR notification, 17 (57%) countries notified the WHO AFRO IHR focal point through their national IHR focal point when they detected an EVD case in their territory based on the injects. Twenty (67%) of the PHEOCs reported the existence of a PHEOC handbook and other procedures to guide the emergency management process in their respective PHEOCs. Only 5 (16%) PHEOCs reported operationalization of their business continuity plan to ensure continuity of operations following the damage of their primary PHEOC. PHEOCs are expected to produce an incident action plan (IAP) to guide response activities by objectives; a key component of an IAP is an IMS that defines the response structure and individuals assigned to each function. It was found that 17 (57%) PHEOCs developed an IAP and 19 (63%) PHEOCs (including the 17 PHEOCs that developed an IAP with 2 other PHEOCs) developed an IMS.
Survey of Member States on Testing of Plans, Procedures, and Incident Management Systems, African Region, December 2022 (N=30)
Abbreviations: IAP, incident action plan; IMS, incident management system; PHEOC, public health emergency operations center; SITREP, situation report; SPOTREP, spot report.
Multisectoral Coordination
Management of public health emergencies, including disease outbreaks (eg, EVD), demands interventions beyond the health sector and requires multisectoral coordination with relevant stakeholders at all levels. Assigning stakeholders based on their technical capacity under the IMS is crucial to ensuring coordinated emergency management. Multisectoral coordination also helps leverage knowledge, expertise, and resources, enabling all stakeholders to benefit from combined and diverse strengths toward a common goal.
This capability was tested during the exercise. Of the 30 countries that provided feedback, 15 (50%) reported that a liaison was delegated in the IMS to serve as a point of contact for coordination, communication, and information sharing with national emergency management authorities, relevant sectors, and other stakeholders including partners. Furthermore, 12 (40%) PHEOCs had representation from key stakeholders outside the health sector to support response efforts through the established IMS. Key stakeholders included actors supporting emergency management efforts, such as disaster management agencies, ministries of agriculture, ministries of defense, ministries of environment, and partners (eg, WHO, Africa CDC, US CDC). In half of the PHEOCs (n=15, 50%), a procedure for communication, coordination, and information-sharing was established to guide the various actors. Furthermore, 14 (46%) PHEOCs responded to requests from their respective heads of state by confirming that a coordination mechanism with the national disaster management authority was in place.
Information Management for Decisionmaking
Another key capability for PHEOCs is information gathering and analysis to support decisionmaking and to provide MOH senior management and other relevant stakeholders with timely situational updates. PHEOCs were expected to respond to an inject regarding a request from their respective heads of state, and 16 (53%) of the PHEOCs did so. The 16 PHEOCs also developed a request for assistance (eg, human resources, financial, logistics) from international partners and donors in regard to the evolving EVD outbreak in their regions.
Cross-Border Collaboration and Communication
Cross-border collaboration and communication, including the timely exchange of information and situational updates, is critical for effective emergency management. PHEOCs serve as central communication points for coordinating and sharing updates with neighboring countries and beyond. Countries were divided into 4 groups, based on their subregional locations, and were tested on their capability for cross-border collaboration and information sharing between national PHEOCs. As a result, 18 (60%) countries were able to share EVD epidemiological situation and response intervention updates with PHEOCs in their respective subregions via emails and direct phone calls, while 16 (53%) countries sent a request to neighboring countries inquiring about specific EVD outbreak information.
PHEOC Telecommunication Systems
Telecommunication systems (audio and video) are key to helping PHEOCs communicate with relevant stakeholders at regional and international levels to provide updates and request resources. During the exercise, telecommunication systems of the national PHEOCs were tested by allowing PHEOCs to call the WHO AFRO Strategic Health Operations Centre room using its dedicated landline telephone. It was observed that 17 (57%) PHEOCs called and provided situational updates. In testing the PHEOCs’ video conferencing facility, 23 (77%) PHEOCs made a video call to the Africa CDC emergency operations center using a Zoom link.
Participant Feedback
More than 95% of the 461 participants who responded to the postexercise survey agreed with the affirmative responses to the questions. In response to the question about whether the prebriefing session was useful and prepared them for the exercise, 85% moderately agreed, agreed, or strongly agreed, while 14% disagreed or strongly disagreed (1% did not answer the question). In response to a question about whether the exercise helped them identify some strengths and an understanding of existing systems, plans, and procedures, 422 (91%) responded affirmatively (Table 2).
Participant Responses to Postexercise Survey, African Region, December 2022 (N=461)
In addition to rating 7 statements on a Likert scale, participants were asked to respond to open-ended questions by listing the exercise’s key strengths, areas for improvement, and recommendations to address gaps. Table 3 provides a summary of these responses.
Strengths and Areas for Improvement as Identified by the Regional SimEx Participants, African Region, December 2022
Abbreviations: PHEOC, public health emergency operations center; SimCell, simulation exercise coordination cell.
Discussion
This review presents key findings from the third regional functional exercise conducted from December 6 to 7, 2022, involving participants representing PHEOCs of WHO African Region member states. The exercise aimed to assess the functionality of national PHEOCs in the region during an EVD (Sudan-type) outbreak scenario. More specifically, it was conducted to document key strengths and areas for improvement based on actions undertaken in response to exercise injects, as well as recommendations to further strengthen the public health emergency management capabilities of national PHEOCs in the region.
A functional exercise, typically conducted from an emergency operation center with staff in tactical and strategic command roles, helps to identify strengths and areas for improvement in emergency response policy, plans, and procedures.9,12 It is critical to review and assess any actions taken as part of a public health response to capitalize on best practices, identify areas and required actions for improvement, and promote individual and collective learning. 8
Debriefing sessions play an important role in identifying lessons learned from real events and exercises, and recommendations and actions that lead to effective interventions are necessary. 13 After the end of the exercise, a debriefing was held with participants, during which evaluators from all participating countries identified strengths, areas for improvement, and recommendations to improve similar exercises in the future. During the debriefing session, some of the strengths identified were the presence of a PHEOC to engage with various stakeholders, multisectoral involvement, the availability of emergency management documents, and effective coordination and transmission of exercise-related information from the exercise SimCell. Areas for improvement included the timing of the exercise, which was organized at the end of the year and affected the ability of some stakeholders to participate due to other competing activities, shortcomings in the evaluators’ comprehension of how to conduct functional exercises, and participant knowledge gaps, particularly among those from outside the health sector. The management team of the regional simulation exercise and and the participants recommended to test the PHEOC’s functionality and build core competencies by organizing at least 1 functional simulation exercise each year (early or midyear) at regional and national levels. They also recommended to train country-level evaluators in the design and execution of simulation exercises, hold more preexercise briefing sessions at the regional and national levels, and provide regular orientation to surge staff on key existing PHEOC policies, plans, and procedures.
The existence of a legal framework provides the PHEOC with a mandate to operate as a response coordination hub with defined objectives, stakeholder roles and responsibilities, and funding mechanisms.3,14,15 Approximately half of the PHEOCs participating in the exercise recognized the importance of having a legal framework, which helped them clarify the roles and responsibilities of the various stakeholders, define functions of the PHEOC including timely decisionmaking, and mobilize resources (eg, response personnel, logistics, funding). As mentioned by some PHEOCs, the lack of an approved legal framework affected the rapid assignment of stakeholders and staff to the IMS because stakeholder roles and responsibilities had not be defined, which affected the mobilization of resources needed for the response and decisionmaking process. During the exercise, half of the PHEOCs were able to test their existing emergency policy, plans, and procedures.
To provide effective support in the event of a public health emergency, staff must be aware of their responsibilities during response operations and know how to work under the IMS. Over 90% of the participants reported that the exercise had improved their understanding of their roles during an emergency response. This finding is in agreement with the findings of studies conducted by Biddinger et al, 16 Emery et al, 17 Perry, 18 and Bartley et al. 19 Many participants also reported that the exercise had improved their understanding of current emergency management systems, plans, and procedures, consistent with previous research showing that functional exercises help participants better understand emergency plans and response roles. 8
Cross-border communication is critical for effective emergency preparedness and response. More than half of the countries involved in the exercise demonstrated the availability of information technology to facilitate real-time information sharing with neighboring countries. They found it essential to maintain contact details of key PHEOC and emergency management focal points to facilitate information and communication sharing.
WHO has recommended that PHEOCs should operate at 3 levels: watch, alert, and response. They should constantly be in watch mode to monitor potential public health concerns even if they are activated to direct response activities. A PHEOC should be able to conduct risk assessments to decide whether the level of activities should be heightened, resulting in alert or response modes. It was discovered that two-thirds of the PHEOCs had a watch mode system for monitoring health threats on a routine basis, whereas one-third had no such services because they only coordinate response activities when a public health emergency occurs. When the EVD outbreak scenario spread across countries in the region, about two-thirds of PHEOCs intensified their event monitoring system without conducting a risk assessment to determine the level of threat to their country, and only half of the PHEOCs were able to move to an alert mode and intensify their event monitoring guided by the risk assessment findings.
Most of the response rates to individual questions in this exercise were found to be not more than 70%. Findings from the regional PHEOC implementation status in the WHO African Region also indicated that about 70% of PHEOCs in the region have not met the minimum requirements to have fully functional PHEOCs. 20 Synergized efforts are underway to support member states to have fully functional PHEOCs in the coming years.
The management team of the regional simulation exercises described in this article recommended planning, funding, and conducting regular simulation exercises at regional and national levels at least once a year. Such exercises should aim to assess the existing operational capacities and capabilities of PHEOCs and their state of readiness to effectively support response to potential public health threats.
One of the limitations identified was that half of the participants did not respond to the online postexercise survey, which may have influenced the true picture of the level of understanding of the exercise. Furthermore, the lack of well-documented findings from prior regional exercises hampered comparisons of achievements with present results.
Conclusion
The regional functional exercise was well structured and used realistic scenarios designed to initiate response actions by the participating PHEOCs. Additionally, the exercise met its objectives and offered an opportunity to meaningfully test the scenario. Key lessons drawn from the exercise were the importance of involving multisectoral and multidisciplinary experts, ensuring good coordination, effectively facilitating the exercise, and developing realistic scenarios. However, one-third of participants emphasized that the preexercise briefing session did not prepare them well for the exercise. Furthermore, areas for improvement included the timing of the exercise at the end of the year, which affected the ability of stakeholders to participate due to other competing priorities, and shortcomings in the evaluators’ comprehension of exercise planning and conduct. We recommend that regional and national functional exercises be conducted at least once a year, in the early or midyear, and training should be provided to identified in-country evaluators and controllers drawn from various stakeholders. In addition, at least 2 or 3 briefing sessions should be organized at the national level by their respective facilitators. An improvement plan should also be developed at the national and regional levels to ensure identified strengths are maintained and gaps are addressed to improve response capability in the future.
Footnotes
Acknowledgments
We would like to thank all participants, controllers, and evaluators from participating countries for their active engagement and completion of the exercise checklist and survey.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.