
Abstract
The New York City Department of Health and Mental Hygiene and the Greater New York Hospital Association held 3 workshops and 2 follow-up meetings with hospital emergency managers and colleagues to determine hospitals’ response actions to a scenario of a 10-kiloton improvised nuclear device detonation. The scenario incorporated 3 zones of damage (moderate, light, and beyond damage zones) and covered the period of 0 to 72 hours postdetonation divided into 3 24-hour operational periods. The Joint Commission’s critical emergency areas were used to determine the objectives and response actions that would be initiated. The response actions were motivated by the resource-constrained clinical situation demanding the rationing of supplies and the application of crisis standards of care. Actions included seeking situational awareness concerning the incident and maintaining a safe and secure working environment. Due to the severance of the medical material supply chain and the levels of destruction, inner damage zone hospitals considered termination of operations and evacuation. Beyond damage zone hospitals prepared to receive patients from the inner damage zone facilities. However, these plans would not be fully successful without a significant amount of logistical aid from outside local or regional partners. Four broad planning areas with outside partners emerged from the follow-up meetings: staffing, resupply, communications/situational awareness, and guidance. Dwindling resources will require a plan for rationing and implementing crisis standards of care and maintaining staff morale. Communications efforts need to include a formalized plan with scheduled broadcast times and identified sources of authority for hospitals to acquire and disseminate information. Information about fallout radiation, instructions for measuring contamination, and guidance for triaging and diagnosing acute radiation sickness are also needed.
Introduction
I
As was seen with the first wartime nuclear detonations in Hiroshima and Nagasaki, Japan, hospitals that survive a detonation become islands of care until further medical resources can be made available. However, depending on their location relative to ground zero, some hospitals may suffer extreme damage, which would severely hamper their operations. Other hospitals may escape damage or experience casualties and damage light enough to continue functioning. One must also consider the larger operating environment, where water, electricity, food, and transportation may be interrupted by the detonation, turned off by government order, or terminated by damage and radioactive fallout. The authors sought to determine the type of support that hospital leadership would attempt to obtain for their patients and staff and whether they would consider postdetonation patients. Therefore, a workshop series was designed to solicit hospital emergency response actions and to provide some basis for health system-level planning for such a crisis.
At the conclusion of the workshops, a summit meeting and a subsequent executive meeting were held to summarize the workshop findings and the requests that hospital emergency experts identified as needing government emergency planners’ attention.
Workshops to Discuss INDetonation Response
Planning and hospital emergency support specialists at the New York City Department of Health and Mental Hygiene (hereafter NYC Health Department) initiated this project primarily because, at the time, hospitals had not been fully considered in national response planning for a nuclear detonation. Documentation of hospitals’ postdetonation actions would be needed for local and regional planners to factor hospitals into an IND detonation response. Therefore, to capture these postdetonation actions and needs, emergency managers from hospitals and health systems with facilities inside and outside of New York City were asked to attend a series of facilitated workshops. The invitees were chosen using the membership information of the Greater New York Hospital Association (GNYHA). † GNYHA is a trade association representing more than 160 hospitals within health systems in the states of Connecticut, New Jersey, New York, and Rhode Island. The extensive effects of a nuclear detonation, particularly fallout that can spread hundreds of miles, was a primary reason for the necessity to call upon hospitals outside of New York City. Another reason was the presumed exodus of a large population from the affected area, which could impact suburban hospital operations.
The hospital representatives developed response actions during the workshops based on the nuclear weapon scenario detailed in the next section. Discussions were then facilitated by GNYHA and NYC Health Department representatives. The workshop is described in more detail in the Workshop Organization section.
Workshop Scenario
The effects from nuclear weapons include light, heat, blast, ionizing radiation, and fallout. Table 1 provides a brief summary of the effects of a 10-kiloton daytime surface burst scenario presented to workshop participants. 2 Although all effects are important, the workshop facilitators emphasized blast damage, fallout, and roadway blockages caused by flash blindness and building collapses, all of which obstruct the public and first responders’ access to hospitals to varying extents.
Summary of Nuclear Detonation Effects Considered in the Workshop Scenario
Abbreviations: PPE, personal protective equipment; R, roentgen.
The location of ground zero was deemphasized in favor of descriptions of the damage areas: severe damage zone, oderate damage zone (MDZ), light damage zone (LDZ), and beyond damage zone (BDZ). We were interested in response actions under no-notice and limited information conditions. Given the substantial level of destruction and fatalities anticipated in the severe damage zone, actions in that zone were not discussed. Instead, the workshop proceedings focused on actions that would be initiated in facilities located in the other zones during 3 distinct time periods: 0 to 24 hours, 24 to 48 hours, and 48 to 72 hours postdetonation.
It was postulated that the weapon would produce radioactive fallout but that the wind directions were unknown—a real-life condition likely to be true. Therefore, the workshop participants made the conservative assumption that their hospitals were located in the dangerous fallout zone ‡ for at least 24 hours. Participants were told that fallout may be observed and the associated radiation may be measured. They were asked to consider the potential radiation exposure of patients and staff despite the shielding offered by the hospital building. They were apprised of the widespread damage to surrounding infrastructure that would instantaneously create a resource-poor environment. The disruptions to power, communications, and transportation are summarized in Table 2. The incapacitation of transportation, both public and private, was emphasized because of the ramifications to the medical supply chain and subsequent patient care. Radiation exposure, acute radiation syndrome (ARS), and other effects, such as flash blindness, were described to them for contextual completeness. Participants were told that prompt fatalities for a workday summertime detonation of a 10-kiloton weapon in New York City’s Times Square would be in the hundreds of thousands with additional casualties if people do not shelter from fallout exposure. 3 The participants were also made aware that federal assistance was not expected to arrive for 72 hours (Table 3). 4 Until then, and perhaps longer, they would have to function independently of assistance.
Summary of the Projected Effects of a Nuclear Detonation on NYC Infrastructure
Abbreviations: BDZ, beyond damage zone; LDZ, light damage zone; MDZ, moderate damage zone; NYC, New York City.
Summary of Expected Local and Federal Responses to a Nuclear Detonation
The Emergency Support Function 6—Mass Care, Emergency Assistance, Housing, and Human Services—led by the US Department of Homeland Security/Federal Emergency Management Agency and the American Red Cross coordinates and provides life-sustaining resources, essential services, and statutory programs when the needs of disaster survivors exceed local, state, tribal, territorial, and insular area government capabilities.
Abbreviations: CDC, US Centers for Disease Control and Prevention; HHS, US Department of Health and Human Services; MDZ, moderate damage zone; NYC, New York City.
Workshop Organization
A preliminary meeting was held to introduce the workshop objectives and to discuss the postdetonation environment. Workshop discussion topics were formulated based on The Joint Commission’s 6 critical areas for emergency response plus a section on incident command. 5 This framework was chosen because of the participants’ familiarity with these emergency planning considerations. Table 4 illustrates how the zones of destruction and the 3 periods of time postdetonation were used to differentiate response priorities for each of the critical areas. Responses were collected by NYC Health Department and GNYHA notetakers, then compiled and summarized by GNYHA staff for review by the workshop organizers.
Workshop Discussion Matrix
The 3 workshops were held in small groups of approximately a dozen representatives to consider and discuss their responses to The Joint Commission’s critical areas for a particular damage zone. Typically, each workshop consisted of 3 sessions, with representatives from hospitals from each zone discussing response initiatives for 90 minutes per session. Actions were obtained for 3 time periods postdetonation (0 to 24 hours, 24 to 48 hours, and 48 to 72 hours), 1 time period per workshop. At a subsequent summit meeting, participants summarized and validated their proposed emergency actions. The participants were separated into groups charged with reviewing response actions for 2 or 3 Joint Commission critical areas.
Emergency management personnel made up most of the workshop attendees, supplemented occasionally by facility engineers. Representatives from key response agencies and organizations also participated, including those from the Fire Department of the City of New York and the Radiation Injury Treatment Network. Up to 25 hospitals and/or networks participated per workshop. The workshops were facilitated by the authors of this article and a third partner from the US Centers for Disease Control and Prevention, who had a medical background (see Acknowledgments).
Following the workshops, a summit meeting was held to finalize the workshop findings. This included agreeing on the response actions for each critical area for each 24-hour operational period postdetonation and the overall posture of hospitals in each damage zone. This was achieved using a breakout session comprising 7 separate work groups, 1 for each of the 6 emergency response categories plus a category designated for incident command. GNYHA outlined the results in hospital key response actions grids6,7 that break down the response actions by topic (critical area) and by damage zone (ie, the same findings are presented in 2 formats). The workshop and summit meeting discussions made apparent that some actions would greatly benefit the hospital response if taken before the incident. GNYHA’s Hospital Key Response Actions by Zone report indicates these findings in a separate column. 7
Response Actions Identified by Type
The response actions are summarized in the timelines depicted in Figures 1 through 8. The actions of the MDZ and LDZ facilities, often similar but occasionally with important differences, are grouped in the upper portion of the figures, and the BDZ hospital responses are placed in the lower portion. In some cases, actions are common to all 3 zones across 2 or 3 operational periods; in other cases, the actions may diverge. These are so indicated in the figures.

Incident command initiatives – 0 to 72 hours. Abbreviations: BDZ, beyond damage zone; EOC, emergency operations center; LDZ, light damage zone; MDZ, moderate damage zone; RTR, radiation triage, treat, and transport.
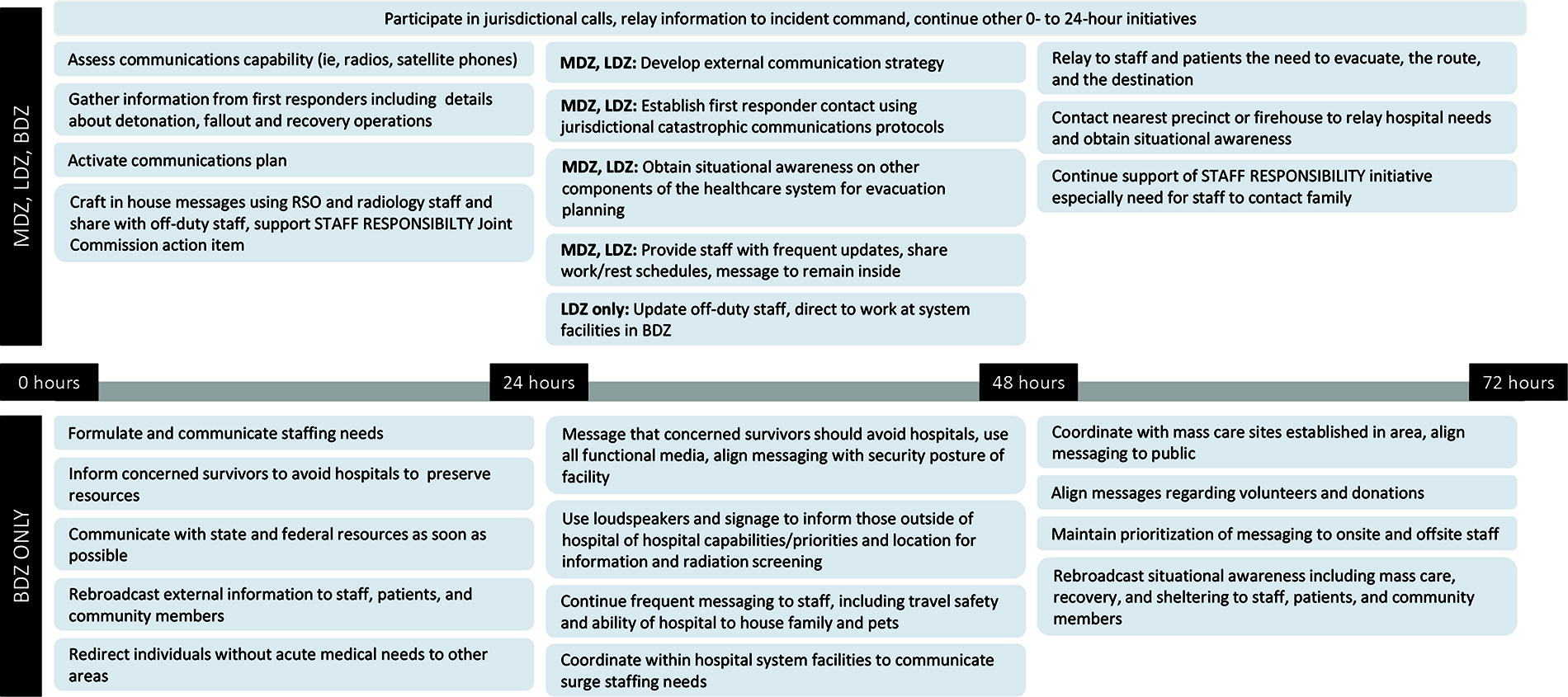
Communications initiatives – 0 to 72 hours. Abbreviations: BDZ, beyond damage zone; LDZ, light damage zone; MDZ, moderate damage zone; RSO, radiation safety officer; JC, The Joint Commission.
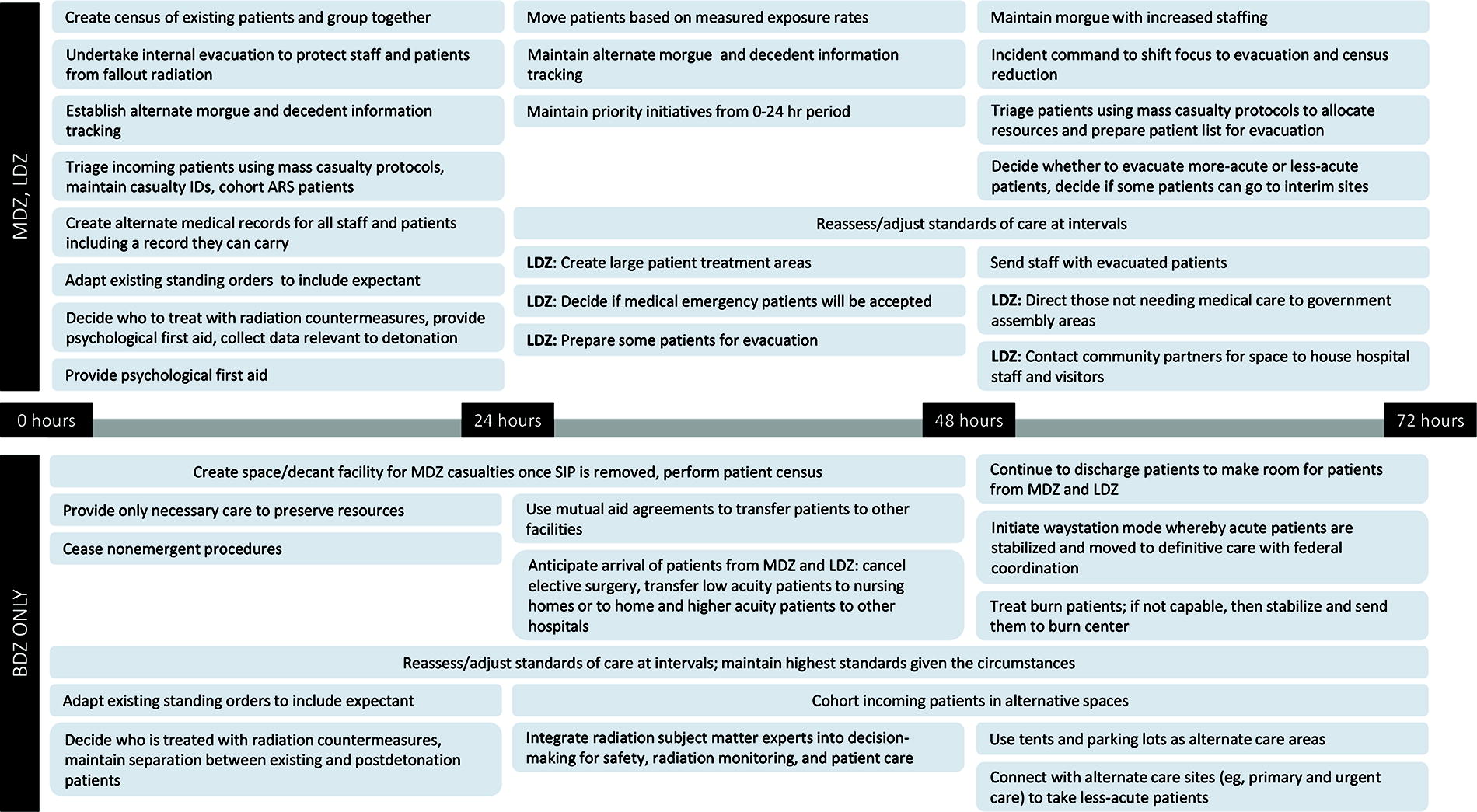
Patient care and clinical support initiatives – 0 to 72 hours. Abbreviations: ARS, acute radiation syndrome; BDZ, beyond damage zone; LDZ, light damage zone; MDZ, moderate damage zone; SIP, shelter in place.

Resources and assets initiatives – 0 to 72 hours. Abbreviations: BDZ, beyond damage zone; LDZ, light damage zone; MDZ, moderate damage zone.
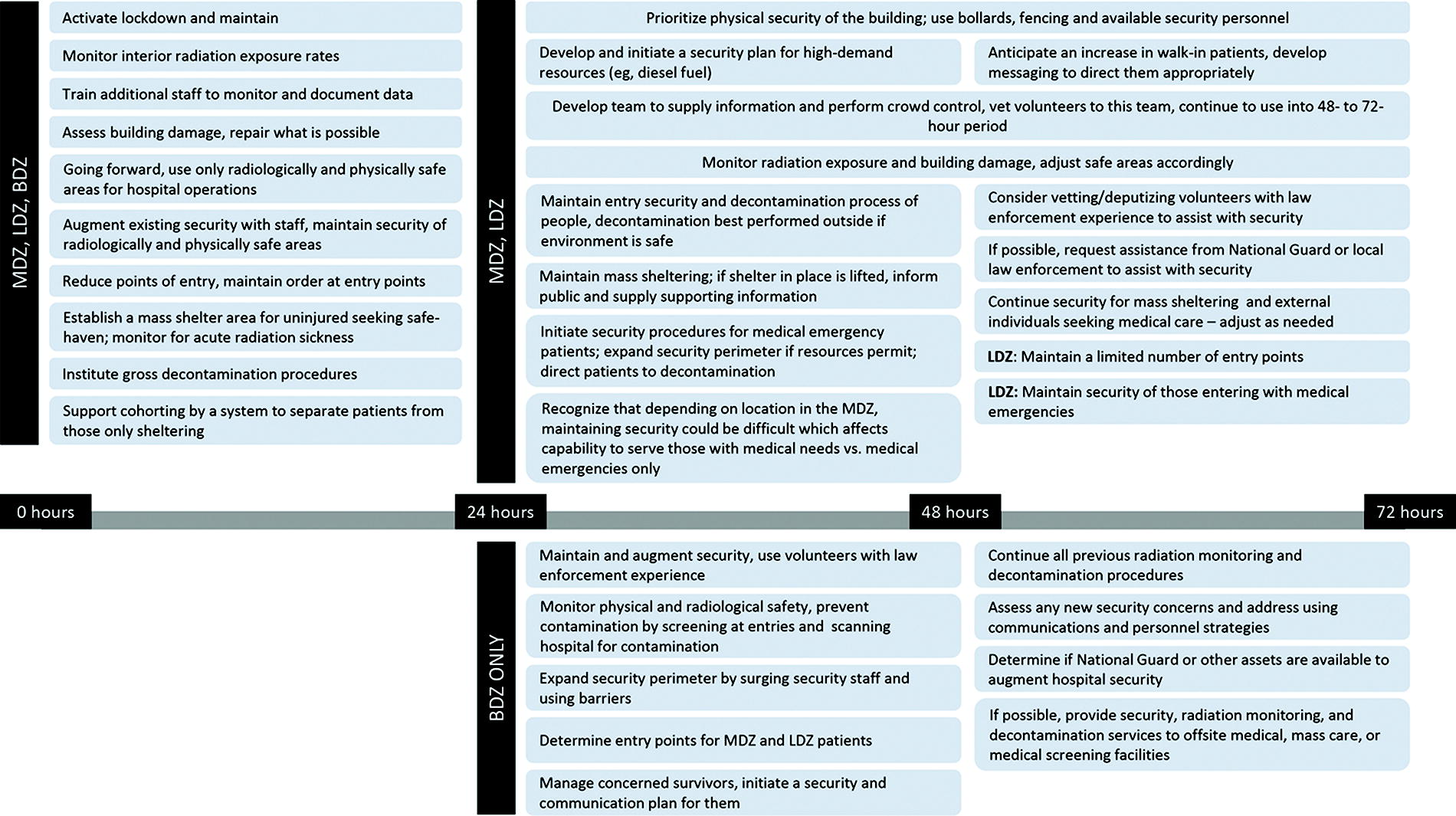
Safety and security initiatives – 0 to 72 hours. Abbreviations: BDZ, beyond damage zone; LDZ, light damage zone; MDZ, moderate damage zone.
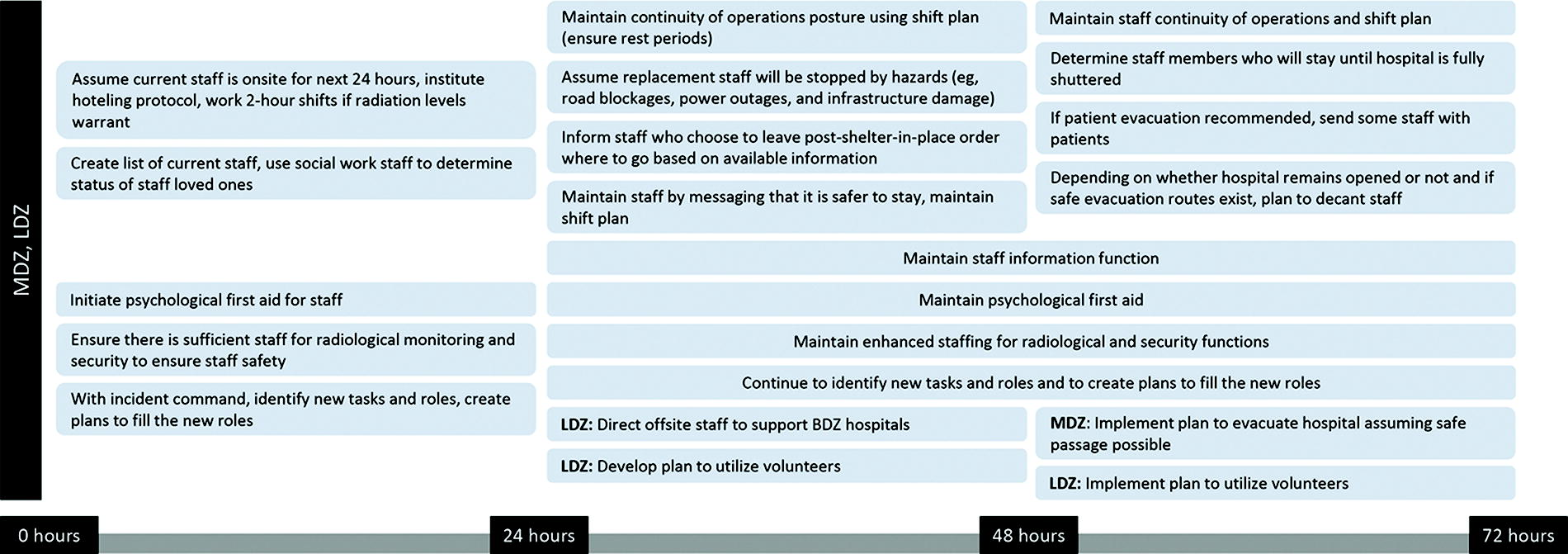
Staff care initiatives, part 1 – 0 to 72 hours. Abbreviations: BDZ, beyond damage zone; LDZ, light damage zone; MDZ, moderate damage zone.

Staff care initiatives, part 2 – 0 to 72 hours. Abbreviations: BDZ, beyond damage zone; LDZ, light damage zone; MDZ, moderate damage zone; SIP, shelter in place.

Utilities initiatives – 0 to 72 hours. Abbreviations: BDZ, beyond damage zone; HVAC, heating, ventilation, and air conditioning; LDZ, light damage zone; MDZ, moderate damage zone.
Workshop Findings
Outside Assistance Is Required
From the GNYHA hospital key actions, the overall postures of the hospitals by zone soon became apparent. The hospital emergency managers were constrained in their choices by the resource-poor conditions of the hospital, its potentially damaged infrastructure, and the hazardous outdoor environment.8,9
Given the constraints, the posture of hospitals in the MDZ was to assume that medical services would not be sustainable due to the infrastructure, security, and resource challenges. Hospitals in the LDZ may assume postures that are dependent on infrastructure damage. The inner LDZ hospitals may be forced to choose objectives similar to most MDZ hospitals, whereas those in the outer LDZ may act as way stations for both evacuated patients from the MDZ and those seeking medical attention from injuries caused by the detonation. Hospitals in the BDZ can also plan to manage survivors and accept transferred patients, but the medical supply chain must be in place.
Realizing that outside assistance was crucial to the success of hospital evacuation or continued operations, a summary of needed resources became the goal of the final executive meeting of workshop participants. The experts were divided into the following breakout groups: situational awareness and communications, staffing, and supplies and guidance. The resource needs agreed upon were organized into an acute care needs report. 10 The highlights of that report and additional material are summarized next.
Acute Care Needs Identified
Distilling the acute care needs in this catastrophe is not an easy task. Prioritizing preincident federal assistance is difficult as each need is predicated on the zone of destruction, damage actually done, and the environmental circumstances. Nevertheless, there are some common threads, which are summarized in Table 5. These needs can be broadly organized into 4 categories:
Hospital Acute Care Needs and Actions in the Aftermath of a Nuclear Detonation
The Interagency Modeling and Atmospheric Assessment Center is the coordinating and disseminating body for federally produced dispersion models for nuclear detonation fallout. An initial fallout plume map can be transmitted within an hour or so of detonation based on local meteorology; however, this may have a high degree of uncertainty and would not be available to the general public, including hospitals. Therefore, hospitals should assume they are in the fallout plume until advised otherwise.
Abbreviations: ARS, acute radiation syndrome; BDZ, beyond damage zone; CSC, crisis standards of care; IC, incident command; IND, improvised nuclear device; LDZ, light damage zone; MDZ, moderate damage zone; REMM, Radiation Emergency Medical Management; SIP, shelter in place.
Crisis Standards of Care
Crisis standards of care (CSC) were not discussed in depth in the workshops. They were mentioned only as being necessary for the response. CSC development in the United States is a state function that has produced a wide variety of CSC plans, not all of which appear to be adequate. Research at the NYC Health Department indicates that many do not address such issues as fatality management (78%), mental or behavioral health specifications (60%), or interstate/intrastate coordination (88%). 14 Therefore, until some unifying effort is made, CSC is likely to remain a patchwork of guidelines that, depending on geography, will not cover every contingency in a severe emergency. In addition, there is the problem of initiating CSC—a decision not easily made because of the high-risk consequences to patients and staff. However, in the case of an IND, the decision will not have to be made by a state health department and transmitted to the hospitals. The effects of the IND will make the decision obvious to healthcare providers almost immediately.
Medical Operations Coordination Centers
The workshops preceded experience with medical operations coordination centers (MOCCs) 15 ; consequently, participants did not consider them an operational asset. In mass casualty circumstances, a MOCC’s goal is to ensure patient load balancing across healthcare facilities and systems to provide the highest possible level of care for all patients before the need to transition to crisis measures. MOCCs help to promote a consistent standard of care and to apply healthcare assets equitably across a region, a state, or a healthcare coalition. MOCCs do this by directing secondary referrals to the most appropriate hospital, by providing a referral line for rapid placement of patients needing critical care, by providing consultation with specialty medical providers, and by convening hospitals for situational information, including current contingency measures. They have been proven to work effectively during the COVID-19 pandemic. In theory, MOCCs would be a useful hospital tool in an IND response due to the regional nature of the catastrophe.
Interestingly, some MOCC functions were echoed in the workshop participants’ response actions, as evidenced by their repeated need for situational awareness from in-network and out-of-network facilities. In addition, the concept of triaging for ARS and then transferring ARS patients to Radiation Injury Treatment Network hospitals (Table 3) is aligned with the MOCC concept. We can speculate that if the workshop were conducted now, the attempts at gathering situational awareness would be couched in the context of MOCCs. However, one cannot assume optimal functioning of a MOCC after an IND detonation. The communications infrastructure must be in place for MOCCs to be effective. In the BZD, where communications are more likely to be operational, MOCCs or a version thereof may function well enough to assign patients in need of specialty care to the proper hospitals—assuming that the damaged environmental and infrastructure circumstances permit transport.
Credentialing
Healthcare provider credentialing can be a slow process that may take months to accomplish. The surge in demand for healthcare professionals during the COVID-19 pandemic highlighted the need to speed up the process. This had to be done while maintaining the standards for provider credentialing set by such organizations as The Joint Commission and the Centers for Medicare and Medicaid Services. In the pandemic, it was necessary for hospitals to invoke their disaster plans in order for credentialing to be waived to allow physicians to work where they were most needed. The process is ordinarily complex with potential obstructions that range from incomplete to out-of-date healthcare provider data, including inaccurate provider contact, certification, or licensure information. The process includes, as a final step, review of credentialing applications by a credentialing committee. In an emergency situation, especially one as devastating as an IND, this process would not be adequate given the immediate need for physicians in receiving facilities. In the workshops, credentialing was identified as a problem but not discussed further as it was beyond the scope of the project. Since the COVID-19 pandemic, proposals have been made to reduce these inefficiencies, including development of a single national database for physician credentials 16 and adoption of a national physician license. Until that happens, credentialing will remain inadequate to respond to a pandemic crisis and, as assumed by the workshop participants, to an IND. Once again, waiving of the credentialing process will be necessary.
Hospitals in Jurisdictional Nuclear Detonation Emergency Planning
Whether in New York City, other large metropolitan areas, or smaller, less-populated cities, this scenario is likely to play out in the MDZ and the inner LDZ: detonation, hospital response actions as indicated in this article, the dwindling of supplies, and finally the consideration of hospital evacuation. Planning work performed in New York City since the workshops assumes that a self-initiated mass exodus of the public would simultaneously occur parallel to response efforts—a likely scenario in any IND incident. Therefore, we believe that the findings of the workshops and its subsequent meetings are applicable nationally. Wherever it makes sense to plan for an IND incident, hospitals should be considered. The planning should concentrate on the first 72 hours, a minimum of 24 hours of which will be needed to wait for fallout exposure rates to reduce to 10 roentgen per hour—still a high rate.
Hospitals should be prioritized because of their unique characteristics: their patients represent a vulnerable population that includes children, pregnant people, older adults, and those with functional needs. They are sources of invaluable medical talent that will be needed in the upcoming months and years of environmental and economic recovery. Lastly, they face rapidly diminishing medical resources with very high consequences for their clients.
Hospitals in inner damage zones will be faced with a high-stakes decision to evacuate hospital patients and staff into an environment fraught with multiple life-threatening hazards and little or no motorized transportation. It is, at best, a problematic calculus with a low probability of success. To increase the probability of saving as many patients and staff as possible, hospitals need to be included in a jurisdictional IND plan where potential assistance comes from outside the affected areas.
To assist with overall IND planning, federal partners have recently published planning guidance for the first 72 hours postdetonation. 4 This document may be one of the first federal planning guides to consider hospitals. It acknowledges that hospitals in the MDZ would have limited operational time and that LDZ hospitals should prepare to receive patients, both of which are in line with the findings of this article. It also states that the austere medical supply situation would warrant resupply of hospitals—another finding that was considered in our workshops. Furthermore, it recognizes that the loss of water and electricity will terminate hospital functions. Most importantly, this document reinforces that federal assistance will not arrive locally for at least 72 hours postdetonation.
The reality of collapsed buildings, vehicular accidents, and other street congestion, including the chaos of the predicted mass evacuation of the public, will make responder access to hospitals extremely challenging. Emergency planners can identify the sources of heavy equipment (and operators), which may come from sanitation departments located in nearby jurisdictions. The feasibility of roadway clearance to meet the stringent timeline for total hospital shutdown and potential evacuation may not be determined until the day of the incident.
Interagency planning with partners, such as local police and transportation departments, may help to predict probable public and hospital evacuation routes. Those discussions may also predict where radiation triage, treat, and transport sites 11 may arise and be supported to assist all evacuees. Of course, communications are absolutely key to coordinate such an effort.
As indicated earlier, communications should be made a priority in an effort to coordinate the resupply of some hospitals with medical equipment, medical staff, and other resources. The means to provide a survivable communications platform between hospitals and local or nearby jurisdictional authorities should be explored (an example program is shown in the Appendix of this paper, available at www.liebertpub.com/doi/suppl/10.1089/hs.2023.0106). The local National Guard is another key resource for this capability. As a potential model for other jurisdictions, consider that New York City maintains the Radiological Response and Recovery Committee for dirty bomb emergency response, from which a nuclear detonation work group was formed. This standing committee brings together hazardous materials and chemical, biological, radiological, and nuclear experts from the NYC fire, environmental protection, and emergency management departments, with other representation from the police, local Federal Bureau of Investigation office, New York State Metropolitan Transportation Authority, US Environmental Protection Agency Region 2, and New Jersey Environmental Protection. It provides a nucleus to build out further regional planning.
Conclusion
Although hospitals are mentioned in the federal 72-hour nuclear response guidance, 4 hospital emergency managers should not assume that a local or even a regional IND plan exists. An IND catastrophe may be perceived (quite rightly) as a “big city” challenge only. However, the extent of fallout, its dependence on meteorology, and the predicted evacuation of a damaged radioactive urban area create an unprecedented planning challenge for suburban areas and, in particular, for the BDZ receiving hospitals.
Hospitals can prepare for an IND catastrophe independently by recognizing and proactively acting on the findings in this article concerning the needs for just-in-time training on ARS and radiation detection by drawing on available online resources. These preparations can be done at little or no monetary cost by accessing the Radiation Emergency Medical Management website for the appropriate topics and storing the information as hard copies onsite in an appropriate location (eg, emergency operations center). Other preparation, such as training to properly use radiation detection equipment and dosimeters, can also be done almost cost-free except for time and effort.
The hospital emergency managers and other representatives who participated in the workshops treated the catastrophe scenario seriously, providing well-considered and thoughtful response actions designed to save or prolong the lives of patients and staff. The distinct impression was given that provided with situational awareness, preincident resources to recognize ARS, and the hope that assistance is arriving, many of the staff would act appropriately to save lives. Government emergency planners must consider hospitals in a crisis of this magnitude and support the varied response actions needed to save as many of their clients and staff as possible.
Footnotes
Acknowledgments
The authors would like to acknowledge Timothy Styles, MD, MPH, former medical director of the Bureau of Healthcare and Community Readiness at the NYC Health Department and career epidemiology field officer at the US Centers for Disease Control’s Center for Prevention and Response, now serving in the Division of Injury Compensation Programs of the US Health Resources and Services Administration. His insight and assistance with the planning and running of the workshops were invaluable as was his postworkshop analysis. Eliot Calhoun, formerly of New York City Emergency Management and now with the US Department of Homeland Security, provided valuable insight at the workshops concerning the response of New York City first responders to a terrorist-sponsored nuclear detonation. The authors are also appreciative of the time, consideration, and effort of all the hospital representatives at the initial meeting, the 3 workshops, and the 2 follow-up meetings. Patients and clinical staff are safer and well served by their expertise, which is rarely seen except when needed in a crisis. The authors are also grateful to our notetakers: Cory Pardo of the NYC Health Department and Samia McEachin and Ed Lieber, both of GNYHA, who accurately and deftly captured the creativity and skill expressed by the hospital representatives. We also acknowledge Maurice Zuniga of New York City Emergency Management for generously contributing a description of the New York City Emergency Radio Communication Program. Caroline Nguyen, director of the Chemical, Biological, Radiological, and Nuclear Unit in the NYC Health Department is thanked for her thoughtful review of this publication.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.