
Abstract
High-level isolation units (HLIUs) are facilities strategically outfitted to receive patients with suspected or confirmed high-consequence infectious diseases (HCIDs). Although most HCID outbreaks occur in low- and middle-income countries, global travel and migration and the deployment of healthcare workers to global outbreaks have led to the occurrence of HCIDs in high-income countries that requires the activation of an HLIU. Despite the existence of HLIUs worldwide, there has been little collaboration between units at the international level. This study reviews the results of a descriptive survey of global HLIUs conducted between December 2022 and February 2023. The purpose of the survey was to identify traits and attributes of global HLIU peers to determine commonalities and differences among the units, identify priorities for increased networking, and inform future activities among global partners. Findings from this survey demonstrate the array of similarities and differences among HLIUs across the globe, indicate potential areas of further investigation, and identify areas in which alignment could be improved and global standards could be created.
Background
H
HCID outbreaks typically emerge and reemerge in low- to middle-income countries; however, high-income countries can also have HCID cases that require the activation of a HLIU, as a result of global travel and migration, climate change, geopolitical factors, and the deployment of healthcare workers to global HCID outbreaks. The 2014-2016 EVD outbreak highlighted the value of HLIUs to both facilitate the repatriation of citizens and to enhance national preparedness for the rare event of an HCID case presenting in the United States. According to the US Centers for Disease Control and Prevention (CDC), the World Health Organization (WHO) has declared 6 public health emergencies of international concern since 2009. 4 More recently, WHO declared the following outbreaks as posing potential risks to international communities: the 2022 Lassa fever outbreak resulting in the activation of an HLIU in the United Kingdom 5 and the 2022 outbreaks of Sudan EVD in Uganda 6 and Marburg virus disease in Equatorial Guinea and Tanzania. 7
While HLIUs are established in many regions of the world, there are limited formalized platforms for interaction and collaboration among them. Previous publications have supported a call to action for global collaboration among HLIUs and those supporting the field of HCIDs. For example, Herstein et al suggested that increased collaboration among HLIUs may lead to “more synergistic working relationships” and increased advocacy for funding and general awareness about the important role HLIUs play in ensuring the public’s health and wellbeing. 8 Additionally, authors Xia and Yuan described the benefits of international collaboration as helping to harmonize HLIU requirements and standards, improve systems, exchange experience, and share resources such as training materials and other information. 9 Lastly, in an article advocating for collaboration among European units, Ippolito et al mentioned that the benefits of partnerships may also affect research in the sharing of “diagnostic protocols, samples, reagents, and personnel for training,” as well as the creation of new testing schema. 10
The National Emerging Special Pathogens Training and Education Center (NETEC) is a collaboration of 13 US-based HLIUs called Regional Emerging Special Pathogens Treatment Centers (RESPTCs).
11
NETEC was established in 2015 as a consortium of the 3 US institutions that cared for patients with EVD in 2014. It is funded by the US Department of Health and Human Services
In 2021, NETEC began to explore collaborations and establish relationships with global HLIUs. The International Partnerships and Programs (IPP) was added to NETEC’s portfolio with a mandate from funders for NETEC HLIUs to engage, learn, and exchange experiences with international peers. The work of IPP is focused on 2 main goals: building partnerships and sharing knowledge. As engagement among global HLIUs increases, NETEC needs a better understanding of the history, demographics, and key characteristics of HLIUs. In 2018, an HLIU survey was conducted at the International Workshop on High-Level Isolation, coorganized by NETEC and held in Washington, DC. 12 In 2022-2023, IPP conducted a survey to update and supplement the previous dataset and to identify traits and attributes of global HLIU peers to determine commonalities and differences among these units and priorities for increased networking and inform future activities among global partners. In this article, we review the results of the descriptive survey.
Methods
Participant Recruitment
Representatives from 36 international HLIUs were invited to complete the survey via email. The target population was determined based on existing NETEC relationships with international HLIUs and a landscape analysis performed by the NETEC International Work Group in 2021. Additionally, a majority of the surveyed cohort attended the 2018 workshop in Washington, DC. 12 Of the 36 global units invited, 31 completed the survey.
Survey Instrument and Analysis
A team of HLIU experts from the 13 US RESPTCs created and refined the online survey. The survey was sent to 3 international HLIU partners to review its relevancy and adaptability to non-US HLIU contexts. The final 42-question survey included multiple choice (ie, select all or select a single answer) and open-ended qualitative questions. The survey was divided into 5 categories: HLIU information, operational readiness and terminology, advocacy/sustainability, ongoing collaboration/coordination with other HLIUs, and best practices and challenges. The number of questions displayed to each participant was conditional on their prior responses. The survey was available in English only and the research team did not provide it in another language. The survey opened with a landing page that required participants to indicate whether their HLIU cared for patients with HCIDs. If they answered “yes,” they could complete the survey. Those who answered “no” were not allowed to complete the survey.
The survey was disseminated electronically via email to representatives from 36 international HLIUs via the Qualtrics platform (Qualtrics, Provo, UT) in December 2022. Two follow-up reminders were sent to nonresponding units before the survey closed in February 2023. Data were analyzed using descriptive statistics in Microsoft Excel.
Results
Participants
Thirty-one global units participated in the survey (86% participation rate), representing 4 continents and 16 countries. Of note, 2 HLIUs invited to complete the survey were not active at the time of survey dissemination and did not participate. The number of participating units represented as answering individual questions varied depending on applicability and the opportunity for participant preference to answer and are noted in text.
Definition of and Designation as an HLIU
Twenty units (65%) indicated that their country uses a specific definition for HLIUs. Some definitions included unspecified national mandates, whereas others outlined specific requirements; for example: “a unit where the care for patients with (suspected) viral hemorrhagic fever and other high-consequence infectious diseases (nonspecified) can be safely provided according to existing regulations,” and “a list of set criteria for training of staff, as well as technical details regarding ventilation, containment, PPE.” Notably, not all countries activate an HLIU for every HCID. For example, 1 country uses an HLIU for contact diseases only, such as viral hemorrhagic fevers (VHFs), and treats airborne diseases elsewhere. Conversely, when prompted to describe their definition, 1 respondent stated that a definition of an HLIU “cannot be described in 1 sentence, this would break the mould.”
A majority (n=23, 74%) of the HLIUs received designations from their federal governments, followed by local governments (n=18, 58%) and local health departments (n=12, 39%). Twenty-two (71%) responding units reported receiving HLIU designations from multiple authorities. Twenty-seven HLIUs (87%) reported that they were required to meet specific capabilities in order to maintain their designation.
Establishment and Location of HLIUs
Thirteen (43%) HLIUs out of 30 (1 did not respond to the question) were established before the 2014-2016 West Africa EVD epidemic. Of these, 11 are in Europe and 2 are in North America. An additional 14 units (47%) were established in 2014-2019, and 3 units (10%) were developed after the declaration of the COVID-19 pandemic in 2020. Participating HLIUs (N=31) are located in both dedicated units activated only for HCID cases (n=13, 42%) and flexible-use units used daily for non-HCID cases when not activated (n=18, 58%). Across all units, 118 beds are available for treating VHFs (average 3.8, median 2) and 197 beds are available for treating respiratory diseases (average 6.3, median 6). All units serve adults and 28 (90%) serve pregnant women, 26 (84%) serve children, and 21 (68%) serve neonates. One unit (3%) indicated they would admit only confirmed cases, while 18 (58%) would admit suspected and confirmed cases, and 12 (39%) would usually admit only confirmed cases, but they might admit unconfirmed cases depending on the situation.
Twenty-two (71%) of the units are located within a main hospital building, while 4 (13%) are within independent/standalone facilities. Additionally, HLIUs indicated whether the facility was located on the same or different campus as a biosafety level (BSL)-3 or BSL-4 laboratory: 4 (13%) reported having a BSL-4 laboratory on their campus, 20 (65%) said they have a BSL-3 laboratory on campus, while 6 (19%) have a BSL3 laboratory off campus, and 5 (16%) have a BSL-4 laboratory off campus.
HLIU Financial Support
HLIUs reported various streams of funding to maintain operations, with 18 units (58%) citing more than 1 source. HLIUs indicated financial support from federal governments (n=24, 77%), local governments (n=5, 16%), hospitals (n=20, 65%), philanthropic groups (n=1, 3%), and other organizations such as nongovernmental organizations (n=6, 19%).
HLIU Role in Early Days of COVID-19 Pandemic
Most HLIU respondents (n=27, 87%) reported serving at least 1 role following the declaration of the COVID-19 pandemic (Figure 1). Of these, 74% (n=20) took on the role of educator, providing training materials or programs to other healthcare agencies in their region/country. In regard to developing standard operating procedures, 85% of respondents (n=23) reported taking responsibility for developing these resources for local dissemination. Fifty-nine percent of HLIUs (n=16) had staff who served as trainers or subject matter experts for other local hospitals.
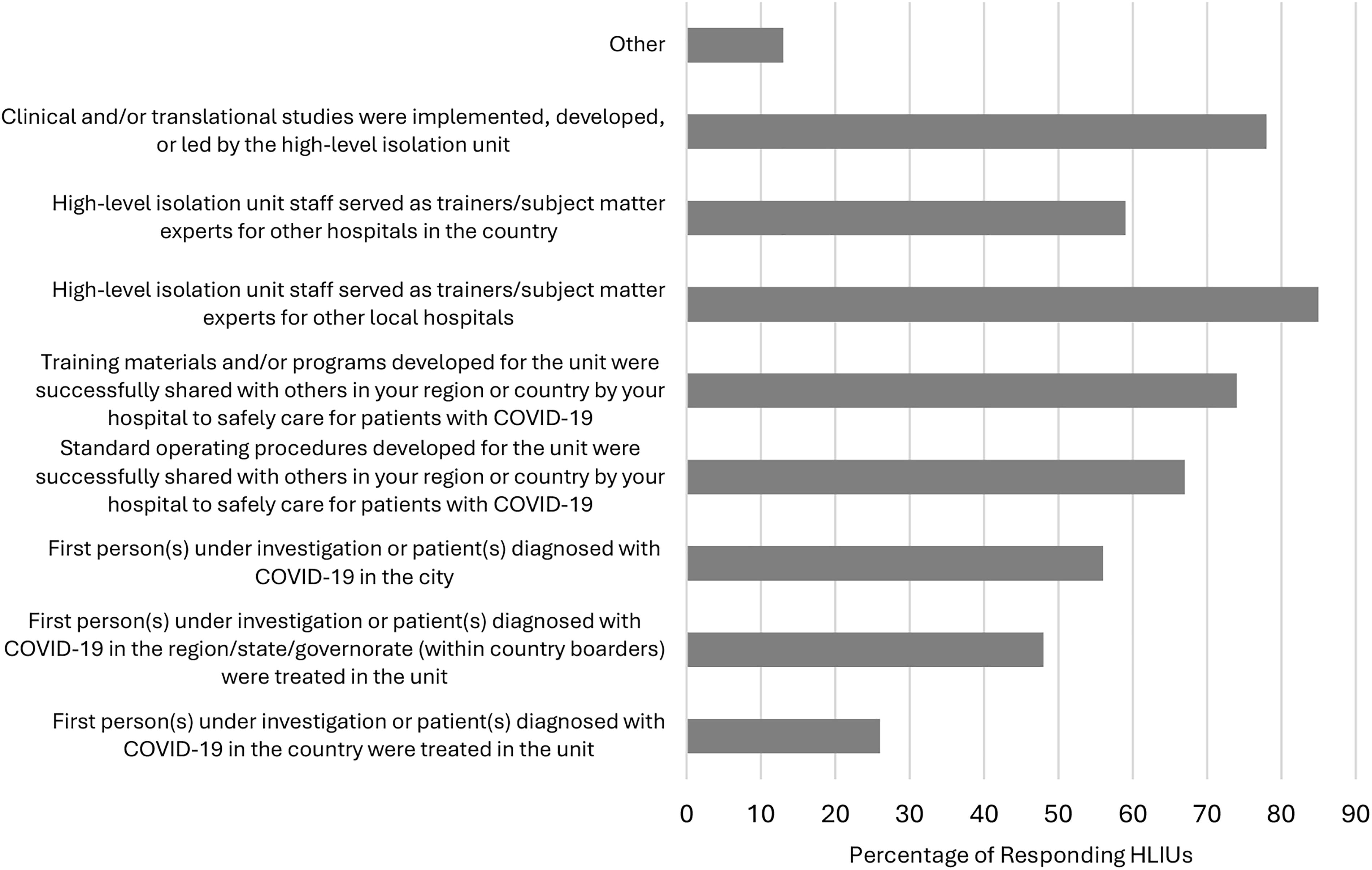
HLIU role during the early days of the COVID-19 pandemic.
Of the 27 HLIUs involved in the early days of the pandemic, 26% (n=7) provided care for the first person(s) under investigation in their respective countries, while 48% (n=13) treated the first patients in their region, state, or governorates within their country’s borders. At a local level, 56% (n=15) of the units reported caring for person(s) under investigation in the early days of the pandemic. Of the HLIUs that played a role during this period, 78% (n=21) implemented, developed, or led clinical and/or translational studies.
Of the 31 HLIUs represented in the survey, 26 (84%) had staff who advised local or national/federal government officials and nongovernmental or international organizations on the COVID-19 response (Figure 2). Nineteen of the 26 (73%) units advised national or federal government officials while 21 (81%) advised local government officials. Six (23%) units indicated they provided advice to nongovernmental or international organizations, such as the World Health Organization.

Organizations advised during the COVID-19 pandemic.
Ongoing HLIU Collaboration and Coordination
The majority (n=27, 87%) of responding units indicated that more than 1 HLIU exists in their country; of these, 81% (n=22) reported belonging to a formalized national system. Conversely, 13% (n=4) units reported being the only HLIU in their country. Regarding international collaboration, 71% (n=22) of the HLIUs have engaged with other units outside of their country, although the level and duration of those engagements were not indicated. Finally, 84% (n=26) of the HLIUs said they were a member or were aware of existing international networks that share resources, knowledge, and technical assistance.
Discussion
The findings from this survey demonstrate the array of similarities and differences among HLIUs across the globe, indicate potential areas of further investigation, and identify areas in which alignment could be improved and global standards could be created. As far as we know, a formal body for the regulation and licensure of HLIUs does not exist at the global level; this, along with local and national requirements and regulations and the lack of a standard global definition of a HLIU, may explain many of the differences reported by responding HLIUs. Of the 31 units participating in the survey, 27 (87%) reported that their facility was required to meet specialized standards for designation; however, only 20 (65%) respondents reported that their unit had a specific HLIU definition. Additionally, there was substantial variability and a general vagueness in the definitions provided. In 2009, the European Network for Infectious Diseases created a consensus definition for “highly infectious disease.” 2 In addition, the UK Health Security Agency maintains an updated web page that defines and provides a list of HCIDs. 3 While a strict global definition may not be required, a set of consensus recommendations for key principles of an HLIU would facilitate collaboration and serve as a core resource to hospitals seeking to develop an HLIU.
HLIUs require significant expenses due to their specialized features and general maintenance, among other factors, according to results from the 2018 survey that showed a mean annual operating budget of US$484,615. 12 Participants in the current survey reported receiving funding for operations from governmental bodies, hospitals, and philanthropic groups. Eighteen (58%) HLIUs reported receiving funding from more than 1 fiscal source. Similar to results from the 2018 survey, 12 most HLIUs in the current survey indicated being funded by the national government. Conversely, the results from this survey demonstrate that 20 (65%) of units receive funding from their hospital, whereas only 3 (10%) indicated this funding stream in the prior survey. This might indicate a growth in utilization of the spaces as “flex units” that are used on a regular daily basis.
Before 2020, HLIUs primarily served as units supporting the care of suspected or confirmed persons with VHF, as demonstrated during the 2014-2016 EVD outbreak, which required the activation of HLIUs in both the United States and Europe. Moreover, HLIUs proved to be invaluable during the initial outbreak of COVID-19 and after the pandemic was declared. Results of this survey showed that a vast majority of units played critical roles, particularly during the early days of the pandemic and specifically in national and local patient care and healthcare worker training. The ability of HLIUs to demonstrate these capacities, and to provide highly trained personnel and a cache of resources such as personal protective equipment, is highlighted in the literature and emphasizes the wealth of knowledge, personnel, and resources HLIUs and their staff can provide during a novel outbreak.13-15 Undoubtedly, the existence of a group of key global experts who provide not only care but also train peers helped build a more prepared workforce and increased local health and global security.
All responding HLIUs reported having the capacity and capability to care for adult patients. Compared with the 2018 survey of global HLIU capabilities, 12 a greater proportion of HLIUs in this survey reported being able to care for pregnant women (79% in 2018 compared with 90% in the current survey), children (74% compared with 84%), and neonates (47% compared with 68%). These findings could signify an increased focus over the last few years on expanding HLIU capabilities for special populations. Similar to the 2018 survey findings, HLIUs in this survey reported a higher bed capacity for respiratory HCIDs than for VHFs, which may be due to more intensive care needs for VHFs and a higher staff-to-patient ratio. However, the mean bed capacity for both VHFs and respiratory HCIDs reported in this survey were lower than those reported in the 2018 survey (4.8 beds compared with 3.8 for VHF and 8.8 beds compared with 6.3 for respiratory HCIDs). There is an opportunity to further explore whether HLIUs have generally seen decreases in capacity since the pandemic and factors affecting that capacity (eg, staffing, sustainability).
Survey results demonstrated that collaboration and formalized national networks of HLIUs do exist. At the global level, 22 (71%) respondents reported engaging with HLIUs outside of their country. The existence of these groups at national and global levels demonstrates the interest among professionals in engaging with each other to learn and exchange knowledge. Leveraging the existing national systems and international networks to formalize and grow a global HLIU collaboration could expedite learning and exchanging knowledge to improve best practices and address gaps in research and knowledge. This could be done through routine virtual sessions to share best practices and experiences in high-level isolation, multisite clinical research, and applied research on high-level isolation processes (eg, decontamination, personal protective equipment) or exchange of experts to observe and evaluate HLIU partners’ exercises and trainings. Managing an international collaboration in the science community may come with barriers related to languages spoken, differences in research standards and intellectual property rights, and establishing trust. Nevertheless, these partnerships also serve as mechanisms by which research is strengthened, networking occurs, and academicians are fostered.16-19
This study was not without limitations. A small sample was recruited and participated in the survey. Those recruited represent a majority of the known global HLIUs, but we recognize that others exist, especially outside of high-income countries, which are the only countries with HLIUs represented in these data. Due to formal HLIU systems known by the research team, many independent HLIUs from the United States and Germany completed the survey, and thus, these countries are overrepresented. Lastly, data are self-reported and not validated. Some surveys may have been completed collaboratively among HLIU staff while others may have been completed by a single representative.
Conclusion
To our knowledge, this is the largest global survey of existing HLIUs and the most recent survey conducted among international units since 2018. Results of this survey demonstrate the role of international HLIUs in responding to the COVID-19 pandemic and their capacity to provide medical care for those affected by HCIDs. In a more globalized world, collaboration and networking among global HLIUs could increase knowledge sharing, create standardization of regulations, and advance practices and treatment of HCIDs in future pandemics.
Footnotes
Acknowledgments
The authors would like to thank and recognize all who contributed to the design of this survey as well as those units and professionals who participated.