
Abstract
Patients with suspected or confirmed high-consequence infectious diseases (HCIDs) may present for care at any acute care facility. However, there are limited data to inform recommendations for the design, maintenance, and operation of isolation spaces for patients with suspected or confirmed HCIDs. To address this gap, we developed consensus statements by convening a group of 29 subject matter experts to participate in a modified Delphi process facilitated by a validated tool (the RAND-developed ExpertLens system). The subject matter experts participated in 3 consensus rounds, providing feedback and rating the appropriateness of 36 draft consensus statements. These draft statements were then revised based on their feedback. As a result, we developed 36 consensus statements addressing 5 domains: (1) patient room physical space, (2) doors and windows, (3) air handling, (4) electrical and plumbing, and (5) soiled utility rooms and waste management. These statements could inform the approaches of frontline acute care facilities when building new spaces or modifying existing spaces to enable appropriate HCID patient isolation and care.
Introduction
H
At the healthcare facility level, ensuring the safe and effective delivery of care requires not only prompt identification and isolation of suspected HCIDs (eg, implementation of the Identify, Isolate, and Inform framework 2 ). It also requires appropriate physical space for patient placement and provision of care. The US Centers for Disease Control and Prevention (CDC) recommends initial placement of a patient with a suspected VHF in a single occupancy patient room with a private bathroom. 3 While previous consensus statements have been issued related to the construction, maintenance, and operation of specialized biocontainment units for care of patients with VHFs,4,5 dedicated units are beyond the scope of most healthcare facilities. In the United States, the US Department of Health and Human Services established regional emerging special pathogens treatment centers, which now total 13. These centers have the required equipment and capabilities to provide clinical services and prolonged biocontainment for patients with suspected or confirmed HCIDs. Outside of these 13 centers, specialized units for biocontainment of HCIDs are uncommon. Thus, all frontline healthcare facilities face the challenge of being prepared at a minimum to be able to immediately isolate and stabilize patients with suspected or confirmed HCIDs prior to coordinated transfer to a specialized center with a biocontainment unit if required. 6
The aim of this project was to develop consensus statements addressing physical space construction or modification in frontline facilities to enable effective infection control and facilitate suspected or confirmed HCID patient management. In this article, we describe the consensus approach and outcomes. We used a modified Delphi process to arrive at a list of statements that adhere to existing healthcare facility design standards and reflect the consensus of a group of expert participants.
Methods
The project team consisted of 2 infectious diseases physicians and healthcare epidemiologists, an experienced nurse and healthcare emergency management professional, an infection preventionist, and a program manager. The project team oversaw the creation of the draft statements, invited participants for the modified Delphi consensus process, and moderated and responded to feedback during the consensus process. Under guidance from a modified Delphi process expert, the project team reviewed the statement rating data and compiled the list of final consensus statements. The overall project timeline is summarized in Figure 1.
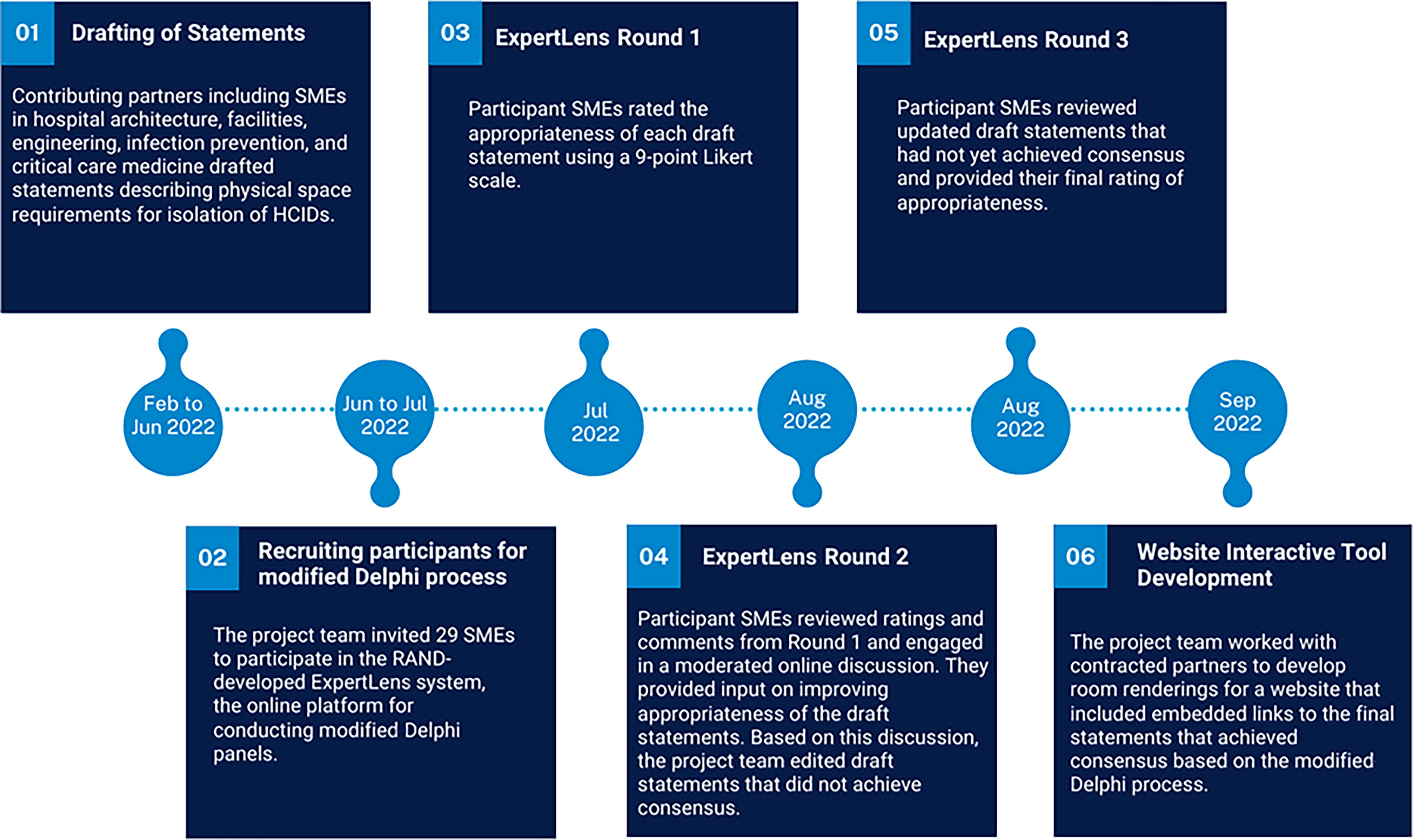
Project timeline. Abbreviations: HCID, high-consequence infectious disease; SME, subject matter expert.
Drafting of Statements
The project team defined the scope of the statements to address the patient room specifications, patient room doors and windows, air handling, electrical, plumbing, soiled utility room, and waste management. Based on this scope, the project team approached professional societies and organizations such as the Society of Critical Care Medicine; American Society for Heating, Refrigerating and Air-Conditioning Engineers; American Society for Health Care Engineers; Facility Guidelines Institute; Association for Professionals in Infection Control and Epidemiology; and NBBJ (an architecture firm with experience in healthcare facility design) to recruit voluntary subject matter experts (SMEs) who could help draft initial statements. While recommended as representatives by their professional societies and organizations, their contribution to the draft statements was informed by their professional expert capacity and do not necessarily reflect their respective organizations' official position on the matter. The SMEs were tasked with developing draft statements in their respective disciplines that incorporated existing standards. For matters not addressed by guidelines or standards, draft statements were based on expert opinion and available evidence. The draft statements were circulated to the entire SME group and discussed at a series of virtual working group meetings. Based on feedback, 36 draft statements were revised and included in the modified Delphi process.
Modified Delphi Process
The modified Delphi process is an established iterative method used to reach consensus on an issue that has limited evidence and where expert opinion is important. 7 All quality and methodological criteria for reporting on Delphi studies proposed by Diamond et al were followed. 8 The project team invited 29 participants from 3 key groups (Table 1): (1) SMEs affiliated with professional societies/organizations or public health agencies, (2) clinical or healthcare operations experts, and (3) field experts in areas important for this work. Using a modified Delphi process, participants were asked to provide input on the appropriateness of 36 draft statements to provide guidance on the physical infrastructure for HCID patient isolation and management at frontline acute care facilities. The first group included SMEs from the CDC and from the major professional societies and organizations representing public health officials, healthcare epidemiology, infection control, healthcare facility construction, engineering, and air handling. The second group included experts with extensive experience in healthcare facility HCID preparedness and management of suspected or confirmed HCID patients. The third group included field experts whose professional work and qualifications in relevant areas such as healthcare facility air handling, electrical systems, waste management, plumbing, and architectural design. The invited participants were selected because they had the appropriate educational background, training, field expertise, clinical experience, and/or organizational affiliation to provide expert opinions on physical space requirements to optimize infection control management of patients with suspected or confirmed HCIDs. The project team selected the professional societies and public health organizations, subject matter experts, and societies based on the scope and content of the draft statements. The societies and organizations were asked to select an appropriate expert to speak broadly to the project (eg, critical care physician with relevant experience) or to the specific subject matter (eg, management of plumbing and water in healthcare facilities). These participants were asked to provide their individual expertise and not to represent their organization in an official capacity. The findings and conclusions presented here reflect those of the authors and do not represent the endorsement or policies of their affiliated organizations.
Expertise and Stakeholders Invited to Participate in the Modified Delphi Process (N=29)
Note: Some organizations or expertise had more than 1 affiliated participant (indicated in parentheses), and 2 participants were affiliated with more than 1 organization. Therefore, the counts in parentheses may exceed the total number of participants for each category. Individuals from professional societies or health systems provided their individual expertise and did not represent the views or positions of their affiliated organization.
To solicit input and explore consensus among modified Delphi process participants, we conducted the panel using the online RAND-developed ExpertLens system 9 with 2 prespecified rounds of ratings and a discussion round in between (Figure 2).

A description of each round of the modified Delphi process, facilitated by the RAND-developed ExpertLens system. Abbreviation: SME, subject matter expert.
During Round 1 (July 7 to 29, 2022), participants rated the appropriateness of each of the 36 draft statements on a 9-point Likert scale (1 = very inappropriate, 9 = very appropriate). They also had an opportunity to enter a comment on each statement explaining the rationale behind their rating. The draft statements were grouped into categories: patient rooms; patient room doors and windows; air handling; electrical and plumbing; and waste management and soiled utility room. Participants were instructed to rate the statements based on the following rubric:
The statement is not appropriate to include in the consensus statements and may need to be removed (scores 1 to 3). The statement might be appropriate to include in the consensus statements but requires revisions (scores 4 to 6). The statement is appropriate and should be included in the consensus statements (scores 7 to 9).
In addition to rating the statements and providing an explanation of their responses, participants who rated statements between 4 and 6 were asked to suggest revisions for more appropriate statements.
During Round 2 (August 2 to 11, 2022) participants reviewed Round 1 results. For each statement, participants were presented: (1) a distribution, median, and interquartile range of statement ratings; (2) a color-coded statement indicating whether the panel deemed it appropriate, not appropriate, or of uncertain appropriateness determined using the RAND/UCLA Appropriateness Method 10 approach to calculating consensus; and (3) a summary of participants’ comments. They also participated in an asynchronous discussion through an online discussion forum moderated by 2 SMEs from the project team. Participants posted questions and comments anonymously. Discussion moderators followed a standard moderator protocol for ExpertLens panels. They asked clarifying and probing questions to generate additional explanations of appropriateness and engaged with those whose perspective differed from group consensus. 11 The project team then reviewed the ratings, comments, and discussion from Round 2. Statements that achieved consensus for inclusion in the guidance and did not elicit any suggested revisions were accepted and not included in Round 3. Other statements were revised to incorporate feedback from participants and included for review in Round 3. A list of original and revised statements is included in Appendix A (available in Supplemental Materials; www.liebertpub.com/doi/suppl/10.1089/hs.2024.0013).
During Round 3 (August 19 to 26, 2022), participants were presented with updated statements and any statements that had not yet reached consensus. They were asked to rate the appropriateness of revised statements using the same scale in Round 1. The modified Delphi process was concluded after Round 3 and final ratings were analyzed to determine whether consensus was established for accepting or rejecting each statement.
Data Analysis
To establish panel consensus after the 3 rounds were completed, we applied the RAND/UCLA Appropriateness Method 10 approach to final Round 3 data. Briefly, this 3-step approach first evaluates the distribution of ratings across the 3 tertiles of the 9-point scale to determine whether more than a third of responses are in the upper and lower tertiles. If they are, then the panel failed to reach consensus. If they are not, then consensus was reached and the median determines the final panel results. A median rating below 3 indicates that the statement is inappropriate to include and is, therefore, removed from the final list of statements. A median above 6.5 means that it is appropriate to include in the final list of statements. To assess the level of participation, overall response rates for each statement in Rounds 1 and 3, respectively, were calculated. Percentage attrition in participation was calculated for all participants and for each group, respectively, by comparing the largest number of responses per item in Round 1 versus Round 3.
Ethical Considerations
This study was reviewed by the institutional review boards at Massachusetts General Hospital (exempt, #2022P001471) and RAND (#2022-N024).
Results
Twenty-nine SMEs with wide ranging areas of expertise were invited to evaluate 36 draft statements over the 3 rounds of a modified Delphi process facilitated by the RAND-developed ExpertLens system. After the first 2 rounds, 18 statements reached consensus for inclusion without additional revisions. These statements were from the following categories: patient rooms (5), patient room doors and windows (3), air handling (5), electrical and plumbing (3), and soiled utility room and waste management (2). The remaining 18 statements that did not achieve consensus in the first 2 rounds were included for review in Round 3 (Table 2). The project team reviewed the ratings from Round 1, along with comments and discussion from Round 2, and made recommended revisions to the statements. The 18 updated statements were reviewed by SME participants in Round 3 and reached consensus for inclusion. No statements generated by the drafting team failed to reach consensus for inclusion after appropriate revisions based on feedback. Ratings of each statement in Rounds 1 and 3, respectively, are provided in Table 2. Final consensus statements are provided in Appendix B (available in Supplemental Materials).
Subject Matter Expert Review of Statements by Category in the Modified Delphi Process (N=29)
Note: Gray shading in rows indicates statements that reached consensus for inclusion after the first round of ratings and did not require further revisions. They were not included for reassessment in Round 3.
Abbreviation: A, appropriate; HCID, high-consequence infectious disease; HEPA, high-efficiency particulate air; HVAC, heating, ventilation, and air conditioning; PPE, personal protective equipment; SD, standard deviation.
The overall response rate for each question is reported in Table 2. Among all invited participants (n=29), the largest number of responses in Round 1 was 21 and the largest number in Round 3 was 15, for a 29% attrition rate in participation between Round 1 and Round 3. Among the participant groups—professional societies/organizations or public health agencies (n=10), clinical or healthcare operations experts (n=9), and field experts (n=10)—the number of participants by group in Round 1 was 6, 7, and 8, respectively. In Round 3, the number of participants by group was 6, 3, and 6, respectively. Accordingly, attrition from Round 1 to Round 3 was 0%, 57%, and 25%, respectively, for the 3 groups.
Discussion
All healthcare facilities must be prepared to safely care for patients presenting with suspected or confirmed HCIDs. During the 2014-2016 West African outbreak, US healthcare facilities provided care for 11 patients with Ebola virus disease including patients evacuated from other countries. 12 US healthcare facilities have also diagnosed and managed patients with other HCIDs, including Marburg virus disease, 13 Middle East respiratory syndrome, 14 and Lassa fever, with no evidence of nosocomial transmission.15-17 Through a modified Delphi process, we found consensus on specific features of the built environment that can support frontline healthcare facilities as they engage in HCID preparedness.
The CDC has articulated the Identify, Isolate, and Inform framework that healthcare facilities should implement to safely evaluate patients with HCIDs. 2 This involves promptly identifying patients with suspected HCIDs, isolating them in an appropriate space, and informing public health authorities. Implementing this framework ensures that immediate isolation is implemented and that clinicians are equipped to perform further evaluation and management safely. At a minimum, all healthcare facilities should implement symptom and exposure history screening for patients at all points of entry. This screening tool may be modified based on current outbreaks of concern. Screening at points of entry serves to identify patients who should have further assessment for a possible HCID and need prompt isolation in a private room or area. Staff at the point of entry should be trained to immediately contact relevant healthcare facility leadership and public health authorities to facilitate next steps in evaluation. A necessary component of the Identify, Isolate, and Inform framework is ensuring that the physical space used for evaluation and care is appropriately designed.
Space design and redesign is an integral feature to safely isolate those with suspected or confirmed HCIDs. Because there are few highly specialized facilities for HCID care, and transfer of patients to those facilities can take several hours or longer, it is critical for all frontline acute care facilities to consider having the physical space capable of providing isolation and initial clinical care to patients with suspected or confirmed HCIDs. Effective July 1, 2024, The Joint Commission has adopted a new standard that requires hospitals to implement protocols to support preparedness for HCIDs. 18
The hierarchy of controls approach is useful when evaluating the relative effectiveness of various infection control measures. 19 The consensus statements provide strategies across the spectrum of these controls from elimination, substitution, engineering controls, administrative controls, and use of personal protective equipment (PPE). For example, physical space should support appropriate administrative controls such as unidirectional flow. Having a designated PPE doffing room, or at least a designated doffing area in the patient room, facilitates proper PPE use and mitigates risk of self- and cross-contamination during doffing. By implementing measures along the entire hierarchy of controls, healthcare facilities can mitigate the risks posed by HCIDs.
After incorporating revisions based on feedback, all statements that underwent the modified Delphi process were ultimately included. While criteria for consensus were met, 10 there were 3 statements that required all 3 rounds of deliberation and ratings before consensus could be reached: (1) whether an anteroom is required for airborne infection isolation rooms, (2) the negative pressure gradient requirement, and (3) hands-free sinks and risk of waterborne pathogen transmission. The discussion regarding anterooms acknowledged that while this design element may support PPE doffing practices, it also adds cost to the initial space design or retrofit of existing spaces. The final statement did not require the inclusion of an anteroom (Appendix B, Statement #5 (Appendix B available in Supplemental Materials). SMEs acknowledged the lack of clear evidence to support an upper limit for the negative pressure gradient.4,5 Ultimately, 2.5 Pa was recommended, a pressure gradient that is consistent with CDC recommendations for airborne infection isolation rooms (Appendix B, Statement #16). Discussion related to hands-free sinks centered on the potential for the mechanical design to promote the growth of waterborne bacteria. This potential concern was weighed against the risk of touch contamination, and the final statement did recommend providing a handwashing station with a hands-free faucet in the patient room (Appendix B, Statement #28).
The consensus statements are subject to 2 types of limitations: those related to the scope of the final statements and those related to the modified Delphi process. First, the statements are based on currently available technologies. It is possible that newer technologies, such as disposable modular airborne isolation systems, may improve the scalability of isolation approaches for HCIDs at frontline facilities. Second, the statements do not address the physical spaces required for other workflows such as the clinical laboratory, procedure suite, operating room, or labor and delivery unit. Those spaces were beyond the scope of this project, but they remain important to consider. Third, the approach to staff training to effectively use the elements of the space were beyond the scope.
Finally, some limitations were related to the modified Delphi process. Not all panelists who had accepted our invitation to participate ended up submitting ratings on all the draft statements, which is common for Delphi studies. 20 To optimize response rates, we provided scheduled reminders for all participants to submit their ratings and comments on the draft statements. Although attrition could have biased our results, it is unlikely because nearly all draft statements were already rated as “appropriate” by all participant groups (Table 1) in Round 1. Some of these “appropriate” statements were subsequently revised based on feedback, then reconfirmed as “appropriate” in Round 3 ratings. The group with the largest attrition between Round 1 and Round 3 (professional societies/organizations or public health agencies) provided ratings in line with the other groups, so there is lower likelihood of bias due to their attrition. In Round 1, the field expert group disagreed on whether 2 statements should be included. However, after the Round 2 discussion, both statements were rated again as “appropriate” by the field expert group in Round 3. The field expert group had higher participation for these 2 statements in Round 3 than in Round 1, and 80% of Round 1 participants also rated the statements in Round 3. Therefore, for the 2 statements where there was initial disagreement, attrition did not significantly bias the final result.
While we asked all SMEs participating in the modified Delphi process to review, rate, and comment on all 36 draft statements, each group had different areas of expertise and experience. Although SMEs may have experienced difficulty assessing statements on topics outside of their scope of work, the invited SMEs were chosen because each had sufficient core knowledge about HCIDs and infection control. Moreover, Round 2 of the ExpertLens process allowed for a discussion between participants with differing areas of expertise, which may have helped inform their final ratings in Round 3.
Despite these limitations, our project addresses an important gap in the existing literature by providing guidance on building or modifying physical space to enable frontline healthcare facilities to isolate and stabilize patients with suspected or confirmed HCIDs. Given the lack of evidence to support these standards, we used a well-established modified Delphi process 7 to systematically achieve consensus on the final statements based on expert opinion.
Content Dissemination
Final consensus statements were posted on the MyPACT website with an interactive tool involving room renderings and embedded links to individual statements (Figures 3A and 3B). 21 The room renderings were generated by a representative from a contracted architectural firm, with guidance from the project team. The renderings were not provided for consideration as part of the modified Delphi process.

Room renderings of (A) the overall unit and (B) the patient room. The renderings were posted on the website along with embedded links (indicated by white circles) to consensus statements and implementation strategies.
Conclusion
Suspected or confirmed HCID patients may present at frontline acute care hospitals for evaluation. One key element of preparedness for HCIDs is defining the design, maintenance, and operation elements of isolation spaces. The consensus statements produced by a modified Delphi process provide specific guidance for frontline acute care facilities on how to support effective isolation and patient care when building new spaces or modifying existing spaces.
Footnotes
Acknowledgments
We thank Stephanie Rejoui, MHA, for providing administrative support for this project. This project was supported by CDC Project Firstline through cooperative agreement CDC-RFA-CK19-1905: National Infection Control Strengthening. The contents of this article are those of the authors and do not reflect the views of the CDC.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.