
Abstract
The demands for vaccination, testing, and community outreach during the COVID-19 pandemic extended beyond public health capabilities. The role of independent pharmacies proved invaluable as they partnered with local, state, and federal public health entities to provide additional capacity. However, the complexities of federal partnering agreements and the limited awareness of independent pharmacy networks could delay engagement and support for underserved communities in future responses. Addressing this challenge requires tailored public–private partnership agreements and resilience frameworks for data sharing based on experience and exercises. This case study describes the experiences of independent pharmacies during the COVID-19 response, opportunities for sustained public health and pharmacy engagement, and recommendations for building a framework for rapid scale-up before the next public health emergency. Under the direction of the National Community Pharmacists Association Innovation Center, aggregators of independent pharmacies have collaborated to form the Independent Community Pharmacy Consortium for Federal Government Engagement. This consortium represents a majority of the 18,900 independent pharmacies in the United States and establishes a single initial point of contact for government agencies to reach independent pharmacies. The development and management of the consortium remains outside of the government, enabling continuity and flexibility. This case study offers a unique perspective of public health engagement and partnership with independent pharmacies based on documented responses, exercises, and discussions.
Introduction
T
Pharmacists working in independent pharmacies in healthcare deserts and rural settings have championed health outcomes based on social determinants of health. 5 These determinants include impacts to economic stability, neighborhood and built environment, social and community context, healthcare access and quality, and education access and quality.6-8 Through individualized clinical counseling, health education, and chronic disease management, independent pharmacists and pharmacies are in a prime position to be frontline responders in the next public health emergency. They provide medication access, medication adherence through counseling and education, immunizations, and interventions—all leading to greater health equity. 4 However, unlike chain pharmacies, each independent pharmacy is a separate entity with disparate responsibilities and intricacies for entering into formal agreements. Engaging each independent pharmacy individually is a burdensome process for any entity executing an emergency response.
An emergent threat to a community could cause substantial stress on local public resources that require contingency plans, especially in communities with challenging environments and infrastructure concerns as measured by the Social Vulnerability Index. 9 Including independent community pharmacies as frontline healthcare professionals in emergency planning is critical, given past reliance on these pharmacies to operationalize services to deliver products, education, and other support. Planning often includes national pharmacy chains under single management, but it often excludes the nation’s 18,900 independent pharmacy locations, where essential services are provided for communities across the country, including in areas where other healthcare providers and chain pharmacies are not present. 10
These small businesses are trusted in their communities and have established community connections that enable coordinated implementation of services. Their capabilities include disseminating education and guidance to empower citizens and dispel inaccurate information, serving as distribution points (either centrally or through existing delivery services) for products such as personal protective equipment, and administering vaccines and other medications. The Zika virus outbreak, for example, resulted in the engagement of pharmacies with nationwide networks, including US territories. For the first time, marketing of family planning products was co-located with messaging about insect repellent and virus transmission in pharmacies. Pharmacists received current science-based information to address the risks of Zika infection to patients in high-risk areas, including when purchasing family planning products. 11
These pharmacies gained experience during the H1N1 and COVID-19 pandemics to scale services and provide care, such as testing and childhood immunizations, when other providers were not available. To leverage independent pharmacies, health officials need an efficient and effective way to engage community pharmacy teams.
Independent pharmacies have played a crucial role in public health emergencies, including as a key provider of vaccines during the 2009 H1N1 flu pandemic and the COVID-19 pandemic through the Public Readiness and Emergency Preparedness (PREP) Act.12,13 Independent pharmacies were engaged only at the state or local level, however, until the first coordinated federal partnership with pharmacy services administrative organizations occurred during the COVID-19 response, as described later. Pharmacies were also engaged by federal, state, and local public health agencies for information dissemination, medical referrals, point-of-care testing, and mask distribution. 14 By some estimates, pharmacy interventions during the COVID-19 pandemic contributed to US$450 billion in healthcare cost savings. 15 Within the pharmacy landscape, independent pharmacies and the organizations that support them play a unique and vital role.
Independent pharmacies are often associated with aggregators called pharmacy services administrative organizations (PSAOs), which serve a group of pharmacies by providing contracting and funding mechanisms to facilitate partnerships. 16 This approach to pharmacy operations differs from chain drugstores or grocery-based pharmacies that may have a central management structure. The PSAO aggregation structure can present challenges to government public health partnerships due to the lack of transparency about which pharmacy is affiliated with which PSAO; arranging such partnerships takes time and could delay the implementation of a response. However, it is essential to include independent pharmacies in a response because they are often located in areas where few to no chain pharmacies or other healthcare options are present. 17 The consortium described later addresses this coordination challenge.
The largest engagement of independent pharmacies occurred during the US COVID-19 response as part of the Federal Retail Pharmacy Program (FRPP) for COVID-19 Vaccines. 18 With the activation of the program, a network of pharmacies received a supply of lifesaving COVID-19 vaccines that placed them within 5 miles of 90% of the population. 19 Approximately 11,000 of the 18,900 independent pharmacies in the United States were included in this program, leveraging 41,000 pharmacies nationally. 15 The independent pharmacy aggregators successfully reduced the number of contacts and burden on the US Centers for Disease Control and Prevention (CDC) for coordinating with the enrolled pharmacies during the COVID-19 pandemic. Independent pharmacies filled in health equity gaps, with store locations in rural, suburban, and urban communities where other healthcare providers and chain drugstores were not accessible. This expansive coverage would not have been possible without the inclusion of independent pharmacy aggregators.
The structure and recommendations provided in this COVID-19 case study offer next steps for engaging independent pharmacies before the next public health emergency and provides a collaborative framework for maintaining momentum from the COVID-19 pandemic.
Methods
Scale and Abilities of Public Health and Independent Community Pharmacies
During the COVID-19 vaccination campaign, chain drugstores, PSAOs, long-term care group purchasing organizations (LTC GPOs), and a clinically integrated pharmacy network signed a binding, unfunded partner agreement for the ordering and administration of government-funded COVID-19 vaccine. The aggregators of nonchain pharmacies served as the centralized points of contact and signatory partners in the FRPP to establish the required chain pharmacy-like agreements. Aggregators of independent pharmacies gathered required information for participation and provided the administration functions required in the FRPP agreement.
The FRPP enrollment processes resulted in 7 separate agreements between the CDC and the PSAOs, LTC GPOs, and the clinically integrated pharmacy network representing independent pharmacies. Each of the independent pharmacy aggregators that signed the CDC FRPP network agreements took on chainlike responsibilities for oversight, education, and centralized data reviews and reporting to fulfill the US government required processes for network administration, vaccine ordering, distribution, and multisystem data reporting. For example, the agreement required each pharmacy organization to report through a technical architecture including 7 different data channels including state immunization information systems and federal data ordering, reporting, and locator systems, requiring costly upgrades and unreimbursed connectivity development (Figure).20-22
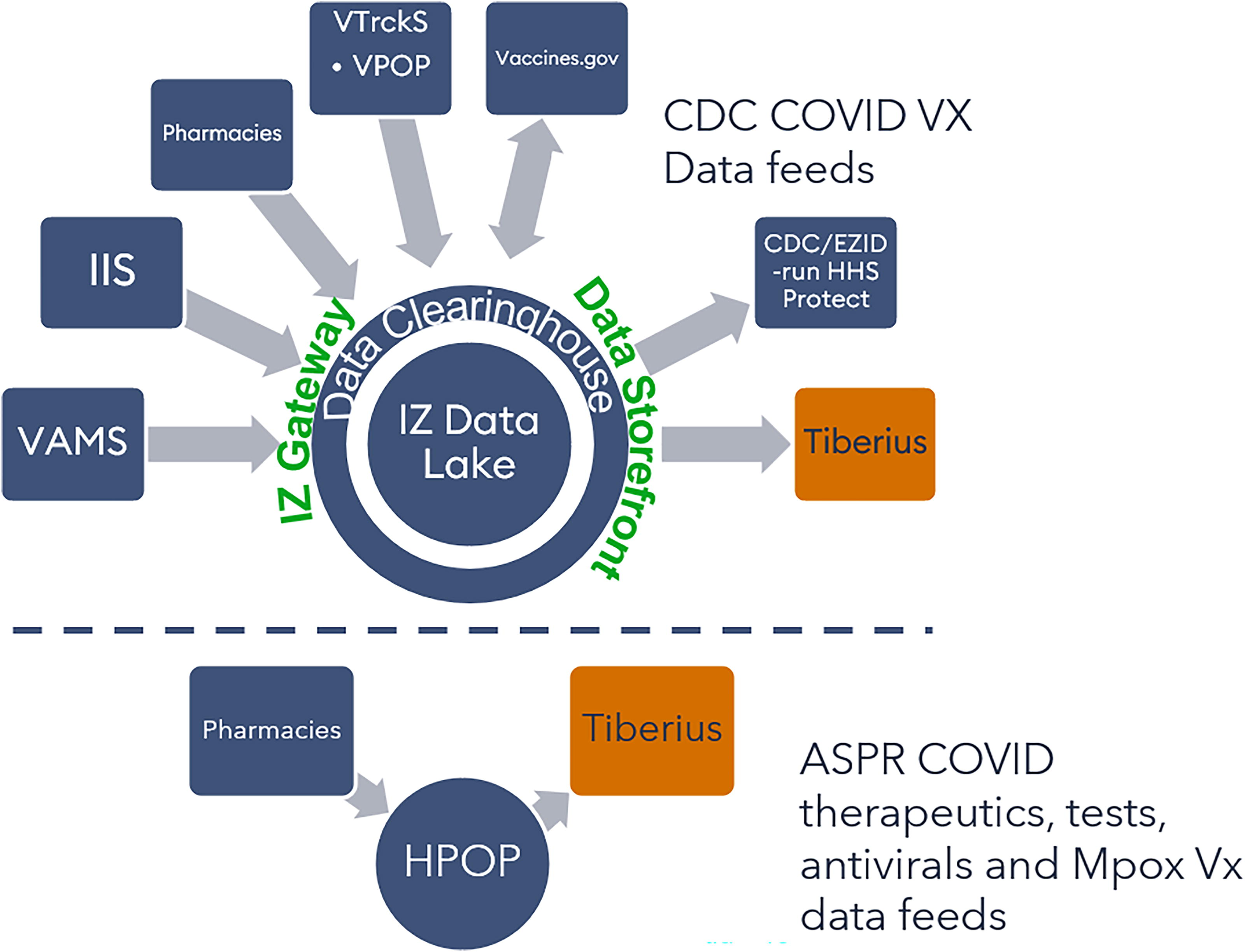
Data systems required by the US Department of Health and Human Services for pharmacy ordering, tracking, and reporting COVID-19 vaccines and therapeutics. Abbreviations: ASPR, Administration for Strategic Preparedness and Response; CDC, US Centers for Disease Control and Prevention; EZID, National Center for Emerging and Zoonotic Infectious Diseases; HHS, US Department of Health and Human Services; HPOP, Health Partner Ordering Portal; IIS, Immunization Information System; IZ, Immunization Gateway; VAMS, Vaccine Administration Management System; VPOP, Vaccine Provider Order Portal; VTrckS, Vaccine Tracking System; Vx, vaccination.
The same partner agreement template was used for large chain drugstores, long-term care pharmacies, and independent pharmacy aggregators. There is a need for tailored agreements that are separate from chain drugstores, which the authors will outline in the discussion section.
Federal outreach for the FRPP began in September 2020 and pharmacy onboarding for data systems began in November 2020 in anticipation of vaccine manufacturing and availability. 22 The federal government allotted tranches of vaccine between state territorial and tribal nations and a separate allocation of COVID-19 vaccine to pharmacies. The federal government asked state health departments if they wished to transfer a portion of their allocation to a partner in the FRPP and recommended that they limit their choices to 1 to 2 pharmacy companies. State health departments unfamiliar with independent pharmacy aggregators and their broad geographic coverage often chose large chains. However, some quickly shifted to independent pharmacy aggregators when they recognized that independent pharmacies could provide expanded access to vulnerable communities through the FRPP pharmacy aggregators.23-26 The Federal Retail Pharmacy Therapeutics Program used the same approach over a year later.
The Centers for Medicare and Medicaid Services and the Health Resources and Services Administration supported billing and reimbursement of COVID-19 vaccine administration, therapeutics, and testing. However, in the case of independent pharmacies, only the individual pharmacies were compensated for the claims and not the aggregators. 27 Chain drugstores were able to leverage reimbursement funds for national operations costs, whereas aggregators had to defray the costs related to coordination and data requirement for the federal programs. This challenge could be resolved for all pharmacy partners with the recommendations provided in this article.
The networks of independent pharmacies continued to support government response initiatives, but fewer independent pharmacies were able to participate with each additional program (discussed in the next paragraph). These programs included the US Department of Health and Human Services (HHS) Administration for Strategic Preparedness and Response antiviral dispensing Federal Retail Pharmacy Therapeutics Program at the end of 2021, Test to Treat in spring of 2022, and government N95 mask giveaways in October 2023.28-30
Independent pharmacies and pharmacy aggregators were able to adapt their operations and systems to successfully contribute to the COVID-19 response. This ability to adapt highlights the scale and capabilities of the independent pharmacy network, including:
Expanding the vaccinator workforce by tens of thousands during the COVID-19 pandemic through the PREP Act
31
Contributing to more than 304 million COVID-19 vaccine doses administered in programs through state-supplied vaccine allocations, the Federal Retail Pharmacy Program, and CDC’s Bridge Access Program as of June 2023, including in rural communities and areas with high social vulnerability, and ensuring vaccine distribution equity22,32 Disseminating COVID-19 therapeutics through the Federal Retail Pharmacy Therapeutics Program and the Test to Treat program28,29 Distributing N95 respirators on behalf of the federal government, as an additional service to HHS
30
Delivering evolving clinical training to pharmacy staff, as well as messaging and public health education to patients and communities including the V-safe vaccine safety monitoring system
33
Reporting of procurement activity, current supply, and administration data that feed into 8 government data portals and ordering systems (see Figure)
Independent Community Pharmacy Consortium for Government Engagement
Opportunities to build sustained partnerships between governmental public health systems and independent pharmacies for national readiness and response are gaining momentum. As of June 2024, there are as many independent pharmacies as chain pharmacies, based on IQVIA Rx Universe data. 34 Before the next public health emergency, it will be vital to develop tailored public–private partnership agreements, funding models to sustain community-based pharmacy providers, and frameworks for sharing data and information based on lessons learned.
Since the end of the COVID-19 public health emergency, the NCPA Innovation Center has gathered a group of independent pharmacy aggregators to discuss engaging with government entities to ensure emergency readiness by increasing national public health capacity. This group, the Independent Community Pharmacy Consortium for Government Engagement, represents a majority of the 18,900 independent pharmacies in the United States. 23 It includes PSAOs that can engage independent pharmacies with a single affiliation and wholesalers who can support independent pharmacies and manage physical distribution of public health countermeasures and personal protective equipment. 35 The consortium can also engage pharmacy management software vendors as data partners before the next public health emergency. The consortium structure offers a framework for engaging independent pharmacies for contracting, physical distribution, and operations support services and data for readiness and response. The government and each consortium partner would be able to scale up based on a preestablished structure and consolidated agreement. The consortium could use a fraction of the time spent in coordination meetings and open response participation to all independent pharmacies within active consortium membership. Each consortium member organization has a shared goal to maintain engagement with government planners and operational staff before and during an event that requires extensive capacity beyond a governmental response.
Based on the experiences of government collaboration from the 2009 H1N1 pandemic through the COVID-19 pandemic, discussions within the consortium have centered on what would make it easier for government to engage with independent pharmacy aggregators. For each novel activity, the consortium will determine and communicate event-specific roles and responsibilities. The NCPA Innovation Center, as the consortium lead, will collaborate with partners and use its existing relationships with government agencies to support independent pharmacy surge capacity for public health emergencies and emerging public health threats. Other response-related aspects, such as unique or day-to-day pharmacy capabilities, are outside the scope of the consortium.
Lessons Learned and a Path Forward
The consortium has developed guided, discussion-based exercises to articulate communication, planning, and response activities based on realistic scenarios in which government organizations would request support before and during a public health emergency. Through these exercises, consortium members determine what steps they would take and what requirements they might need based on prior experience and current independent pharmacy aggregator requirements, in preparation to be effective response partners in a public health emergency. These novel 45-minute virtual drills are abbreviated tabletop exercises called “desktop drills” that leverage a concept adapted from the Michigan Department of Agriculture and Rural Development. 36 The desktop drills are designed to be snapshots in time with specific objectives for focused discussion.
In 2024, the consortium held 2 desktop drills, a Zika outbreak scenario and a hurricane response scenario. The structured objectives in the first desktop drill focused on pharmacy activities in a response before and during an emergency declaration, such as determining thresholds for activating the consortium, identifying triggers for changes in activation, identifying potential communication coordination and pharmacy training needs, and defining the roles responsibilities of each consortium member during a response. Objectives for the second desktop drill in 2024 focused on what the consortium could do as a group and what each participating member should manage separately. Examples of objectives include (1) identifying response and recovery planning needs that can be managed by the consortium lead or as a collective (ie, communicating aggregated pharmacy capabilities to government groups, consolidating requests for data, retrieving data from standard sources to alleviate the burden on pharmacist and pharmacy staff, navigating mutual aid agreements, alternative distribution routines), (2) identifying the process for coordinating training for participating consortium members and their representative pharmacies through the NCPA Innovation Center, and (3) articulating the broad capabilities and needs for hurricane response and recovery that may require expanding consortium membership.
The rich discussions highlighted numerous opportunities and next steps. All participants recognized that independent pharmacies are a first line for impacted patients and communities, as well as small businesses within those communities. They will want to be involved in some way and will want the most up-to-date information, as well as connections to other public health and emergency responders in the area.
Recommendations
Through the consortium framework for rapid scaling and the observations and recommendations articulated in this case study, independent pharmacy aggregators are continuing response and readiness planning. In the early phases of any emergency response, government officials work to incorporate proven plans and protocols that meet emergent needs of the communities while maintaining routine services provided by governmental public health systems, including health messaging, epidemiology, and continuation of other day-to-day public health activities.
The consortium exists to be responsive to independent pharmacies and to facilitate collaboration with public health officials. Engagement with public health and emergency management can occur in parallel. Public health officials are encouraged to consider consistent and supportive integration of the consortium and independent pharmacies for future readiness and response initiatives. Research has validated the value of pharmacies in disease detection and emergency surge capacity, and the valuable roles that pharmacists play. Now is the time to address the need for collaboration between independent pharmacies and the government to solve operational barriers including service reimbursement, training, data sharing, and bidirectional communication. 37
To that end, independent pharmacy aggregators have compiled a list of actionable recommendations for sustainable public health partnerships at the local, state, and federal levels (Table). The recommendations are based on lessons learned and are grouped into 4 categories: agreements tailored for independent pharmacy aggregators, funded agreements, streamlined reporting, and sustained partnerships.
Recommendations for Sustained Public Health and Independent Pharmacy Aggregators
Abbreviations: ASPR, Administration for Strategic Preparedness and Response; CDC, US Centers for Disease Control and Prevention; CMS, Centers for Medicare and Medicaid Services; HHS, US Department of Health and Human Services; PIN, Personal Identification Number; PSAO, pharmacy services administrative organization.
Conclusion
Independent pharmacies are a vital force multiplier for public health and healthcare systems that require support to fill healthcare gaps, especially in rural settings and areas with measurable healthcare disparities. Consortium members are open to sharing real-time data on pharmacy access with decisionmakers in government. 41 Through the consortium leadership and the NCPA Innovation Center, new opportunities exist to fund engagement with the largest network of pharmacies in the United States. Relationships can be maintained and strengthened before the next public health emergency through continued public health engagement and structured public–private partnerships. Absent this effort, rapid deployment and realization of maximum potential of independent pharmacies in an emergency response will be diminished.
During the COVID-19 pandemic, community pharmacies endured the strain of unreimbursed services as a cost of doing business, aside from the undisclosed costs on the independent pharmacy aggregation organizations that saw no reimbursement for the data systems upgrades, pharmacist education, and federal coordination for delivery and reporting vaccine dispensing.26,42 Pilot projects and emergency planning with contracts and funding mechanisms in place would reinforce partnerships. In addition to providing funding, government entities such as pharmacy boards and public health departments should clearly define the legal and professional liabilities of community pharmacists. They should also establish consistent standards to ensure uniform patient care and clinical capabilities. 43 Supporting and partnering with the consortium facilitates planning, preparing and rapid engagement of all 18,900 independent pharmacies.
Footnotes
Acknowledgments
The authors thank the members of the Independent Community Pharmacy Consortium for Federal Government Engagement, all previous participants in the Federal Retail Pharmacy Program during the COVID-19 response, for their contributions to the discussions leading to this case study.