
Abstract
Immunotherapy with whole cell cancer vaccines has been tested in various tumor types. This study investigated the safety profile and antitumor activity of an allogeneic prostate carcinoma cell line, LNCaP, expressing recombinant human interleukin-2 and human interferon-γ. Thirty HLA-A*0201-matched patients with progressive, castration-resistant prostate cancer received four intradermal injections on days 1, 15, 29, and 92, and then every 90 days, as long as no tumor progression occurred. Three patients received a dose level of 7.5 million cells, and 27 patients received 15 million cells per injection. The primary study criteria were safety and the difference in prostate-specific antigen doubling time (PSA-DT), determined in the pretreatment phase (before the start of vaccination) and in the trial treatment phase (during vaccination). No dose-limiting or autoimmune toxicity was seen. During vaccination there was a significant prolongation of the PSA-DT compared with the prevaccination period (prolongation from 63 to 114 days; p < 0.01; intention to treat). In addition, results showed a period of PSA stabilization of at least 12 weeks, together with stable bone scans in 12 of 30 patients, and 3 patients sustained a >50% decrease in PSA versus baseline. The median overall survival time from first vaccination was 32 months (mean value, 34 months). Immune monitoring revealed T cell stimulation in the majority of patients. This vaccine strategy was found to be safe and well tolerated and was accompanied by prolongation of PSA-DT. The results of this trial warrant clinical development of this vaccine.
Introduction
The combination of these cytokines (IL-2 and IFN-γ) has already been used in clinical trials by other groups (Redman et al., 1990; Weiner et al., 1991; Margolin et al., 1992; Kim et al., 1996; Palmer et al., 1999; Negrier et al., 2000; Atzpodien et al., 2001).
Autologous and allogeneic whole cell vaccines that showed some promising results have already been tested in clinical trials up to phase III (Hsueh et al., 2002; Jocham et al., 2004; Simons et al., 2006; Small et al., 2006; Higano et al., 2008). The use of allogeneic irradiated whole tumor cells has clear advantages in terms of vaccine production and quality, and obviates the need to procure autologous tumor tissue for vaccine production.
Primary objectives of this study were to determine safety and tolerability of vaccination and to obtain evidence of antitumor activity in patients with progressive metastatic CRPC by assessing the difference in prostate-specific antigen doubling time (PSA-DT) determined during the prevaccination phase and during the treatment phase (Freedland et al., 2007; Tomioka et al., 2007; Scher et al., 2008). This trial was conducted in compliance with the trial protocol, Good Clinical Practice as defined by the International Conference on Harmonisation (ICH-GCP), and the applicable regulatory requirements. The trial protocol was approved by the Recombinant DNA Advisory Committee (RAC, NIH protocol no. 102) (Rosenberg et al., 1999, 2000) and the responsible ethics committee as well as the competent authorities in Germany.
Patients and Methods
Study design and patient selection
This trial was designed as an open-label, dose-escalating, single-center phase I/II study. Screening and treatment of patients were performed after written informed consent was obtained. Eligible patients had histologically proven adenocarcinoma of the prostate, serum testosterone less than 50 ng/dl, and an HLA-A*0201 allotype. Patients had received ongoing androgen deprivation therapy with a luteinizing hormone-releasing hormone analog or had undergone bilateral orchiectomy. Patients on maximal androgen deprivation underwent antiandrogen withdrawal before study entry. All patients had progressive CRPC defined as at least three consecutive increases in PSA, new metastatic lesion(s) on radionuclide bone scan, or progressive tumor lesions on examination and/or cross-sectional imaging.
Detailed inclusion and exclusion criteria have been published previously (Brill et al., 2007).
Vector and cells
Taking into account that HLA-A*0201 is the most frequent HLA-A allele in Western white individuals (40–50%), we chose the HLA-A*0201-positive prostate cancer cell line LNCaP (American Type Culture Collection [ATCC], Manassas, VA) for our vaccine platform. LNCaP cells are androgen sensitive and express PSA, prostatic acid phosphatase (PAP), prostate-specific membrane antigen (PSMA) (Lu and Celis, 2002) and prostate stem cell antigen (PSCA) (Simons et al., 1999; Kiessling et al., 2002), and a large number of other antigens that are not restricted to expression in prostate tissue, such as survivin, NY-ESO, and the proto-oncogene HER-2/neu. It is possible that gene transduction may alter antigen expression, and therefore we measured the levels of survivin expression both pre- and posttransduction at the mRNA and protein levels. Comparison by quantitative RT-PCR (qRT-PCR) with normal kidney tissue revealed a relative overexpression of survivin: 413-fold in LNCaP cells pretransduction and 576-fold in cells posttransduction. Intracellular staining showed protein expression in more than 85% of vaccine cells (data not shown).
However, LNCaP cells express only low levels of surface MHC class I molecules, as do the majority of human PC specimens obtained from patients undergoing radical prostatectomy or biopsy of metastatic lesions (Bander et al., 1997; Pandha et al., 2003). MHC I expression of LNCaP cells was increased 2-fold by exogenous IFN-γ treatment (Lee et al., 2000). Intradermal injection was chosen as the mode of delivery because of the abundance of Langerhans cells, that is, skin-residing dendritic cells, which constitute critical antigen-presenting cells for priming immune responses to tumor cells (Simons et al., 1999).
LNCaP cells were retrovirally transduced with an N2 vector, which is derived from the genome of the Moloney murine leukemia virus and contains the bacterial neomycin resistance gene (neo) as a selectable marker. By fusing DNA fragments encoding the major immediate-early human cytomegalovirus promoter and the herpes simplex thymidine kinase promoter with the human IFN-γ and human IL-2 cDNAs and cloning these fusion products into different sites of the N2 vector, an N/CIFN-γ/TIL-2 retroviral vector was established to infect LNCaP cells, resulting in IL-2 and IFN-γ secretion (Rosenthal et al., 1994). Manufacturing was conducted according to Good Manufacturing Practices (Molecular Medicine BioService, Carlsbad, CA). Immediately before administration, vaccine cells were thawed, washed three times with a 5% human albumin solution (Humanalbin; Aventis Behring, Marburg, Germany), counted and assessed for viability, lethally irradiated (150 Gy), and injected within a time frame of 2 hr.
Treatment, drug administration, and dose escalation
Patients were scheduled to receive four intradermal vaccine injections on days 1, 15, 29, and 92. In the absence of disease progression, patients received further vaccinations every 3 months. Designed as a dose-escalating study, the first three patients in the trial received a dose level of 7.5 × 106 cells in 1 ml of albumin solution (5%). Once safety at this dose was established (no dose-limiting toxicity) the next 27 patients received the second dose level of 15 × 106 cells.
Baseline/follow-up evaluations and safety assessment
Computed tomography (CT) or magnetic resonance (MR) imaging and radionuclide bone scans were performed within 4 weeks before study entry and repeated if abnormalities were noted or if progression of disease was stated by the principal investigator. Toxicity was graded on the basis of National Cancer Institute Common Toxicity Criteria, version 2.0 (see
Efficacy assessment
As primary efficacy assessment, PSA was determined at screening (prevaccination phase) via three successive measurements. PSA-DT based on the baseline PSA value determined at screening (third measurement) was calculated from the individual PSA values of each patient.
The secondary efficacy assessment included overall survival time (for all patients since time of first vaccination to date of last contact) and time to progression (PSA and radiologic). The PSA plateau of each patient was determined as the longest time period with an increment of PSA of less then 25% (Brill et al., 2007). Time to bone progression in patients with bone metastases was defined as the appearance of at least one new bone lesion on a bone scan.
Additional efficacy assessment: Immune monitoring, histopathology of vaccination sites, and artificial neural network analyses
The following studies were also performed: determination of (1) frequency of antigen-specific T cells (enzyme-linked immunospot [ELISPOT] analyses) and (2) cellular composition of vaccination sites (immunohistopathology), and (3) additional statistical analysis (artificial neural network [ANN] analyses).
ELISPOT analyses
To investigate the frequency of antigen-specific T cells at defined time points pre- and postvaccination, peripheral blood mononuclear cells (PBMCs) were directly stimulated in the IFN-γ ELISPOT analyses with HLA-A*0201 peptide ligands for various antigens. The potential peptide ligands were selected from sequences, using the HLA-A*0201 motif-based epitope predictions available on the web (Rammensee et al., 1999; Nussbaum et al., 2001) or as published in the literature. The following peptides were used: prostate-specific antigen PSA-123 (FLTPKKLQCVDLHVISNDVCAQV, amino acids 141–163, containing the peptides PSA-1, PSA-2, and PSA-3) (Correale et al., 1998), prostate-specific membrane antigen PSMA-P2 (ALFDIESKV, amino acids 711–719) (Salgaller et al., 1998), PSMA-P4 (VLAGGFFLL, amino acids 27–35) (Lu and Celis, 2002), prostate stem cell antigen PSCA-P3 (VLLALLMAGL, amino acids 4–13) (Matsueda et al., 2004), PSCA-P4 (ALQPGTALL, amino acids 14–22) (Dannull et al., 2000), EpCAM Ep-2H (heteroclitic ILYENNVIV, amino acids 184–192) (Trojan et al., 2001), prostate-specific G protein-coupled receptor PSGR-1 (ILLVMGVDV, amino acids 202–210) (Brill et al., 2007), six-transmembrane epithelial antigen of prostate STEAP-3 (LLLGTIHAL, amino acids 262–270) (Machlenkin et al., 2005), preferentially expressed antigen of melanoma PRAME-P4 (SLLQHLIGL, amino acids 425–433) (Kessler et al., 2001), prostatic acid phosphatase PAP-5 (ALDVYNGLL, amino acids 299–307) (Peshwa et al., 1998), Survivin-P1 (ELTLGEFLKL, amino acids 95–104) (Schmitz et al., 2000), Survivin-P2 (TLPPAWQPFL amino acids 5–14) (Schmitz et al., 2000), parathyroid hormone-related protein precursor PTH-r-P1 (YLTQETNKV, amino acids 103–111) (Yao et al., 2005), NY-ESO-1 (SLLMWITQC, amino acids 157–165) (Jäger et al., 1998), Her2/neu-P3 (ALCRWGLLL, amino acids 5–13) (Kawashima et al., 1998), and prostate carcinoma tumor antigen PCTA-1-P2 (IMVLKDKFQV, amino acids 106–115).
Peptide synthesis and in some cases vaccine cell lysate preparation were performed as described (Brill et al., 2007). As for the internal positive control, the CEF peptide pool (CMVpp65, NLVPMVATV, amino acids 495–503; EBV-BMLF1, GLCTLVAML, amino acids 280–288; EBV-LMP-2, CLGGLLTMV, amino acids 426–434; influenza M1 protein, GILGFVFTL, amino acids 58–66; and influenza RNA polymerase, PAFMYSDFHFI, amino acids 46–54) with 0.2 μg of each peptide per well (PANATecs, Tübingen, Germany) was used.
For ELISPOT analyses, preimmunization PBMCs (day 0), postimmunization PBMCs (post-1, day 8; post-2, day 22; post-3, day 36; and post-4, day 99), and PBMCs from two additional time points (days 57 and 183) were thawed, rested for 2 hr, and seeded at 1–2 × 105 cells in triplicate on antibody-precoated polyvinylidene difluoride (PVDF ) plates (Mabtech, Nacka, Sweden). Because of variation in the amount of PBMCs obtained from different patients at different time points it was not possible to test the T cells of every patient at every time point against the full set of peptides (but all data shown in Fig. 3 and in Tables 3 and 4 represent at least 22 patients). In subjects with long-lasting responses to the vaccine, additional samples were assayed in the same manner. PBMCs were stimulated directly with the peptides (5 μg/ml) in culture medium containing 10% human AB serum pretested for low background (Brill et al., 2007). Spots were counted with the AID reader system ELR03 with software version 4.0 (AID Autoimmun Diagnostika, Strassberg, Germany).
Histopathology
For histopathology of vaccination sites, all patients were asked to undergo a skin biopsy of a vaccination site 1 week after the first and third vaccinations. Immunostaining by heat-induced antigen retrieval was performed as described previously, using an automated immunostainer according to standard protocols (Brill et al., 2007).
Artificial neural network analysis
The clinical data, histopathology parameters, and immune monitoring data were evaluated by Mann–Whitney U test, receiver operator characteristic (ROC) analysis, χ2 test, and an artificial neural network (ANN) approach as published by other groups (Michael et al., 2005).
Before the development of a final ANN model, optimal input data were determined using the feature selection algorithms that are implemented in the network software. A probabilistic neural network approach was carried out that stepwise adds input variables and calculates the resulting predictive error. With the variables identified by the feature selection, the main network training process was started. For ANN analysis, linear scaling of input data (minimum, 0; maximum, 1) and Boolean representation of response status (patient group 1 = PSA plateau: 12 weeks = 1, patient group 2 = PSA plateau <12 weeks = 0) were performed, and the cases were subdivided into 60% training cases, 20% (blind) validation cases, and 20% (blind) test cases by random extraction for each new network. Five thousand different ANN models were built using different combinations of inputs and hidden nodes (multilayer perceptron model with a sigmoid activation function and a back-propagation algorithm) (Rumelhart et al., 1986). Training was stopped for each model when the error reached convergence. The best ANNs were selected according to their performance (correct prediction) in validation cases and test cases. Sensitivity analysis was performed on the best ANN models to determine the relative influence of the input variables.
Statistical considerations
Descriptive and inferential statistics of the primary and secondary efficacy parameters for the full analysis set and the per-protocol set were performed (Observed Cases approach). For inferential statistics, PSA changes from baseline were analyzed by Wilcoxon signed-rank test (α = 0.025, one-sided primary efficacy hypothesis) and Spearman rank correlation with stage and grading.
To analyze additional efficacy parameters the clinical data (physical examination and complete blood count), histopathology parameters, and immune monitoring data were recorded in one spreadsheet file and subsequently imported into the statistical software packages (SPSS 15 [SPSS, Chicago, IL]; STATISTICA 8 and STATISTICA Neural Networks 7 [StatSoft, Tulsa, OK]). Differences between group 1 patients and group 2 patients were analyzed by Mann–Whitney U test. ROC analysis was used to determine sensitivity and specificity of response assessment. p < 0.01 was regarded as significant. Furthermore, the data were evaluated by an artificial neural network approach similar to that described by Michael and colleagues (2005).
Results
Patient characteristics and treatment
A total of 95 patients were screened for the HLA-A*0201 allotype at the study center and 30 patients were enrolled in this trial. Of the 95 patients screened, 56 were not HLA-A*0201 positive (58%) and 9 met other exclusion criteria. It should be noted that the first 6 patients in this study are actually the phase I patients described in our previous publication (Brill et al., 2007). Thus the phase I part was not repeated, but all patients were included in this analysis. Detailed patient characteristics are provided in Table 1.
Abbreviations: EBRT, external beam radio therapy; KPS, Karnofsky performance status; PSA, prostate-specific antigen.
LNCaP is a well-characterized PC cell line originally isolated from a lymph node metastasis of a patient with PC. The retrovirally transduced LNCaP cells used in this trial secrete measurable amounts of IL-2 (30 U/106 cells per 24 hr) and IFN-γ (6 U/106 cells per 24 hr). LNCaP cells, in contrast to other PC cell lines used as cancer vaccines, do not express transforming growth factor (TGF )-β (see Fig. 1).
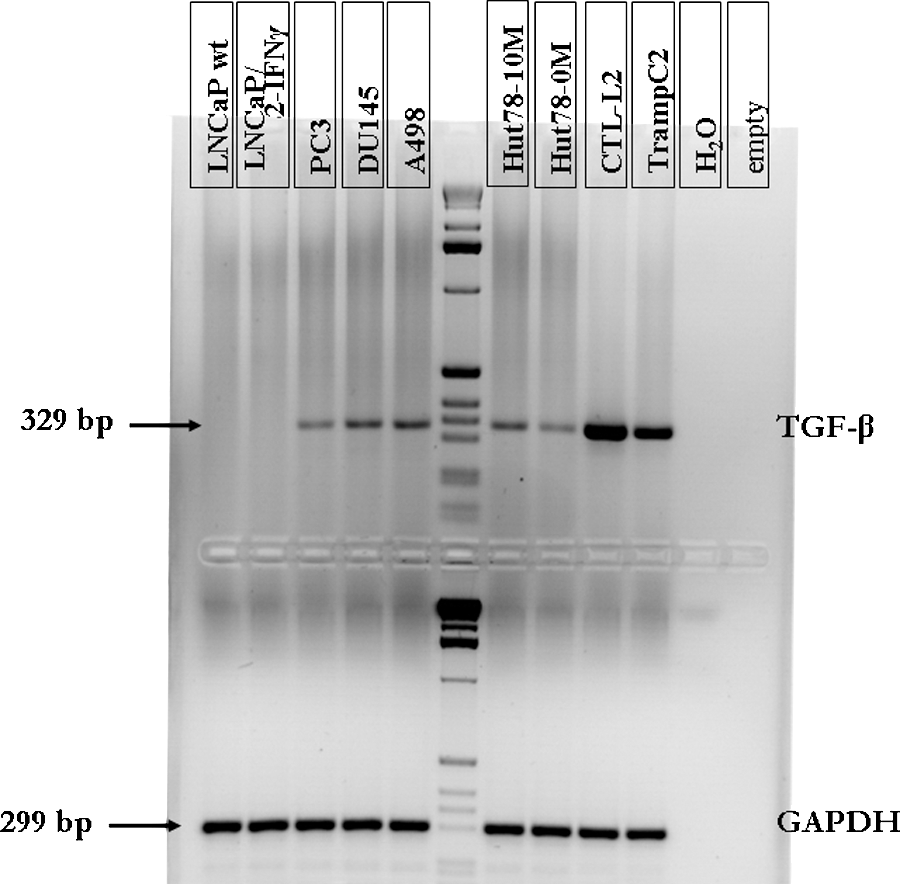
Transforming growth factor (TGF )-β expression in various prostate cancer (PC) cell lines. A498, human renal epithelial cell line; LNCaP/IL-2/IFN-γ, vaccine cells; LNCaPwt, untransfected LNCaP cells; PC3, DU145, and TRAMP-C2, PC cell lines; Hut78-10M and Hut78-0M, human tumor cell line with 10 or 0% medium, respectively; CTL-L2, T cell line; GAPDH, housekeeping gene (glyceraldehyde-3-phosphate dehydrogenase); bp, base pairs.
All enrolled patients received at least three vaccinations with LNCaP(IL-2/IFN-γ) cells, resulting in a minimal time on vaccination therapy of 29 days. Twenty-three patients completed the trial, being vaccinated at least four times (vaccination period between 13 and 138 weeks; 4 to 14 vaccinations). Seven patients were withdrawn after the three priming vaccinations but before the booster vaccination, because of disease progression. The number of patients in the safety set, the full analysis set, and the per-protocol set was n = 30.
Toxicity
No grade 4 toxicity occurred on study and no patient discontinued because of drug-related adverse events. During the course of this trial, all patients experienced a total of 117 adverse events (AEs). In four patients seven serious AEs (SAEs) (including three laboratory AEs) occurred. The most frequently reported AEs were injection site erythema (30 patients), bone pain (6 patients), nasopharyngitis (5 patients), and vomiting and headache (4 patients each). Toxicity details are listed in Table 2.
>3.5%; safety set; n = 30.
Clinical results
The primary efficacy objective was to evaluate the difference in PSA-DT between the prevaccination phase and the treatment phase. A total of 22 of 30 patients showed a prolonged PSA-DT during the treatment phase. Eight of 30 patients showed a decrease in the resulting PSA-DT. The median PSA-DT was 63 days during the prevaccination phase and 114 days during the vaccination (i.e., treatment) phase (p = 0.0035). Figure 2A shows a box-and-whisker plot of pre- and posttreatment PSA kinetics (full analysis set; n = 30). Median time to bone progression was 6 months in patients with bone metastases at baseline (see Fig. 2B).

Clinical results. (
Secondary efficacy objectives included overall survival time determined for 30 patients. A total of 24 patients died during follow-up, 17 of them due to PC and 7 due to other reasons than PC. Six patients are still alive at 5 years of follow-up. The median overall survival time (intention to treat [ITT]) since first vaccination was 32 months (mean value, 34 months). PSA values during vaccination with LNCaP(IL-2/IFN-γ) cells initially showed an ongoing increase followed by a period with stable or decreasing PSA values (PSA plateau), before a new phase of increase (+25% cutoff; Brill et al., 2007). The PSA plateau was estimated by the SAS procedure NLIN, wherein a piecewise linear model with possible plateau (i.e., approximately constant part) was fitted. The duration of PSA stabilization varied from individual to individual (mean value, 2 months [ITT]; maximum of 21 months). Twelve of the 30 patients showed a PSA plateau for 12 weeks or longer (data not shown).
Three of 30 patients sustained a >50% decrease in PSA versus baseline (patient 113: PSA decreased from 2.5 to 0.3 ng/ml with a time below the 50% level of 68 weeks; patient 125: 126.0 to 14.0 ng/ml, 19 weeks; patient 184: 8.0 to 0.6 ng/ml, 25 weeks).
Additional efficacy assessment: Immune monitoring, artificial neural network analyses, and histopathology of vaccination sites
Immune monitoring
In all patients, IFN-γ-secreting T cells with peptide reactivity could be observed, with time courses showing variability among individuals. By ELISPOT analysis of all 30 patients, at least a 2-fold increase in antigen-specific T cells was seen in most of the patients, with variations in the numbers of reactive T cells and peptide specificity between pre- and posttreatment samples. Table 3 summarizes the prevaccine response measured on day 0 versus the maximal response to each antigen detected at any time point in the vaccine schedule. For example, in one patient (patient 113) showing a prolonged and late onset of serum PSA decrease (90% decrease with nadir on day 246), the increase in numbers of specific T cells was detectable at later time points. This patient showed no increase in specific T cells in the periphery before study day 365 (seventh vaccination), with an exception for PSGR-1 and PSMA-P2 and -P4 after the second and third vaccinations (data not shown). As no correlation could be drawn by a simple comparison between PSA course and ELISPOT data, artificial neural network (ANN) analysis was performed to generate new hypotheses for further consideration.
Abbreviations: PSA, prostate-specific antigen; PSGR, prostate-specific G protein-coupled receptor; STEAP, six-transmembrane epithelial antigen of prostate; PAP, prostatic acid phosphatase; PSCA, prostate stem cell antigen; PSMA, prostate-specific membrane antigen; PRAME, preferentially expressed antigen of melanoma; PTH-rP, parathyroid hormone-related protein precursor; PCTA, prostate carcinoma tumor antigen.
Per 150,000 cells pre/postvaccination.
Values represent absolute numbers of spots for pre- and postvaccination (pre/post) responses. These values are given after subtraction of background responses. Values representing a greater than 2-fold increase in reactivity against the peptides post- versus prevaccination are indicated in boldface. Empty fields, not tested.
Values indicate the number of patients with reactivity (more than 2-fold increase post- versus prevaccination) in comparison with the number of patients tested against the respective antigen.
Patients were divided into two groups, with the first group (group 1; n = 12) showing a PSA plateau for at least 12 weeks, together with a stable metastatic state during the time of PSA plateau (Scher et al., 1999, 2005), and the second group (group 2; n = 18) showing a shorter or no PSA plateau. These two groups showed a significant difference in their reactivity against survivin-P1/P2 on day 36 (Fig. 3). Group 1 showed higher reactivity than group 2. The p value for this difference was calculated as p = 0.007 in ROC analysis, and the area under curve was 0.829 (95% confidence interval, 0.646–1.012). There were no differences in reactivity against the vaccine cell lysates on day 0 between groups 1 and 2 (data not shown).

T cell reactivity against survivin-P1/P2 peptides in group 1 (n = 12) and group 2 (n = 18) patients on day 36 (shown as box-and-whisker plots; boxes represent the interquartile range (upper quartile, median, and lower quartile), and whiskers show the highest and lowest values; p value determined by Mann–Whitney U test).
Artificial neural network analysis
The initial input data selection procedure on ELISPOT data identified a set of 19 variables. These were used to train 5000 ANN models with different input subsets and different numbers of hidden nodes. The best network model was able to detect a group 1 patient and a group 2 patient reactivity pattern with 86, 75, and 75% accuracy, respectively, for training, (blind) validation, and (blind) test data, respectively. This ANN used 7 of the preselected 19 input variables. Sensitivity analysis was carried out to estimate the influence of each variable on the network's decision (Table 4). The highest influence on the network's decision had survivin reactivity on day 36.
Histopathology of vaccination sites
Morphological examination of the biopsy sites revealed significant interindividual variation in the intensity of the inflammatory infiltrate. The magnitude of the inflammatory cell response at the injection sites appeared to increase according to the numbers of vaccine cells injected. In the biopsies, none of the residual vaccine cells were identified morphologically or by immunostaining for pan-cytokeratin (data not shown). The inflammatory infiltrate was usually located around dermal vessels and in the adjacent subcutaneous fatty tissue. A minority of biopsies with marked inflammation showed a significant admixture of eosinophils within the infiltrate. Phenotypically, CD3+ T cells predominated over B cells in all cases. The CD4:CD8 ratio varied but showed an increase with increasing inflammation and for the third in comparison with the first vaccine application (data not shown). The CD4:CD8 ratio was higher in patients of group 1 than in group 2 (p = 0.02; data not shown). The number of CD56+ natural killer (NK) cells was always low. CD68+ macrophages were only mildly increased.
Discussion
Historically, prostate cancer has been regarded as a nonimmunogenic cancer. Several clinical trials using different vaccine strategies have induced antitumor immunity and have shown moderate clinical response rates (Jocham et al., 2004; Webster et al., 2005; Small et al., 2006; Higano et al., 2008, 2009). In contrast to the other trials, we have used a single cell line, LNCaP, genetically modified with IFN-γ and IL-2 to enhance the presentation of potential tumor-associated antigens and to augment antigen-specific T cell frequencies. In a previous study, we have shown that immunotherapy of PC with this vaccine platform is safe and feasible (Brill et al., 2007). Now we show that whole tumor cell vaccination can influence PSA-DT without inducing significant toxicity. Compared with other whole cell vaccination trials we used relatively low numbers of vaccine cells (e.g., 15 million cells vs. up to 300 million cells) (Higano et al., 2008). PSA-DT is a strong prognostic parameter used in many trials (Michael et al., 2005; Oudard et al., 2007; Dreicer et al., 2008), and proposed by the PSA Working Group to measure therapeutic activity (Arlen et al., 2008), and was used as our primary end point. The median PSA-DT was 63 days during the prevaccination phase and 114 days during the treatment phase (p = 0.0035). It is unlikely that our vaccination selectively eliminated high PSA-producing tumor cells, although not impossible. Median time to bone progression was 6 months. In symptomatic patients with CRPC, the median time to progression has been reported to be about 3 months (Small et al., 2000). Skin biopsies taken from the injection sites clearly demonstrated that we induced strong immune responses against vaccine cells. The injected cells were effectively destroyed and were not present in any day 7 injection site biopsies. The combination of alloantigens with IL-2 and INF-γ led to the induction of a mononuclear cell infiltrate at the injection site. The absence of TGF-β expression by the vaccine cells is certainly helpful, because IL-2 and TGF-β are known to play a central role in the activation and maintenance of the induced form of T regulatory cells (iTreg). On the other hand, it is possible that the IL-2 secreted by our vaccine cells induces proliferation and survival of recently activated effector T cells, but at the same time possibly counteracts this effect by stimulating Tregs locally (Huter et al., 2008; Zheng et al., 2008).
Our study population consisted of white men with a median age of 63.5 years and a median prevaccination PSA of 19.6 ng/ml. Immunotherapy approaches are useful in the setting of low tumor burden and low antigen load and less likely to work if large tumor masses are already established.
As expected, immune monitoring revealed variable reactivity in the study subjects. All patients showed an increase in T cell frequencies specific for several peptides used for analysis, but there was no correlation between PSA course and ELISPOT reactivity, confirming many previously published reports. Artificial neural network (ANN) analysis is particularly useful to analyze the complex set of immune monitoring data in a comprehensive manner, allowing individual classification of patients (Krogh, 2008). ANN analysis and other artificial intelligence methods have been used in various medical studies, including urological tumors (Michael et al., 2005; Abbod et al., 2007). Therefore, we used ANNs in addition to conventional statistical methods to analyze the immune monitoring data in our study, similar to the strategy of Michael and colleagues in their PC vaccination trial (Michael et al., 2005). Nonparametric comparison of ELISPOT reactivity by Mann–Whitney U test, ROC analysis, and the ANN approach showed similar results with respect to discrimination between the subgroups of patients. All three approaches identified consistent ELISPOT reactivity against survivin on day 36 as the most important factor. Similar results–enhanced reactivity against the tumor-associated antigen survivin–were shown by others in patients with cancer undergoing radiation therapy (Schaue et al., 2008). These results confirm that special immune reactivity patterns can be used to predict the response to cancer immunotherapy. ANN analysis deserves further evaluation as a promising tool for the analysis of complex immunological data, in the hope that patterns defined by ANN analysis could be used to predict the response of patients to cancer vaccines in further clinical trials.
In summary, our data suggest that vaccination with LNCaP secreting IL-2 and IFN-γ can prolong the PSA-DT. Additional studies must be completed to determine whether this type of vaccination will have an impact on the survival of patients with CRPC.
Footnotes
Acknowledgments
The authors gratefully acknowledge the patients and their families for active participation, and the hospital staffs (Urology: G. Kugler, J. Spiess; Laboratory of Tumor Immunology: B. Stadlbauer; Radiation Therapy: G. Sieler, F. Wuehrschmitt; Institute for Experimental Oncology: E. Hammerschmid, G. Stejskal) for excellent collaboration. This work was supported in part by research grant 01GE9625 from the BMBF (B.G.), Vakzine Projekt Management (B.G.), ClinCorpGroup (H.P.), and the Helmholtz Alliance on Immunotherapy of Cancer (D.J.S.).
Author Disclosure Statement
For T.H.B, no competing financial interests exist; for H.R.K., no competing financial interests exist; for H.P. no competing financial interests exist; for A.B. no competing financial interests exist; for F.F. no competing financial interests exist; for T.S. no competing financial interests exist; for H.R. no competing financial interests exist; for R.P. no competing financial interests exist; for T.K. no competing financial interests exist; for C.P. no competing financial interests exist; B.E. is an employee of Vakzine Project Management; for J.B. no competing financial interests exist; for R.H. no competing financial interests exist; for D.J.S. no competing financial interests exist; for B.G. no competing financial interests exist.