
Abstract
Hereditary inclusion body myopathy (HIBM) is an autosomal recessive adult-onset myopathy due to mutations in the GNE (UDP-N-acetylglucosamine 2-epimerase/N-acetylmannosamine kinase) gene. Affected patients have no therapeutic options. We have previously demonstrated in preclinical testing the ability to safely correct GNE gene function through liposomal delivery of the wild-type GNE gene. Results were verified in a single patient treated by intravenous infusion of GNE gene lipoplex. A single patient (patient 001) with severe HIBM treated with a compassionate investigational new drug received seven doses of GNE gene lipoplex via intravenous infusion at the following doses: 0.4, 0.4, 1.0, 4.0, 5.0, 6.0, and 7.0 mg of DNA. GNE transgene expression, downstream induction of sialic acid, safety, and muscle function were evaluated. Transient low-grade fever, myalgia, tachycardia, transaminase elevation, hyponatremia, and hypotension were observed after infusion of each dose of GNE gene lipoplex. Quadriceps muscle expression of the delivered GNE, plasmid, and RNA was observed 24 hr after the 5.0-mg dose and at significantly greater levels 72 hr after the 7.0-mg infusion in comparison with expression in quadriceps muscle immediately before infusion. Sialic acid-related proteins were increased and stabilization in the decline of muscle strength was observed. We conclude that clinical safety and activity have been demonstrated with intravenous infusion of GNE gene lipoplex. Further assessment will involve a phase I trial of intravenous administration of GNE gene lipoplex in individuals with less advanced HIBM with more muscle function.
Introduction
We constructed a GNE-wt-DNA vector, using human GNE cDNA and the pUMVC3 expression vector. Transgene expression of GNE mRNA and GNE/MNK protein, in correlation with subsequent increased production of sialic acid, was demonstrated in vitro (Jay et al., 2008). We also complexed the GNE expression vector with a cationic liposome, composed of 1,2-dioleoyl-3-trimethylammonium-propane (DOTAP) and cholesterol (GNE gene lipoplex) and demonstrated dose-related safety in BALB/c mice (Phadke et al., 2009). Moreover, we demonstrated safety and a durable improvement in local regional skeletal muscle function of a single severely affected patient with HIBM (patient 001) in correlation with GNE transgene upregulation and local induction of sialic acid production after a series of local regional intramuscular injections of the GNE gene lipoplex (Nemunaitis et al., 2010). We now report safety and response after a series of dose-escalating intravenous infusions of GNE gene lipoplex into patient 001.
Materials and Methods
Study design
The subject received GNE gene lipoplex mixed with 250 ml of D5W (5% dextrose in water) every 60 days, administered via 30-min intravenous infusions for seven doses (0.4, 0.4, 1.0, 4.0, 5.0, 6.0, and 7.0 mg). The subject was premedicated with oral dexamethasone and a combination of intravenous histamine H1 and H2 blockers, oral indocin, and oral acetaminophen. After injection of the GNE gene lipoplex, the subject was observed for 4 hr. During the observation period, vital signs were taken every 30 min for the first hour, and then every hour until hour 4. Vital signs during this period included blood pressure, temperature, pulse, respiration, and oxygen saturation. Toxicities were graded and reported according to the National Cancer Institute (NCI, Bethesda, MD) Common Terminology Criteria for Adverse Events (CTCAE), version 3.0. The subject was assessed for GNE gene expression, sialic acid production, and muscle strength before treatment with GNE gene lipoplex.
The histopathology and quantitative assessment of GNE transgene expression and sialic acid levels of the quadriceps muscle were assessed through sequential biopsy done at baseline (right quadriceps) before injection of the 5- and 7-mg doses of GNE gene lipoplex and at 24 hr (for the 5-mg dose) and 72 hr (for the 7-mg dose), both involving the right quadriceps after intravenous infusion.
Muscle strength was measured by force generation of selected muscles, using a break test technique (Bohannon, 1988, 1992; Stratford and Balsor, 1994; Burns et al., 2005) with a handheld dynamometer (HHD). Isokinetic muscle function testing with an HHD has previously been done to assess quantitative changes in muscle strength (Andres et al., 1986; Mendell et al., 1989; Florence et al., 1992; Personius et al., 1994; Roy and Doherty, 2004; Paternostro-Sluga et al., 2008). In our study, muscle force generation was measured with a Chatillon FCE-200 digital HHD (AMETEK, Largo, FL). It uses a digital ordinal scale for the measurement of muscle force in pounds, kilograms, or newtons. This dynamometer displays force measurements to the nearest 0.2 lb to a maximum of 200 lb for a total of 1000 potential muscle force readings.
Muscle strength was tested preinjection and on days 1, 2, and 30 after each injection. Thirty muscle groups were tested for muscle strength over time with an HHD, before the first intramuscular injection and subsequently thereafter: 4 muscle groups in the neck, 2 in the shoulders, 10 in the legs, and 14 in the arms (including the injected muscles). The muscle groups tested included the right lateral neck flexors, left lateral neck flexors, forward neck flexors, neck extensors, shoulder elevators, elbow flexors, wrist extensors, elbow extensors, finger flexors, finger extensors, finger abductors, thumb extensors, hip flexors, knee extensors, ankle dorsiflexors, long toe extensors, and ankle plantar flexors. Before the first intravenous injection, four additional muscle groups were added for testing: right and left sides for wrist flexion and forefoot flexion.
The break technique requires the examiner to overpower a maximal effort by the subject, thereby producing a measurement of eccentric muscle strength. Ten repeat measurements were taken for each muscle at each time point.
A symptom-directed physical examination was performed at baseline and on days 3, 8, 15, and 30 of each cycle. Blood studies (complete blood count [CBC], chemistry, creatine phosphokinase [CPK], aldolase, erythrocyte sedimentation rate [ESR], and C-reactive protein [CRP]) were done at baseline and on days 3, 8, 15, and 30 of each cycle. Long-term follow-up involved physical examination, blood studies (CBC and chemistry) and muscle strength testing on days 60, 90, 120, 150, and 180. Pulmonary function studies were performed in an independent laboratory by a certified technician, in accordance with American Thoracic Society guidelines, with an ongoing quality control program (American Thoracic Society, 1991, 1995). Pulmonary function studies were done every 2 months (at baseline and before each subsequent injection).
Study population
A single patient with HIBM was enrolled. The following inclusion criteria were met: (1) the ability to understand and the willingness to sign a written informed consent; (2) histological and genotypic confirmation of HIBM; (3) no acceptable effective treatment options; (4) age >18 years; (5) life expectancy greater than 3 months; and (6) normal organ and marrow function defined as leukocytes (>3000/μl), absolute neutrophil count (>1500/μl), platelets (>100,000/μl), total bilirubin (within normal institutional limits), aspartate transaminase (AST; serum glutamic oxaloacetic transaminase [SGOT])/alanine transaminase (ALT; serum glutamic pyruvic transaminase [SGPT]) (<2.5 × institutional upper limit of normal), creatinine (within normal institutional limits), and creatinine clearance (>60 ml/min/1.73 m2 for patients with creatinine levels above institutional normal limits).
The patient was not receiving any other investigational agents, had no history of allergic reactions attributed to compounds of similar chemical or biological composition, had no uncontrolled intercurrent illness, was not pregnant or nursing, and was not HIV positive.
GNE gene lipoplex
The DNA vector is composed of a 2169-base pair wild-type human GNE1 isoform (NCBI reference sequence NM_005476.3) driven by the cytomegalovirus (CMV) promoter. The plasmid backbone is the pUMVC3 vector from Aldevron (Fargo, ND). Further details about the vector construction can be found in our previous publication (Jay et al., 2008). The liposome delivery vehicle is composed of a 10:9 molar ratio of two lipids, DOTAP and cholesterol (Templeton et al., 1997). The GNE gene lipoplex size ranged from 400 to 500 nm and the ζ potential ranged from 50 to 59 mV. The final product was suspended in D5W USP for a total volume of 100 μl/injection. Manufacturing details are provided in prior work (Nemunaitis et al., 2010).
The final product consisted of 4 mM DOTAP:cholesterol and GNE DNA (0.5 μg/μl).
Real-time quantitative PCR analysis
We used a method of reverse transcription to convert total RNA into cDNA. Extracted total genomic DNA and converted cDNA were analyzed via quantitative PCR (qPCR) relative to a known standard to quantitate the unknown samples. This method has been previously described (Jay et al., 2008; Phadke et al., 2009). Briefly, tissues were homogenized with a TissueLyser (Qiagen, Valencia, CA), and total nucleic acid was extracted with RNeasy and DNeasy kits (Qiagen). One microgram of total RNA was used as starting material for cDNA synthesis, using a Bio-Rad (Hercules, CA) iScript cDNA kit. GNE-specific primers were designed so that only the plasmid (recombinant GNE transcript, rGNE) would be amplified without cross-reacting with the endogenous GNE mRNA.
Histological analysis
Single needle core biopsies taken from the right quadriceps muscle at baseline and 24 hr after the fifth intravenous infusion (5 mg) were formalin fixed and paraffin embedded (FFPE). Slides were prepared, stained with hematoxylin and eosin (H&E), and analyzed by a certified pathologist (Propath, Dallas, TX).
Immunohistochemical analysis
FFPE sections were deparaffinized and rehydrated. For lectin stains, sections were blocked with 0.1% bovine serum albumin (BSA) and labeled with fluorescein isothiocyanate-conjugated wheat germ agglutinin (FITC–WGA), FITC-conjugated peanut agglutinin (FITC–PNA), or FITC–Jacalin (jackfruit agglutinin) (EY Laboratories, San Mateo, CA) for 1 hr at room temperature. For polysialylated neural cell adhesion molecule (PSA-NCAM), antigen retrieval was performed with 0.1 M sodium citrate, and sections were blocked with 1% BSA and labeled with mouse anti-PSA-NCAM (Chemicon International/Millipore, Temecula, CA) overnight at 4°C followed by Alexa 555-conjugated goat anti-mouse (Molecular Probes/Invitrogen, Carlsbad, CA). Imaging was done with an LSM 510 Meta confocal microscope (Carl Zeiss, Thornwood, NY).
Statistical analysis
Statistical analysis was performed on the HHD data generated for each muscle group. Separate comparison of the mean muscle strength at each time point was made with the baseline mean for each muscle, using the Student t test.
Results
Patient description
Patient 001 is a 41-year-old female who developed muscle weakness at age 18. She has experienced typical disease progression and gradually lost muscle mass and function over the last 23 years. Diagnosis of HIBM on the basis of molecular criteria revealed compound heterozygosity for GNE gene mutations in exon 7 (c.1132G>T; p.D378Y) and in exon 11 (c.1892C>T; p.A631V). Both mutations were previously reported in HIBM (Eisenberg et al., 2003; Huizing and Krasnewich, 2009). The disease-specific family history was negative.
The GNE gene lipoplex investigational new drug (IND) was initially approved by the U.S. Food and Drug Administration (FDA) in July 2008 for a single patient intramuscular injection trial and later amended for administration of intravenous injections. Patient 001 received four intramuscular doses of GNE gene lipoplex (0.4 mg of DNA for first intramuscular injection and 0.2 mg of DNA for each of the next three intramuscular injections) and demonstrated local injected muscle strength improvement in correlation with GNE transgene and sialic acid increase on day 3 after injection compared with baseline before the first injection. Transient grade 1/2 flulike symptoms and transaminase elevation were observed within 24 hr of each dose (Nemunaitis et al., 2010). Deterioration of diaphragm and intercostal muscle strength justified the protocol amendment to explore intravenous testing.
Safety
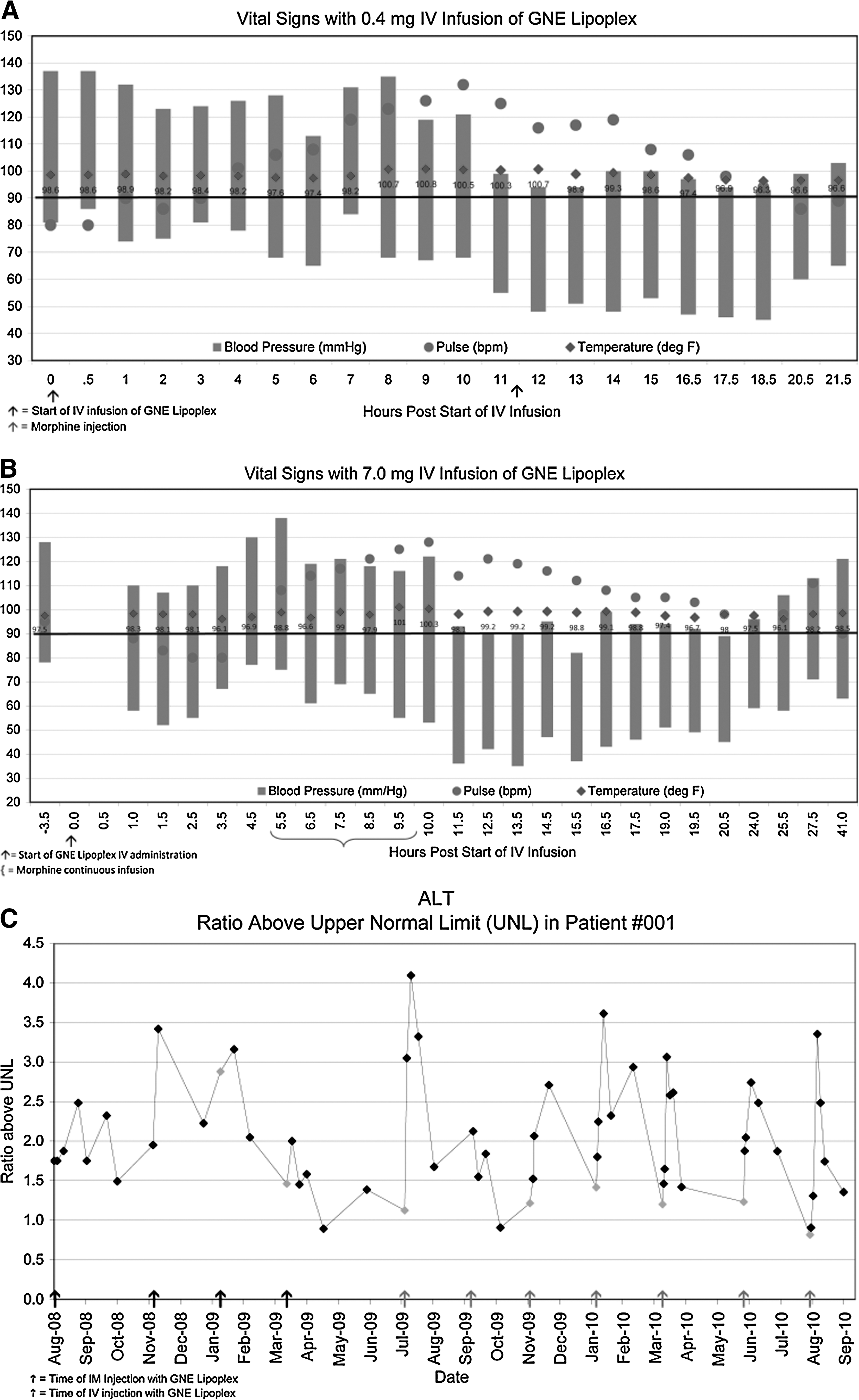
Patient 001 treatment with intravenous GNE gene lipoplex was well tolerated. Within 24 hr of each cycle, a low-grade fever of 100°F developed (Fig. 1A–C). This was associated with transient grade 1/2 myalgias, tachycardia, hypotension, and liver enzyme elevation (from grade 1 pretreatment baseline) after each dose (Fig. 1A–C). At 48 hr, myalgias diminished and tachycardia, hypotension, and fever resolved. No evidence of myalgia was detected 1 week after the administration of each dose. Slightly greater duration of myalgias, tachycardia, and hypotension was observed at the 7.0-mg dose (Fig. 1B), although no grade 3 or greater toxic effect was observed. Consistent grade 1–2 hyponatremia, transiently associated with each dose greater than or equal to 1.0 mg, was also observed (Fig. 2).
(

Relationship of blood sodium level in patient 001 to time of dose with GNE gene lipoplex. Gray shading represents the normal value range used by the laboratory. Light gray symbols indicate the value before treatment.
Muscle function
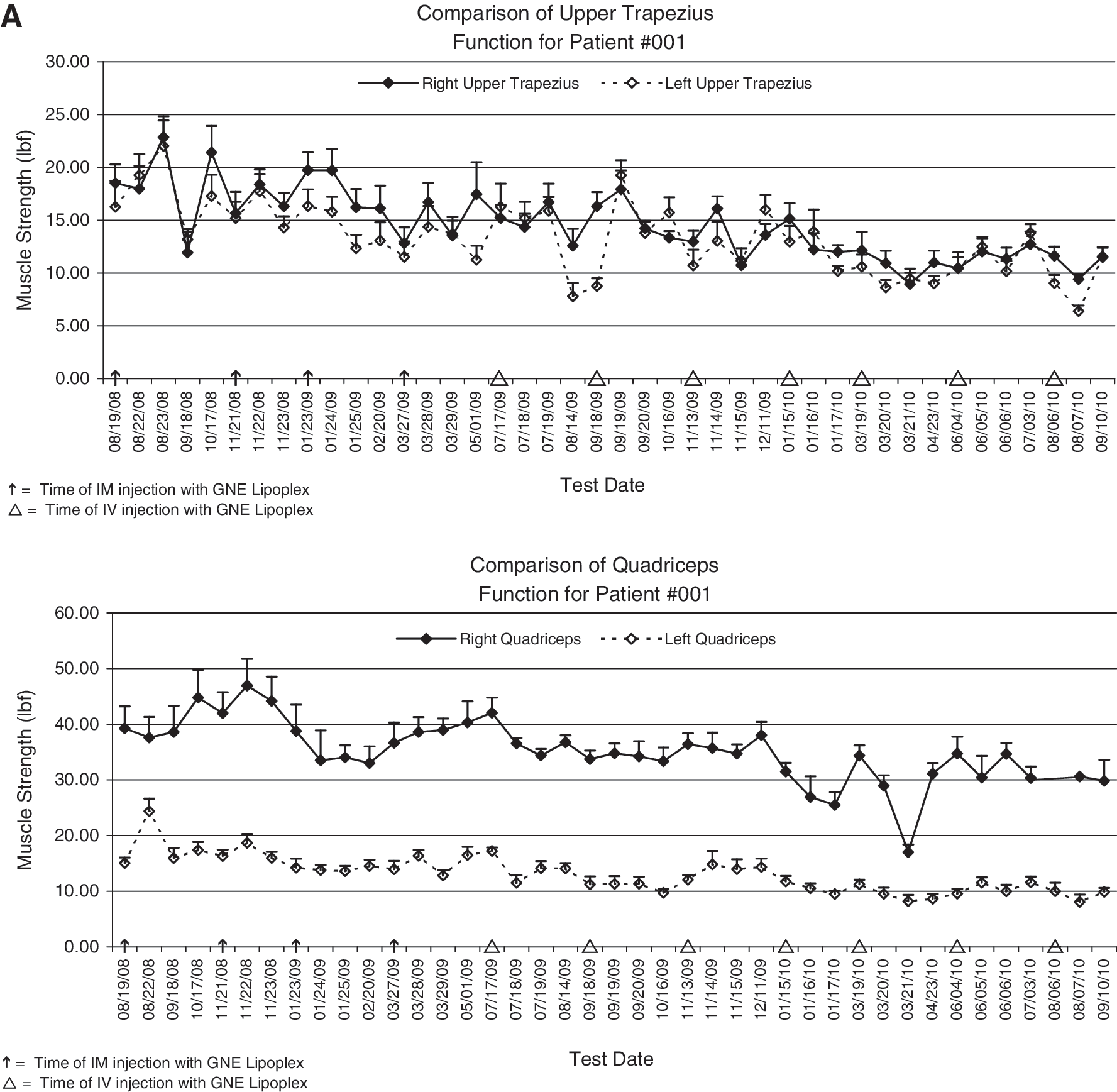
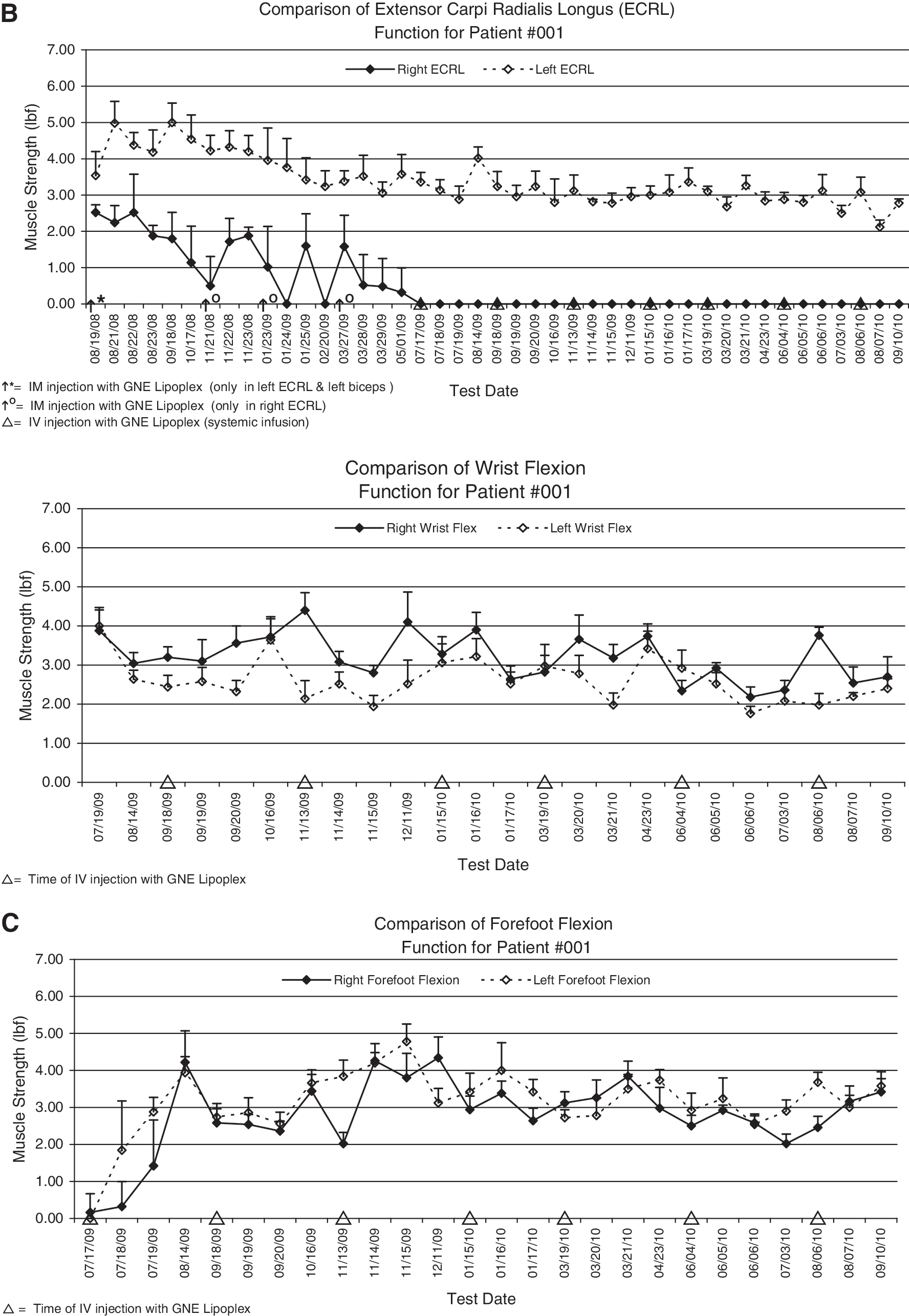
Muscle strength testing with a dynamometer revealed a variable distribution of skeletal muscle functional changes manifested by a loss of force generated in some muscles (e.g., upper trapezius and quadriceps; Fig. 3A), stabilization in others (extensor carpi radialis longus, and wrist flexion; Fig. 3B), and rare improvement in others (forefoot flexion; Fig. 3C).
(
However, manual muscle testing on patient 001 suggested overall stabilization of muscle function. The following muscle groups were tested on each side of the body, using the Medical Research Council (MRC) Scale (Medical Research Council, 1981): elbow flexors, wrist extensors, elbow extensors, finger flexors, finger abductors, hip flexors, knee extensors, ankle dorsiflexors, long toe extensors, and ankle plantar flexors. The sum of the motor scores from the 20 muscles was defined as the total motor score.
Review of past records revealed several incomplete and complete manual muscle examination records on the 20 muscles that were used for this study. The first recorded examination was on February 5, 1992, which revealed a total motor score of 61 and subsequently a total motor score of 55 on April 9, 1998.
Regular manual muscle testing by a single examiner on a monthly basis started on March 16, 2007 and continues to date (Fig. 4). The total motor score on her initial examination on March 16, 2007 was 34. She had her first intramuscular GNE gene lipoplex injection on August 19, 2008 and before the injection a total motor score of 25 was recorded. The first intravenous GNE gene lipoplex infusion was on July 17, 2009 and her total motor score before the injection was still 25. The last examination, on September 10, 2010, 1 month after her most recent intravenous GNE injection, revealed a total motor score of 23. The recorded total motor score dropped 27 points from 1992 to 2007, and then dropped 9 points during the first 5 months of the study period. After GNE gene lipoplex administrations her total motor score dropped only 2 points over the next 24 months from 2008 to 2010 (Fig. 4). These results are suggestive of stabilization of muscle function during GNE gene lipoplex treatment.
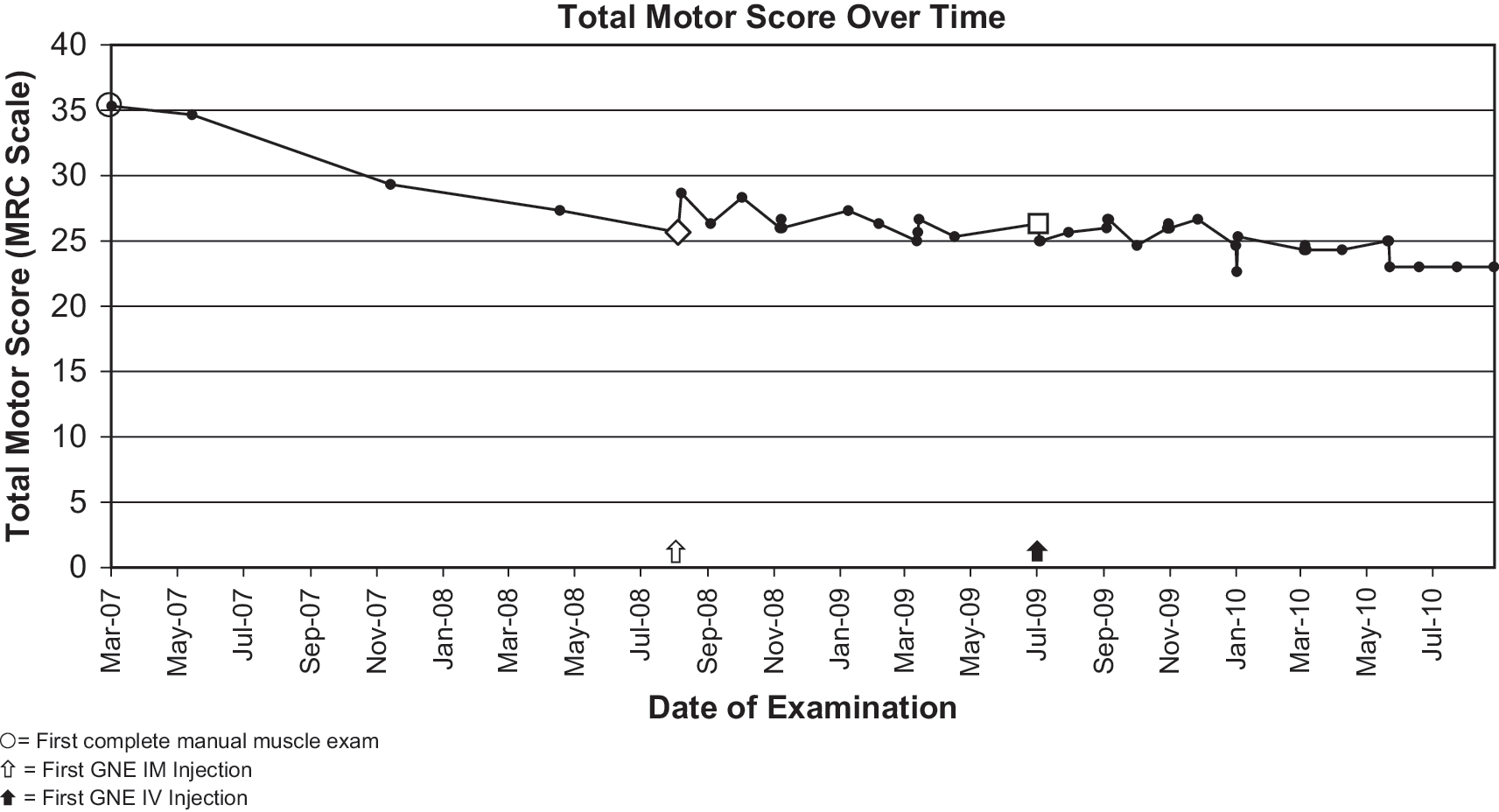
Progression of muscle weakness (Total Motor Score) over time (years) in patient 001. The diamond indicates the value before the first intramuscular injection. The square indicates the value before the first intravenous injection.
In addition, the May 29, 2007 (first examination by dynamometer) results revealed 18 of 30 muscles producing force. Seventeen months later, at the time of first intramuscular injection of GNE gene lipoplex, seven more muscles had lost the ability to produce force. However, during the 24 months of treatment with intramuscular and intravenous GNE gene lipoplex, no additional muscles lost significant detectable force by dynamometer measurement. In fact, one additional muscle recorded generated force. Pulmonary function as an assessment of diaphragm and intercostal muscle strength was determined by monitoring forced vital capacity (FVC). Pulmonary function appeared to stabilize as well, as highlighted by FVC in comparison with baseline and prior pulmonary function tests (PFTs) in correlation with improved ability to sleep in a flat position (Fig. 5).
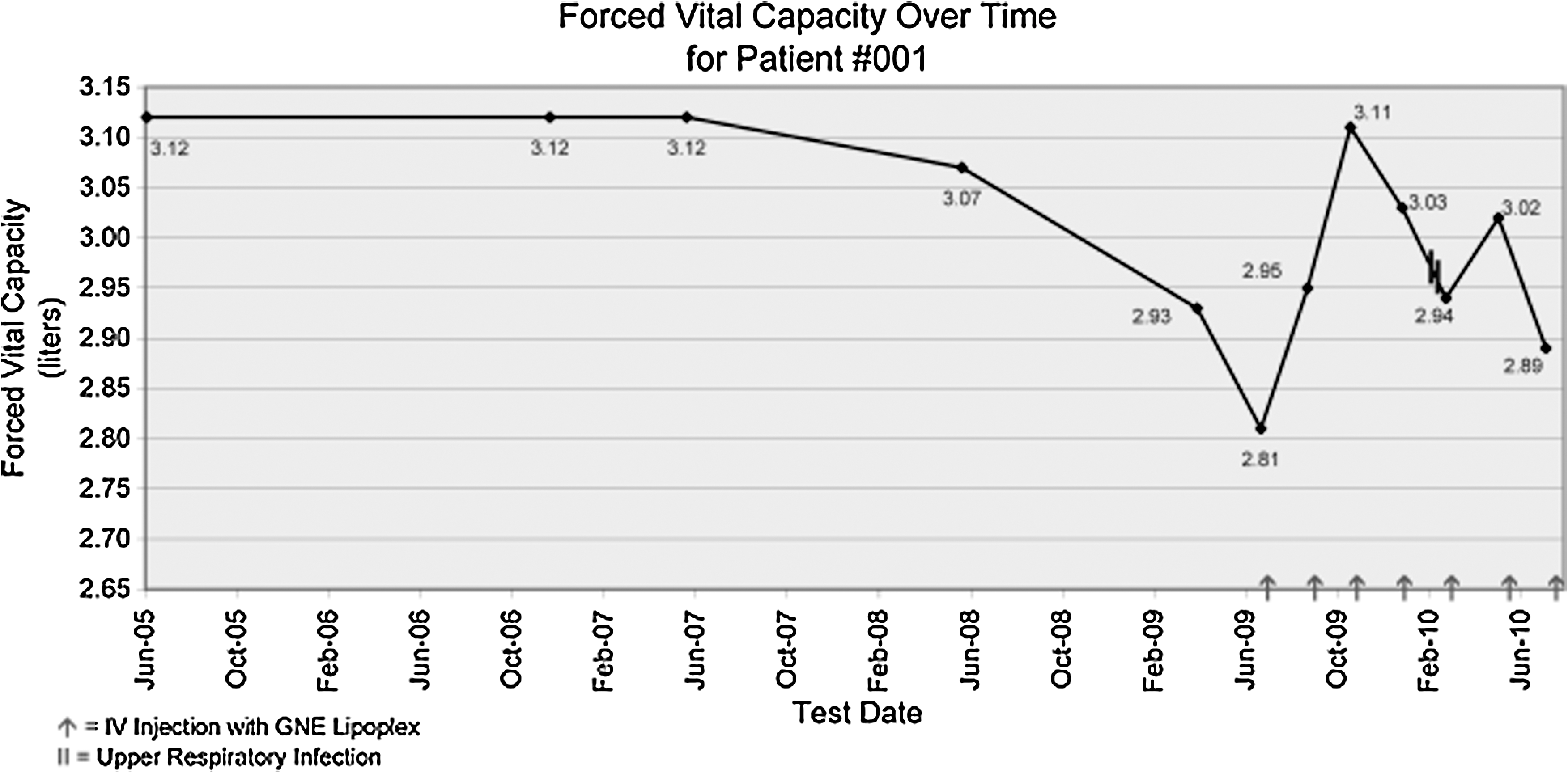
Forced vital capacity (FVC) over time for patient 001.
Results suggest overall stabilization in the loss of muscle strength via manual muscle testing.
Histological analysis
Histological analysis of the quadriceps tissue showed skeletal muscle tissue with a small amount of connective tissue. Ringed inclusion bodies consistent with HIBM were also observed.
Immunohistochemical analysis
Three different lectins (WGA, PNA, and Jacalin) and antibodies to one protein (polysialylated neural cell adhesion molecule, PSA-NCAM) were used for staining (Fig. 6). Results of Jacalin and PSA-NCAM staining are consistent with modest improvement in sialic acid expression 24 hr after infusion of GNE gene lipoplex. However, no change in PNA was observed. WGA binds the terminal sialic acid on all glycans and provides a general overview of all sialylation. Its intensity was expected to remain constant. PNA labels terminal O-linked and N-linked galactose groups and is a marker for hyposialylation. The day 0 quadriceps sample was brightly stained, indicating hyposialylation, but there was no improvement (reduction in staining) at 24 hr. Jacalin predominantly labels terminal galactose groups on O-linked glycans (indicating hyposialylation) and the staining results illustrated a reduction in staining (increased sialylation) intensity at 24 hr. The PSA-NCAM antibody binds to polysialylated NCAM protein and the results demonstrate increased staining, indicating increased sialic acid on NCAM 24 hr after GNE gene lipoplex infusion.
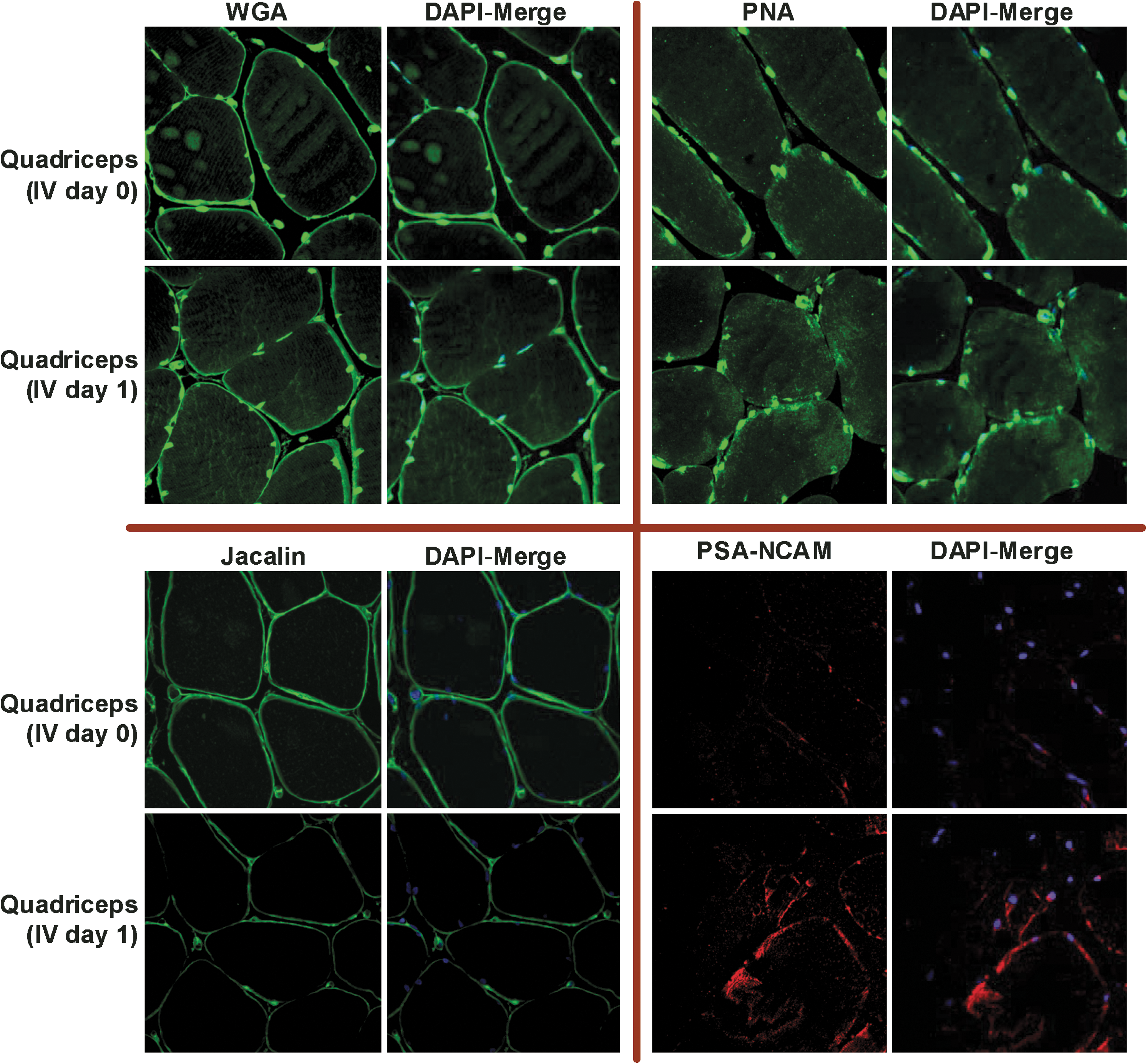
Immunohistochemical staining of quadriceps biopsies from patient 001before and after GNE gene lipoplex infusion. Wheat germ agglutinin (WGA): Predominantly binds terminal sialic acid on all glycans. This stain is a general “overview” of how much sialic acid is present in the tissue; it is nonspecific. For patient 001, there was no difference in WGA stain before and after treatment. This was as expected, and as previously described for human HIBM muscle. Peanut agglutinin (PNA): Predominantly labels terminal galactose groups, and therefore is a marker for hyposialylated glycans. Patient 001 showed bright PNA staining, indicating hyposialylation. There appeared to be no difference in intensity of the PNA stain before and after treatment. Jackfruit agglutinin (jacalin): Predominantly labels terminal galactose groups on O-linked glycans, and therefore is a marker for hyposialylated O-linked glycans. Jacalin staining showed a slight decrease in intensity after treatment, suggestive of improvement in hyposialylation on O-linked glycans. Polysialylated neural cell adhesion molecule (PSA-NCAM) antibody: Binds PSA-NCAM. PSA-NCAM showed a modest increase in intensity after treatment, consistent with improvement in hyposialylation.
qPCR analysis
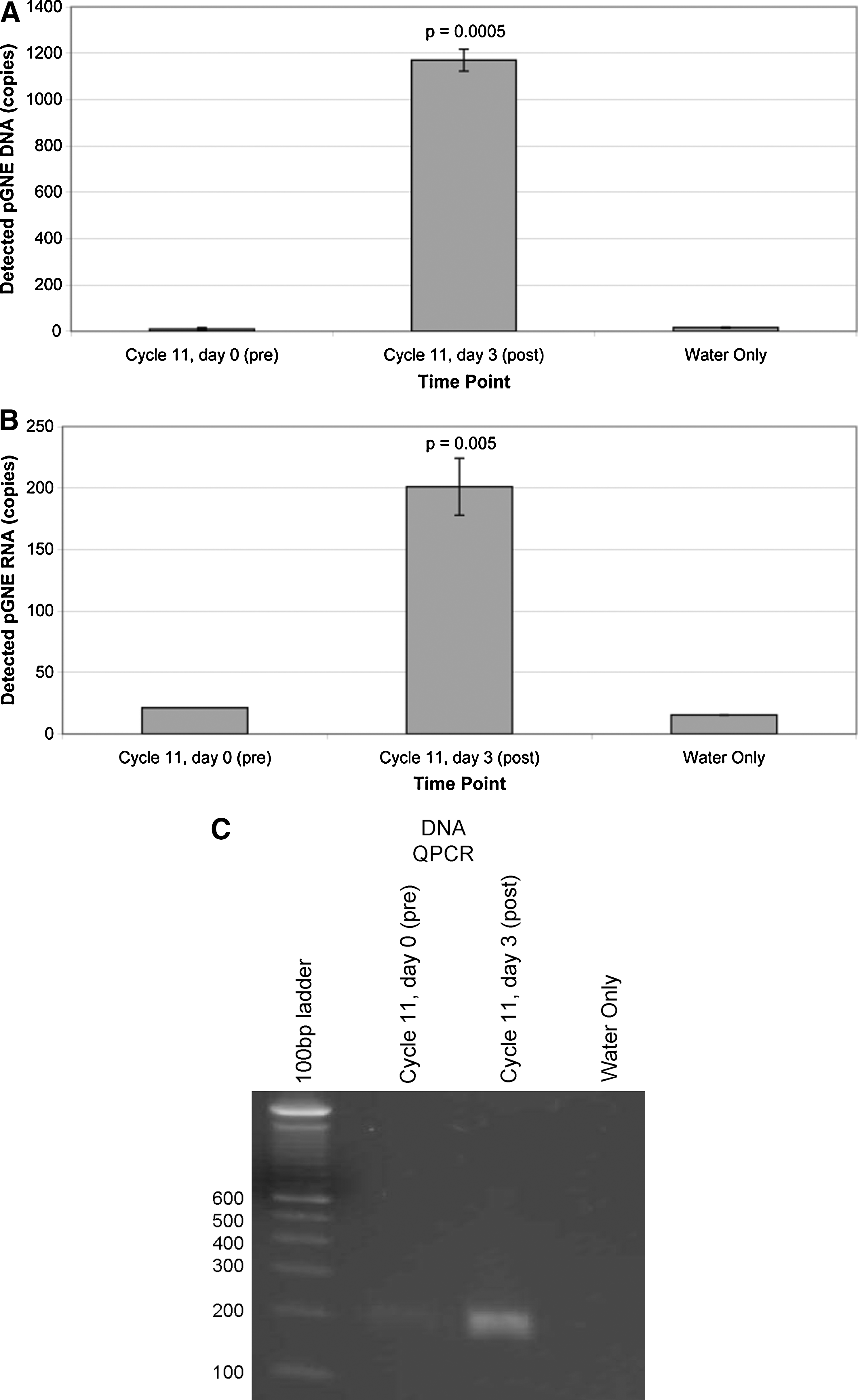
Total DNA and RNA were extracted and qPCR analysis confirmed significant human wild-type GNE plasmid in the quadriceps muscle sample 24 hr after infusion of 5 mg of GNE gene lipoplex (p = 0.00003). In addition, modest expression of GNE RNA was demonstrated by RT-qPCR (p = 0.05) from the same tissue. However, a substantial increase in expression of RNA (p = 0.005) and DNA (p = 0.0005) was detected in a 72-hr posttreatment biopsy from the same quadriceps muscle treated with a 7-mg dose, in comparison with pretreatment baseline (Fig. 7A–C).
(
Discussion
We have demonstrated acceptable safety after a series of seven intravenous infusions of GNE gene lipoplex up to a dose of 7 mg of GNE gene lipoplex over a 13-month span in a single patient with late-stage HIBM. Variable stabilization and limited transient improvement in muscle strength, correlating with significant detection of plasmid, rGNE transgene, and consequent increase of cell surface sialylation (via Jacalin and PSA-NCAM staining), were observed in the biopsied quadriceps muscle 24 hr after intravenous infusion in comparison with preinfusion levels, verifying successful vector delivery to target organ. Moreover, stabilization of pulmonary function associated with quality of life improvement (reclining to supine sleeping position) are encouraging observations; however, additional HIBM patients with extensive functional monitoring will be required for further study before conclusions on GNE gene lipoplex effect are made. Nevertheless, these results are encouraging and justify further phase I trial investigation.
GNE/MNK enzymatic activity in HIBM may impair sialic acid production and interfere with proper sialylation of glycoconjugates (Huizing and Krasnewich, 2009; Jay et al., 2009). Data using the D176V-Tg mouse model demonstrated that muscle atrophy and weakness could be prevented with prophylactic treatment of sialic acid metabolites (Malicdan et al., 2009). Untreated mutant mice showed hyposialylation in multiple organs, including skeletal muscle, whereas oral treatment with NeuAc or ManNAc improved sialylation and reduced the number of rimmed vacuoles and amyloid deposits. Sialic acid is the only sugar component of glycoproteins that bears a net negative charge. This charged sugar provides the terminal carbohydrate on a variety of N-linked and O-linked glycans of proteins, as well as glycolipids that mediate cell–cell and protein–protein interactions (Varki, 1997, 2008).
Hypoglycosylation of α-dystroglycan, a central protein of the skeletal muscle dystrophin–glycoprotein complex, could be one mechanism that may provide an explanation for the muscle weakness of patients with GNE mutations. α-Dystroglycan helps to anchor the extracellular matrix to the cytoskeleton of the sarcolemma. If hypoglycosylated α-dystroglycan is unable to properly bind to the extracellular matrix, the connection between the extracellular matrix and the cytoskeleton provided by dystroglycan is lost and cannot stabilize the sarcolemma during contraction-induced stress. Previous examinations of the glycosylation status of α-dystroglycan in muscle biopsies of four individuals with HIBM (Huizing et al., 2004) showed absent or markedly reduced immunolabeling with two different antibodies (VIA4 and IIH6) to glycosylated epitopes of α-dystroglycan. These findings resemble those found for other congenital muscular dystrophies, suggesting that HIBM may be a “dystroglycanopathy,” and providing an explanation for the muscle weakness of patients with HIBM.
Despite demonstrated proof of principle that intravenous infusion of GNE gene lipoplex can be safely administered, subjective improvement in this single individual with severe HIBM has been limited (improved wheelchair control, bed-to-chair transfer, restful sleeping). Continuation of dose escalation may result in greater muscle functional effect. However, it is possible that the level of muscle deterioration in this patient has advanced beyond reversibility, thereby limiting efficacy to stabilization, as was observed. Previous biopsies in muscles other than the quadriceps (characteristically spared until late in the course of disease progression) revealed sparse muscle fiber residue. It is also encouraging that plasmid and RNA expression was demonstrated and verified with GNE gene lipoplex in the quadriceps muscle, suggesting appropriate dosing and functional capacity of the GNE gene lipoplex. Results support continued dose escalation in the current patient and justify further phase I testing in patients with less advanced disease.
Footnotes
Acknowledgments
The authors thank Susan Mill for competent and knowledgeable assistance in the preparation of this manuscript. Samir Sliheet is also acknowledged for transport support. The authors thank Dr. Gregory Bevels, M.D., of Primary Care Specialists (Alexandria, LA) for assistance with weekly physical assessments during the study period. This work was partially supported by the Intramural Research Program of the National Human Genome Research Institute, National Institutes of Health (Bethesda, MD). The authors are also grateful for the financial support of the Mary Crowley Cancer Research Centers (Dallas, TX) and the Neuromuscular Disease Foundation (Beverly Hills, CA).
Author Disclosure Statement
John Nemunaitis, Neil Senzer, Phillip Maples, and Nancy Templeton have direct affiliation with Gradalis, Inc., in which they own stock. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in this paper.