
Abstract
Degeneration of nigrostriatal neurons in Parkinson's disease (PD) causes progressive loss of aromatic
Introduction
Materials and Methods
Animals
Ten adult female rhesus monkeys (Macaca mulatta, 5.2–12.8 kg) were lesioned with 1-methyl-4-phenyl-1,2,3,6-tetrahydropyridine (MPTP) as previously described (Bankiewicz et al., 1986, 2000; Eberling et al., 1998). Briefly, MPTP lesioning consisted of one right intracarotid artery infusion of 2.0–4.0 mg of MPTP-HCl. Behavioral assessment was performed that indicated mild to moderate parkinsonism. This model is characterized by almost complete nigrostriatal lesioning of the ipsilateral hemisphere with little or no effect on the contralateral hemisphere (Eberling et al., 1998). Experiments were performed according to National Institutes of Health (Bethesda, MD) guidelines and to protocols approved by the Institutional Animal Care and Use Committee at the University of California San Francisco (San Francisco, CA).
Behavioral assessment
The modified Parkinson Clinical Rating Scale (CRS) employed here was developed in our laboratory and closely approximates those reported in the literature (Imbert et al., 2000). The scale evaluates 14 parkinsonian features, each of which receives a score from 0 to 3 in order of increasing severity. Individual scores are summed to arrive at a final score. Features evaluated include tremor (right and left sides), locomotion, “freezing,” fine motor skills (right and left sides), bradykinesia (right and left sides), hypokinesia, balance, posture, startle response, and gross motor skills (right and left sides). Normal animals score in the range 0–4 and severely parkinsonian monkeys score above 21. An experienced rater, blinded to treatment group, performed all measurements.
Vector production
The human AADC cDNA was cloned into an AAV2 shuttle plasmid, and a recombinant AAV2 carrying hAADC under the control of the cytomegalovirus promoter was manufactured by the AAV Clinical Vector Core at Children's Hospital of Philadelphia (Philadelphia, PA) as previously described (Matsushita et al., 1998; Wright et al., 2003). AAV2-hAADC was purified from cell extracts by CsCl centrifugation and was concentrated to approximately 7.2×1012 vector genomes (VG)/ml.
Surgical procedure
Two weeks before infusion, NHP underwent stereotactic placement of a skull-mounted, MRI-compatible, threaded plastic adaptor plug (diameter, 12 mm; height, 14 mm) for later attachment of frame. After craniectomy, the plug was secured to the skull over the right hemisphere with dental acrylic. After placement of the adaptor plug, animals recovered for at least 2 weeks before initiation of iMRI infusion procedures. Only animals receiving AAV2-hAADC underwent MRI-guided CED; control animals were infused with phosphate-buffered saline (PBS) via SmartFlow catheter in a stereotactic frame but without image guidance.
ClearPoint system, target selection, trajectory planning, and cannula insertion
Both the delivery system and the procedure have been described previously in detail (Richardson et al., 2011a,b). Briefly, the ClearPoint system (MRI Interventions [formerly SurgiVision], Memphis, TN) consists of the SmartFrame, an infusion cannula (SmartFlow), and a software system that communicates with both the MRI console and the operating neurosurgeon in the MRI suite. The SmartFrame houses an MRI-visible (gadolinium-impregnated) fluid stem and integrated fiducials that are detected by the software. On the day of infusion, NHP were sedated with intramuscular ketamine–xylazine (7 and 3 mg/kg, respectively), intubated, and placed on inhaled isoflurane (1–3%). The plug adaptor was prepared under sterile conditions and the NHP was placed supine in an MRI-compatible stereotactic frame. The SmartFrame was attached by screwing the base onto the adaptor plug over the right hemisphere. The NHP was moved into the bore and a controller was attached to the SmartFrame, which allows the surgeon to manually “dial in” distance changes to align the cannula to the desired trajectory in four directions (pitch, roll, anterior–posterior, medial–lateral) as instructed by the ClearPoint software.
First, a high-resolution anatomical MR scan was acquired for target identification and surgical planning. Images were then transferred to the ClearPoint system, where the target for cannula tip placement was selected. In all animals, two precommissural locations in the right hemisphere: one in the caudate nucleus and one in the putamen were selected.
Next, rapid scans were obtained that allowed the ClearPoint software to detect the position and orientation of the SmartFrame fluid stem. The software used this image to compare the current SmartFrame trajectory with the target trajectory and generate instructions to adjust SmartFrame alignment via the pitch and roll controls. After these adjustments were made, the image was reacquired to measure the new expected error and this process was repeated as necessary. When the expected error was within 1.0 mm, the pitch and roll axes were locked and more scans were acquired along the sagittal and coronal planes of the guide stem for fine adjustment of the SmartFrame x–y stage. This process was repeated until the software reported an expected error of <0.5 mm, typically requiring no more than two iterations.
The infusion system included FDA-approved SmartFlow catheter, a custom-designed, ceramic, fused silica reflux-resistant cannula with a 3-mm stepped tip (Krauze et al., 2005; Fiandaca et al., 2008). The cannula was attached to a 1-ml syringe mounted onto an MRI-compatible infusion pump (Harvard Bioscience, Holliston, MA). Infusion was initiated at 1 μl/min and, after visualizing fluid flow from the cannula tip when held at the height of the head of the NHP, the cannula was inserted through the SmartFrame guide stem and into the brain. When the depth stop encountered the top of the guide stem, it was secured with a locking screw.
Infusion and imaging data analysis
Infusions were performed as previously described in more detail (Richardson et al., 2011a,b). After cannula insertion, repeated multiplanar FLASH (fast low angle shot) images were obtained every 5 min for the duration of the infusion. After visualization of Gd infusion at the cannula tip, the infusion rate was ramped up from an initial 1 μl/min to a maximum of 3 μl/min by 0.5-μl/min increments every 5 min. Each NHP first received an infusion in the right putamen (50 μl) and then in the right caudate nucleus (50 μl). Distribution volumes of Gd were measured with OsiriX, an open source DICOM (Digital Imaging and Communications in Medicine) reader and imaging workstation. Software was written and applied as an OsiriX plug-in to auto-segment each infusion on individual MRI slices from which a total infusion volume was calculated.
Tissue processing
Each NHP was perfused transcardially with PBS and PBS–4% paraformaldehyde–0.1% glutaraldehyde ∼8 months after the infusion session and 3–8 weeks after
Results
Performance of delivery platform and cannula
The SmartFlow cannula and ClearPoint targeting system (with SmartFrame skull attachment modified for NHP use; Richardson et al., 2011a) were used (Fig. 1) to infuse either AAV2-hAADC (n=6) or PBS (n=4) to the right caudate nucleus and putamen (total of 20 cannula insertions). The two infusions per NHP were performed sequentially during the same procedure with no technical limitations encountered in redirecting the cannula for infusion of the second site. The ratio of volume of distribution (V d) to volume of infusion (V i) relationship (V d/V i) is important in real-time CED for planning drug doses and was calculated for each infusion. The mean V d/V i ratio was 1.6 (95% confidence interval [CI], 0.3) and 3.1 (95% CI, 0.6) for caudate nucleus and putamen, respectively; the latter similar to that previously reported for NHP putamen (Richardson et al., 2011b). No MRI-visible hemorrhages occurred during cannula placement, and no adverse effects occurred during RCD or subsequently. However, some leakage of infusate was observed dorsally into the internal capsule in one of the animals during the putaminal infusion (Fig. 2), although no pathological signs were observed in this animal immediately after surgery or subsequently.
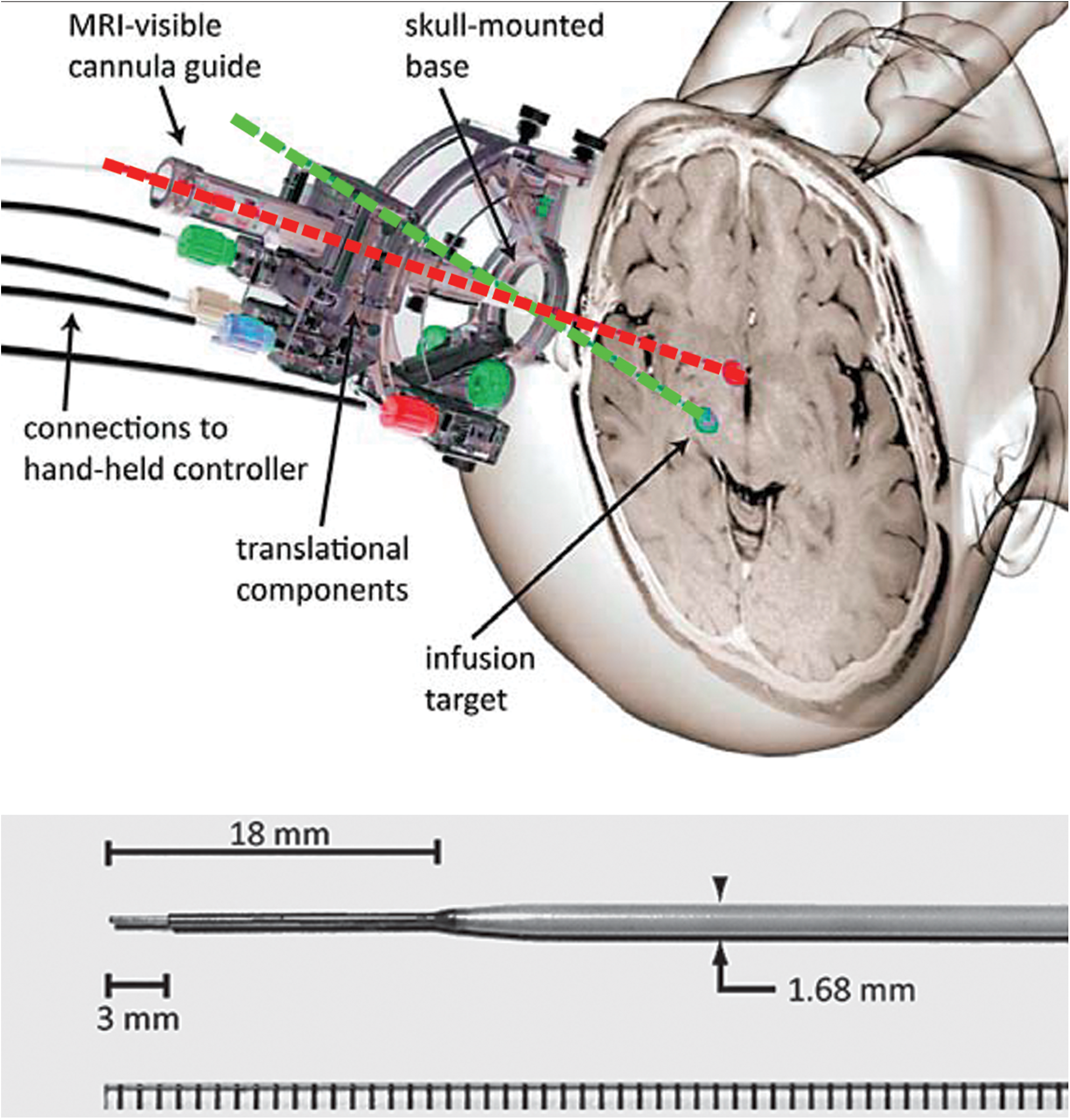
Top: MRI-compatible stereotactic aiming device and cannula. SmartFrame stereotactic aiming device includes a skull-mounted holder for the infusion cannula and controls that permit adjustment of the trajectory while the patient is in the MR bore. Planning and intraoperative adjustment are accomplished with the aim of ClearPoint software as described in more detail by Richardson and colleagues (2011a). Bottom: The SmartFlow MRI-compatible cannula. The step in the outer dimensions prevents infusate reflux. Color images available online at
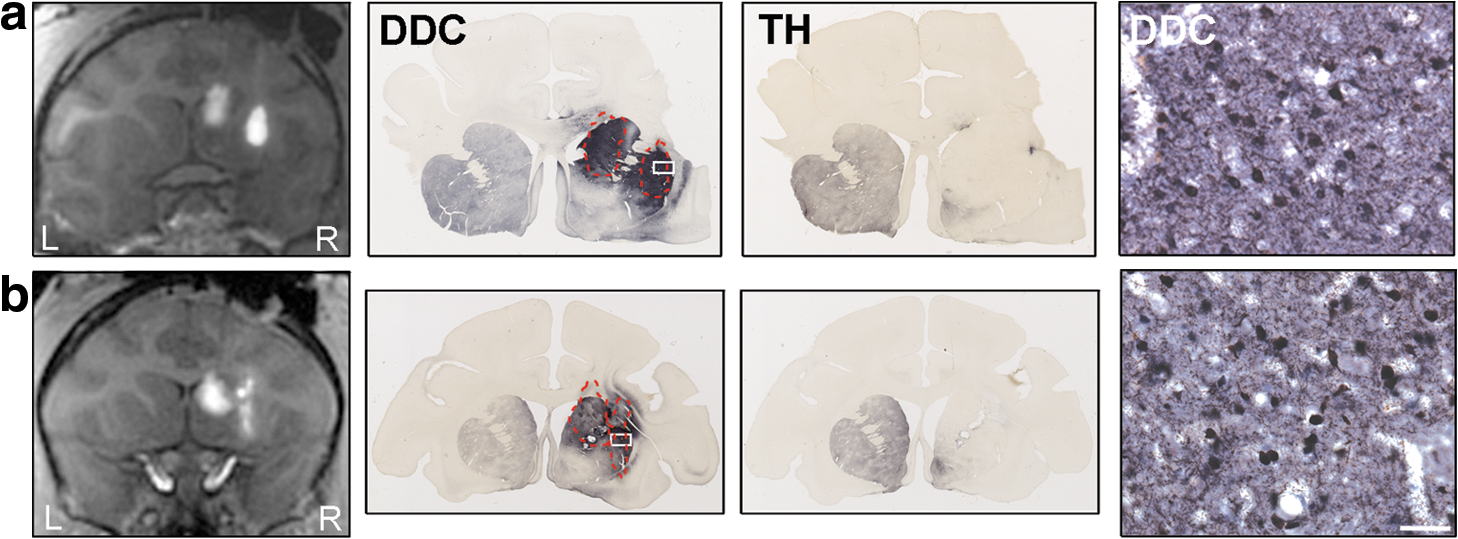
Correlation between gadoteridol and AADC expression. MRI images (first column) show gadoteridol distribution at the end of both caudate nucleus and putamen CED after
Intervention-related pathology
H&E staining and GFAP or Iba1 immunohistochemistry were performed to assess any tissue damage related to the surgery. H&E staining showed no evidence of overt pathology, such as cerebritis, infarcts or cellular infiltrates around the delivery sites in any of the animals, control or AAV2-hAADC (Fig. 3, left and middle columns). Only a moderate inflammatory reaction to the cannula insertion could be seen. This reaction was confined to the area surrounding the cannula tract, where the presence of standard lymphocytes and macrophages containing some hemosiderin was noticed. The rest of the target region appeared normal. Also, the white matter around the target nuclei (caudate nucleus and putamen) was spared and looked the same in both the ipsilateral and contralateral hemispheres. One animal that received AAV2-hAADC, however, presented with some cellular infiltration that correlated with the spread of infusate in the striatum and internal capsule (Fig. 3, right-hand column). Analysis of H&E-stained sections at high magnification from this animal evinced some reactive astrocytes (gliosis) and many lymphocytes in the corona radiata leakage area, indicative of chronic inflammation. Curiously, some eosinophils were also detected in this region. The presence of this type of blood cell is unusual in the brain parenchyma and suggestive of an infection as the cause of the inflammatory process detected. However, this animal presented no subsequent behavioral signs or other pathology related to the leakage. One of the animals in the control group exhibited pathological signs of hemorrhage close to the infusion area in the putamen that was revealed during gross anatomical inspection of the postmortem brain. However, the animal did not show any pathological behavior or signs.
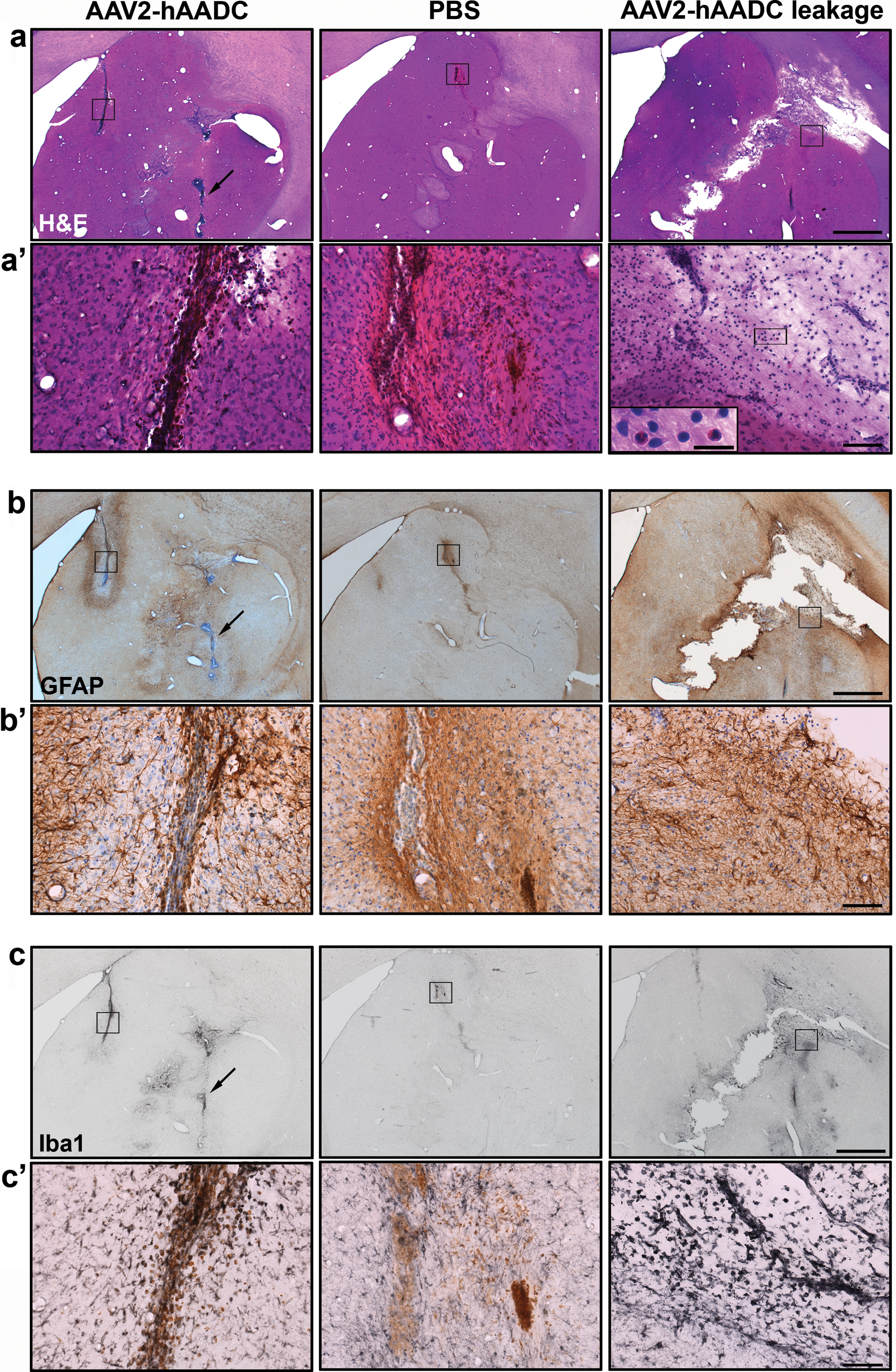
Lack of tissue damage in target structures. Representative images show cannula tracts with H&E
In each animal, regardless of control or active group assignment, moderate Iba1 and GFAP expression was noted along the cannula tracts and at the depth of the proximal, fused silica tip (Fig. 3b and c), consistent with previous reports demonstrating slight inflammation after CED from a stepped cannula (Su et al., 2009). In all animals, areas of both caudate nucleus and putamen 0.75 mm away from the infusion site were not considered positive by H&E staining, or by GFAP and Iba1 staining, because they exhibited basal expression of these markers.
High-dose AAV2-hAADC vector distribution
The open label phase I clinical trial investigated two dose levels (9.0×1010 and 3.0×1011 VG) with a higher planned dose (9.0×1011 VG) not conducted because of manufacturing constraints. Some patients in this trial displayed a modest improvement in UPDRS score in both off- and on-medication states (Christine et al., 2009). However, retrospective comparison with an earlier dose-ranging study in NHP (1.2×1010 to 1.0×1012 VG) suggests that the doses in the phase I trial were at the threshold for expected therapeutic effect when adjusted for the 5-fold difference in striatum volume between humans and NHP. Thus, a higher dose and greater infusion volumes should be investigated in future studies.
The vector dose for the animals in the present study was 7.0×1011 VG (infused unilaterally), a 2-fold higher total vector dose than that received by high-dose phase I trial patients (Table 1). No animals infused with AAV2-hAADC in the present study developed any adverse effects or signs of toxicity related to the vector. All the animals remained healthy (i.e., no weight loss) throughout the study and exhibited only the behavioral signs expected in mildly hemi-MPTP-lesioned parkinsonian animals. In fact, if anything, their parkinsonism tended to ameliorate after AAV2-hAADC infusion (mean CRS before surgery, 10±3; mean CRS ∼8 months after surgery, 8±4). All the animals were responsive to
BL, bilateral; c., commissural; Cd, caudate nucleus; hemis., hemisphere; NHP, nonhuman primate; pr.c., precommissural; pt.c., postcommissural; Put, putamen; UL, unilateral; VG, vector genomes; V i, infusion volume.
The postmortem analysis of the tissue revealed a broad distribution of AADC expression in the putamen and caudate nucleus that closely overlapped areas of Gd signal observed during infusion, with a large number of AADC-positive striatal neurons and fibers evident (Fig. 2a). Infusate was well contained within both target structures in all animals, even though the relative infusion volume was larger for the caudate nucleus, a small structure compared with the putamen. As mentioned previously, one of the animals that received AAV2-hAADC exhibited significant leakage into the internal capsule and histological signs of infection in the same area. Nevertheless, a large number of medium spiny neurons and fibers were found in both caudate nucleus and putamen (Fig. 2b). We noted some AADC expression in neuronal cell bodies and fibers in structures within the infused hemisphere, such as in the internal and external globus pallidus, subthalamic nucleus, and substantia nigra pars reticulata (data not shown), indicating anterograde transport of the vector (Ciesielska et al., 2011).
Discussion
The purpose of this study was to determine the long-term safety of a new, image-guided parenchymal acute delivery system for AAV vectors. Previous clinical experience has indicated that inadequate distribution of transgene expression in the putamen may be responsible for discrepancies in efficacy between NHP and human subjects (Christine et al., 2009; Bartus et al., 2011). Accordingly, we have sought to improve vector distribution by means of visual surrogate markers that permit intraoperative monitoring of infusions (Richardson et al., 2009). This innovation enabled quantitative analyses of dynamic parameters that influence parenchymal vector distribution, such as ventricular leakage and cannula reflux (Varenika et al., 2009), as well as optimal cannula placement (Yin et al., 2010, 2011) and rate of infusion (Varenika et al., 2009). These investigations led to the development of a clinical platform for MRI-monitored CED in the brain. This system integrates three component technologies: the SmartFlow catheter, a custom-designed, ceramic, fused silica cannula with a 3-mm stepped tip that makes it reflux-resistant; the SmartFrame, which is an MRI-guided adjustable trajectory frame; and ClearPoint software, a software system that detects gadolinium fiducials housed in the SmartFrame and communicates the frame position to the MRI console, thereby allowing the operator to align the frame to the target trajectory (see Richardson et al., 2011a, for details). The combination of these three components results in improved control of infusate delivery and visualization of therapeutic distribution.
The purpose of the present study was to test the safety of the entire system in the context of delivering AAV2-hAADC into the parkinsonian monkey putamen. It was unnecessary to conduct an efficacy study of AAV2-hAADC in NHP because that has been abundantly established (Bankiewicz et al., 2006; Forsayeth et al., 2006; Hadaczek et al., 2010). These data form the basis of a proposed clinical trial of AAV2-hAADC in PD with the recognition that the delivery technique in previous phase I studies (Eberling et al., 2008; Christine et al., 2009; Muramatsu et al., 2010) was unable to ensure sufficient distribution and transgene expression to be able to achieve optimal non-rate-limiting AADC activity in transduced tissue (Forsayeth et al., 2006). The experiments in this paper show the safety and tolerability of administering a higher dose of AAV2-hAADC under real-time MR imaging guidance CED in the precommissural striatum of parkinsonian NHP with an optimized clinical cannula. There were no behavioral or histological indications of parenchymal injury due to cannula insertion, despite two cannula insertions occurring close to each other in the same hemisphere of every animal. Only in one case, out of 10, did we detect significant leakage of the infusate into the internal capsule, where some cellular infiltration was revealed by H&E staining, suggesting an infection, although it was asymptomatic. In our experience, the NHP putamen and other smaller nuclei are inappropriate targets for testing the larger infusion volumes proposed for clinical study (>200 μl per site), due to leakage beyond the anatomic boundaries of these small targets. Of the two infusion sites in this study, the caudate nucleus was the smaller, receiving 50 μl of infusate, and this was well tolerated. Even though the caudate nucleus will not be targeted in clinical trials, the fact that the infusion in this small structure was uneventful and well tolerated further demonstrates the safety of the delivery system tested in the present work. However, the V d/V i ratio obtained from MRI images for this region was lower than expected (V d/V i caudate nucleus, 1.6). Leakage into the lateral ventricle during the caudate infusion seemed to be absent because we could see a well-contained Gd signal in the MR images. However, as previously described by Song and Lonser (2008), infusate leakage into the ventricle is not detected on T1-weighted MRI but only on fluid-attenuated inversion MRI. Because we did not acquire this kind of sequence, we cannot rule out the possibility that some undetected infusate extravasation into the lateral ventricle occurred, and this may explain the low V d/V i determined for the caudate nucleus. Even so, we observed robust AADC expression in all test animals. Our data support the value of real-time image-guided drug delivery to ensure the most accurate and predictable delivery of therapeutic drugs directly into the brain parenchyma. To optimize distribution of AAV2 vectors via CED within the human putamen, we propose delivery of 900 μl across four infusion sites (two sites per hemisphere). This increase in vector volume is consistent with the difference in the volume of the putamen between humans and NHP. Overall, these data provide additional support for a clinical study with the highest vector dose previously approved for clinical study. A clinical dose of 9.0×1011 VG has an extrapolated safety margin of more than 5-fold relative to the current study.
Intracranial hemorrhage is a common risk of stereotactic craniotomy (Binder et al., 2005) and was also seen in the AAV2-hAADC phase I clinical trial patients with PD (Christine et al., 2009; Muramatsu et al., 2010). Similarly, one of our PBS control animals presented with a possible hemorrhage in the putamen detected only postmortem. The fact that the putamen is profusely irrigated by lenticulostriate arteries, which branch from the middle cerebral artery, makes the putaminal region prone to hemorrhagic strokes (Feekes and Cassell, 2006). Because the iMRI ClearPoint system also allows the clinical team to identify large blood vessels and make any necessary adjustments to the cannula trajectories, the potential for hemorrhages should be reduced. The present technique also provides rapid feedback on the physical and anatomic diffusion parameters important for optimizing gene transfer (Richardson et al., 2011b).
All animals receiving AAV2-hAADC infusion showed good coverage of the target structures, both caudate nucleus and putamen, whereas the striatum of control animals was devoid of AADC signal on the lesioned side after the PBS infusion. In contrast to previous studies in our laboratory (Richardson et al., 2011a,b), striatal AADC expression did not perfectly match gadolinium signal on MRI. The region of AADC immunostaining in the striatum was somewhat greater than indicated by MR images. This phenomenon could be due to a discrepancy between the postsurgical interval in previous and present studies; that is, 1–5 weeks previously and ∼8 months in the present study. We have previously reported that the AAV2-hAADC distribution appears to broaden slowly over time in NHP, resulting in a larger coverage of target regions (Daadi et al., 2006). In addition, because AAV2 vector is transported anterogradely through the axons (Ciesielska et al., 2011), we also found AADC expression in structures outside the striatum such as the globus pallidus, subthalamic nucleus, substantia nigra pars reticulata, and thalamus.
We also tested a relative vector dose higher than the highest dose administered to patients in the phase I trial (Christine et al., 2009). Animals slightly improved their parkinsonism after receiving AAV2-hAADC, because study animals were only mildly lesioned with MPTP in contrast to preclinical efficacy studies in which animals were severely overlesioned (Bankiewicz et al., 2006; Forsayeth et al., 2006). This high vector dose (7.0×1011 VG) resulted in strong AADC expression in the striatum. The possible toxic effect of such a high AAV vector dose was ruled out because we did not find any signs of tissue damage related to the high vector dose in any of the treated animals. Also, all animals remained free of
Footnotes
Acknowledgments
The authors thank Peter Piferi and Geoffrey Bates of MRI Interventions (formerly Surgivision) for providing the ClearPoint equipment and for assistance in this study. This work was supported by NIH grant R01NS050156 to K.S.B.
Author Disclosure Statement
Authors have no conflicts of interest.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.