
Abstract
We report the results of a long-term follow-up of subjects in a phase 1 study of AAV2-hAADC (adeno-associated virus type 2–human aromatic
Introduction
PET imaging during the first 6 months of a phase 1 study of AAV2-hAADC gene therapy demonstrated a significant elevation in AADC expression, a good safety profile, and preliminary indications of clinical benefit (Christine et al., 2009). It has not yet been established whether AADC gene therapy has an effect on patients in the OFF state, the clinical state when the benefits of dopaminergic medications are minimal in patients with fluctuating motor symptoms. The OFF state typically occurs a number of hours after the last of
Materials and Methods
Subjects
A detailed description of the human study methods has been published (Eberling et al., 2008; Christine et al., 2009) and is summarized here only briefly. Ten patients (five men and five women) with a mean age of 64 years (range 57–71) were entered into the study. Two dose cohorts (five patients each) were evaluated. The low-dose cohort received a total dose of 9×1010 vector genomes, and the high-dose cohort received 3×1011 vector genomes. The entry criteria included the following: PD with intractable motor fluctuations despite optimized medical treatment; Hoehn and Yahr Stage III to IV off medication; a history and screening examinations showing improvement with dopaminergic therapy; and optimized and stable anti-PD medication for at least 2 months prior to screening.
Putaminal AAV2-hAADC infusion
On the morning of the operation, subjects were admitted to the neurosurgical service and antiparkinsonian medications were withheld. The subjects were fitted with a Leksell stereotactic head frame (Elekta, Norcross, GA) with local anesthesia at the pin sites and intravenous sedation with midazolam. The target in the postcommissural putamen was localized with gadolinium-enhanced volumetric T1 and either T2 or inversion recovery slab magnetic resonance (MR) acquisitions of the brain. Two parallel cannulae were placed 6 mm apart in the center of the postcommissural putamen, one anterior and one posterior. Trajectories to these targets were planned so as to avoid traversing the lateral ventricle, sulci, and cortical veins. Subjects were infused bilaterally with a total volume of 200 μl over the four injection sites (50 μl/site) with CED at a flow rate of 1 μl/min (van Hilten et al., 1994; Bankiewicz et al., 2000). Customized infusion cannulae were designed to minimize potential reflux up the injection tract, and a “waiting period” of 10 min after cessation of active infusion was observed before the cannulae were removed.
PET scanning
Subjects underwent positron emission tomography (PET) scans with the AADC-specific tracer [18F]fluoro-
UPDRS evaluation
Subjects were evaluated clinically at baseline and then monthly for 6 months postoperatively. Standardized evaluations with the UPDRS (van Hilten et al., 1994) and the stand–walk–sit test (O'Sullivan et al., 1998) were performed at baseline and 6 months and then annually in the off- and on-medication states. The UPDRS is a widely used rating scale that evaluates cognitive, functional, motor deficits (UPDRS, part III) and medication-related complications. UPDRS scores indicate worse disease as the score increases. It was administered in the morning in the OFF state, 12 hr after the last dose of dopaminergic medication, and in the fully ON state, as judged by the patient and clinician. In most cases, this occurred 1 hr after the usual morning medications were taken. However, if the subject was not fully “on,” an additional 12.5/50 or 25/100 of carbidopa/
Statistics
Comparisons between groups were made with Student's t test, with a threshold of p<0.05 considered significant.
Results
FMT uptake
The Ki C values showed a significant increase in the first 6 months that was maintained throughout the 4-year duration of the study (Fig. 1). After an initial increase of 25% and 65% in the low- and high-dose groups, respectively, there was no significant change in Ki C in either group.
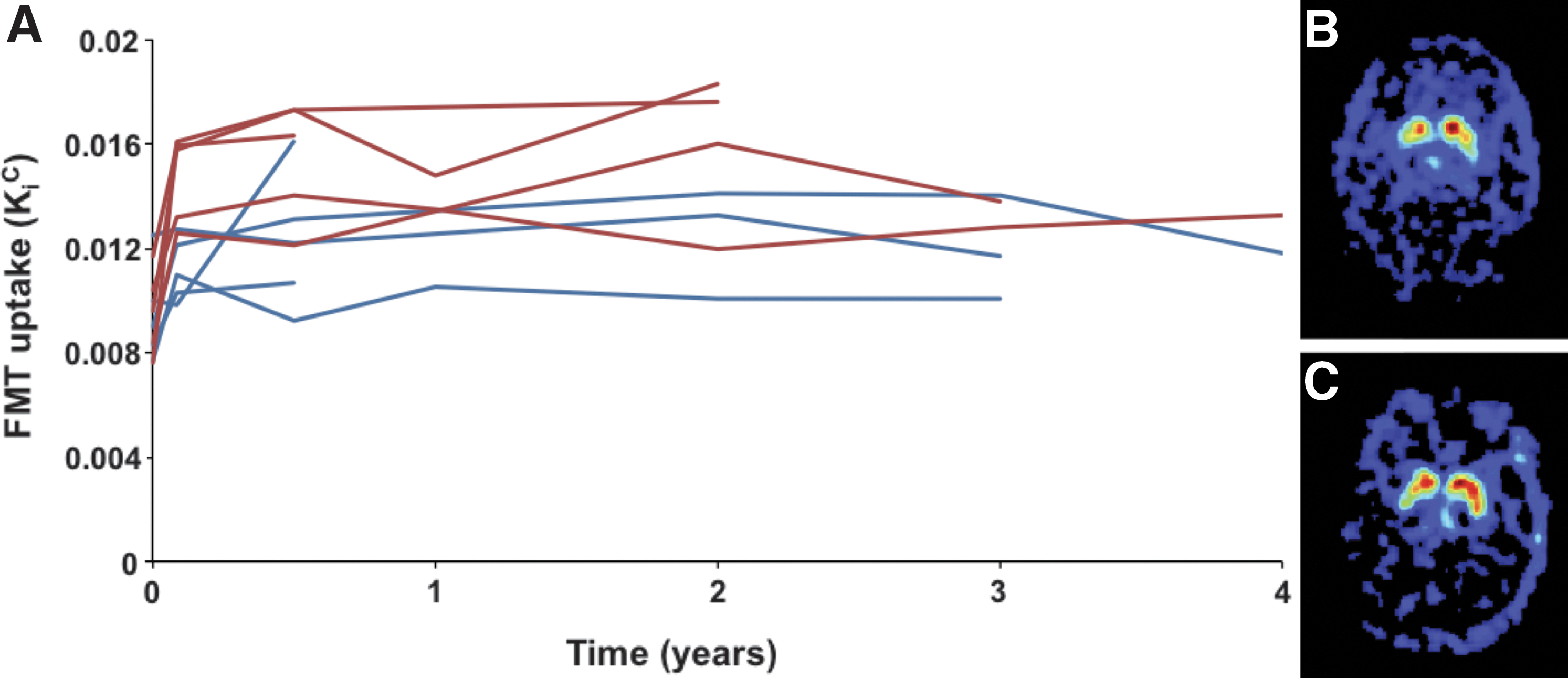
Time course of FMT-PET.
Clinical safety and efficacy
Six and one half years after infusion of the first subject, all subjects are alive and ambulatory. One patient did not return for follow-up UPDRS and PET evaluations after the first year follow-up. Four subjects underwent treatment with deep brain stimulation (DBS) after gene therapy (at 10, 18, 30, and 50 months), and data obtained after DBS surgery were removed from the UPDRS analysis. Table 1 lists adverse events that have occurred so far. Mild worsening of dyskinesias occurred in four subjects; this was transient and responded to adjustments of
Designation includes adverse events that were possibly, probably, or definitely related to the intervention.
Subject 9 suffered a hemorrhagic infarct (attributed to an arterial rupture). The other two events were asymptomatic and discovered incidentally on postoperative MRI. One subject had a small subdural and subarachnoid hemorrhage, and the other an intra-cerebral hemorrhage thought to be secondary to venous infarction. All hemorrhages were dorsal to the infusion site and were attributed to the surgical procedure.
Partial seizure disorder developed 4 months after surgery in the subject with an intra-cerebral arterial hemorrhage and resolved on treatment with phenytoin.
Temporal analyses of the UPDRS scores in the ON and OFF states for all subjects are summarized in Fig. 2. Both ON and OFF scores showed a significant improvement in the first 12 months in all patients, followed by a slow deterioration over the following years. There were no significant differences between the high- and low-dose patients in either the ON or OFF score.

Time course of UPDRS ON and OFF scores.
Discussion
This study showed that AAV2-hAADC treatment was safe and that AADC gene expression was maintained at least 4 years after administration of therapy. The PET analysis showed that FMT uptake increased initially and remained elevated throughout the study duration, indicating an improvement in comparison with other studies that have documented a decrease in FMT uptake over time in PD patients (Asari et al., 2011). The persistent elevation of FMT suggested that a similar number of neurons continued expressing the transgene throughout the study, consistent with our previous observations in 1-methyl-4-phenyl-1,2,3,6-tetrahydropyridine (MPTP)–lesioned rhesus macaques (NHPs) (Hadaczek et al., 2010).
These results demonstrate the dose dependence of the treatment and support nonclinical data indicating that vector dose determines the number of neurons expressing the transgene (Cunningham et al., 2008). However, a pivotal dose-ranging study in NHPs (Forsayeth et al., 2006) showed that, as vector dose is increased, there is a modest positive linear correlation between vector dose and FMT-PET that is followed by a sharp transition to a much higher PET signal. We found that the low signal was bound by the ranges of PET values found in MPTP-lesioned animals, and the high signal by the range of values found in unlesioned animals. This striking transition suggests that expression of AADC activity in putamen is either rate-limiting or not. The fact that the two doses of vector in the phase 1 study display a modest positive correlation, but a low overall intensity, suggests that a higher vector dose will be required to maximize the efficacy of
Aside from the three intracranial hemorrhages (two were asymptomatic and were detected by postoperative scans), adverse effects during the course of the study were no more than would be expected in any long-term study of PD subjects, namely, fractures due to falls and infections of lung and bladder. The increased anxiety and depression that occurred in one patient are also common in PD.
The UPDRS showed a dramatic improvement within the first 12 months. This is most likely due, at least partly, to a placebo effect, which has been well documented for PD (de la Fuente-Fernández and Stoessl, 2002). As this was an open-label study, both patients and physicians were susceptible to a placebo effect, as we acknowledged in our original publication.
In comparable sham-controlled studies in which striatal implantation of DA-secreting cells (Gross et al., 2011) or AAV2 containing neurturin cDNA (Marks et al., 2010), improvements of 7–10 points on the UPDRS motor score (on or off medication) were seen in both sham and active arms of the two studies (for review, see Forsayeth et al., 2010). This is very similar to the degree of improvement seen in the present study in the first 12 months. The fact that the two cited studies showed no clinical benefit shows the importance of a sham surgery control group and limitation in using the UPDRS as a primary outcome measure in the first 12 months.
After the first 12 months, there was a long period during which patients' responsiveness to
There are several important implications of these clinical data. AAV2-mediated gene transfer appears to be permanent, and it is altered little by the ongoing neurodegenerative process. Because AAV2 targets striatal interneurons that do not degenerate in idiopathic PD, we conclude that gene transfer in PD patients is permanent. The results of this trial do not exclude a likely placebo effect most dramatically in evidence in the first 12 months, and this should be borne in mind in the design of any phase 2 trials. Furthermore, measuring treatment effects by the difference between ON and OFF scores may be a reasonable approach to evaluating the efficacy of
Footnotes
Acknowledgments
This study was supported by Genzyme Corporation, which was also the study sponsor.
Author Disclosure Statement
Dr. Kaplan is an employee of Genzyme Corporation, the study sponsor. No other authors have any financial disclosure to make.