
Abstract
Duchenne muscular dystrophy (DMD) is a severe muscle wasting disorder caused by mutations in the DMD gene, affecting 1 in 3500 newborn males. Complete loss of muscle dystrophin protein causes progressive muscle weakness and heart and respiratory failure, leading to premature death. Antisense oligonucleotides (AONs) that bind to complementary sequences of the dystrophin pre-mRNA to induce skipping of the targeted exon by modulating pre-mRNA splicing are promising therapeutic agents for DMD. Such AONs can restore the open reading frame of the DMD gene and produce internally deleted, yet partially functional dystrophin protein isoforms in skeletal muscle. Within the last few years, clinical trials using AONs have made considerable progress demonstrating the restoration of functional dystrophin protein and acceptable safety profiles following both local and systemic delivery in DMD patients. However, improvement of AON delivery and efficacy, along with the development of multiple AONs to treat as many DMD patients as possible needs to be addressed for this approach to fulfill its potential. Here, we review the recent progress made in clinical trials using AONs to treat DMD and discuss the current challenges to the development of AON-based therapy for DMD.
Introduction
About 70% of DMD cases are caused by dystrophin gene deletions, leading to the loss of one or more exons (Aartsma-Rus et al., 2006). Frame-shift mutations caused by out-of-frame deletions in the DMD gene, result in complete loss of expression of dystrophin and a severe DMD phenotype (Fig. 1). The deletion of specific in-frame exons leads to the expression of an internally deleted, yet partially functional dystrophin protein and the typically much milder Becker muscular dystrophy (BMD) phenotype. There are various preclinical and clinical trials in progress for the genetic treatment of DMD. In particular, the antisense oligonucleotide (AON)-mediated exon skipping approach has demonstrated the restoration of functional dystrophin expression in DMD patients in current clinical trials. Modulating the splicing of specific DMD exons by exon skipping using AONs can induce the exclusion of targeted exons, leading to the restoration of the reading frame and the expression of an internally deleted, yet partially functional BMD-type dystrophin molecule (Fig. 1). The in-frame transcript typically contains both the N- and C-terminal domains of dystrophin and hence is functional since these domains provide stability to muscles by linking the cytoskeleton to the sarcolemmal membrane. It ameliorates the severe muscle damage with improvement of muscle function seen in mdx mice and canine X-linked muscular dystrophy (CXMD) dogs (Lu et al., 2005; Alter et al., 2006; Heemskerk et al., 2009; Yokota et al., 2011).
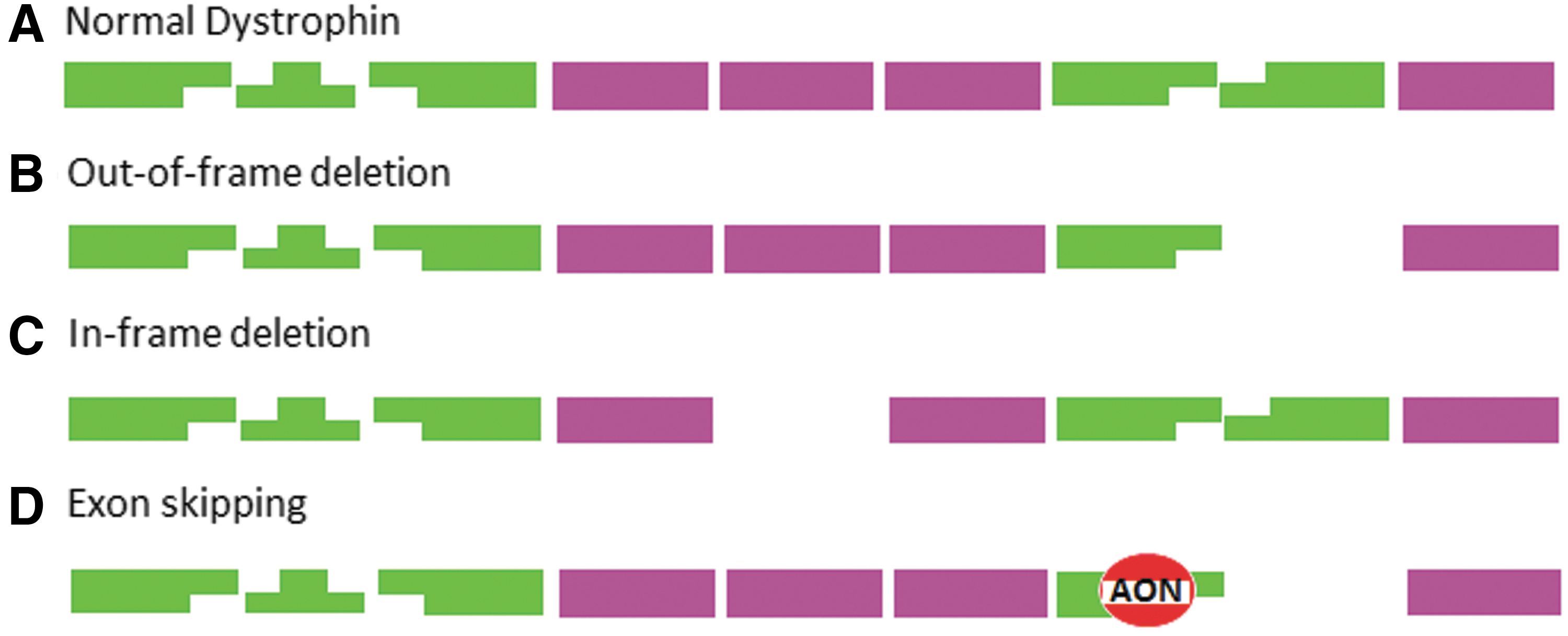
Antisense oligonucleotide (AON)-mediated exon skipping of the human DMD gene.
AONs are synthetically modified, single-stranded nucleic acids, which are designed to hybridize to consensus exon recognition or exonic splicing enhancer sequences on pre-mRNA. The length of AONs necessary for efficient exon skipping is typically 20 to 30 nucleotides. Antisense-induced exon skipping is thought to occur by interfering with the binding of serine/arginine-rich proteins, which play a crucial role in targeting consensus splice sites. This process involves specific exon exclusion along with its flanking introns from the mature mRNA. Several studies have been undertaken to investigate the optimal AON sequences within target exons or intron/exon boundaries including donor or acceptor splice sites or branch points (Arechavala-Gomeza et al., 2007; Popplewell et al., 2010, 2011). Evidence from a number of studies suggests that exon-internal targeting AONs are more efficient than AONs targeting the branch points or donor or acceptor splice sites (Errington et al., 2003; Aartsma-Rus et al., 2005, 2010). Exon skipping approaches would be applicable to approximately 83% of all DMD patients (Table 1); 54% of all patients with deletion mutations, 23% with small mutations, and 6% with duplications (Aartsma-Rus et al., 2009). However, 17% of DMD patients with larger deletions of more than 36 exons or deletions in the actin-binding N-terminus or the C-terminus of dystrophin are not treatable by exon skipping (Aartsma-Rus et al., 2009).
DMD deletions were reported in the Leiden DMD mutation database (
DMD, Duchenne muscular dystrophy.
Several groups have conducted successful preclinical studies using AONs to restore internally deleted yet functional dystrophin protein expression in animal models of DMD both in vitro (Graham et al., 2004; Iversen et al., 2009) and in vivo (Lu et al., 2005; Alter et al., 2006; Heemskerk et al., 2009; Yokota et al., 2011), in DMD patient cells in vitro in culture (van Deutekom et al., 2001; Aartsma-Rus et al., 2004) and in DMD patient muscle explants (Arechavala-Gomeza et al., 2007). On the basis of preclinical proof-of-concept, a number of clinical trials, phase I, phase II, and more recently phase III, have been undertaken using two different AON chemistries; 2′O-methyl phosphorothioate (2OMe-PS) and phosphorodiamidate morpholino (PMO) (Table 2).
2OMe-PS, 2′O-methyl phosphorothioate; i.m., intramuscular; i.v., intravenous; PMO, phosphorodiamidate morpholino; s.c., subcutaneous.
2OMe-PS–Mediated Exon Skipping
2OMe-PS comprises chemically synthesized, negatively charged, single-stranded RNA molecules with a phosphorothioate (PS) backbone that hybridize to the target exon (Dias and Stein, 2002; Bennett and Swayze, 2010). This PS moiety is very stable and resistant to intracellular endonucleases and exonucleases (Stein et al., 1988; Eckstein, 2000). To further increase this resistance to nuclease activity, hydrogen is replaced by a methyl group in 2OMe-PS (Opalinska and Gewirtz, 2002; Kurreck, 2003). Several studies have demonstrated successful exon skipping induced by 2OMe-PS in mdx mice (Lu et al., 2003, 2005), the CXMD dog model (Yokota et al., 2011), and DMD patient cells (van Deutekom et al., 2001; Aartsma-Rus et al., 2002, 2003, 2004). In the first clinical trial following preclinical studies, a phase I clinical trial of exon 51 skipping in DMD patients was undertaken to evaluate safety and tolerability of 2OMe-PS (PRO-051/GSK2402968; ProsensaTherapeutics). Four boys with DMD carrying deletions of exon 50, exons 48–50, exons 49–50, and exon 52 received a single intramuscular injection into the tibialis anterior muscle with a 0.8 mg of 20mer 2OMe-PS. Twenty-eight days after injection, each patient showed specific exon 51 skipping, leading to internally deleted but functional dystrophin protein expression. On muscle biopsy of these patients, 64% to 97% of myofibers at the sarcolemma were dystrophin positive with the mean intensity of dystrophin staining ranging from 17% to 35% of normal dystrophin protein intensity as seen in healthy muscle biopsy. No clinically adverse events were detected (van Deutekom et al., 2007).
Based on this intramuscular safety study, a phase I/IIa dose-escalation clinical trial of systemic administration using 0.5, 2, 4, and 6 mg/kg doses was completed with each dose administered to three DMD patients (Goemans et al., 2011). Following weekly abdominal subcutaneous injections of 2OMe-PS (PRO-051/GSK2402968) for 5 weeks in 12 patients, dystrophin expression was evaluated at 2 and 7 weeks after the last dose in the group injected with ≥2 mg/kg, and 2 weeks after the last dose in the group injected with 0.5 mg/kg. Dystrophin expression was observed in 60% to 100% of myofibers in 10 out of the 12 patients with a maximal dystrophin intensity signal of 15.6% of that observed in healthy muscle. Two patients receiving 0.5 mg/kg of 2OMe-PS did not have any detectable dystrophin protein apart from revertant fibers. It is important to note that this dystrophin quantification was normalized to healthy muscle tissue due to the lack of pretreatment biopsies in all patients. Despite the presence of dystrophin-positive fibers in treated muscles, there was no increase in the distance relative to baseline in the 6-min walk test at 2 weeks and 13 weeks after the last dose. After an interval of 6 to 15 months after the last dose, 10 patients entered a 12-week open label extension study receiving 2OMe-PS (PRO-051/GSK2402968) at a dose of 6 mg/kg per week. Unfortunately, two patients did not participate in the extension phase. One of these patients had become nonambulant and the other declined entry to the study. Following this further study, the distance that the participants could walk in 6 min had increased by a mean of 35 m from baseline in 8 of the 10 patients (Goemans et al., 2011). The 6-min walk test has been used to measure therapeutic outcomes and assess functional capacity in neuromuscular disorders, and a recent study demonstrated the reliability of this measurement (Goemans et al., 2013). It is very promising that systemically injected 2OMe-PS showed dose-dependent efficacy and benefits in walking distance without any severe adverse effects. However, it should be noted that this study was open label and therefore a confounding placebo effect on walking distance cannot be ruled out.
Following two studies using 2OMe-PS (PRO-051/GSK2402968) to assess different dosing regimens (ClinicalTrials.gov identifier: NCT01128855 and NCT01153932), a phase II clinical trial assessing efficacy, safety, and pharmacokinetics is ongoing. Fifty-four ambulant boys over 5 years of age with DMD will receive 3 or 6 mg/kg of 2OMe-PS, once weekly for 24 and 48 weeks with placebo controls (2:1 ratio) (ClinicalTrials.gov identifier: NCT01462292). Functional outcome will be measured at 24 and 48 weeks at completion of treatment. To investigate the safety and efficacy of this same drug in large groups of DMD patients, a phase III study is currently recruiting DMD patients. One hundred eighty ambulant patients over 5 years of age will receive 6 mg/kg of 2OMe-PS (PRO-051/GSK2402968) by subcutaneous injection once weekly for 48 weeks (ClinicalTrials.gov identifier: NCT01254019). The efficacy and safety of this drug will be investigated and compared to placebo controls. This study will be extended to an open label phase III clinical trial in which will 220 DMD patients from phase II and III clinical trials will receive 6 mg/kg of 2OMe-PS (PRO-051/GSK2402968) by subcutaneous injection once weekly for 104 weeks (ClinicalTrials.gov identifier: NCT01480245). This is the first long-term study of longer than 2 years' duration to study AON-mediated therapy in DMD patients. It will provide long-term safety, tolerability, and efficacy data in a large group of DMD patients. The estimated study completion date is December 2014.
To target exons other than exon 51 a phase I/IIa dose-escalating safety study using a 2OMe-PS (PRO-044; ClinicalTrials.gov identifier: NCT01037309) targeting exon 44 is currently underway. This drug can be applicable to DMD patients with deletions of exon 43, exon 45, exons 38–43, exons 40–43, exons 42–43, and exons 45–54. One group of DMD patients between 5 and 16 years of age will receive 0.5, 1.5, 5, 8, 10, and 12 mg/kg of 2OMe-PS (PRO-044) subcutaneously once weekly for 5 weeks. Another group of patients will receive 1.5, 5, and 8 mg/kg of 2OMe-PS (PRO-044) intravenously once a week for 5 weeks. In addition, PRO-045, PRO-052, PRO-053, and PRO-055, targeting exon 45, exon 52, exon 53, and exon 55 are currently in development by ProsensaTherapeutics. By skipping exons 45, 52, 53, or 55, approximately 8%, 4%, 8%, or 2% of DMD patient mutations would be potentially treatable (Aartsma-Rus et al., 2009). Encouraging safety and efficacy data targeting a second exon will not just be important for this second subset of DMD patients, but it is likely to accelerating the regulatory process for fast-track approval of 2OMe-PS AONs as a class of exon skipping compound.
PMO-Mediated Exon Skipping
PMOs are AONs characterized by the replacement of the deoxyribose moiety with a morpholine ring and replacement of the phosphodiester link by an uncharged phosphorodiamidate link (Hudziak et al., 1996; Summerton and Weller, 1997; Opalinska and Gewirtz, 2002; Kurreck, 2003). PMOs induce efficient exon skipping in vitro (Summerton et al., 1997) and in vivo (Alter et al., 2006; Heemskerk et al., 2009). The structure of uncharged PMOs is resistant to enzymes such as hydrolases, and it is therefore very stable in serum and plasma (Hudziak et al., 1996). PMOs have certain advantages over 2OMe-PS. They give more sustained, consistent exon skipping in mdx mice (Fletcher et al., 2006; Heemskerk et al., 2009) and in human DMD muscle explants (van Deutekom et al., 2007), although cell uptake of PMO is relatively poor compared with 2OMe-PS in vitro (Iversen et al., 2009). Moreover, PMOs exhibited a favorable safety profile with very low toxicity in cells (Iversen, 2001), mice (Sazani et al., 2010), and nonhuman primates (Sazani et al., 2011). This might be due to the fact that PMOs are uncharged and do not bind to plasma proteins, with the results that they are cleared rapidly from the circulation through urinary excretion, minimizing the risk of PMO accumulation in the liver and kidney. A single bolus intravenous injection of up to 2000 mg/kg of PMO (AVI-4658/Eteplirsen) showed no significant toxicological effects in mice (Sazani et al., 2010). Following a maximal feasible dose of 320 mg/kg of PMO (AVI-4658/Eteplirsen) by bolus intravenous or subcutaneous injection once weekly over 12 weeks in cynomolgus monkeys, there was no evidence of drug-related effects on clinical observations such as food intake, body and internal organ weights, urinalysis, and ophthalmoscopic and electrocardiographic examination (Sazani et al., 2011). However, a minimal to moderate renal drug effect was shown, following 12 weekly injections of 320 mg/kg of PMO (AVI-4658/Eteplirsen), leading to mild tubular vacuolation in the kidney of monkeys (Sazani et al., 2011).
On the basis of preclinical studies seen in the mdx mouse model (Gebski et al., 2003; Alter et al., 2006; Fletcher et al., 2006, 2007), the first clinical trial using PMO was completed. In a phase I/II clinical trial studying safety and efficacy of PMO, the UK MDEX Consortium has developed a 30-mer PMO (AVI-4658/Eteplirsen) in collaboration with AVI BioPharma (recently renamed Sarepta Therapeutics). This AON targets an intraexonic sequence in exon 51 of the human DMD gene. In a dose-escalating trial with seven DMD patients, PMO was injected intramuscularly into the extensor digitorum brevis muscle with contralateral muscle receiving a saline injection as a control (ClinicalTrials.gov identifier: NCT00159250). These patients carried deletions of exons 45–50, exons 47–50, exons 48–50, exons 49–50, exon 50, exon 52, and exons 52–63. Five patients receiving the highest dose (0.9 mg) of PMO (AVI-4658/Eteplirsen) exhibited good levels of local dystrophin protein production in treated extensor digitorum brevis muscles. The mean dystrophin fluorescent intensity ranged from 22% to 32% of that in healthy muscle and had a 17% increase compared to contralateral saline-treated muscle (Kinali et al., 2009). There was no dystrophin protein expression in two patients, who received 0.09 mg of PMO (AVI-4658/Eteplirsen). The treatment had no adverse effects. Following this intramuscular safety study, a phase Ib/II clinical trial into the clinical evaluation of PMO (AVI-4658/Eteplirsen) was extended to an open-label, dose-escalation study (0.5, 1, 2, 4, 10, and 20 mg/kg) of 12 weekly intravenous infusions of PMO in 19 ambulatory patients with DMD (Cirak et al., 2011) (ClinicalTrials.gov identifier: NCT00844597). Two weeks after the last dose of the drug, muscle biopsies were performed and analyzed. A dose-dependent restoration of dystrophin production was clearly seen. Out of 19 patients, seven patients showed an increased mean dystrophin fluorescence intensity of 9% to 16% of that in healthy muscle. The expression of this internally deleted dystrophin protein also restored components of the DAPC at the sarcolemma such as α-sarcoglycan, β-dystroglycan, and neuronal nitric oxide synthase, indicating that the induced dystrophin was functional (Cirak et al., 2012). This chemistry showed no adverse effects. Patients in this study displayed variation in their response to the drug. In particular, three patients showed 314%, 198%, and 110% increase in dystrophin fluorescence intensity compared to pretreatment biopsy taken from the same patients following treatment with 2, 10, and 20 mg/kg of PMO (AVI-4658/Eteplirsen), respectively. Elucidating the cause of such variation will be important for understanding how best to apply exon skipping therapy and for patient selection in future studies.
More recently, a phase II clinical trial has been ongoing with higher doses of PMO (update from Action Duchenne Conference 2012;
PS-Mediated Exon Skipping
PS comprises antisense DNA oligodeoxynucleotides that can bind to a complementary sequence on pre-mRNA, disrupting the use of splicing enhancer sequences (Askari and McDonnell, 1996; Pramono et al., 1996). PS-mediated DMD exon 19 skipping was demonstrated in DMD patient cells (Takeshima et al., 2001) and mdx mice (Takeshima et al., 2005). Following these preclinical studies, a clinical trial targeting exon 19 skipping in one DMD patient was conducted in Japan. A 31mer-PS was designed to hybridize to the exon splicing enhancer of exon 19 in order to induce an in-frame dystrophin mRNA (deletion of exons 19 and 20). This PS was administered to a 10-year-old DMD patient with an exon 20 deletion in the DMD gene (Takeshima et al., 2006). The patient received 0.5 mg/kg of PS, once weekly for 4 weeks. Following every intravenous infusion, the level of exon-skipped dystrophin mRNA was examined in peripheral lymphocytes collected from whole blood. Exon 19 skipped dystrophin mRNA product in peripheral lymphocytes was not detectable after the first two infusions and started to become visible after the last two infusions (Takeshima et al., 2006). One week after the last treatment, dystrophin-positive fibers were observed at the sarcolemma on biopsy of the biceps muscle of the patient with 6% exon-skipped dystrophin RNA product (Takeshima et al., 2006). This clinical trial, although only carried out with a single patient, demonstrates the apparent safety of delivering antisense DNA oligodeoxynucleotides by intravenous infusion to a DMD patient. However, it showed only very poor dystrophin restoration in peripheral lymphocytes and skeletal muscle. PS has therapeutic disadvantages with a relatively low binding affinity to targeted pre-mRNA and also cellular toxicity (Kurreck, 2003). The clinical assessment data of a single patient has limitations in evaluating the safety and efficacy of the drug. However, such clinical trials could still prove beneficial in the clinical development of AONs skipping rarer exons that can only help a minority of patients.
Peptide-Conjugated PMO-Mediated Exon Skipping
Noncharged PMOs have limited tissue uptake, and in particular, the exon skipping efficiency in cardiac muscle is very low; therefore, the development of second generation compounds is imperative. Above 90% of DMD patients suffer from a dilated form of cardiomyopathy, often leading to cardiac death in 10% to 20% of DMD patients (Bushby et al., 2003). Any potential therapy should ideally target cardiac muscle as well as skeletal muscles to have an overall clinical benefit to these patients. In order to improve cellular uptake of PMO, conjugation to cell-penetrating peptides (CPPs) can be used to dramatically enhance internalization of the PMO (Moulton et al., 2007; Jearawiriyapaisarn et al., 2008; Yin et al., 2008, 2010). CPP conjugation to PMO may enhance the binding affinity between the cationic CPP-conjugated PMO and anionic cell surface proteoglycans during endocytosis (Abes et al., 2006). A number of peptide conjugates that show enhanced uptake to skeletal and cardiac muscles in vivo are currently undergoing preclinical development. For example, positively charged arginine-rich peptide-conjugated PMOs with either (RXR)4XB or (RXRRBR)2XB (known as B peptide) motifs have shown very efficient delivery of PMO into skeletal muscle and heart in mdx mice (Yin et al., 2008). More recently, arginine-rich, PMO internalization peptide (Pip)-conjugated PMOs have been developed (Ivanova et al., 2008). Pips are characterized by a central hydrophobic motif flanked by arginine-rich domains. Pip-PMOs demonstrate efficient exon skipping in various muscles, resulting in up to 50% of the normal dystrophin protein expression in the heart in mdx mice with fivefold increase in exon skipping efficiency compared with B peptide–conjugated PMOs (Yin et al., 2011; Betts et al., 2012). The MDEX Consortium has planned a phase I clinical trial using optimized Pip-PMO for the targeted skipping of exon 53 of the human DMD gene, and it is expected that patients will be recruited in late 2014. Exon 53 skipping can be applicable to ∼8% of DMD patients, which is the third largest population in DMD (Aartsma-Rus et al., 2009).
While peptide-PMOs demonstrate enhanced efficacy in preclinical models, there is a concern that peptide-related toxicity or immune responses could occur in dystrophic animal models and in DMD patients. A toxicity study in 2007 showed that 150 mg/kg of CPP ((RXR)4XB)-conjugated PMO induced significant adverse effects in rats including lethargy and weight loss (Amantana et al., 2007). In addition, B peptide–conjugated PMO (AVI-5038) targeting exon 50 of the DMD gene was investigated for efficacy and safety (Wu et al., 2012). This study reported that monthly intravenous 30 mg/kg of AVI-5038 for 1 year into mdx mice resulted in very efficient exon skipping, leading to >50% and >15% dystrophin expression in skeletal muscles and cardiac muscle, respectively (Wu et al., 2012). However, the half lethal dose (LD50) was approximately 85 mg/kg (Wu et al., 2012). At the TREAT-NMD/NIH conference 2009, AVI Biopharma reported that weekly intravenous bolus injection of AVI-5038 over 4 weeks at a dose up to 9 mg/kg in four cynomolgus monkeys induced 40%, 25%, and 2% dystrophin exon skipping in diaphragm, quadriceps, and heart, respectively (Sazani et al., 2009). However, 9 mg/kg of AVI-5038 also induced mild renal tubular degeneration and higher doses (up to 15 mg/kg) given weekly by bolus intravenous administration for 12 weeks showed significant toxicological effects, particularly in relation to renal function (Sazani et al., 2009). Thus second generation peptide-PMO conjugates have considerable potential with typically excellent efficacy profiles. However, it is crucial to investigate their safety extensively prior to clinical trials.
Combination of Stem Cell Therapy and Exon Skipping
Cell-based exon skipping therapy is another promising approach to treat DMD. Transplantation of genetically modified adult muscle stem cells has great potential to regenerate skeletal muscle tissues. For stem cell therapy, adult muscle stem cells, including mesoangioblasts, muscle-derived stem cells, adult progenitor cells, blood- and muscle-derived CD133+ cells, and bone marrow–derived stem cells can be isolated from either muscle biopsies or blood (Farini et al., 2009). CD133+ cells isolated from peripheral blood or skeletal muscle tissue can be differentiated into muscle, hematopoietic, and endothelial cell lineages (Peault et al., 2007). Several approaches have also been undertaken using lentivirus encoding small nuclear RNA (snRNA) containing AONs against exon 51 in stem cells derived from DMD patients (Benchaouir et al., 2007; Quenneville et al., 2007). Isolated CD133+ cells derived from blood and muscle of DMD patients exhibiting frame-shift deletions of exon 49 and 50 of the DMD gene were corrected by lentivector expressing the U7 snRNA containing AONs to skip exon 51 (Benchaouir et al., 2007). Forty-five days after intramuscular transplantation of exon-skipped blood- and muscle-derived CD133+ DMD patient cells into immunodeficient scid/mdx mice, an increased number of dystrophin-positive fibers (136±54 and 417±53 dystrophin-positive fibers induced by blood- and muscle-derived CD133+ DMD patient cells, respectively) were shown in maximum cross-sections of tibialis anterior muscles of scid/mdx mice. There was also improvement of muscle physiology (Benchaouir et al., 2007). This study demonstrates the safety and feasibility of transplantation of exon-skipped CD133+ cells of DMD patients in an animal model. A possible next step would be correcting CD133+ DMD patient stem cells by exon skipping using a lentivector expressing snRNA to promote dystrophin expression in CD133+ cells. Corrected CD133+ autologous patient cells could then be safely transplanted back into a patient, minimizing the risk of immune response against donor cells in a recipient patient and abolishing the need for immunosuppressants. However, the full spectrum of extensive investigation of possible immune response against exon-skipped muscle and blood-derived stem cells in DMD patients is necessary prior to clinical trials.
Current Challenges and Future Considerations
Within the last few years, preclinical and clinical exon-skipping approaches using AONs for DMD treatment have been progressing rapidly with collaboration between multiple research centers, pharmaceutical companies, and patient groups. The data from clinical trials have so far shown that there are likely to be therapeutic benefits in the treatment of DMD patients, although it seems most likely that these benefits will be rather limited to first generation AONs. Moreover, there are several challenges to the development of AON-mediated exon-skipping therapies. Firstly, the exon-skipping approach is applicable only to specific exons corresponding to certain mutations in DMD patients. It is not possible to treat all DMD patients with a single exon-skipping therapy, since DMD patients have significant genetic heterogeneity. Regulatory authorities consider each AON with a different sequence targeting a specific exon to be an individual drug, and therefore the process of clinical approval for personalized AONs is currently challenging with the high costs of developing these drugs. A modified regulatory procedure is required to reduce the current hindrance to the development of AONs, which currently requires lengthy and expensive clinical trials. The Leiden group has estimated that ∼83% of DMD patients can be treated using single and double exon-skipping approaches (Aartsma-Rus et al., 2009). The major hotspot mutation regions are located between exons 43 and 53. In particular, exon 51 skipping, which is being studied in current clinical trials, would target the largest population (13%) of DMD patients and exon 53 skipping would target the third largest group (8%) of DMD patients (Aartsma-Rus et al., 2009). It has been suggested that multi-exon skipping, using cocktails of AONs or chemically linked AONs, around deletion hotspot regions (e.g., exons 45–55) may have the potential to treat approximately 63% of DMD patients (Beroud et al., 2007). Recently, a number of groups have developed multi-exon skipping using cocktails of AONs to skip multiple, nonadjacent DMD exons. Such a strategy has been shown to work in mdx mice (Aoki et al., 2012), the CXMD dog model (Yokota et al., 2009, 2011), and DMD patient cell line using AON cocktails (van Vliet et al., 2008) or self-complementary adeno-associated virus encoding U7 snRNA (Goyenvalle et al., 2012). Yet, this strategy is technically challenging due to low efficacy and will require further improvement of delivery of AON cocktails.
Another challenge is that the dystrophin restoration level by exon-skipping approaches is highly variable among different muscle groups even after repeated systemic administration (Heemskerk et al., 2010). Long-term treatment with AONs in mdx mice showed that efficacy of a dose regimen is dependent on the muscle group analyzed (Malerba et al., 2011; Wu et al., 2011). In particular, cell uptake of AONs in cardiac muscle is very poor compared with skeletal muscles (Brutsaert, 2003). It has been reported that dystrophin expression in skeletal muscles, leading to increase of activity, without correction of dystrophin expression in cardiac muscle results in 5 times increased cardiac injury along with dilated cardiomyopathy in mdx mice (Townsend et al., 2008). In contrast, dystrophin restoration in the skeletal muscles and diaphragm only, but not in the heart of mdx or dystrophin/utrophin-deficient double-knockout (dko) mice treated with B peptide–conjugated PMO improved cardiac function (e.g., left and right ventricular ejection fraction) to near wild-type levels (Crisp et al., 2011). The question of indispensability of dystrophin restoration in cardiac muscles for therapeutic outcomes in cardiac function remains controversial. Improvement of the delivery and efficacy of PMOs into the heart as well as skeletal muscles of DMD patients using cell-penetrating peptide-conjugated PMOs may overcome the current limitations. The expression of dystrophin in the brain and retina can also be affected in DMD. Loss of dystrophin protein in cerebral cortex cerebellum, hippocampus, and Purkinje cells of the brain leads to intellectual and cognitive impairment in 30% of DMD patients (Bresolin et al., 1994; Wicksell et al., 2004). In addition, DMD patients can suffer from lack of dystrophin expression in retina, leading to disturbed neurotransmission and impairment in red–green color vision (Cibis et al., 1993; Costa et al., 2007). Therefore, it is also important to consider the difficult task of delivering AONs through the blood–brain barrier in order to improve cognitive function in DMD patients. Since AONs have short half-life in biological environments, repeated administrations of therapeutic doses of AONs would likely be required for the lifetime of DMD patients to maintain adequate therapeutic effect. Therefore, safety issues must be examined extensively prior to clinical trial to assess the drug accumulation effects following repeated drug administration over an extended period. Improvement of exon-skipping efficiency and biodistribution of AONs could overcome these current obstacles of clinical trials. It may reduce the therapeutic dose and interval of administrations, minimizing the potential toxicity, off-target effects, and the cost burden.
Footnotes
Acknowledgments
The authors acknowledge funding from a Wellcome Trust Health Innovation Challenge Fund research grant. The authors thank to Linda Popplewell, Graham McClorey, Caroline Godfrey, and Andrew Douglas for providing scientific advice.
Author Disclosure Statement
No conflicts of interest exist.