
Abstract
Mucopolysaccharidosis type IIIA is a severe degenerative disease caused by an autosomal recessive defect of a gene encoding a lysosomal heparan-N-sulfamidase, the N-sulfoglycosamine sulfohydrolase (SGSH), the catalytic site of which is activated by a sulfatase-modifying factor (SUMF1). Four children (Patients 1–3, aged between 5.5 and 6 years; Patient 4 aged 2 years 8 months) received intracerebral injections of an adeno-associated viral vector serotype rh.10-SGSH-IRES-SUMF1 vector in a phase I/II clinical trial. All children were able to walk, but their cognitive abilities were abnormal and had declined (Patients 1–3). Patients 1–3 presented with brain atrophy. The therapeutic vector was delivered in a frameless stereotaxic device, at a dose of 7.2×1011 viral genomes/patient simultaneously via 12 needles as deposits of 60 μl over a period of 2 hr. The vector was delivered bilaterally to the white matter anterior, medial, and posterior to the basal ganglia. Immunosuppressive treatment (mycophenolate mofetil and tacrolimus) was initiated 15 days before surgery and maintained for 8 weeks (mycophenolate mofetil) or throughout follow-up (tacrolimus, with progressive dose reduction) to prevent elimination of transduced cells. Safety data collected from inclusion, during the neurosurgery period and over the year of follow-up, showed good tolerance, absence of adverse events related to the injected product, no increase in the number of infectious events, and no biological sign of toxicity related to immunosuppressive drugs. Efficacy analysis was necessarily preliminary in this phase I/II trial on four children, in the absence of validated surrogate markers. Brain atrophy evaluated by magnetic resonance imaging seemed to be stable in Patients 1 and 3 but tended to increase in Patients 2 and 4. Neuropsychological evaluations suggested a possible although moderate improvement in behavior, attention, and sleep in Patients 1–3. The youngest patient was the most likely to display neurocognitive benefit.
Introduction
M
Previous studies have reported absence of therapeutic benefit for bone marrow transplantation and for treatment with miglustat or genistein (Guffon et al., 2011; De Ruijter et al., 2012). A trial (
We report here the results of a phase I/II clinical trial in four children suffering from MPSIIIA who received intracerebral injection of an AAVrh.10-hMPS3A vector. We observed no sign of toxicity or lack of tolerance. Neuropsychological tests and behavior analysis suggested a possible improvement.
Protocol Design, Patients, and Methods
Protocol design
The study (
The treatment plan involved direct injections of the investigated product into both sides of the brain through six image-guided tracks with two deposits per track, one deep and one superficial, in a single neurosurgical session. Immunosuppression was achieved by the administration of a combination of tacrolimus and mycophenolate mofetil.
After surgery, safety and toxicity were evaluated by a weekly contact between the principal investigator (PI) and the families as well as during 14 in-person visits. At each visit, clinical progression was assessed and blood and urine analyses were carried out. Cerebrospinal fluid (CSF) was collected and analyzed at inclusion and at months 1, 3, and 12 after surgery. MRI was performed at inclusion and at 1 week, and 3 and 12 months after surgery. Neuropsychological tests were carried out at inclusion (1 month before surgery) and 1 year after surgery.
Selection of the patients
Recruitment information was transmitted to families potentially interested in participation by parents' associations and by pediatric neurologists and metabolic disease specialists. Parents were asked to express their interest in inclusion directly to the PI. Two to three face-to-face meetings between families and the PI took place before formal inclusion. An information letter and an informed consent document were distributed at least 15 days before inclusion. Twelve families expressed interest, but seven of the patients concerned did not meet the inclusion criteria. Four of the five eligible children were chosen for inclusion in this study on the basis of clinical criteria.
Product investigated: AAVrh.10-hMPS3A
The gene transfer vector used in the study was based on an AAV2 genome packaged into a serotype rh.10 capsid. The expression cassette included the mouse phosphoglycerate kinase promoter, the human SGSH cDNA, the internal ribosomal entry site from the encephalomyocarditis virus, the human SUMF1 cDNA, and the bovine growth hormone polyadenation unit (Winner et al.,2014). The AAVrh.10-hMPS3A vector was produced by a two-plasmid cotransfection procedure at the Belfer Gene Therapy Core Facility (Weill Cornell Medical College, New York, NY) under good manufacturing practice conditions. The production procedure included the transfection of a certified Human Embryonic Kidney 293T cell line with a plasmid containing the expression cassette (pAAVrh.10-hMPS3A) and an adenovirus/AAVrh.10 helper plasmid (Sondhi et al., 2012). The vector was released from cells by freeze–thaw cycles and purified on an iodixanol step gradient followed by affinity chromatography on heparin-agarose columns. The clinical formulation was obtained by dialysis against phosphate buffered saline, and 200 μl aliquots was stored at a concentration of 1×1012 vector genome per ml (vg/ml). Full characterization of the final formulated vector included an enzyme-linked immunosorbent assay (ELISA) for capsid protein, polymerase chain reaction (PCR) for transgene DNA, and Western blot analysis and activity assays for the transgenic protein. After the release of the GMP batch, the biological activity of the vector was assayed in vitro for infectivity and in vivo by assessing the induction of SGSH activity in the brains of MPSIIIA mice.
Surgical procedure
A previously described surgical procedure (Crystal et al., 2004; Souweidane et al., 2010) was adapted and performed by two trained senior neurosurgeons. The child was placed in a concord position, under general anesthesia, with the head maintained in position with a Mayfield headrest. The target and trajectories were decided on the basis of preoperative MRI performed under general anesthesia immediately before surgery. A neuronavigation system (Surgiscope; Isis) was used throughout the surgical procedure. Six 2 cm skin incisions and six skull burr holes were performed on the preplanned positions based on the preoperative MRI. The entry points and the trajectory were chosen to reach the white matter anterior, medial, and posterior to basal ganglia avoiding the vessels and the sulci. Three Greenberg autostatic flexible arms were installed on each side of the patient and six lumbar puncture needles (90 mm, 18G) were secured to the arms and used to perforate the dura. Two coaxial glass injections capillaries were inserted within each lumbar puncture needles. Each capillary, marked to indicate the preplanned depth, was connected to a microsyringe (Hamilton glass syringe 100 μl) for injection of the viral suspension and pushed down slowly to the injection site. The 12 injections were performed simultaneously, each delivering 60 μl of product at a rate of 0.5 μl/min to injection site (PHD ultrasyringe pump; Harvard Apparatus). A computed tomography scan was performed at the end of surgery to evaluate immediate blood effusion.
Biodistribution
The biodistribution of the vector was evaluated on urine specimens collected at H12, H36, and every 24 hr thereafter until a value below the threshold of 4.3×102 vg/ml was obtained for two consecutive determinations and then on day 7 and at months 1 and 3, using real-time quantitative PCR amplification of the bovine growth hormone polyadenation sequence present in the vector genome.
Clinical, neuropsychological, and safety evaluations during follow-up for 1 year
Patients were followed by weekly e-mail contact with families and by formal neurological examinations performed before surgery, daily (control of motricity and consciousness) and then weekly during the first month after surgery and at 3-month intervals thereafter.
Patients were subjected to the same series of tests, including the Psychoeducational Profile, 3rd edition (PEP-3), assessing the development, skills, and behavior of children with autism or other disabilities relating to communication (Schopler et al., 2005), the Vineland adaptive behavior scale (Vineland-II test) (Sparrow et al., 1984), and the Toddler Behavior Assessment Questionnaire (TBAQ) (Lemelin et al., 2007), at inclusion and 1 year after surgery. Patient 4 was also evaluated with the Brunet–Lezine revised test. None of the patients could be tested by the WPPSI-III, K-ABC, or Conners tests, because of their level of disability. Evaluations were performed by the same trained neuropsychologist throughout the study. Moreover, two informal written accounts were obtained from parents and from other care takers, describing the child at inclusion and 1 year after surgery.
Magnetic resonance imaging
Cerebral MRI was performed under general anesthesia (when possible), with a 1.5 T whole-body system (Achieva; Philips). Sequences included three-dimensional gradient echo (GE) T1-weighted sequences with multiplanar reconstructions (MPR) before and after gadolinium intravenous injection, coronal fluid attenuated inversion recovery (FLAIR) sequence, axial turbo Spin Echo, and GE T2 weighted and diffusion imaging sequences (b0, b1000) including apparent diffusion coefficient map. The brain and ventricular measurements were performed on reformatted T1 frontal slices parallel to the posterior edge of the brain stem, by measuring the largest bi-frontal horn diameters. On the same section, we also determined the amount of parenchyma present by measuring the largest bi-insular diameter immediately above the Sylvian fissure. The transverse diameter of the occipital horns was determined at the posterior limit of the splenium of the corpus callosum. The thickness of the corpus callosum was evaluated on a midsagittal section by Sylvius aqueduct lumen, measuring its maximum thickness at the levels of the genu and splenium (Martin et al., 2012).
Immunosuppressive treatments
Immunosuppressive treatments were initiated 14 days before surgery at doses of 0.2 mg/kg/day for tacrolimus (in oral solution) and of 1200 mg/m2/day for mycophenolate mofetil (in oral solution). Mycophenolate mofetil 4 hr pharmacokinetic profile was measured at a steady state, 7 days after treatment initiation. Mycophenolate mofetil dose was adapted to obtain AUC0-12h above 30 mg·g/liter and was maintained for 6 weeks after surgery. Trough blood Tacrolimus concentrations were measured weekly in the first month after surgery and subsequently at 3, 6, 9, and 12 months after surgery. Tacrolimus dosage was adjusted to reach trough blood concentrations ranging from 10 to 15 ng/ml during the first 3 months and from 7 to 10 ng/ml thereafter (during this first year). Prednisolone was also administered at a dose of 1 mg/kg/day for 10 days beginning the day before surgery.
Biological evaluation of safety and tolerance
The following blood tests were performed at inclusion, on day 7, and at months 1, 3, 6, 9, and 12 after surgery: hematological tests (erythrocytes counts; hemoglobin determinations; hematocrit; white blood cell count, including differential counts; platelet counts; coagulation tests; and erythrocyte sedimentation rates), biochemistry (electrolytes, proteins, total CO2, creatinine, urea, alkaline phosphatase, bilirubin, total protein, ASAT, ALAT, γGT, C-reactive protein, and troponin levels), immunovirology (serological tests for VZV, EBV, CMV, and IFNα titer). CSF samples were obtained on inclusion and at months 1, 3, and 12 after surgery while the patient was under general anesthesia for MRI. We determined the concentration of protein and glucose in the CSF, together with cell counts and IFNα titer. Urine samples were obtained on day 7 and at months 1, 3, and 12, and were evaluated for protein, glucose, and nitrite contents with a urinary dipstick test. Serum, peripheral blood monocytic cells, CSF, and urine samples were collected for storage in a biobank at the same time points.
Ethics: external supervision
The protocol was formally approved by the Agence Nationale de Sécurité du Médicament et des produits de santé for four patients and by the local ethics committee (Comité de Protection des Personnes Ile-de-France II) and had the support of parents' associations. A pre-established electronic case record form was completed by the PI at each visit and in cases of adverse events. Conformity was checked by an independent contract research organization and all serious adverse events were reported to a specialized independent pharmacovigilance organization. An international independent data-monitoring committee was established before the start of the trial to assess its progress and the safety data. This committee provided recommendations for the study, evaluated adverse events, and allowed the serial inclusions, at times separated by at least 2 months, of the four patients.
Results
Characteristics of the patients at inclusion
The characteristics of the patients at diagnosis and inclusion are described in Table 1. Patient 4 was younger than Patients 1–3. Patient 1–3 already displayed a considerable reduction of neurocognitive abilities. Neurocognitive performances were significantly better for Patient 4, but remained significantly lower than that of the general population of the same age (Table 1 and Supplementary Table S1; Supplementary Data are available online at
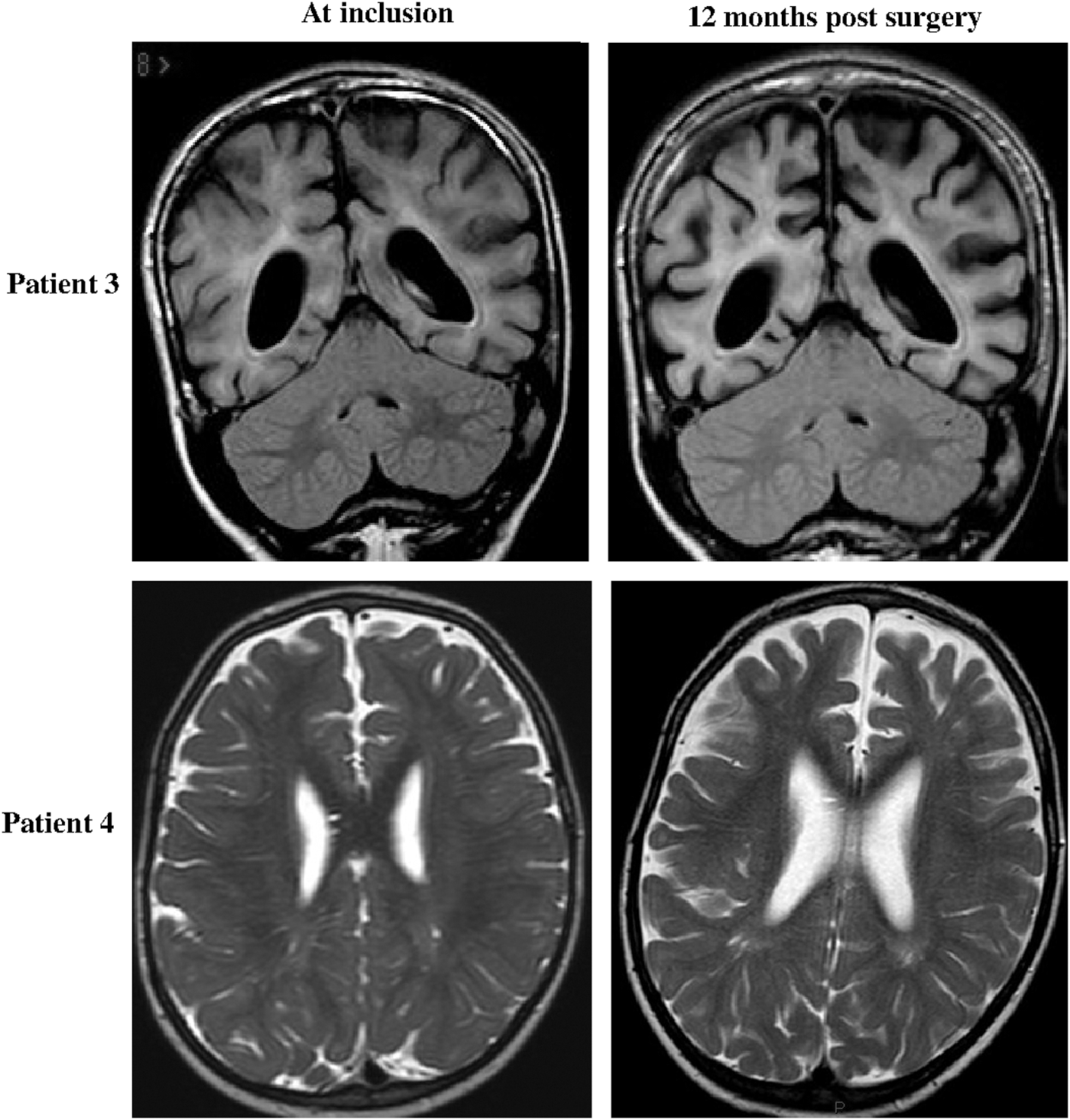
MRI scans of representative Patients 3 and 4 showing the presence (Patient 3) or absence (Patient 4) of brain atrophy at inclusion, and comparative MRI scans obtained at the end of follow-up. Patient 3: Frontal FLAIR sequences showing a stable ventricular passive enlargement (deep atrophy) at inclusion and stability 12 months after surgery. White matter hypersignal intensity is visible. Patient 4: Axial T2 sequences showing a normal ventricular size at inclusion and an increased ventricular size at the end of follow-up. FLAIR, fluid attenuated inversion recovery; MRI, magnetic resonance imaging.
PEP-3, Psychoeducational Profile, 3rd edition; SD, standard deviation.
Ability to communicate in two-word combinations and time when this ability was subsequently lost.
Too young.
Results given as developmental age. See also Supplementary Table S1 for exhaustive data.
L, left; R, right.
See the Protocol Design, Patients, and Methods section for a description of the measurements. All measurements are given in mm.
Neurosurgical procedure and biodistribution
The therapeutic vector was delivered at a dose of 7.2×1011 vg/patient as 12 deposits over a period of 2 hr, according to the protocol, in all four patients. No significant events were observed during the procedure itself. Viral titers in urine were above the threshold of detection for the first 3 days after surgery in Patient 1 (maximum 5.4×103 vg/ml at H12), for 24 hr in Patient 2 (maximum 1.7×104 at H12), for 3 days in Patient 3 (maximum 3.6×104 at H12), and for 2 days in Patient 4 (maximum 9.5×102 at H36). They were below the detection threshold in subsequent samples obtained up to 3 months after surgery. None of the four patients displayed interferon-α activity in serum samples on day 7 or in CSF 1 month after surgery (the first time points of the evaluation), or thereafter. Anti-AAVrh.10 or anti-SGSH antibodies were not detected by ELISA in the serum of the four patients 1, 3, 6, and 12 months after surgery (Supplementary Fig. S1).
Primary endpoints: safety and tolerance
The postoperative clinical period was uneventful and all four patients were discharged from hospital 9 days after surgery. Clinical examination and general appearance, including growth rates, remained stable during the year of follow-up. The sizes of the liver, spleen, and kidney and the principal heart measurements (left ventricular size in diastole and systole, ventricular septum and posterior wall thickness, shortening fraction, Doppler hemodynamic measurements of flow throughout cardiac valves and great arteries) were identical at inclusion and at the end of follow-up. No suspected unexpected serious adverse drug reaction was reported. In total, 87 emergent adverse events were recorded between the inclusion visit and the end of follow-up (Table 3). All 87 events were classified as mild to moderate in severity. Five adverse events were classified as serious because they required a short period of hospitalization. All resolved within 1–4 days. The five serious adverse events were gastroenteritis, head injury, viral lung infection, transient bronchospasm at induction of anesthesia, and acute viral infection. The two most frequently reported adverse events were upper respiratory tract infections and diarrhea, both of which were noted in the medical history before inclusion. Diarrhea increased in intensity and chronicity in two patients but was present in all four patients included. It was greatly improved by a fiber-free, residual-free diet. Immediate postsurgical brain imaging showed the sites of bone penetration (Fig. 2).

Postsurgical aspects in representative Patient 2. Left: 3D bone reconstruction on computed tomography scan performed immediately after surgery, demonstrating the six burr holes. Middle and right: MRI 7 days after surgery (middle: axial MPR sequence; right: axial turbo Spin Echo sequence) showing four tracks (arrows) and blood effusion at the level of the left posterior track. MPR, multiplanar reconstruction. Color images available online at
Upper respiratory tract infection, fever, acute viral infection.
Hemiparesis for a few hours the day after surgery (no sign of bleeding on computed tomography scan and on magnetic resonance imaging [MRI] on day+8).
Hemosiderin deposits observed on MRI on day+8.
Intraparenchymatous tracks were barely visible and intraparenchymatous blood effusions were observed in 3 of the 24 tracks (6 tracks per patient) (Fig. 2 at day 7 for Patient 2 with the largest blood effusion). Intraparenchymatous blood effusions, or the sequelae of them, were not detected on MRI performed at the 12-month visit. No sign of inflammation (hypersignal in FLAIR sequences or T2-weighted sequences) or necrosis was detected, including at day 7 after surgery.
No lack of compliance with the immunosuppressive drug treatment was reported. The results of mycophenolate mofetil AUC0-12h performed at day 7 after treatment initiation were 41, 59, 31, and 60 mg·hr/liter in Patients 1–4, respectively, leading to drug adjustment in three of the four patients. No further titration was performed until the end of treatment at 6 weeks after surgery. The mean trough blood tacrolimus concentration was 10.4±2.8 ng/ml (mean±SD) during the first 3.5 months (target=10–15 ng/ml; Patient 1=9.8±1.4 ng/ml; Patient 2=10.3±3.6 ng/ml; Patient 3=11.4±4.1 ng/ml; Patient 4=10.0±1.6 ng/ml) and frequent modifications of drug dose were required during this initial period (10% of titrations were >15 ng/ml and 43% <10 ng/ml). The mean tacrolimus concentration was 8.4±1.4 ng/ml in the following period (target=7–10 ng/ml; Patient 1=7.5±1.1 ng/ml; Patient 2=10.0±0.9 ng/ml; Patient 3=8.5±0.7 ng/ml; Patient 4=9.5±1.9; 20% of concentration >10 ng/ml and 15%<7 ng/ml). No leukopenia or lymphopenia was observed in the four patients (leukocytes=4.98±0.6×109/liter at inclusion and 10.38±2×109/liter at end of follow-up; lymphocytes=1.70±0.23×109/liter and 3.79±1.70×109/liter) (Supplementary Table S2). Mean plasma creatinine concentration was 30 μM (range 21–34 μM) before the start of treatment and 47.5 μM (range 47–56 μM) at the 12-month visit (normal range 27–77 μM) (Supplementary Table S2). CSF samples remained normal in terms of their cellular and proteins contents.
Secondary endpoint: initial evaluation of efficacy
No surrogate marker of efficacy was validated before the trial, and the results at 1 year were analyzed with the aim of defining endpoints for use in future efficacy studies. Changes in brain atrophy were analyzed by MRI (Fig. 1). Six measurements were made on two plane slides on MRI at inclusion and at 12 months after surgery (Table 2). Brain atrophy values were similar and high in Patients 1 and 3 and showed a tendency to increase over the follow-up period in Patients 2 and 4. The PEP-3, Vineland-II, and TBAQ tests were successfully administered, together with the revised Brunet–Lezine test for Patient 4. The changes in performances of each child on the PEP-3, Vineland, and TBAQ tests are shown in Fig. 3 (the child being compared with him/herself; see Supplementary Table S1 for full data). PEP-3 results for cognitive and motor skills were stable and low for Patients 1–3 but with a decrease in performance noted for the “Fine motor” items for Patients 2 and 3 and for “Receptive language” items for Patient 2. Patient 4 displayed an improvement in motor abilities and stable language and cognition. Patient 4 also displayed an improvement in characteristic motor behavior items. The Vineland test results showed improvements in autonomy and motricity for Patient 4, whereas Patient 2 displayed a decrease of performance in these two areas and in communicative skills. Finally, the TBAQ showed an improvement in social interactions and more focused behavior in all four patients. These findings were consistent with the reports from the families who also noted improvements in sleeping pattern and an increase in the overall quality of family life. The sleep and mood regulators that were already part of the treatment of two of the four patients before inclusion were discontinued 6 and 8 months after surgery. Following neurological and general clinical evaluations, Patients 1–3 were considered to be clinically stable and Patient 4 was considered to have improved.
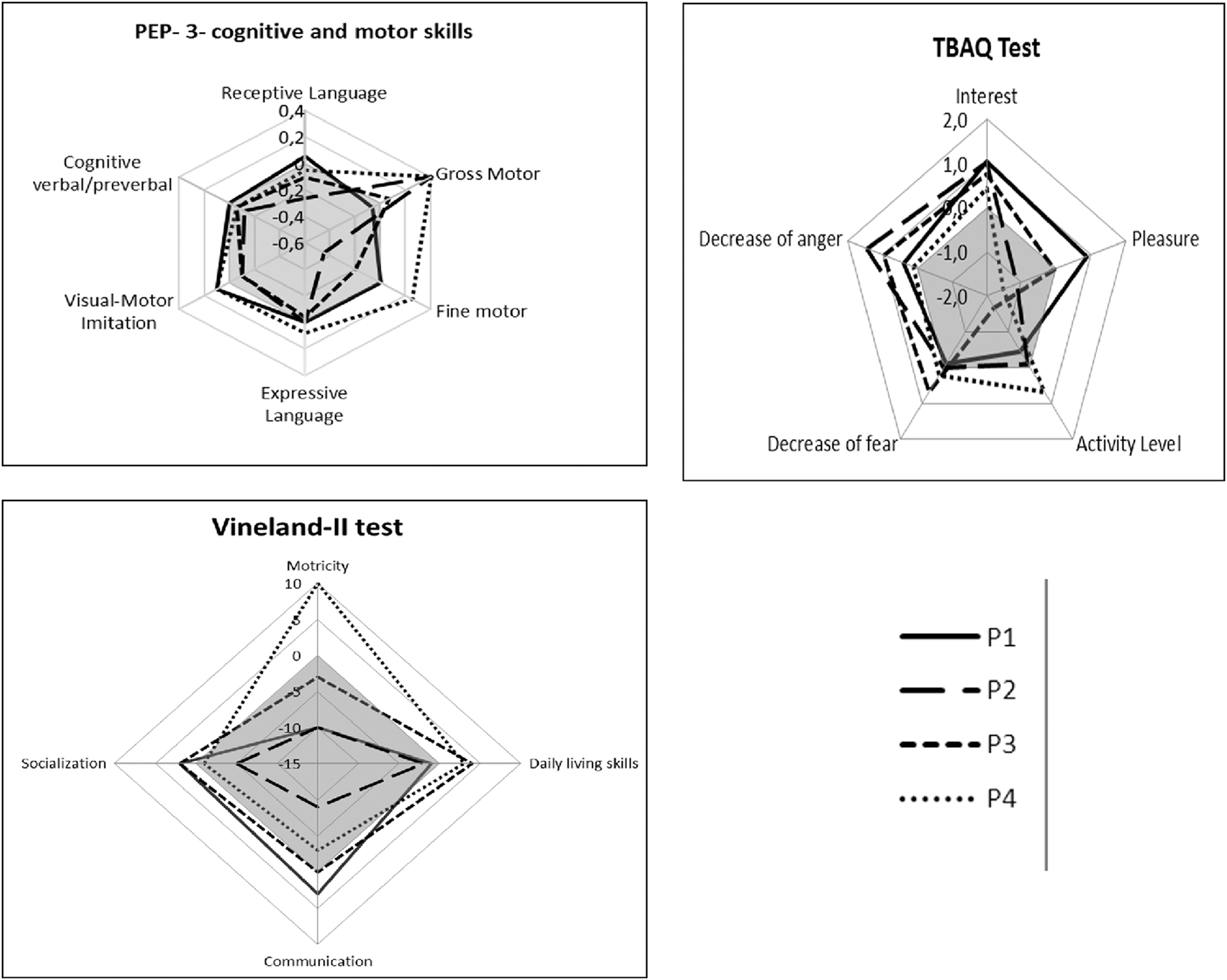
Schematic representations of changes over the follow-up period in the performances of each of the four patients in the PEP-3, Vineland, and TBAQ tests. The scales indicate the changes in score between onset and at the end of follow-up, each patient being compared with himself or herself. The negative area in gray corresponds to a decrease in performance. The positive area in white indicates an improvement in performance. PEP-3, Psychoeducational Profile, 3rd edition; TBAQ, Toddler Behavior Assessment Questionnaire; Vineland, Vineland adaptive behavior scale (Vineland-II test).
Discussion
Mucopolysaccharidosis, particularly forms with severe brain involvement, have long been recognized as prime candidates for gene therapy. We report here initial results evaluating safety and efficacy in the first gene therapy clinical trial in patients with MPS. An AAV vector with a serotype rh.10 capsid and encoding both human SGSH and SUMF1 cDNAs was injected intracerebrally in four children with Sanfilippo type A disease (MPSIIIA) and were followed up for 1 year.
Five main parameters were taken into account when designing the clinical study: age at inclusion, type of vector, route and sites of injection, and the use of immunosuppression. Retrospective natural history studies have shown that evidence of cognitive regression is first observed at the age of 3 years, whereas diagnosis occurs at a mean age of 5 years (Héron et al., 2010). This information governed our choice of the age range at inclusion. However, a thorough evaluation of the four children at inclusion demonstrated that the three patients over the age of 5 years already presented cognitive delay and brain atrophy. The youngest patient, who was less than 3 years old at inclusion, already had a moderate cognitive deficit, but no brain atrophy on initial MRI. The vector, its dose, and its route of injection were selected on the basis of the high efficiency reported in animal models of MPS (Ellinwood et al., 2011) and existing clinical data suggesting safety in children with neurodegenerative diseases (Worgall et al., 2008; Leone et al., 2012; Hwu et al., 2012). In preclinical studies performed in MPSIIIA and MPSIIIB mice, broader intracerebral vector and enzyme axonal transport was observed for MPSIIIB than for MPSIIIA. This may reflect differences in vector design and concentration or may be because of the ability of the enzymes produced to be transported along axons. We decided to use 12 points of injection into the supratentorial white matter during a single neurosurgical session, to increase the amount of vector injected, to ensure the broadest possible diffusion, and to limit the risks. Finally, we administered immunosuppressive treatments based on the preclinical results obtained in MPSIIIB dogs and the high frequency of antivector antibody production reported in previous intracerebral gene therapy trials in human patients, consistent with antigen presentation outside the brain and a risk of the transfected cells being eliminated by the host immune response. Alternative strategies are currently being developed by other groups, in mouse and dog models of MPSIIIA, with less invasive routes of injection, including the administration of AAV2/9 encoding SGSH via the CSF or systemically and liver gene transfer with an AAV2/8 encoding an engineered sulfamidase that efficiently crosses the blood–brain barrier (Ruzo et al., 2012; Haurigot et al., 2013; Sorrentino et al., 2013). These alternative systems may provide options for gene therapy in the future.
Despite a slow injection of the vector and a very limited surgically induced blood effusion, measurable vector leakage to the periphery occurred in the first 3 days after surgery, as shown by the detection of the vector at low titers in the urine of all four patients. However, no anti-AAVrh.10 or anti-SGSH antibodies were detected by ELISA in the serum 12 months after surgery. The normal CSF results obtained 7 days and 1 month after surgery, the absence of FLAIR or T2-weighted hypersignals in the white matter, and the absence of abnormal enhancement around the injection points on the MRI scans performed 7 days and 3 months after surgery suggested that there was little or no inflammatory or specific intracerebral immune response at the vector deposition sites. This might be because of the adjunct steroid and immunosuppressive treatment, as observed in dogs treated with a human cDNA-containing vector (Ellinwood et al., 2011). It may also reflect a pre-existing degree of tolerance in children, as three of the children studied here had residual enzymatic activity in the blood before treatment. The use of a species-specific transgene probably decreases the intensity of antitransgene immune responses and the level of nonspecific inflammation, as demonstrated in a feline model of Sandhoff disease and in the MPSIIIA dog model (Bradbury et al., 2013; Haurigot et al., 2013).
The safety data for this trial were reassuring. The neurosurgery was uneventful although technically difficult in Patient 3, who had the highest degree of brain atrophy. Eighty-seven adverse events were reported through very careful weekly monitoring, a number of events similar to that reported in other similar protocols (Leone et al., 2012). Infectious events, presumably viral in nature, which occur frequently in the natural course of this disease, did not appear to be more frequent during follow-up. Diarrhea, which was also reported in the medical histories of all patients, was the most troublesome adverse effect, but was improved by dietary modification. The results of biological tests performed during follow-up were in the normal range, including those for creatinine concentration, which nevertheless increased, as frequently reported in patients on tacrolimus.
The evaluation of efficacy was only a secondary end point in this phase I/II trial on four children with a relatively short follow-up period. Measuring SGSH enzyme activity or levels of heparan sulfate degradation intermediates in the lumbar CSF may provide useful surrogate markers of the transgene activity in the brain, but no validated assays have been developed so far in MPSIIIA. In order to gather material for future validation studies, CSF samples were collected during the trial and stored. Preliminary measurements of the HS degradation intermediates using the Sensi-Pro method (Lawrence et al., 2012) in these samples did not show obvious modifications after treatment (data not shown). However, these results must be interpreted with caution in the absence of assay validation.
The rate of development of brain atrophy, a feature of the disease reported in all patients, during the natural course of the disease has never been determined on large series (Banone et al., 1999; Zafeiriou et al., 2001; Kara et al., 2008). Brain atrophy was observed at inclusion in three of the four children and remained stable in the two children with the highest levels of atrophy. Conversely, Patient 4 displayed no atrophy on inclusion, but brain atrophy, or at least the ventricles sizes, in this patient increased during the year of follow-up. This suggests that brain atrophy occurs early in MPSIIIA and that it may take time to slow or stop this atrophy, after initiation of treatment.
The choice of appropriate neuropsychological tests was limited by the initially very low cognitive level of Patients 1–3. In these three patients, the results of the PEP-3 neurocognitive tests suggested stability for most items, but a decrease for the fine motor and receptive language items. The initially low cognitive level of Patient 1 and the floor effect of the tests made it impossible to assess a possible loss of cognition. The Vineland and TBAQ tests and the parents' reports suggested changes in attention levels, more focused behavior, and improvement in sleep. A longer follow-up period would be required to determine whether the moderate benefit or absence of decline observed is persistent and steady. The general behavior and neuropsychological performances of Patients 1 and 2 remain the same 24 months after surgery. For Patient 4, evaluations suggested some progress in most of the items tested, whereas regression would normally have been expected. These observed benefits, particularly in the youngest patient (Patient 4), may result from the local production of SGSH, as hoped. However, extensive neuroinflammation is a common feature of MPSIIIA (Jeyakumar et al., 2004; Denny et al., 2006; Ellinwood et al., 2011; Archer et al., 2014) and the anti-inflammatory activity of immunosuppressive drugs may also have a positive effect on neuropathological lesions. In addition, we cannot also exclude the possibility that the observed benefit was within the range of variation observed over a single year in the natural course of the disease, although only a few results have been published for serial neuropsychological evaluations in children with MPSIIIA (Valstar et al., 2011).
In conclusion, the intracerebral administration of AAVrh.10 carrying the human SGSH and SUMF1 cDNAs was safe and well tolerated after 1 year in the four children studied, validating the surgical approach for direct AAV vector delivery in the brain parenchyma. Neurocognitive evaluations suggested a cognitive benefit in the youngest child receiving the vector, whereas such a benefit was considered possible, but more limited, in the three older patients. We believe that the safety of the approach allows considering further trials in children under the age of 5 years with no evidence of brain atrophy on MRI. Increased vector dosage as well as additional injection sites could be tested. In addition, neonatal screening should be made mandatory if therapeutic benefit can be demonstrated (Meikle et al., 2004).
Footnotes
Acknowledgments
We thank the four participating patients and their parents and, in alphabetical order, K. Aiach, P. Aubourg, G. Bensasson, B. Bigger, P. Bourget, B. Chauvin, B. Crawford, A. Le Meur, F. Piguet, F. Rosenberg, D. Sondhi, M. Souweidane, and A.-M. Taburet, Alliance SanFilippo, Association Française contre les Myopathies, Fondation Sanfilippo Suisse, and the five members of the Independent Data Safety Monitoring Committee. The study was sponsored by Lysogene and conducted by the investigators in accordance with the protocol and with good clinical practice guidelines.
Author Disclosure Statement
M.T., M.Z., B.H., S.B., K.D., C.A., C.B., V.F., A.B., A.F., R.G.C., T.B., T.R., and J.-M.H. have no conflicts of interest relating to this trial to disclose. O.D. holds equity in Lysogene SAS. M.H. and F.V. are full-time employees of Lysogene SAS.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.