
Abstract
Enzyme replacement therapy (ERT) is the standard-of-care treatment of Pompe disease, a lysosomal storage disorder caused by deficiency of acid α-glucosidase (GAA). One limitation of ERT with recombinant human (rh) GAA is antibody formation against GAA. Similarly, in adeno-associated virus (AAV) vector-mediated gene transfer for Pompe disease, development of antibodies against the GAA transgene product and the AAV vector prevents therapeutic efficacy and vector readministration, respectively. Here a nondepleting anti-CD4 monoclonal antibody (mAb) was administrated intravenously prior to administration of an AAV2/9 vector encoding GAA to suppress anti-GAA responses, leading to a substantial reduction of anti-GAA immunoglobulins, including IgG1, IgG2a, IgG2b, IgG2c, and IgG3. Transduction efficiency in liver with a subsequent AAV2/8 vector was massively improved by the administration of anti-CD4 mAb with the initial AAV2/9 vector, indicating a spread of benefit derived from control of the immune response to the first AAV2/9 vector. Anti-CD4 mAb along with AAV2/9-CBhGAApA significantly increased GAA activity in heart and skeletal muscles along with a significant reduction of glycogen accumulation. Taken together, these data demonstrated that the addition of nondepleting anti-CD4 mAb with gene therapy controls humoral immune responses to both vector and transgene, resulting in clear therapeutic benefit in mice with Pompe disease.
Introduction
P
During ERT for Pompe disease, the administrated rhGAA provokes high antibody titers in a subset of patients, which has correlated with poor long-term outcomes. 1,3,4 Pompe disease patients who lack any residual GAA protein, and therefore are incapable of inducing self-tolerance to GAA, are deemed cross-reacting immune material (CRIM) negative. CRIM-negative Pompe disease subjects are at higher risk of producing very high anti-GAA antibodies, which markedly reduce efficacy from ERT with rhGAA. 5 This issue was demonstrated in the first clinical trial of ERT in Pompe disease using Chinese hamster ovary cell-derived rhGAA, 5 in which the initial two CRIM-negative patients produced much higher titers of anti-GAA antibodies than did the third, CRIM-positive patient. Formation of high-titer anti-GAA antibodies correlated with markedly reduced efficacy in the CRIM-negative patients.
Current approaches to the control of immune responses in Pompe disease include broad-based immunosuppressive agents, including a variable combination of drugs such as rituximab, methotrexate, and intravenous immunoglobulin, based largely on experience form autoimmune disease and hemophilia. 6 –9 These agents have successfully lessened neutralizing responses to rhGAA in patients with Pompe disease, but they are associated with untoward side effects.
An established model of Pompe disease, a GAA knockout (KO) mouse, features the accumulation of lysosomal glycogen in muscle and several organs, along with excessive accumulation of autophagic substrates and impaired fusion of autophagosomes with lysosomes. 10 –12 GAA-KO mice are similar to CRIM-negative patients with Pompe disease with regard to immune tolerance to GAA, because the mice do not produce endogenous GAA and lack immune tolerance to introduced GAA, either in the form of ERT 13 or expression from an adeno-associated virus (AAV) vector that constitutively expressed GAA. 14 We previously reported a strategy for inducing immune tolerance in GAA-KO mice with an AAV vector containing a liver-specific regulatory cassette, by administering a low number of the vector particles to GAA-KO mice prior to the initiation of ERT. 15 The method induced immune tolerance against administrated GAA with the increase of therapeutic efficacy in the heart and diaphragm. Efficacy from this immunomodulatory gene therapy required liver-specific hGAA expression that activated antigen-specific regulatory T-regulatory (Treg) cells. 16
High-affinity antibody production requires T helper cell, and CD4-deficient mice lacking helper T cells fail to initiate antibody formation to the protein products of gene therapy. 17 An in vitro study with lymphocytes showed that CD4+ and CD8+ T cells displayed an increase in expression of proinflammatory cytokines including intracellular interferon-gamma (INF-γ) and tumor necrosis factor-alpha (TNF-α), in response to rhGAA in treated patients, compared with untreated patients and healthy subjects. 18 This suggests that T cells play a critical role in the immune response to rhGAA in Pompe patients. In a series of studies using a nondepleting anti-CD4 monoclonal antibody (mAb), reduced immune responses have been demonstrated in a variety of settings, including infusion of foreign proteins, 19 graft rejection, 20 and autoimmune diseases, 21 including rheumatoid arthritis. 22
Extensive preclinical studies in rodents and nonhuman primates, using nondepleting anti-CD4 mAb, have demonstrated that a short 1–2-week course of mAb treatment, in conjunction with the desired antigen, is capable of inducing long-term immune tolerance to the antigen. 19 –23 The use of nondepleting anti-CD4 mAb has also shown to decrease the immune response to introduced rhGAA in Pompe disease mice. 24 Anti-CD4 mAb in combination with cyclosporine was effective at suppressing anticapsid antibodies in response to administration of an AAV vector, although the effect was transient. 25 In the present study, we describe the inhibition of T helper cells by anti-CD4 mAb to achieve the control of immune responses to an AAV vector in GAA-KO mice. The vector administered contains a ubiquitously active regulatory cassette, and previously provoked robust immune responses in GAA-KO mice. 14 We hypothesized that suppressing transgene-directed immune responses would enhance the efficacy achieved by this vector. To our knowledge, this is the first successful use of nondepleting anti-CD4 mAb alone to prevent antibody formation against a therapeutic protein in the context of gene therapy.
Materials and Methods
Preparation AAV vectors
Briefly, 293 cells were transfected with the p-trsLSP-GFP (courtesy of Dr. Douglas McCarty, Nationwide Children's Hospital, Columbus, OH) vector plasmid 26 or pAAV-CBhGAApA vector plasmid, 27 the AAV8 or AAV9 packaging plasmid 28 (courtesy of Dr. James M. Wilson, University of Pennsylvania, Philadelphia, PA), and pAdHelper (Stratagene). Cells were harvested 48 hr following infection and freeze-thawed three times, and isolated by sucrose cushion pelleting followed by two cesium chloride gradient centrifugation steps. AAV stocks were dialyzed against three changes of Hanks buffer with 5% sorbitol added to the third dialysis, and aliquots were stored at −80°C. The number of vector DNA-containing particles was determined by DNase I digestion, DNA extraction, and Southern blot analysis. All viral vector stocks were handled according to Biohazard Safety Level 2 guidelines published by the NIH.
Animal studies
All animal procedures were performed in accordance with Duke University Institutional Animal Care and Use Committee–approved guide lines. Six-month-old GAA-KO mice were administrated 200 μl of 0.1 mg/ml anti-CD4 antibody through intravenous injection. The mice were injected with 1.0×1011 vp AAV2/9-CBhGAApA on day 0. The anti-CD4x3 group (G4; Fig. 1A) received intravenous anti-CD4 mAb (YTS177; 50 mg/kg) at day −1, +6, and +13, whereas the anti-CD4x1 (G3; Fig. 1A) was injected with anti-CD4 only on day −1. For the immune challenge with rhGAA, mice in group G3 (Fig. 1A) were injected intravenously with rhGAA (20 mg/kg) and intraperitoneally with incomplete Freund's adjuvant as described 15 10 weeks after injection of the vector. The mice were euthanized at 14 or 24 weeks following vector injection for collection of tissues. GAA activity and glycogen content were analyzed as described. 29

A short-term treatment with anti-CD4 mAb prevented anti-GAA formation. GAA-KO mice were treated with AAV2/9-CBhGAApA with (+) anti-CD4 mAb (either once or three times) or without (−) anti-CD4 mAb pretreatment.
Antibody quantification
The enzyme-linked immunosorbent assay (ELISA) for anti-GAA IgG1 was performed as described. 30 Briefly, rhGAA (5 μg) in carbonate buffer was coated onto each well of a 96-well plate (Costar cat. no. 3596; Corning Life Sciences) at 4°C overnight. After a wash with PBS containing 0.05% Tween 20, plasma samples with serial dilutions ranging from 1:10 to 1:200,000 were added in duplicate to rhGAA-coated plates and incubated at room temperature. The wells were washed with phosphate buffered saline (PBS) containing 0.05% Tween 20, incubated with a 1:2,500 dilution of alkaline phosphatase-conjugated sheep antimouse IgG1 at room temperature for 1 hr, and washed 3 times with PBS, and finally alkaline phosphatase substrate (p-nitrophenyl phosphate) was added. The absorbance at 411 nm was measured with a Tecan SpectraFluor microplate reader (MTX Lab Systems). All samples yielded absorbance values that were within the linear range of the assay at their respective dilutions. Absorbance values were deemed positive if both values at any given serial dilution were >0.1. In this study, screening for anti-GAA IgG1 was performed in samples diluted 1:200.
Assays of IgG subclasses
To determine the repression of antibody formation by the injection of anti-CD4, an ELISA was performed. Plates were coated with 1 μg/ml of rhGAA in carbonate buffer at 4°C overnight. Standard curves specific for murine IgG (Sigma Chemical Co.), IgG1 (R&D Systems), IgG2a (R&D Systems), IgG2b (R&D Systems), IgG2c (SouthernBiotech), IgG3 (R&D Systems), and IgM (Sigma) were also coated to the wells in seven 2-fold dilution starting from 1 μg/ml. After coating, wells were washed with PBS with 0.05% Tween 20 and blocked with PBS with 2% BSA. Plasma samples were loaded and incubated at 4°C overnight, and detection was made with specific anti-Ig antibodies conjugated with horseradish peroxidase. Detection was performed by adding to the wells 3,3′,5,5′-tetramethylbenzidine substrate (BD Biosciences), and color development was measured at 450 and 570 nm (for background subtraction) on an Enspire plate reader (Perkin Elmer) after blocking the reaction with H2SO4.
Vector readministration
To evaluate the effect of anti-CD4 in the transduction efficiency in liver, anti-CD4 mAb-treated mice were injected with the GFP expression vector, AAV2/8-LSPGFP, at 20 weeks after anti-CD4 injection. The mice were euthanized 4 weeks after the vector administration. Liver samples were immediately embedded and frozen in optimal cutting temperature medium (OCT), and stored at −80°C. The OCT-embedded samples were sectioned with 5 μm thickness and mounted on poly-L-lysine-coated slides. The slides were warmed at 60°C for 15 min to melt the OCT and washed with xylene to remove the OCT following three times washing steps with ethanol (99%, 90%, and 80%). The sectioned tissues were scanned with a confocal microscope (LSM 510 META; Carl Zeisis). After imaging, mean pixel intensity was determined by a Java-based version of NIH image software (ImageJ).
Real-time PCR was performed on liver DNA to quantify vector DNA using primers for eGFP (eGFP F 5′-GGTGT TCTGCTGGTAGTGG and eGFP R 5′-CCCTGAAGTTC ATCTGCACC) and mouse β-actin (β-actin F 5′-AGAGGG AAATCGTGCGTGAC-3′ and β-actin R 5′-CAATAGTGA TGACCTGGCCGT-3′). Plasmid DNA corresponding to 0.01 copy to 10 copies of the eGFP transgene (in 500 ng genomic DNA) was used in a standard curve. To determine the viral copy number, the ΔΔCt values of samples were compared to the standard curve.
Statistical analysis
Data analysis was performed with GraphPad Prism5 (GraphPad Software, Inc.). Multiple comparisons were performed using one-way ANOVA with Tukey's multiple comparison test. Comparison between two data sets used a homoscedastic t-test, including antibody titers in Fig. 1C, comparison of GFP expression in Fig. 2, and sex-dependent GAA activity and glycogen content in Fig. 6. Survival curves were compared with a log-rank (Mantel–Cox) test. The statistical significance of comparisons was indicated as follows: *p≤0.05; **p≤0.01, or ***p≤0.001.
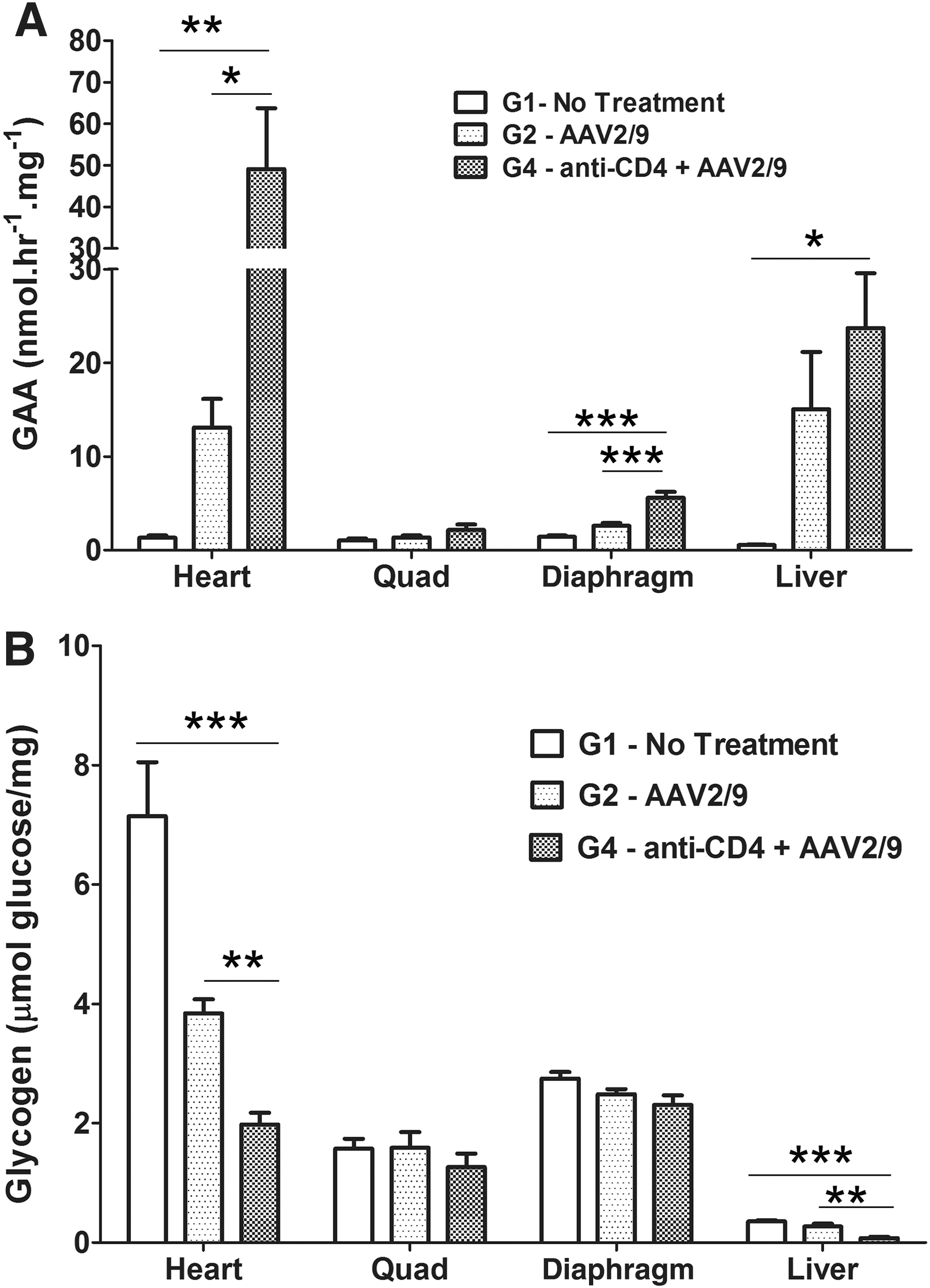
Anti-CD4 mAb enhanced biochemical correction with AAV2/9-CBhGAApA in GAA-KO mice. GAA-KO mice were treated with AAV2/9-CBhGAApA (+) anti-CD4 (3 times; n=6) or without (−) anti-CD4 (n=11) pretreatment, corresponding to groups G2 and G4, respectively. The untreated (G1) group was used for a negative control. At week 14 or 24 following injection, mice were euthanized for tissue analysis.
Results
Short-term anti-CD4 mAb therapy suppressed anti-GAA in response to an immunogenic GAA expression vector
In previous studies in autoimmune disease models with rodents and nonhuman primates, 31,32 immune tolerance was induced by the pretreatment with three doses of anti-CD4 mAb. We also found that the induction of anti-GAA IgG1 responses assessed at 4 weeks after injection of rhGAA in Pompe animals was prevented by administration of a nonlytic anti-CD4 antibody given prior to ERT. 24 Given this effect of anti-CD4 to prevent immune responses, we elected to evaluate anti-CD4 mAb therapy to establish tolerance in the context of gene therapy (Fig. 1A). Therefore, we pretreated GAA-KO mice with anti-CD4 mAb before administering the immunogenic AAV vector, AAV2/9-CBhGAApA, 14 and quantified anti-GAA IgG1at 6 weeks following vector administration (Fig. 1B). Administration of AAV2/9-CBhGAApA without anti-CD4 mAb treatment resulted in high levels of anti-GAA antibodies. In contrast, mice given the vector accompanied by anti-CD4 mAb, either as a single administration (G3) or three injections (G4), demonstrated low antibody titers no different from those of antigen-naïve mice (Fig. 1B).
Sustained immune tolerance to rhGAA has increased the efficacy of gene therapy during preclinical experiments with AAV vectors in Pompe disease. 15,33 GAA-KO mice given a single pretreatment of anti-CD4 mAb were administered an immune challenge consisting of rhGAA together with adjuvant 4 weeks prior to sampling for antibody formation, and these mice maintained their state of immune tolerance (G3 in Fig. 1B). No signs of hypersensitivity were observed at the time of the rhGAA immune challenge, in contrast to the mortality that has been demonstrated in GAA-KO mice following anti-GAA antibody formation. 15 Mice treated with three injections of anti-CD4 mAb experienced 29% mortality over 12 weeks despite maintaining immune tolerance to rhGAA, although the survival curve did not differ significantly from other groups of GAA-KO mice (p=0.4). Mortality was equivalent to that observed in untreated GAA-KO mice at 12 weeks (Fig. 1C). The cause of mortality was not ascertained; however, given the demonstrated lack of toxicity from anti-CD4 mAb administration, it was attributed to the frequency of handling and injection of these rather fragile mice.
Antibody formation against GAA following administration of AAV2/9-CBhGAApA alone was high titer (≥10 μg/ml serum) and comprised of IgG1, IgG2b, and IgG2c, reflecting T helper (Th)2-dependent responses at the 12-week time point (Fig. 1D). The suppression of anti-GAA IgG1 and IgG2b was maintained with small variations in titers at the 24 weeks in response to anti-CD4 mAb administration (Supplementary Fig. S1; Supplementary Data are available online at
Immunological tolerance following therapy with anti-CD4 enhances biochemical correction in the heart and skeletal muscles
To evaluate the effect of anti-CD4 mAb treatment upon biochemical correction from AAV2/9-CBhGAApA, GAA activity and glycogen quantification were performed following administration of three doses of anti-CD4 mAb with AAV2/9 (G4 as shown in Fig. 1A). GAA activity was significantly increased in heart (p<0.05) by anti-CD4 mAb administration, in comparison with vector alone (Fig. 2A). Similarly, GAA activity increased following anti-CD4 mAb treatment in the diaphragm (p<0.001) and liver (p<0.05). Glycogen content was significantly reduced in the heart and liver following anti-CD4 mAb administration, in comparison with vector alone (p<0.01, Fig. 2B). Glycogen content was slightly decreased in the diaphragm and quadriceps without achieving statistical significance.
Next, we evaluated the effect of a single dose of anti-CD4 mAb prior to AAV2/9-CBhGAApA upon immune tolerance to rhGAA by performing an immune challenge with rhGAA (ERT). GAA-KO mice were given a single injection of anti-CD4 mAb 1 day prior to vector injection (G3 in Fig. 1), and subsequently mice were treated with a single injection of rhGAA with adjuvant as an immune challenge at 10 weeks following vector administration (Fig. 3). Anti-CD4 mAb suppressed antibody responses to administrated rhGAA, because anti-GAA IgG1 was not significantly elevated following the immune challenge in the anti-CD4 mAb-treated group (Fig. 3A insert). Anti-GAA IgG1 was significantly reduced in untreated control mice, in comparison with mice that received rhGAA (ERT) alone (Fig. 3A insert). The effect of vector administration in the setting of immune tolerance was apparent, because GAA activity was markedly increased in heart (p<0.01), diaphragm (p<0.01), quadriceps (p<0.05), and liver (p<0.05) of GAA-KO mice by the combination of anti-CD4 and vector (Fig. 3A). The effect of ERT alone was underestimated by quantifying GAA activity 4 weeks following rhGAA administration, because rhGAA has a short half-life. 34 Glycogen accumulation was reduced in heart (p<0.001), quadriceps (p<0.05), and liver (p<0.05) following anti-CD4 and vector administration, which correlated with increased GAA activity in those tissues (Fig. 3B).

A single injection of anti-CD4 achieved biochemical correction from AAV2/9-CBhGAApA in GAA-KO mice. GAA-KO mice were administrated a single injection of anti-CD4 1 day before vector administration, and then the mice were treated rhGAA+adjuvant at week 10 following the vector injection. The mice were euthanized at week 14.
Sex-dependent different GAA activity in liver
Intriguingly, GAA activity in liver was significantly higher in male mice than in females (Fig. 4A). GAA activity was slightly elevated in the heart of male mice treated with vector alone (p<0.05), in comparison with females, and trended higher in males treated with vector, anti-CD4 mAb, and rhGAA (p=0.08) (Fig. 4B). The increase of GAA activity in males, in comparison with females, did not correlate with reduced glycogen accumulation in the liver of male mice (Fig. 4C). We understand the lack of an inverse correlation between higher GAA activity and lower glycogen content in the liver, because most glycogen in the liver is cytoplasmic and not localized to the lysosomes. 35 The effect of anti-CD4 mAb was greater in males, because the glycogen content of the heart of male mice was lower, in comparison with female mice, for mice treated with vector, anti-CD4, and rhGAA (p<0.05; Fig. 4D). Apparently, heart GAA was not sufficiently elevated in males treated with vector only to further lower the heart's glycogen content, in comparison with females. Formation of antibodies against GAA was slightly higher in females than in males, although this increase did not reach statistical significance (Supplementary Fig. S2A). No difference in the formation of anti-AAV9 antibodies based upon the sex of the mice was observed (Supplementary Fig. S2B).

Higher GAA expression in the liver for male mice. Biochemical correction was analyzed for male mice, in comparison with female mice. GAA activity for
Anti-CD4 prior to AAV2/9 administration enhanced subsequent transduction with AAV2/8
Immune responses against AAV capsids present a serious hurdle to gene therapy in Pompe disease, given the potential need to readminister an AAV vector to maintain efficacy. 36 –38 To evaluate the effect of anti-CD4 mAb treatment upon AAV vector readministration, GAA-KO mice initially were treated with anti-CD4 mAb and AAV2/9-CBhGAApA (G4; Fig. 1A) prior to injection of an AAV2/8 vector (AAV2/8-LSPGFP) encoding green fluorescence protein (GFP) at week 20, and were euthanized at week 24. Pretreatment with anti-CD4 mAb increased the measurable transduction of liver cells with GFP (Fig. 5A), which correlated with a significantly higher signal for fluorescence in liver by approximately 5-fold (p<0.05), in comparison with the group of mice that did not receive anti-CD4 (Fig. 5B). Pretreatment of anti-CD4 mAb significantly increased transduction as demonstrated by the 6-fold increased vector genome copy number in the liver (p<0.01; Fig. 5C). Thus, suppression of immune responses with anti-CD4 mAb enhanced transduction efficiency from AAV vector readministration.
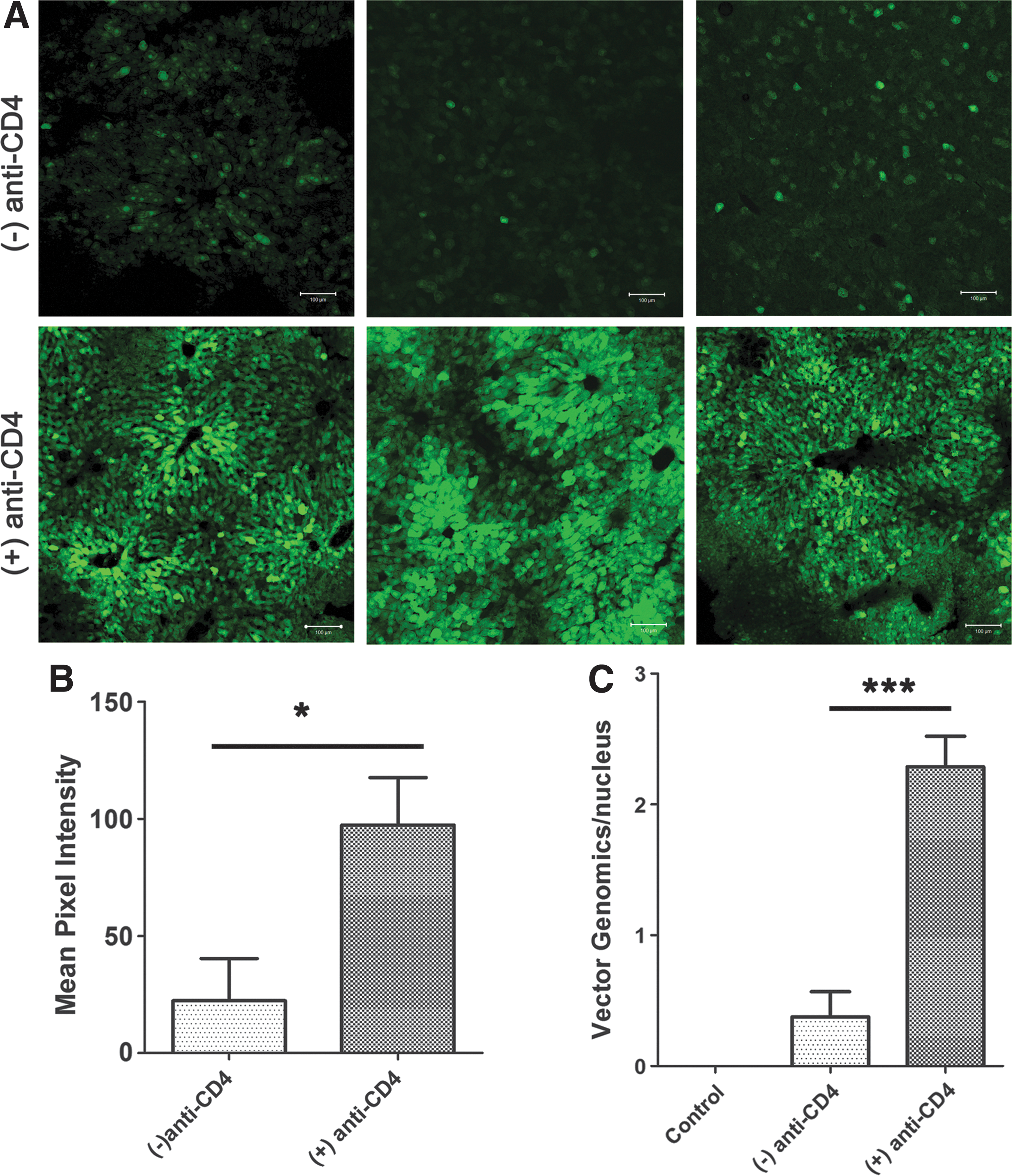
Effect of anti-CD4 upon AAV vector readministration. GAA-KO mice were treated with AAV2/9-CBhGAApA with (+) anti-CD4 (3 times) or without (−) anti-CD4 pretreatment. At week 20, mice were injected with AAV2/8-LSPGFP (n=6 in each group), and euthanized at week 24. Liver was frozen and sectioned to detect GFP expression using confocal microscopy. Images from three different animals in each group are shown
Anti-CD4 mAb suppresses cross-reacting anticapsid antibody formation
To evaluate the induction of immune tolerance by anti-CD4 on anticapsid responses, we analyzed anticapsid antibodies for GAA-KO mice shown in Fig. 5. These mice initially received the AAV2/9 vector encoding GAA, with or without anti-CD4 mAb. As expected, anti-AAV9 antibodies were provoked by AAV2/9 vector administration (Fig. 6A). However, the anti-AAV9 IgG response was significantly reduced by administration of anti-CD4 mAb treatment, although it was still elevated in comparison with untreated mice (p<0.05; Fig. 6A). Somewhat surprisingly, anti-AAV8 IgG levels were significantly elevated following administration of AAV2/9 without anti-CD4, in comparison with untreated GAA-KO mice (p<0.05; Fig. 6B), indicating a high degree of antibody cross reactivity between the serotypes. The latter result explained why pretreatment with anti-CD4 mAb at the time of AAV2/9 administration increased subsequent transduction with AAV2/8, as shown in Fig. 5. The presence of cross-reacting anti-AAV IgG antibodies against AAV2/8 was prevented by anti-CD4 administration (Fig. 6B), and anti-AAV formation correlated inversely with AAV2/8-LSPGFP transduction in the liver (Fig. 5A). Anti-AAV9 titers persisted for the duration of the observation period (Fig. 6C). Moreover, anti-AAV8 increased dramatically following the administration of the AAV2/8 vector at week 20, confirming that immune suppression from anti-CD4 mAb was only transient, and the mice remained immunocompetent to react against a further immune challenge (Fig. 6D).

Suppression of cross-reacting anticapsid antibodies by anti-CD4. GAA-KO mice were injected with AAV2/9-CBhGAApA (+) anti-CD4 (3 times; n=6) or without (−) anti-CD4 (n=6) pretreatment. Blood was sampled for ELISA quantification of anti-AAV9 or anti-AAV8 IgG at week 12. Following the injection of AAV2/8-LSPGFPpA at week 20, blood was sampled again at week 24.
Discussion
Multiple studies with AAV vectors encoding GAA have previously treated GAA-KO mice successfully. 14,27,35,39,40 However, antibody formation remains a major obstacle for GAA gene transfer approaches in which constitutive—versus tissue-specific—expression of the therapeutic transgene is utilized to achieve disease correction. 14,35,41 Despite the correlation between anti-GAA antibody formation and poor outcomes, experiments with AAV vectors containing constitutively active regulatory cassettes have not directly implicated the immune response as opposed to other potential limitations. For example, previous studies compared a vector containing a tissue-specific regulatory cassette with another vector containing a constitutively active regulatory cassette, 14,35 and the latter cassette might simply be less active or might become inactivated in vivo. Our current study has identified immune responses as the cause for poor responses to a vector containing a constitutively active transgene, because blocking the activation of CD4+ lymphocytes markedly increased the efficacy of the same vector.
ERT with rhGAA has prolonged ventilator-free survival and muscle strength in patients with Pompe disease. However, approximately 35–40% of patients with classic infantile Pompe disease treated with ERT develop high, sustained antibody titers, 1 which abrogated the efficacy of ERT. 15,16,33,42 –45 We and others previously demonstrated that liver-restricted expression of GAA could induce immune tolerance via induction of CD4+CD25+ Treg cells, 16,42,45 –47 and speculated that these antigen-specific Treg cells might suppress the activation of B lymphocytes by CD4+ helper T cells. This scenario in particular applies for those gene therapy applications, such as Pompe disease, in which muscle is as a target for transduction, 35,48 known to be more immunogenic tissue in comparison with liver. 49,37 Here we sought to determine whether a nondepleting anti-CD4 mAb would prevent the antibody response to the transgene in mice with Pompe disease injected with an immunogenic AAV vector expressing the GAA transgene under the transcriptional control of a constitutive promoter. The immunogenic AAV vector was delivered intravenously, either with or without simultaneous anti-CD4 mAb treatment. The effect of anti-CD4 mAb was demonstrated by the lack of anti-GAA antibody formation 6 weeks following vector administration (Fig. 1B), whereas mice treated with the vector alone consistently generated anti-GAA antibodies. A single injection of anti-CD4 could clearly block the formation of anti-GAA induced by the injection of AAV2/9-CBhGAApA.
The administration of AAV2/9-CBhGAApA induced the formation of diverse IgG subclasses against GAA, including anti-GAA IgG1a, IgG2b, and IgG2c, which were markedly reduced by the injection of anti-CD4 mAb. CD4+ T cells produce proinflammatory factors, including interferon-gamma (IFN-γ), and elevations of the IgG2b subclass correlated with tissue inflammation. 18,50 Here we observed the suppression of IgG2b formation by pretreatment with anti-CD4 mAb; although the precise role of each IgG subclass of immune response remained to be studied, the therapeutic effect of anti-CD4 mAb appeared to last for more than 24 weeks (Supplementary Fig. S2). According to a previous report, 51 the induced antibodies could interfere with the efficacy of ERT by inhibition of rhGAA uptake in the tissues. We previously reported sustained immune tolerance to rhGAA in the context of liver-specific expression of GAA using AAV2/8-LSPGAApA, 47 which had a very similar beneficial effect to the current strategy of anti-CD4 mAb pretreatment and ubiquitous expression of GAA with AAV2/9-CBhGAApA. In the current study, we also evaluated the increase of GAA activity in heart and skeletal muscles using a ubiquitously expressing AAV vector with immune suppression by anti-CD4 mAb antibodies (Fig. 2A). Thus, the prevention of anti-GAA formation by any method might enhance the efficacy of GAA activity in heart and skeletal muscles, regardless of enzyme sources either transgene-mediated from gene therapy or from ERT.
Patients with two deleterious GAA mutations who are completely unable to form native enzyme are cross-reactive immunological material (CRIM)-negative; patients with presence of some residual, functioning, or nonfunctioning enzyme are CRIM-positive. 1 The administered rhGAA represents a neo-antigen to infantile-onset Pompe patients, including both CRIM-negative and a significant fraction of CRIM-positive infants who form high, sustained anti-GAA antibodies during ERT. 43
In a previous study, we demonstrated that an AAV2/8 vector expressed much higher GAA in male GAA-KO mice, in comparison with female mice. 47 In the present study, we observed higher GAA activity in the liver of male GAA-KO mice, in comparison with female livers (Fig. 3D). However, we did not observe any difference between males and females with regard to antibody formation (Supplementary Fig. S2). Thus, the sex-dependent transgene expression with AAV vectors did not reduce the immunosuppressive effect of anti-CD4 mAb treatment.
In addition to the beneficial effect of anti-CD4 mAb therapy on transgene-mediated efficacy, we also showed enhanced transduction efficiency in the liver following administration of an AAV2/8 vector containing GFP (Fig. 5). The benefit of anti-CD4 mAb extended to readministration via reduction of cross-reacting anti-AAV9 antibodies that otherwise inhibited transduction by the AAV2/8 vector encoding GFP. Cross-reacting antibodies directed against a completely different serotype (e.g., AAV8) following administration of an AAV2/9 vector are not commonly observed in mice. 52 Conversely, cross-reacting anti-AAV antibodies in response to naturally occurring AAV infection have been well-documented. 53 Similarly, cross-reactive anti-AAV antibodies were stimulated by administration of AAV8 vectors in hemophilia B dogs 54 and in nonhuman primates, 55 and preexisting anti-AAV antibodies have been documented in large animal models. 56 In our study, we observed production of cross-reactive antibodies to AAV9 following administration of AAV8 vectors. Given the risk of stimulating cross-reacting anti-AAV in a naïve subject, we have demonstrated an additional benefit from coreceptor blockade with anti-CD4 mAb in terms of facilitating readministration with an AAV vector of a new serotype.
The mechanism for inhibiting transduction with an AAV2/8 vector encoding GFP following administration of the AAV2/9 vector encoding GAA seemed to be the presence of low-level anti-AAV8. Although neutralizing antibodies were not analyzed, it is known that binding antibodies often correlate with neutralizing antibodies and binding antibodies alone can interfere with transduction of the liver. 56 For example, even extremely low anti-AAV neutralizing antibody titers can result in vector neutralization, 57,58 and administration of an AAV2/8 vector to nonhuman primates with preexisting binding, nonneutralizing antibodies against AAV8, resulted in sequestration of the vector in the spleen, with poor transduction of the liver. 59 Therefore, the inverse correlation of liver transduction with low-level anti-AAV8 does suggest that cross-reacting anti-AAV was the likely culprit.
These results are important, as they provide one avenue to readminister the vector that does not involve the use of prolonged and intense immunosuppressive regimens; it is also an important result in the context of a systemic disease affecting children, which may require vector readministration to achieve optimal efficacy or if efficacy is lost as patients become adults. Readministration has been critical to maintaining efficacy from AAV vector-mediated gene therapy in canine glycogen storage disease 38,60 and hemophilia. 37 Previously, it has been suggested that the merely switching serotypes would achieve complete efficacy from readministering an AAV vector, which might be questioned in the future due to the effect of cross-reacting anti-AAV antibodies in the current study.
Heart involvement is the main cause of mortality in infantile Pompe disease, and high anti-GAA antibody titers strongly correlated with cardiomyopathy and mortality in that population. 1,43 Severely affected, infantile patients have a severe deficiency of GAA in association with cardiomyopathy, whereas patients with slightly higher GAA activity have late-onset Pompe disease and no cardiomyopathy. 61 The effect of the anti-CD4 mAb was important, because the biochemical correction of the heart was greatly increased in mice that did not form antibodies following anti-CD4 mAb treatment. While anti-CD4 mAb did not prevent mortality in the GAA-KO mice studied here, we would expect improved clinical outcomes if GAA deficiency could be corrected in the heart by an effective gene therapy.
At present, the control of immune responses to ERT in Pompe disease is limited to immunosuppressive agents with known toxicities, which emphasizes the need for more specific, safer immune modulation. Given this current suppression of antibody responses obtained with a short course of nondepleting anti-CD4 mAb, further preclinical development of this approach is warranted in the context of gene therapy for Pompe disease and other inherited disorders of metabolism.
Footnotes
Acknowledgments
This work was supported by Grant # 241701 from the Muscular Dystrophy Association of the United States and by a grant from Genethon. The AAV packaging plasmids were provided courtesy of Dr. James M. Wilson at the University of Pennsylvania (Philadelphia, PA). GAA-KO mice were provided courtesy of Dr. Nina Raben at the National Institute of Arthritis and Musculoskeletal and Skin Disorders. Nondepleting anti-CD4 mAb (YTS177) was provided by Tolerx, Inc. (Cambridge, MA).
Author Disclosure Statement
D.K. has received research/grant support from Genzyme Corporation. No competing financial interests exist for any of the other authors.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.