
Abstract
Clinical trials testing the effects of a single injection of adenovirus carrying the human hepatocyte growth factor gene (Ad-HGF) in patients with chronic ischemic heart failure failed to show consistent improvements in cardiac function. The aim of this study was to evaluate the efficacy of repeated injections of Ad-HGF in a rat model of postinfarct heart failure. Ad-HGF or Ad-green fluorescent protein (GFP) was administered to Sprague Dawley rat models of postinfarct heart failure via single or fractional repeated intrapericardial injection. Heart function was monitored by magnetic resonance imaging for 4 and 8 weeks after injections. The expression of HGF or factor VIII/Ki-67 was evaluated by Western blot assay or immunofluorescence. We found that Ad-HGF gene expression could be prolonged in vivo by repeated injections and that cardiac function was significantly improved in the Ad-HGF repeat-injection group compared with the Ad-HGF single-injection group. Newly formed capillary density was similarly higher in the Ad-HGF repeat-injection group compared with that in the Ad-HGF single-injection group. We therefore conclude that fractional repeated injections of Ad-HGF may represent a promising therapeutic strategy to improve cardiac function in the setting of postinfarct heart failure.
Introduction
N
In April 2005, we carried out a phase 1 clinical trial approved by the Chinese State Food and Drug Administration to test the safety of administering Ad-HGF to patients with clinically significant coronary artery disease. 8,9 A subsequent phase 2 trial to evaluate the efficacy of Ad-HGF, however, yielded results that were inconsistent with what was expected. Specifically, cardiac function in 9 of 12 patients showed improvement over the short term, but only three patients sustained gains for more than a year and a half and none of the 12 patients showed continuous improvement. A likely explanation for the outcome was the short half-life of the adenoviral vector, which survived only about 14 days in vivo before being cleared by the immune system. We therefore began to explore the idea of repeated Ad-HGF injections. We found that fewer than seven repeated intramuscular injections of the adenovirus in a rat model did not increase autoantibody production, but more than seven injections led to increased serum antibody titers that persisted for 13–14 weeks before returning to baseline levels. 10 In light of the above-described results, we imagined that repeated injections of Ad-HGF may yield continuous improvements in cardiac function in models of postinfarct heart failure.
Materials and Methods
Construction of adenoviral vector
Adenoviral vectors constructed for previous experiments were used in this study. 11 HGF cDNA was amplified by polymerase chain reaction, using human placenta cDNA library as a template. Replication-deficient (E1, E3 deleted) adenoviral vectors carrying the human hepatocyte growth factor gene (Ad-HGF) were constructed with the pAdEasy-1 system (Stratagene, La Jolla, CA), in accordance with the manufacturer's instructions. The recombinant, replication-defective adenovirus was purified by cesium chloride gradient ultracentrifugation. The final plaque-forming units (PFU) were determined by titration on HEK293 cells under an agarose overlay. Adenoviral vectors carrying the gene encoding green fluorescent protein (Ad-GFP) were constructed similarly.
Postinfarct heart failure model preparation and grouping
All animal experiments were performed in accordance with the Guide for the Care and Use of Laboratory Animals (National Research Council of the National Academies; revised 1996) and approved by the Animal Care and Use Committee of Nanjing Medical University (Nanjing, China). The animal protocol was approved by the Ethics Review of Lab Animal Use Application of Nanjing Medical University (Permit No., NJMU-ERLAUA-20140310). Male Sprague Dawley rats weighing approximately 200 g were anesthetized with pentobarbital sodium (50 mg/kg) via intraperitoneal injection. Animals were placed in the supine position on a heating pad and ventilated with 3.5-ml volumes at a rate of 60/min (Harvard Apparatus, Holliston, MA). A thoracotomy was performed and the myocardial infarction (MI) model was created by ligating the left descending coronary artery. Infarctions were confirmed by the increase or decrease of the ST segment through electrocardiography (PowerLab Chart 7 software; AD Instruments, Colorado Springs, CO). Four weeks after MI, magnetic resonance imaging (MRI) was performed to evaluate cardiac function. A left ventricle ejection fraction (LVEF) equal to or less than 40% indicated successful preparation of the postinfarct heart failure model. According to the LVEF, rats were divided into four groups (n = 8 for each group): group a, the Ad-HGF repeat-injection group; group b, the Ad-HGF single-injection group; group c, the null-Ad group; and group d, the saline group. In addition, eight postinfarct heart failure rats were included in the Ad-GFP group. At the end of the experiments, rats were anesthetized with pentobarbital sodium (50 mg/kg) via intraperitoneal injection and sacrificed by carbon dioxide (CO2) suffocation.
Injection of Ad-HGF and Ad-GFP in vivo
Intrapericardial injections were performed through a small incision in the abdominal wall below the xyphoid appendix, via a transdiaphragmatic approach as reported previously. 12 Four weeks after MI, the first intrapericardial injection was performed in all groups: null-Ad group (null-Ad, 100 μl), saline group (saline, 100 μl), Ad-HGF single-injection group (Ad-HGF at 1 × 109 PFU/ml, 100 μl), Ad-HGF repeat-injection group (Ad-HGF at 5 × 108 PFU/ml, 100 μl), and Ad-GFP group (Ad-GFP at 5 × 108 PFU/ml, 100 μl). Eight weeks after MI, the second intrapericardial injection was performed: null-Ad group (null-Ad, 100 μl), saline group (saline, 100 μl), Ad-HGF single-injection group (saline, 100 μl), Ad-HGF repeat-injection group (5 × 108 PFU/ml Ad-HGF, 100 μl), and Ad-GFP group (Ad-HGF at 1 × 109 PFU/ml).
Observation of GFP expression in vivo
After the first intrapericardial injection, one rat was sacrificed every 7 days in the Ad-GFP group. The hearts were harvested, frozen, and sectioned serially and subjected to laser scanning confocal microscopy (Zeiss LSM 710; Carl Zeiss Microscopy, Jena, Germany). The green fluorescence intensity was quantified with Image-Pro Plus image analysis software (Media Cybernetics, Bethesda, MD). Light intensity from the section was measured by integrated optical density (IOD). The observer was blinded to grouping information.
MRI
Four, 8, and 12 weeks after MI, rats were anesthetized with pentobarbital sodium (50 mg/kg) via intraperitoneal injection. Animals were placed in the supine position in a microcoil and their heart rate was monitored (approximately 180–200 beats/min). MRI was performed to study cardiac functional parameters. Cardiac cine imaging was performed with a 3T scanner (MAGNETOM Verio; Siemens Healthcare, Erlangen, Germany). A retrospective ECG-gated Flash-based segmented cine protocol was performed. Detailed protocol parameters are as follows: slice thickness of 2.5 mm with distance factor of 10%; field of view, 154 × 53 mm; TR of 68.2 msec and TE of 3.24 msec with a flip angle of 15 degrees; calculated phases, 50; and number of averages, 4. Coverage of the left ventricle was provided in left ventricular short-axis orientation. The end of the systolic and diastolic phases was determined by previewing images at the level of the left mid-ventricle. Slices were considered part of the LV volume and included in volumetric calculations when at least 50% of the circumference (≥180°) was myocardium. Manual contour detection of the left ventricular endomyocardial borders was performed carefully by a radiologist with 10 years of experience in cardiac imaging, and he/she was blinded to grouping. Borders were detected through the whole left ventricle. End-diastolic volume (EDV) and end-systolic volume (ESV) were calculated automatically by software. Stroke volume (SV) was calculated as EDV minus ESV, and ejection fraction (EF) was calculated as SV divided by EDV (Fig. 1).
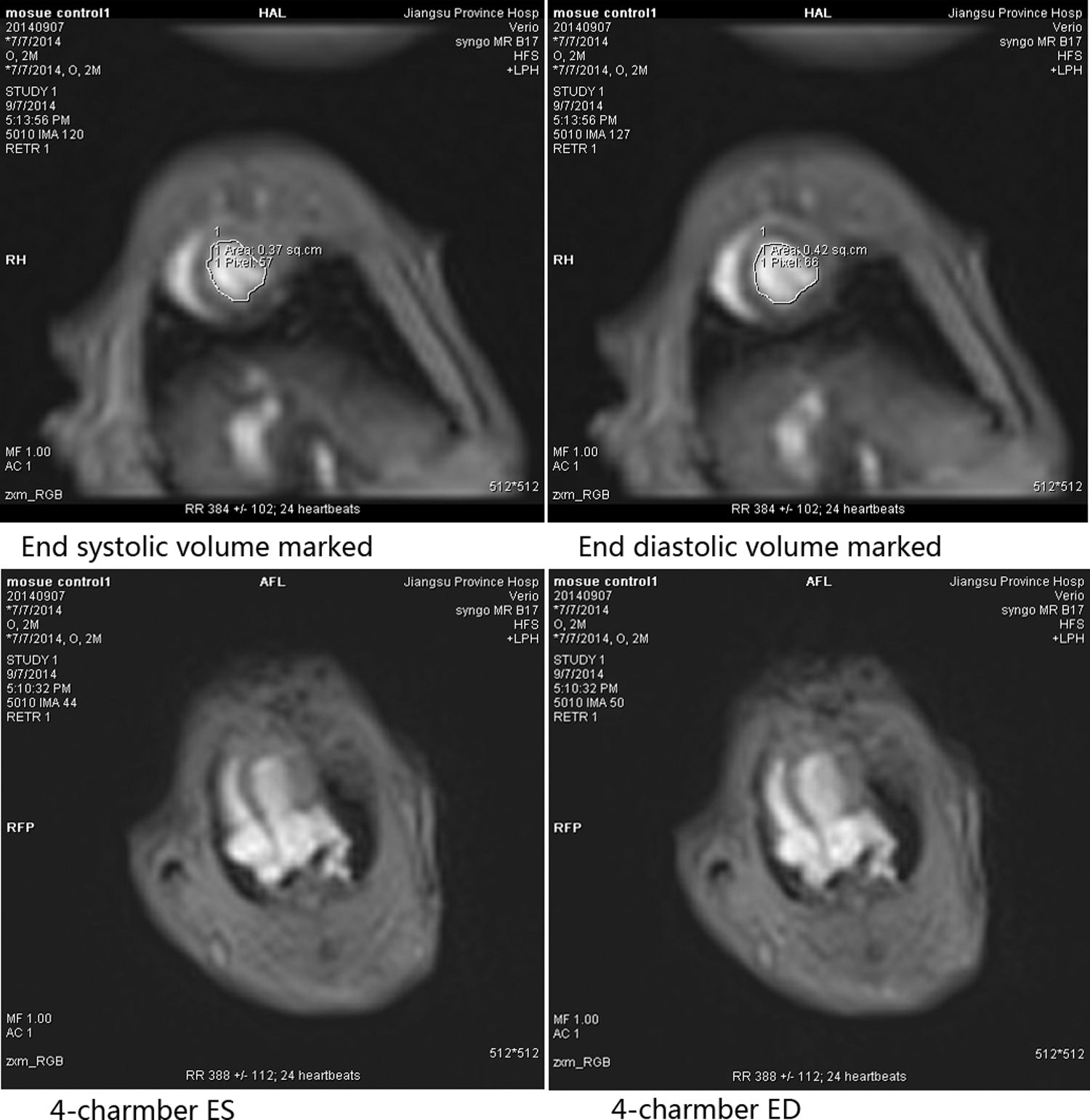
Measurement of rat cardiac chamber parameters.
Western blotting analysis
Technical details of Western blotting analysis have been described previously. 13 HGF, β-actin, and the secondary goat anti-mouse IgG–AP (alkaline phosphatase) antibody (Santa Cruz Biotechnology, Santa Cruz, CA) were used in this study. The observer was blinded to treatment information.
Immunohistochemical analysis
Twelve weeks after MI, the myocardial samples collected from all animals were fixed in 4% formaldehyde, embedded in paraffin, and then cut into 10-μm-thick sections. To detect neoangiogenesis in the periinfarct area, double staining with anti-factor VIII antibody and anti-Ki-67 antibody (Santa Cruz Biotechnology) was observed by immunofluorescence. Nuclei were stained with 4′,6-diamino-2-phenylindole (DAPI). The staining was carried out according to the manufacturer's instructions, and signals were visualized by incubating the sections with secondary antibody labeled with Alexa Fluor 488 or Alexa Fluor 555 (Molecular Probes, Eugene, OR). Sections were analyzed with a Zeiss Axio Imager fluorescence microscope at ×400 magnification (Carl Zeiss Microscopy). Tissue samples obtained from three locations within the transitional zones of each animal were identified. Factor VIII- and Ki-67-positive vessels in each tissue section were counted by an observer blinded to group assignments. The number of vessels in five high-power fields in each section were averaged, and expressed as Ki-67-positive vessels per square millimeter (the area of 400 high-power fields is equal to 0.152 mm2). The averages of five fields for three samples from each animal were used for comparison.
Statistical analysis
Data are expressed as means ± SD. The significance of differences in intragroup quantitative data comparisons was assessed by paired-sample t test. The significance of differences between groups was assessed by analysis of variance and by Student–Newman–Keuls q test. Analysis system software SPSS 19.0 was used for all analysis. A p value less than 0.05 was considered the cutoff for statistical significance.
Results
In vivo GFP expression
Four weeks after MI, the first intrapericardial injection of Ad-GFP was performed. Three rats were sacrificed and their hearts collected every 7 days after the initial injection. Serial frozen sections of rat heart were later subjected to laser scanning confocal microscopy. Green fluorescence intensity gradually weakened from day 7 to day 21, and disappeared by day 28. The second intrapericardial injection of Ad-GFP was then performed 4 weeks after the first injection. Here too, green fluorescence intensity weakened gradually from day 7 to day 14 and was lost by day 21 (Fig. 2).
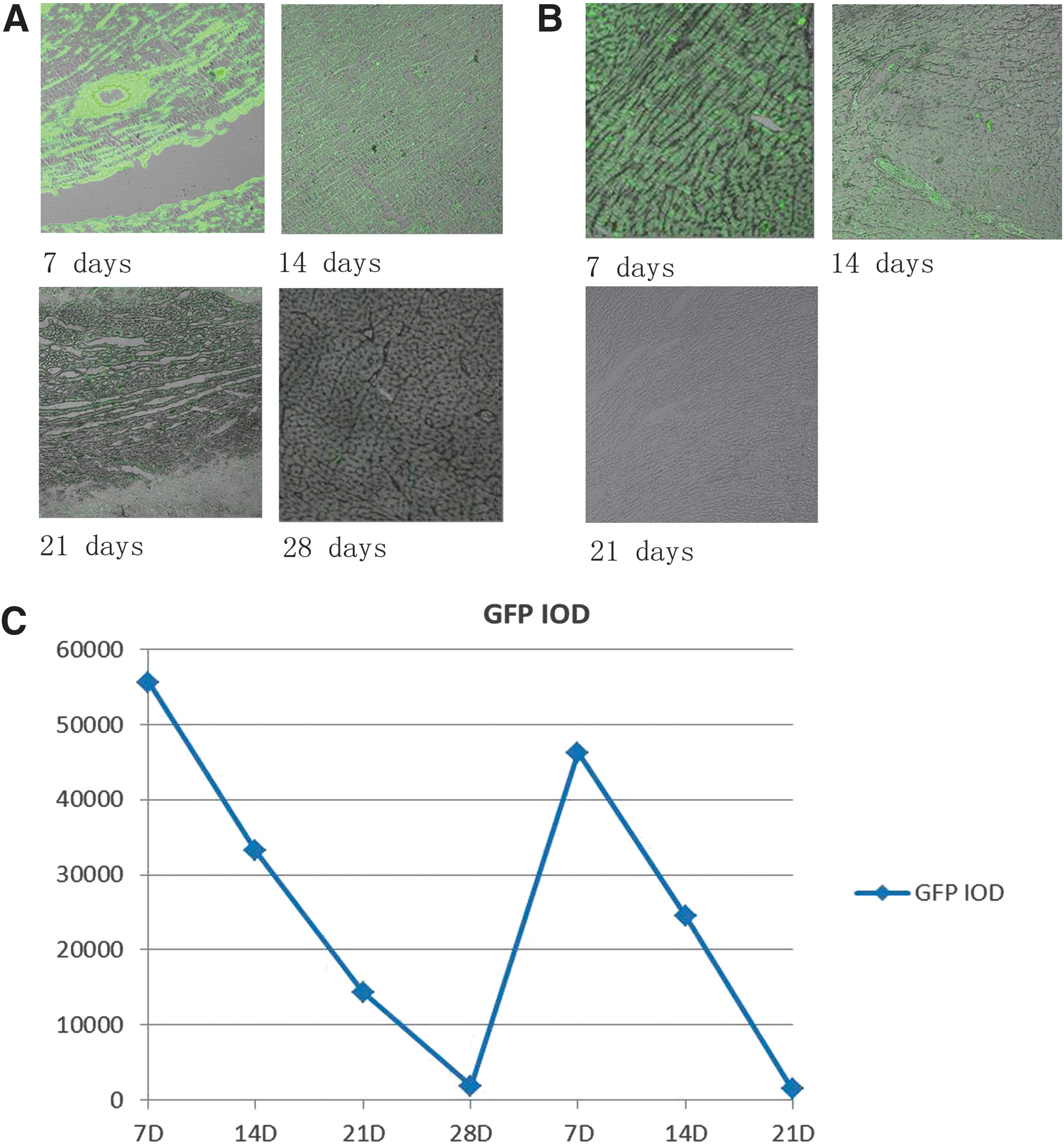
Green fluorescent protein expression in vivo.
HGF expression
To investigate whether the adenovirus could transduce HGF expression in vivo, we performed Western blots 8 weeks after the first injection. We found higher HGF expression in the periinfarct zones of Ad-HGF repeat-injection samples compared with those of the single-injection and control samples. Levels of HGF in the single-injection samples did not differ significantly from the control samples (Fig. 3A and B). These results indicated that Ad-HGF gene expression could be prolonged in vivo through repeated injections.
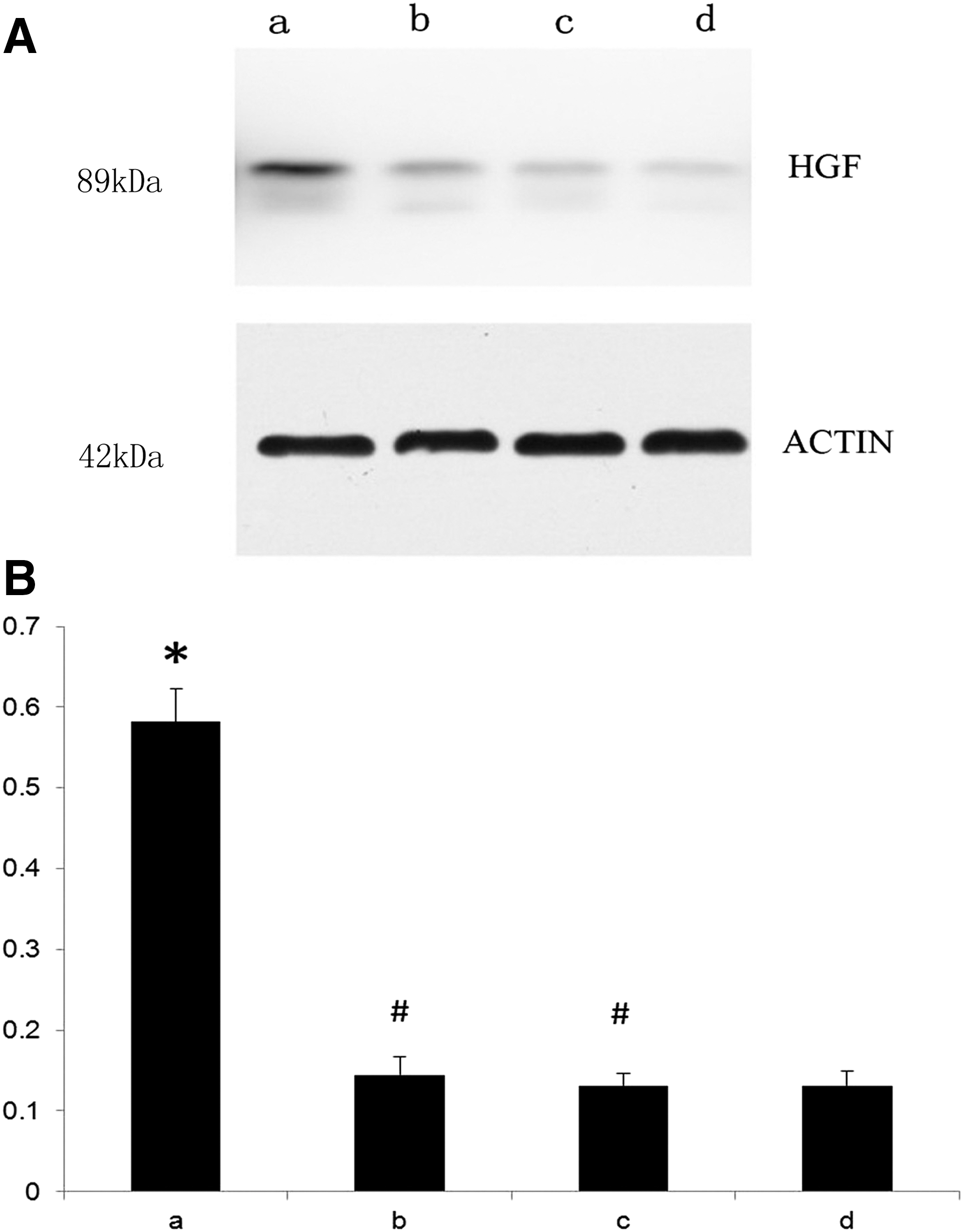
Western blot analysis of HGF expression in vivo.
Improvement of cardiac function
MRI was used to quantitate cardiac function (Fig. 4). Four weeks after MI, LVEF showed no significant difference across the four groups (p > 0.05; Table 1). Eight weeks after MI, LVEF decreased slightly in both the null-Ad and saline groups. In the therapeutic groups, LVEF improved significantly 4 weeks after gene transfer, but no significant differences were observed between the Ad-HGF single-injection group and Ad-HGF repeat-injection group (p > 0.05; Table 1). Twelve weeks after MI, LVEF improvement was greater in the Ad-HGF repeat-injection group than in the single-injection group (p < 0.05; Table 1), whereas LVEF had decreased in both the null-Ad and saline groups (p < 0.05; Table 1).
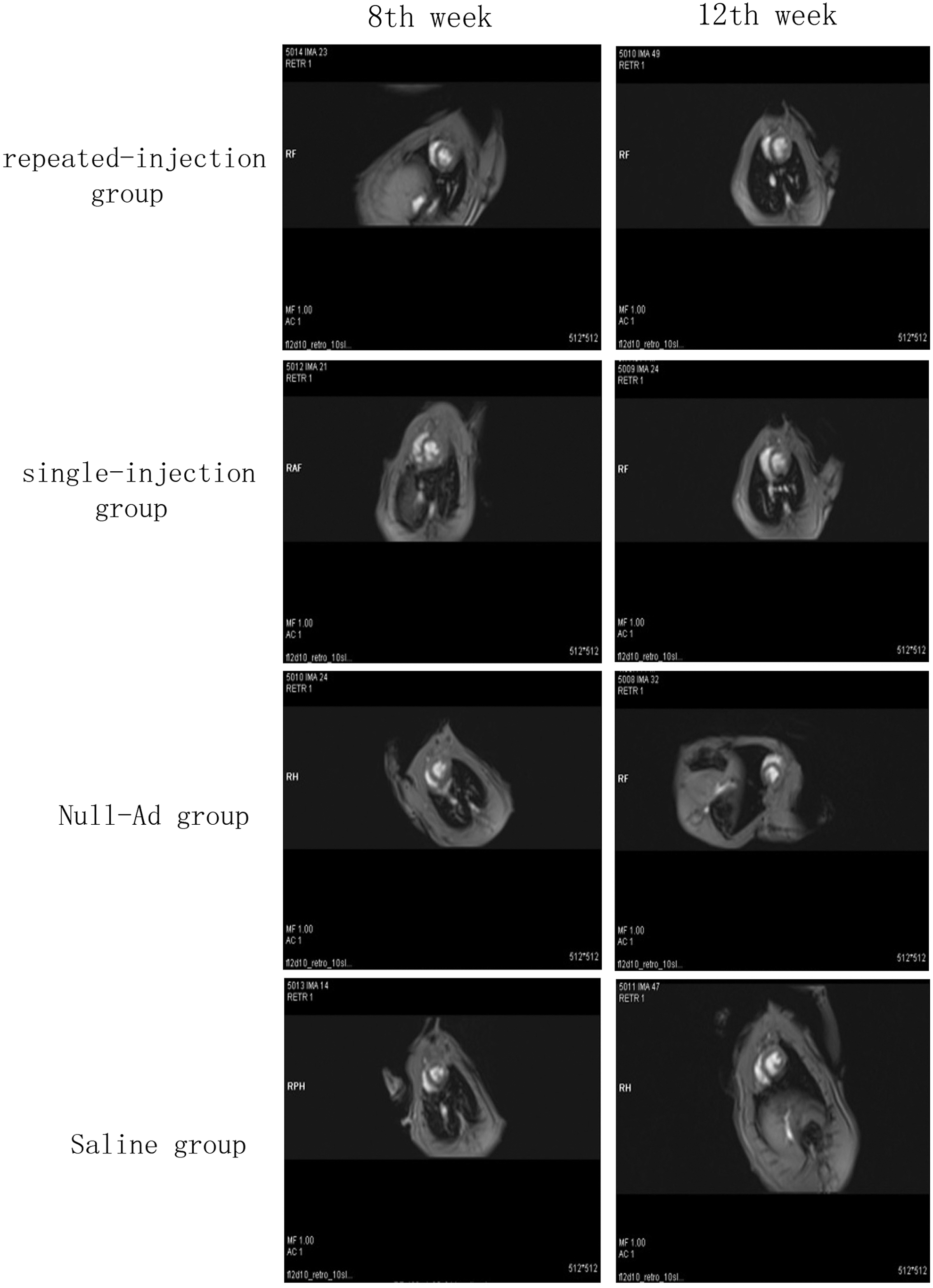
MRI analysis of cardiac functional parameters. Representative images of hearts at weeks 8 and 12, showing left ventricular parameters in all groups.
Left ventricular ejection fraction of the four groups 4, 8, and 12 weeks after myocardial infarction
p > 0.05; LVEF shows no significant difference in the four groups.
p < 0.01; LVEF in week 8 versus that in week 4.
p < 0.05; versus the single-injection group in week 12.
p > 0.05; versus the repeated-injection group in week 8.
p < 0.05; LVEF in week 12 versus LVEF in week 4 or week 8.
LVEDF, left ventricular end-diastolic volume; LVEF, left ventricular ejection fraction; LVESV, left ventricular end-systolic volume.
Angiogenesis
Antibodies against the cell proliferation marker Ki-67, and the endotheliocyte marker factor VIII, were used to determine capillary regeneration through immunofluorescence staining. As Fig. 5A shows, the expression of Ki-67-positive capillary density was increased in samples from the Ad-HGF single-injection and repeat-injection groups compared with samples from the control group (p < 0.05). No significant difference in capillary density was found between the saline and null-Ad groups (51.97 ± 6.16/mm2 vs. 54.47 ± 7.24/mm2 p > 0.05; Fig. 5B). The capillary density in the Ad-HGF repeat-injection group was higher than that in the Ad-HGF single-injection group (102.44 ± 11.94/mm2 vs. 83.88 ± 9.22/mm2, p < 0.05; Fig. 5B).
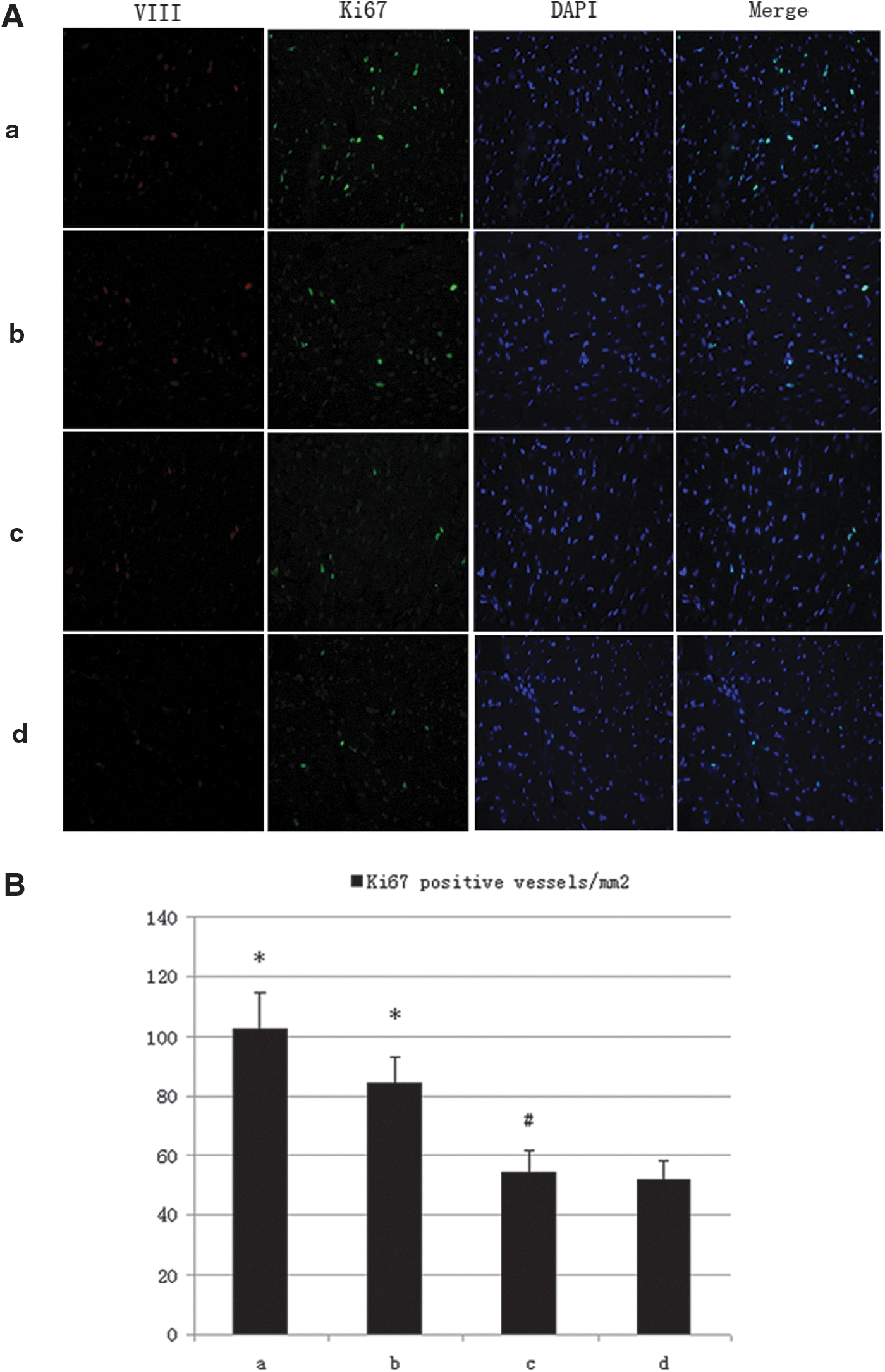
Histological observations.
Discussion
HGF, a heparin-binding glycoprotein, is a disulfide-linked heterodimeric molecule that was initially identified as a potent mitogen for hepatocytes. Because of its potential angiogenic, antiapoptotic, antifibrotic, and stem cell-recruiting effects, HGF has been the subject of increasing study in the context of cardiovascular diseases. The angiogenic properties of HGF may be mediated via upregulation of an essential transcription factor, Ets-1, which HGF regulates at the transcriptional level. Ets-1 is thought to activate HGF, matrix metalloproteinase (MMP)-1, c-Met, and vascular endothelial-derived growth factor (VEGF) expression in vascular smooth muscle cells and endothelial cells, which in turn potentiate degradation of the extracellular matrix and migration of vascular smooth muscle and endothelial cells to effect angiogenesis. 14
HGF is also a potent antiapoptotic factor, which protects cardiomyocytes from apoptosis by modulating MEK (MAPK/ERK kinase)/ERK (extracellular signal-regulated kinase)-dependent phosphorylation of GATA-4. 15 The antifibrotic effects of HGF are thought to be mediated via activation of matrix metalloproteinases, inhibition of collagen formation, and inhibition of angiotensin II-activated transforming growth factor (TGF). 16
We had previously shown that exogenous HGF could promote angiogenesis and improve postinfarction cardiac function in several animal models. 4 –7,11,17 –19 On the basis of this result, administration of Ad-HGF was approved for phase 1 and 2 clinical trials by the Chinese State Food and Drug Administration. In line with other published results, 20 we found that across 12 patients with chronic ischemic heart failure, only short-term improvements in cardiac function were seen, with improvements diminishing within 3–6 months. We hypothesized that this short-lived effect was related to the short half-life of the adenoviral vector, which persisted for only 14 days in vivo. To address this shortcoming, we generated a new-generation, helper-dependent adenoviral vector, which carried only the essential cis-acting elements. This vector had significantly attenuated cell toxicity and immunogenicity, likely due to the decrease in protein-coding function, and could therefore sustain prolonged gene expression in vivo. 21 However, given the regulatory challenges associated with clinical use of a new vector, we chose instead to explore the possibility of repeated injections of Ad-HGF.
A major limitation of the adenoviral vector system for repeated treatment of chronic genetic disease is that the vectors are highly immunogenic. Delivery of adenoviral vectors to immune-competent mice by intravenous delivery resulted in the production of neutralizing antibodies and a block to repeat administration. 22 However, there have been several reports of effective repeat administration of adenoviral vectors in immunocompetent animals by intramuscular or subcutaneous injection. 23,24 These studies demonstrated that the choice of the route of repeat administration is particularly important. Successful repeat administration of adenoviral vectors has also been observed in gene therapy for cancer. Although repeat intratumoral injections induced a serum neutralizing antibody response, that did not attenuate the therapeutic effect. 25,26 Therefore, we imagined that repeated injections of Ad-HGF could yield continuous improvements in patients with postinfarct heart failure. After the second intrapericardial injection of Ad-GFP, green fluorescence persisted for 14 days. Similarly, higher HGF expression was found in the Ad-HGF repeat-injection samples compared with the single-injection and control samples. When considering all of the data, repeated intrapericardial injections of Ad-HGF in rats may be feasible.
Ventricular remodeling with chamber dilation and wall thinning are key hallmarks of postinfarction cardiac failure. 27 In line with other studies, we found the Ad-HGF group to have preserved chamber dilation compared with the null-Ad and saline groups. 3 Four and 8 weeks after HGF transfer, ESV and EDV were lower in the Ad-HGF group compared with the null-Ad and saline groups. LVEF was significantly increased in the Ad-HGF group, indicating an improvement in systolic function. Four weeks after the first HGF transfer, no significant differences in cardiac function improvement were observed between the Ad-HGF single-injection group and the Ad-HGF repeat-injection group. However, at the same time point, that is, 8 weeks after HGF transfer in the single-injection group and 4 weeks after the second HGF transfer in the repeat-injection group, cardiac function was significantly improved in the Ad-HGF repeat-injection group compared with the Ad-HGF single-injection group. Angiogenesis plays a key role in heart function improvement with ischemic heart disease. Through double-immunofluorescence staining, we found that Ki-67-positive capillary density in the Ad-HGF repeat-injection group was higher than in the Ad-HGF single-injection group. These results indicated that Ad-HGF can effectively induce capillary regeneration and improve heart function and that Ad-HGF administered in repeated injections versus a single injection produces greater improvement.
Four weeks after the second injection, protein quantitation indicated that HGF expression was higher in the Ad-HGF repeat-injection group than in the Ad-HGF single-injection group. Improvement of cardiac function and capillary density was also clearly greater in the repeat-injection group than in the single-injection group. An equal dose of Ad-HGF administered as a single injection versus repeated injections, yielded greater improvements in heart function and angiogenesis with repeated injections. These results demonstrated that repeated injections of Ad-HGF are effective at transfecting myocardial tissue and transducing HGF protein expression. Moreover, the results suggested that the therapeutic effect of Ad-HGF on heart failure was enhanced by long periods of gene expression compared with short periods of high gene expression, necessitating either prolonged-action viral vectors or repeated injections. One concern with prolonged expression of HGF regards the risk of tumors. Fortunately, even more than seven repeated injections of Ad-HGF did not lead to tumor occurrence in our local, intramuscular model. 10 Certainly, further studies are required to assess safety before clinical translation.
The protocol for Ad-HGF gene transfer by percutaneous intramyocardial injection used in our clinical trial was amenable to repeated injections. 11 This differed from intramyocardial injections in rats, which required open-heart surgeries and increased mortality with repeated open-heart procedures. Although certain studies had suggested that intrapericardial gene transfer was restricted by the epicardial fiber layer, 12 studies specific to rat models of postinfarct heart failure had demonstrated that the epicardial layer did not influence the effect of transfection. We therefore regarded the intrapericardial injection method as safe and reliable.
When considered altogether, our results suggest that repeated injection of Ad-HGF into rats may be feasible and should be the basis for further study in large mammals.
Limitation
In this study, we observed that the cardiac function of rats had not attenuated by 8 weeks after a single injection of Ad-HGF, which was inconsistent with observations in the clinical trial. One possible explanation is that the cardiac function of rats had not begun to attenuate during the short observation period (only 8 weeks); another possible explanation concerns differences between rats and humans in the process of healing from heart failure. Therefore, the results of repeated administration of Ad-HGF in rats cannot be directly extrapolated to humans, and further research in large mammals must be carried out.
Footnotes
Acknowledgments
This work was supported by grants from the National Natural Science Foundation of China (No. 81270255), the Open Research Fund of State Key Laboratory of Bioelectronics, Southeast University (No. 2013-1-H3), the Project Funded by the Science and Technological Innovation Group of Jiangsu Higher Education Institution “Qing-Lan Project”(JX2161015030), the Natural Science of Jiangsu Province Youth Fund (BK20141020), and the Priority Academic Program Development of Jiangsu Higher Education Institutions (PAPD).
Author Disclosure
The authors declare no conflict of interests.