
Abstract
Detection of exogenous p53 gene and target gene expression in cervical cancer cell lines SiHa and C33A infected by recombinant adenovirus-p53 (rAd-p53) in vitro. The rAd-p53 infection evidently increased the expression of exogenous p53 gene, p21 gene, and Bax gene. The radiosensitization rates of rAd-p53 were 1.19 in SiHa and 1.18 in C33A in vitro. To evaluate the effect and safety of rAd-p53 transfer combined with radiotherapy (RT) in patients with cervical cancer, rAd-p53 transfer combined with radiotherapy (group PRT) in 69 patients with cervical cancer was compared with a control group treated with radiotherapy alone (group RT) in 35 patients with cervical cancer. Patients were intratumorally injected with rAd-p53 (1 × 1012 virus particles) once a week for 6 weeks. Concurrent pelvic RT plus brachytherapy to take point A to 76.0 Gray units (Gy) (range 75–80 Gy). The 5-year overall survival rate of the PRT group was 17.5% higher than that of the RT group (HR = 0.551, 95% CI 0.278–1.095, p = 0.084). The 5-year progress-free survival rate of the PRT group was 17.1% higher than that of the RT group (HR = 0.485, 95% CI 0.234–1.006, p = 0.047). rAd-p53 administration did not increase the adverse events caused by radiotherapy, except for transient fever after rAd-p53 administration. rAd-p53 was safe and biologically active in improving radiotherapeutic survival rates in patients with cervical cancer.
Introduction
T
Irradiation kills tumor cell via a way inducing cell cycle arrest and apoptosis. Wild-type p53 gene promotes this response. Mutation p53 gene abrogates this response and increases intrinsic radio-resistance of tumor cell. 1 Recombinant adenovirus (rAd)-p53 transfer can increase tumor radio-sensitivity both in vitro and in vivo for all tumor cell lines. 2
First, clinical trial phases 1–4 of rAd-p53 were carried out in qualified patients with nasopharyngeal carcinoma in China. The randomized control clinical trial demonstrated that the rAd-p53 in combination with radiotherapy (PRT) increased the 5-year locoregional tumor control rate by 25.3% compared with radiotherapy alone (RT) (p = 0.002). The 5-year overall and 5-year progress-free survival rates of the PRT group were 7.5% higher (p = 0.34) and 11.7% higher (p = 0.21), respectively, than that of the RT group. Result of 6-year follow-up of recombinant adenovirus-p53 was published in the Journal of Clinical Oncology (2009;5:799–804). 3
The first commercial rAd-p53 drug, Gendicine®—an E1 substituted, replication-incompetent recombinant adenovirus encoding the human p53 gene—was approved to market in October 2003 and was formally launched in April 2004 by the China Food and Drug Administration. Gendicine® is the world's first rAd-p53–based gene therapy product approved by a government agency for clinical use. From then, off-label use of Gendicine® has been tested in phase 1–4 clinical trials for the treatment of thousands of patients with various cancers including of lung cancer, liver cancer, pancreas cancer, cervical cancer, etc. in China. 4
Cervical cancer is the second common malignant disease for women worldwide, with over 500,000 new cases diagnosed annually and a 50% mortality rate in Asia. 5
Cervical cancer is strongly linked to infection by human papillomavirus (HPV), which together cause virtually all cervical cancer. 6 –8 HPV oncoproteins E6 and E7 catalyze degradation and neutralize the function of the tumor suppressor gene p53. E6 and mutation of p53 cooperatively induce cervical cancer. 9 A mutation in the p53 gene occurs in 30% to 60% of patients with cervical cancer, which induce refractoriness to radiotherapy. For patients with cervical cancer, the local recurrence rate is 20% to 35%. The distant metastasis rate is 10% to 30%. P53 gene mutation significantly correlated with poor survival of cervical cancer. 10 –15
Meta-analysis of 22 clinical trials involving 3,837 patients with advanced cervical cancer showed no statistical significance difference by adding chemotherapy along with radiotherapy. 16 Another meta-analysis in randomized trials 17 and Chinese data 18 also showed that concurrent chemotherapy and radiotherapy was not able to improve the survival rate of patients with cervical cancer over that of radiotherapy alone. Our retrospective analysis was performed on 101 cases, consisting of 61 cases of cisplatin-based chemotherapy combined with radiotherapy (CRT group) and 40 cases of radiotherapy alone (RT group) for stages 2B and 3B cervical cancer treated in our hospital from the year 2001 to 2007. The 3-year overall survival rate of the CRT group and RT group were 64.8% and 67.8%, respectively, and 3-year progress-free survival rate of the CRT group and RT group were 57.2% and 58.6%, respectively (p > 0.05). It is known that overall survival and progress-free survival of CRT was slightly lower than that of RT, but not significantly different (unpublished data).
Especially in China, most of patients with cervical cancer come from economically poor countryside, with inadequate public health coverage; the sanitary conditions were significantly worse than that for women in the United States and Europe. For them, long-term colporrhagia before cervical cancer often led to low a hemoglobin (Hb) condition. As such, these patients simply cannot tolerate the treatment of radiotherapy plus chemotherapy. Study data for another developing country—India—also showed that improvement in outcome with the addition of cisplatin along with RT. 19 So radiotherapy alone still remains a valid option.
A composite analysis of global data showed that the 5-year overall survival rate for International Federation of Gynecology and Obstetrics (FIGO) stage 2 and 3 patients (98,439 patients) treated by radiotherapy alone was 49.3%. 20 Improvement for such cervical cancer treatment method is needed.
Some studies also demonstrated that rAd-p53 transfer promotes inhibition of cervical cancer cell growth in vitro and remarkably decreasing of the size of tumor in vivo. The combination of rAd-p53 infection with radiation or cytotoxic agents increases the inhibition of growth of cervical cancer cells than any treatment alone in vitro. 21 –23 and provided direct support to conduct clinical trials using rAd-p53 in combination with radiation for patients with cervical cancer.
Recombinant adenovirus-p53 acts as a universal radiosensitizer in the treatment of cancer, so it is also applicable to intratumoral injection of rAd-p53 for cervical cancer and may be expected to increase the effectiveness of RT for cervical cancer. From March 2001 through March 2007, antephase research of rAd-p53 transfer combined with RT for 7 patients with stage 2B to 3B cervical cancer produced a 5-year survival rate of 85.7%. The purpose of this research is to evaluate the effect and safety of rAd-p53 transfer combined with radiotherapy for patients with locally advanced cervical cancer.
Materials and Methods
P53 gene agent and usage
Recombinant adenovirus-p53 (Gendicine®) was supplied by China Shenzhen SiBiono GeneTech Co Ltd, Shenzhen, China. rAd-p53 limits the infectivity of the virus to only one cycle, and the adenovirus genome does not integrate into host genome DNA. rAd-p53 was stored at −20°C in a concentration of 1 × 1012 virus particles (vp)/mL. rAd-p53 solution was thawed and diluted moderately in physiologic saline according to tumor size within 0.5 h of use.
Research of biological radiosensitization of rAd-p53
The human cervical cancer cell line SiHa contains wild-type p53 and has HPV16 infection, and C33A contains mutation p53 and has no HPV infection. Cells lines were supplied from China Beijing XieHe Cell Bank or National Cell Bank, China Infrastruture of Cell Line Resource. National Cell Bank supplied both cell lines, SiHa and C33A, which are typically used in some tests in China. The two cell lines were maintained in Dulbecco's modified Eagle medium (Corning, USA). All cells were supplemented with 10% fetal bovine serum (Gibco, New Zealand) and 1% penicillin/streptomycin (Invitrogen) and cultured at 37°C in a humidified incubator containing 5% CO2. Both SiHa and C33A cell lines were infected by rAd-p53 in 50 MOI (multiplicity of infection), then flow cytometry was used to analyze cell cycle process, Western blot revealed the expression of p53 protein, and immunohistochemical staining was used to assess the expression of p53 gene and p53 target gene. Radiobiologic methods demonstrated the sensitization enhancement of ratio of rAd-p53 to RT.
Study design and patients
This was a randomized control clinical trial. The study protocol and informed consent process was approved by the Peking University Cancer Hospital Ethics Committee. Qualified patients with locally advanced cervical cancer were randomly assigned to one of two groups according the randomized table (2:1) designed by a biostatistician: the group receiving rAd-p53 combined with radiotherapy (PRT group) and the group receiving radiotherapy alone (RT group) as a control. Two cancer centers, Peking University Cancer Hospital (Beijing, China) and Fujian Province Cancer Hospital (Fuzhou, China) participated in this trial together. The inclusion criteria were as follows: patients were between 18 to 80 years of age and had a histologic diagnosis of cervical squamous cell carcinoma with measurable focus in cervix by CT/MRI image and no distant metastasis. Disease was clinically staged according to the FIGO staging system: 2B, tumor with parametrial invasion; and 3B, tumor extends to pelvic wall and/or concomitance hydronephrosis or nonfunctioning kidney. Patients with stage 2B–3B cervical cancer were enrolled in the clinical trial. Patients had to have a life expectancy of at least 6 months and a Karnofsky performance score of at least 70. Patients were required to have adequate bone marrow function (white blood cell count ≥4.0 × 109 cells/L; hemoglobin count ≥100 g/L; platelet count ≥100 × 109 platelets/L) and adequate liver and renal function (aspartate aminotransferase, alanine aminotransferase, blood urea nitrogen and creatinine lower than or equal 1.5 times the upper limit of normal). The exclusion criteria were as follows: pregnant or nursing women, patients with uncontrolled serious infections or with serious heart and lung failure, patients with myelosuppression causing inadequate bone marrow function (WBC count <4.0 × 109/L; hemoglobin count <100 g/L; platelet count <100 × 109 platelets/L), and those with inadequate liver and renal function (aspartate aminotransferase, alanine aminotransferase, blood urea nitrogen, and creatinine higher than 1.5 times the upper limit of normal) were excluded. In addition, selected patients signed the informed consent forms.
For the group PRT, immediately prior to receiving radiotherapy, rAd-p53 at a dose of 1 × 1012 vp was given to the cervical tumor directly via intratumoral multipoint injection through the vagina, once a week for a total of 6 weeks. For the two groups (PRT and RT group), the same irradiation technique was performed with a total of 45 Gray units (Gy) external-beam radiotherapy (EBR) to the whole pelvis of the patient was delivered concurrently in 20–23 fractions by high energy (>6 MV) accelerator photons. Parametrial boost was performed with a dose of EBR 10–15 Gy. High-dose-rate intracavitary brachytherapy was performed during EBR or following its completion with a dose of 20–30 Gy to point A, which is localizasion at cervex oral side 2 cm point, received 75–80 Gy. So pelvic RT plus brachytherapy to take point A to 75–80 Gy. Response was assessed using the response evaluation criteria in solid tumors method. The largest diameter of cervical tumors were measured according to CT/or MRI imaging at pretreatment and two time points of posttreatment: (i) pelvic RT plus brachytherapy to take point A to 75–80 Gy dose, and (ii) validation time point (2 months after the completion of radiotherapy). The tumor size and tumor shrinkage rates were calculated. Immediate tumor response rates, such as complete response (CR), partial response (PR), stable disease (SD), and progressive disease (PD) were determined according to the World Health Organization (WHO) evaluation standard of solid tumor treatment. A comparative study was also performed on the immediate response rate at validation time points and long-term survival between the two groups.
Adverse events
The toxicity grade was determined by Common Terminology Criteria for Adverse Events (CTCAE) version 3.0. Patients were monitored for adverse events. Toxic and adverse events were assessed as light (grade 1), mild (grade 2), serious (grade 3), and life threatening (grade 4) according to the WHO's evaluation standard for adverse events. Particular attention was paid to body temperature.
Statistical methods
All data were statistically analyzed using IBM SPSS 19.0 statistical software. The endpoints were loco-regional recurrence-free survival, distant metastasis-free survival, progress-free survival, and overall survival and were estimated using the Kaplan–Meier statistical method. Endpoints of the PRT group were compared with those of control group RT. Univariate analysis was used to identify prognostically significant variables for these endpoints. For all outcomes, we obtained Cox hazard ratios (HR) using the fixed effect model. Differences between test group and control group were assessed with the log-rank technique. All reported p values resulted from two-sided statistical tests. All p values less than 0.05 were considered significant.
Results
The preclinical study showed that exogenous p53 gene could be transferred efficiently into SiHa and C33A cells’ nucleus after the infection with rAd-p53. Western blot revealed that the expression of p53 gene started at 2 h, and achieved peak at 24–48 h, and decreased to disappearance at 120 h later after the infection with rAd-p53 in both cells. Immunohistochemical staining showed that 1.47% and 23.00% (mutation) of cells expressed the p53 gene, 1.90% and 12.90% of cells expressed p21 gene, and 2.10% and 13.00% of cells expressed Bax gene for SiHa and C33A cells, respectively, before infection with rAd-p53 (control group). At 48 h after infection with rAd-p53, the proportion of cells expressing p53 gene increased to 86.95% and 90.28%, cells expressing p21 gene increased to 81.70% and 88.37%, and cells expressing Bax gene increased to 59.57% and 62.90% for SiHa and C33A cells, respectively. Flow cytometry revealed that G2/M phase ratios of 9.47 and 11.33 in the control group increased to 21.62 and 46.79 for the rAd-p53–infected group for SiHa and C33A cells, respectively. Apoptotic rates of 5.7% and 8.6% for control group increased to 6.7% and 23.2% for rAd-p53–infected group for SiHa and C33A cells respectively. Apoptotic rates of 7.8% and 16.7% for radiation at 6Gy-only group increased to 9.3% and 33.1% for rAd-p53 infection combined with radiation at 6Gy for SiHa and C33A cells respectively. The SF2 (survival fraction at 2Gy) was 36.0% and 27.3% and decreased to 15.0% and 8.8% for rAd-p53 transfer combined with radiation at 2Gy group for SiHa and C33A cells respectively. It was suggested that rAd-p53 sensitizes SiHa and C33A cells to radiation [D0s (final slopes) of the survival curves for the combined group were 1.849 Gy and 1.064 Gy, compared with 2.205 Gy and 1.254 Gy for radiation-only group for SiHa and C33A cells, respectively). The sensitization enhancement of ratios were 1.19 in SiHa and 1.18 in C33A respectively. Upregulation of p53,p21, and Bax genes were observed in both cells after infection with rAd-p53, which revealed that the mechanism of rAd-p53 infection induced cell cycle arrest and apoptosis. The combination of rAd-p53 infection with radiation increases cell cycle arrest at G2/M, apoptosis, and inhibition of cervical cancer cell growth more than any treatment alone in vitro. rAd-p53 has the effect of radiosensitization on both cells. The results provide the potential theoretical foundation for the clinical research.
Response
Because the expected positive results were acheived, this trial was stopped ahead of schedule at 104 cases. According the randomized table (2:1) (March 2007 to November 2011) 104 qualified patients enrolled into this trial. Evaluable for analysis the 104 patients (69 PRT and 35 RT), including rAd-p53 combined with radiotherapy (n = 69, group PRT) and the group receiving radiotherapy alone (n = 35, group RT). As shown in Table 1, no significant differences in sex, age, physical status, histological type, and clinical stage were found between the PRT and RT groups. Of 104 patients with invasive squamous cell carcinoma of the cervix, mean age was 52.0 years old (range 35–68 y for PRT and range 35–77 y for RT, respectively). There were 69 patients with cervical cancers of FIGO stage 2B (38 patients, 55.1%) and 3B (31 patients, 44.9%) for the PRT group and 35 patients with cervical cancers of FIGO stage 2B (21 patients, 60.0%) and 3B (14 patients, 40.0%) for the RT group. The 69 patients were intratumorally injected with rAd-p53 1 × 1012 vp, once a week for 6 weeks. Thus, total injection with mean of 6.0 times (4–8) was completed. rAd-p53 injection weekly concurrently combined with radiotherapy including pelvic RT plus brachytherapy to take point A to 76.0 standard deviation 2.40 Gy (range 75.0–80.0 Gy), and 35 patients of RT group received radiotherapy with pelvic RT plus brachytherapy to take point A to 79.0 standard deviation 3.50 Gy (range 69.0–82.0 Gy); there was no statistical difference in FIGO stage distribution and radiation dose between the PRT group and RT group (p = 0.734 and p = 0.934 respectively).
Characteristics of patients and tumors
PRT group received rAd-p53 combined with radiotherapy; RT group received radiotherapy only.
FIGO, International Federation of Gynecology and Obstetrics Stage System; rAd-p53, recombinant adenovirus-p53; SD, standard deviation; SCC, squamous cell carcinoma.
At pretreatment, the average largest diameter of cervical tumors were 5.1 cm and 4.9 cm for the PRT and RT groups, respectively, and no statistical difference between the two groups (p = 0.181). At the validation time point (2 months after the completion of radiotherapy), immediate tumor response showed that CR, PR, SD, and PD were 66.7%, 33.3%, 0.0%, and 0.0%, respectively, for group PRT and 54.3%, 37.1%, 8.6%, and 0.0%, respectively, for group RT. CR rate of group PRT was 12.4% higher than that of group RT; the tumor response of group PRT was obviously better than that of group RT (p = 0.037).
Adverse events
Total data showed that all the values in bone marrow function, and liver and renal function, remained within normal range before and after treatment in the PRT group compared with that of the RT group (Table 2). Incidence of late radiorectitis occurred in grade II 6 (8.7%), grade III 3 (4.3%), and grade IV 1 (1.4%) for group PRT; and in grade II 5 (12.8%), grade III 2 (5.1%), and grade IV 1 (2.6%) for group RT. Incidence of late radiocystitis occurred in grade II 1 (1.4%), grade III 0 (0.0%), and grade IV 1 (1.4%) for group PRT; and in grade II 0 (0.0%), grade III 1 (2.6%), and grade IV 0 (0.0%) for group RT. There was no significant difference in incidence rate of late adverse events between group PRT and group RT, which proved that rAd-p53 administration did not increase the adverse events caused by radiotherapy.
Bone marrow, liver, and renal function of PRT group compared with that of the RT group
ALT, alanine aminotransferase; AST, aspartate aminotransferase; BUN, blood urea nitrogen; Cr, creatinine; Hb, hemoglobin; Plt, platelet; Wbc, white blood cell count.
The incidence rate of fever events after injections of rAd-p53 was 93.4%, which included grade 1 fever (37–38°C) 4.3%, grade 2 fever (38–40°C) 71.7% and grade 3 fever (40–41°C) 17.4% and no grade 4 (>41°C). Development of fever was observed as early as approximately 3 h after injection, lasting about 4 h and then disappearing spontaneously. Only slight pain and discomfort at local injection sites were reported from the repeat injections.
Eight-year follow-up outcome
The date of last follow-up was April 1, 2015, with median follow-up period of 60.5 months (range 10.8 ∼ 97.0) for two groups. Finally, 1 patient in the PRT group and 2 patients in the RT group were lost to follow-up. The date of lost to follow up was considered as the death date. Incident cases of locoregional recurrence totaled 4 cases in the PRT group and 9 cases in the RT group. The 5-year locoregional recurrence rate was 6.2% in the PRT group and 28.6% in the RT group (HR = 0.197, 95% confidence interval [CI] 0.060–0.639, p = 0.003; Table 3 and Fig. 1). There were 14 incident cases of distant metastasis in the PRT group and 8 cases in the RT group, and distribution sites of distant metastasis were lung (10), bone (1), neck lymph (1), and mediastinum lymph (1) in the PRT group and lung (6), liver (1), and bone (1) in the RT group. The 5-year distant metastasis rate was 21.3% in the PRT group and 25.8% in the RT group (HR = 0.824, 95% CI 0.345–1.967, p = 0.662; Table 3).

Locoregional recurrence free survival rate of the recombinant adenovirus (rAd)-p53 in combination with radiotherapy (PRT) group compared with that of the radiotherapy only (RT) group. HR, hazard ratio.
Eight-year follow-up outcome of PRT group compared with that of RT group
OS, overall survival rate; PFS, progress-free survival rate.
The mean survival time was 79.1 (95% CI 71.9–86.4) months in the group PRT, and 63.9 (95% CI 53.1–74.7) months in the RT group. One-, three-, and five-year survival rates were 97.1%, 83.9%, and 74.2%, respectively, in the PRT group and 97.1%, 71.4%, and 56.7%, respectively, in the RT group (HR = 0.551, 95% CI 0.278–1.095, p = 0.084; Table 3 and Fig. 2). The mean progress-free survival time was 78.8 (95% CI 70.7–87.0) months in the group PRT, and 60.1 (95% CI 47.4–72.7) in the group RT. One-, three-, and five-year progress-free survival rates were 94.1%, 78.4%, and 76.7%, respectively, in the group PRT, and 80.0%, 59.6%, and 59.6%, respectively, in the group RT, (HR = 0.485, 95% CI 0.234–1.006, p = 0.047; Table 3 and Fig. 3).

Overall survival rate of the PRT group compared with that of the RT group.
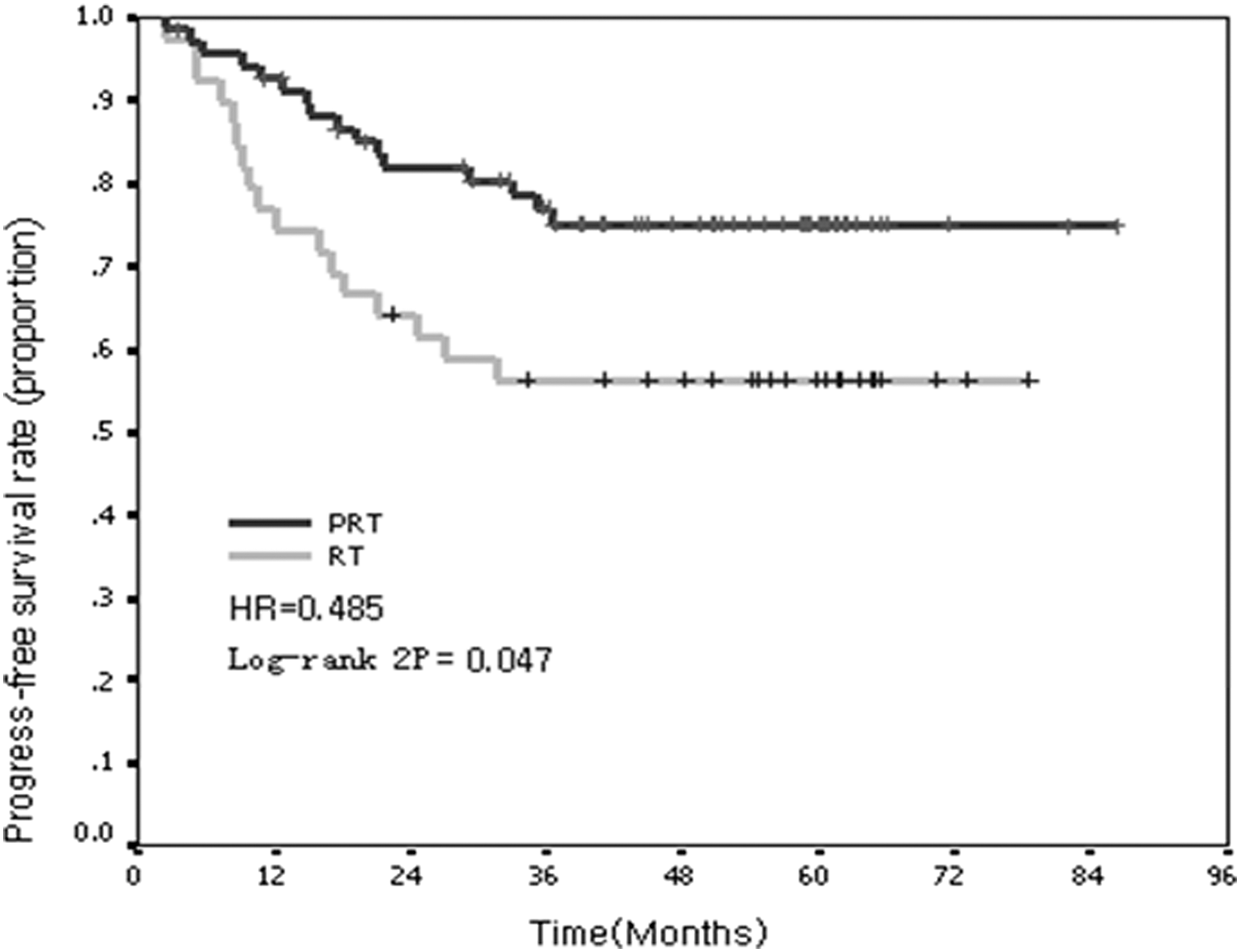
Progress-free survival rate of the PRT group compared with that of the RT group.
Discussion
The preclinical study demonstrated that the rAd-p53 infection of cervical cancer cell lines SiHa and C33A obviously increased the expression of p53, p21, and Bax and has the effect of radiosensitization on both cervical cancer cells in vitro. The clinical study indicated the survival benefit of rAd-p53 in combination with radiotherapy for locally advanced cervical cancer, compared with the control (RT) group, as shown in Table 3 and Figs. 1 –3. Firstly, there were improvements in locoregional tumor control with rAd-p53 in combination with radiotherapy for cervical cancer; the PRT group and the RT group developed 5-year locoregional recurrence rates of 6.2% and 28.6% respectively. Markedly, rAd-p53 improved 5-year radiotherapeutic locoregional tumor control by 22.4% (Table 3, Fig. 1) and has shown potential to increase survival benefit for advanced cervical cancer. The 5-year overall survival rate and 5-year progress-free survival rate of the PRT group were 17.5% (HR = 0.551, p = 0.084, 74.2% vs. 56.7%) and 17.1% (HR = 0.485, p = 0.047, 76.7% vs. 59.6%) higher than those of the group RT (Table 3, Figs. 2, 3). The 5-year distant metastases rate was 21.3% in the PRT group and 25.8% in the RT group (HR = 0.824, p = 0.662), with no statistical difference between the two groups (p = 0.662). rAd-p53 significantly contributed to a decrease in locoregional recurrence rate but not in distant metastasis rate, potentially increasing survival rates for advanced cervical cancer.
Total data showed that all the values in bone marrow function, liver and renal function, and lung and heart function remained within normal range before and after treatment in the PRT group compared with that of RT the group (Table 2). rAd-p53 administration did not increase the late adverse events caused by radiotherapy.
Replacement with normal p53 gene using viral vectors results in suppression and reversal of the malignant phenotype of tumors and induces radiosensitization—a new strategy to convert a radioresistant phenotype into a radiosensitive one. These results support the combination of rAd-p53 with radiotherapy in clinical trials and without exacerbating the side effects resulting from radiotherapy.
This was a randomized control clinical trial, which compared with the control radiotherapy. Five-year survival rate of the PRT group was 74.2%, which is 17.5% higher than that of the RT group.
In conclusion, rAd-p53 in combination with radiotherapy was safe and biologically active to improve radiotherapeutic survival in patients with cervical cancer.
Footnotes
Acknowledgments
We thank the patients who participated in this clinical trial, without whose help this study would not have been possible. This study was registered in the WHO International Clinical Trials Registry, Chinese Clinical Trial Register (registration number ChiCTR-TRC-08000091).
Author Disclosure
No competing financial interests exist.