
Abstract
Ex vivo normothermic lung perfusion (EVLP) is a novel platform and method developed to facilitate functional assessment and implementation of advanced therapies for donor lungs prior to transplantation. This study aimed to determine the safety and immunological and functional benefits of ex vivo adenoviral human interleukin-10 (AdhIL-10) gene delivery to prevent the development of primary graft dysfunction in a large animal survival model. Pig donor lungs were retrieved, preserved for 6 h at 4°C, and then randomly assigned to four groups: (1) AdhIL-10 gene therapy: 12 h EVLP + AdhIL-10 intra-bronchial delivery; (2) EVLP-control: 12 h EVLP; (3) Vector-control: 12 h EVLP + adenoviral vector intra-bronchial delivery; and (4) prolonged hypothermic preservation: additional 12 h of cold ischemia. The left lung was then transplanted and evaluated. The recipients were recovered and kept alive until day 7 post-transplant under standard triple immunosuppression. Plasma levels of hIL-10 were detected in the treatment group throughout the 7 days. Analysis of peripheral blood obtained after transplant showed no signs of hematological, renal, or hepatic toxicity in the AdhIL-10 group. The immediate post-transplant lung function was significantly better in the EVLP-control and AdhIL-10 groups. Gas exchange at day 7 was superior in allografts from the AdhIL-10 group, and the histologic inflammation score was significantly lower. Lymphocytes from AdhIL-10 group harvested from mediastinal lymph nodes at day 7 post-transplantation and co-cultured with donor lymphocytes showed significantly less interferon gamma production in an Enzyme-Linked ImmunoSpot assay when compared with non-treatment groups. It has been demonstrated in this preclinical large animal survival study that ex vivo treatment with AdhIL-10 is safe and improves post-transplant lung function over EVLP alone. Improved function and an immunological advantage in both the innate and adaptive immune responses have been demonstrated.
Introduction
L
Donor lungs not utilized for transplantation, based on conventional criteria, often present with increased levels of pro-inflammatory cytokines. 3 Furthermore, when lungs with high levels of pro-inflammatory cytokines are transplanted, recipients experience a higher incidence of primary graft dysfunction (PGD) and increased 30-day mortality. 4 Therefore, one strategy to increase the utilization of donor lungs safely should be to target inflammation associated with the early innate immune response. A promising approach to decrease organ inflammation is via the administration of adenoviral interleukin-10 (AdhIL-10) gene therapy.
In working toward the ultimate goal of genetically modifying donor lungs to improve function after transplantation, using a stepwise and systematic series of experiments, a technique has been developed to upregulate IL-10 in the donor lung using adenoviral vector-delivered gene therapy.
Techniques (dose, route and delivery system) have been developed to optimize adenoviral vector delivery through the airway in rodent 5 –7 and pig donor lungs. 8 It has also been shown that standard immunosuppression used in clinical transplantation can be used to facilitate gene expression and improve lung function. 5,6,8 It has been shown that adenoviral vector gene delivery could be effectively delivered in an ex vivo lung perfusion (EVLP) system in pig lung transplants and in damaged human lungs that were not used for transplantation to improve lung function to within transplantable parameters. 9,10 Following the recent clinical success of EVLP, 11,12 this lung preservation method has been translated to standard clinical practice as an effective technique to evaluate and treat injured donor lungs. The authors aspire to use this platform to take this concept to the next level and use gene therapy to repair injured human donor lungs and pre-prepare the lungs to make them even more safely useable for transplantation. Besides eliciting less vector-related inflammation due to its ex vivo situation, 10 the ability to improve lung function after transplantation has been shown by decreasing levels of pro-inflammatory cytokines and providing recovery of lung injury, as evidenced by the reconstitution of alveolar epithelial cell tight junction integrity. 9
Although very encouraging, the data reported by previous acute animal studies were limited to a time span of 4 h after transplantation. To advance this technique further toward clinical trial, the safety and efficacy of IL-10 gene therapy needs to be tested in a survival model. The objective of the present study was to examine the safety of AdhIL-10, its capability to maintain IL-10 expression, and its effects on allograft function. This was carried out in a study of ex vivo AdhIL-10 gene therapy in a porcine lung transplantation 7-day survival model.
Materials and Methods
Study design
Male domestic Yorkshire pigs (25–35 kg) were utilized in an experimental protocol approved by the Animal Resource Centre at University Health Network, Toronto, Canada. Animal care was in compliance with Principles of Laboratory Animal Care by the National Society for Medical Research and the Guide for the Care of Laboratory Animals by the National Institutes of Health.
Under general anesthesia, donor animals were submitted to organ procurement following standard technique. 8 The lungs were subjected to 6 h of cold ischemia and then randomly assigned to one of four groups: (1) AdhIL-10 gene therapy: 12 h EVLP +1 × 1010 plaque-forming units (pfu) of intra-bronchial AdhIL-10 (n = 5); (2) EVLP-only (control): 12 h EVLP + vehicle/saline only (n = 5); (3) Ad-Vector: 12 h of EVLP +1 × 1010 pfu of empty virus cassette (n = 4); or (4) CIT: additional 12 h of cold ischemia (no EVLP; n = 4).
Anesthesia protocol
Pigs received pre-induction sedation with intramuscular ketamine (40 mg/kg). Induction was carried with inhaled isoflurane 5%, topical lidocaine was sprayed in the glottis, and animals were intubated with an 8.0 size endotracheal tube. Maintenance agents consisted of intravenous propofol (5–8 mg/kg/h) and fentanyl citrate (10 μg/kg/h).
Ex vivo lung perfusion
Double-lung blocks were extracted from the donor after conventional flush preservation with low potassium dextran solution (Perfadex; XVIVO Perfusion, Denver, CO). The details of this EVLP technique have been previously described. 13 Briefly, the left atrium and pulmonary artery were cannulated, and the trachea was intubated. A custom-made EVLP circuit was connected, and the reservoir was primed with 1.5 L of Steen solution (XVIVO Perfusion) plus 500 mg of methylprednisolone, 1 g of cefazolin, and 10,000 IU of heparin. The lungs were then connected and perfused with gradually increasing flows, achieving full EVLP flow (40% of estimated cardiac output) at 50 min. Gradual rewarming, from room temperature to 32°C and finally to 37°C, was also part of the initiation protocol. Ventilation was started when the lungs reached 33°C, with a tidal volume of 7 mL/kg, a rate of seven breaths per minutes, and a FiO2 of 21%. After 12 h of EVLP, lungs were cooled to 15°C and placed in cold Perfadex on ice while the recipient was prepared for left single-lung transplantation.
Gene therapy vector
A second-generation, E1, E3-deleted, replication-deficient serotype 5 adenoviral vector, under control of a cytomegalovirus promoter containing either human IL-10 sequence or the empty cassette, was provided by the University of Iowa College of Medicine Gene Transfer Vector Core (Iowa City, IA). After the first hour of EVLP, 1 × 1010 pfu of AdhIL-10 diluted in normal saline to a total volume of 10 mL was delivered though a video fiber-optic bronchoscope (Olympus Canada, Markham, Canada), as previously described. 10 The Ad-vector group received 1 × 1010 pfu of empty viral cassette and the EVLP control group received 10 mL of saline.
Lung transplantation and survival model
Left single-lung transplantation was performed following the previously described technique. 14 Thirty minutes after reperfusion, a sample was taken from the transplanted lung pulmonary vein to evaluate graft function. An analgesic intercostal block with bupivacaine was performed. The pleural cavity was drained with a 20 Fr chest tube connected to an ambulatory drainage valve (Pneumostat, Atrium Medical Corp., Hudson, NH). Postoperative analgesia was carried out with fentanyl patches (50 μg/h). Intramuscular buprenorphine was administered as needed. Antimicrobial prophylaxis consisted of intravenous ceftazidime 1 g every 12 h. An oral three-drug immunosuppressive regimen consisted of cyclosporine 5 mg/kg every 12 h, azathioprine 50 mg/kg/day, and prednisone 1 mg/kg/day. At day 7 after transplantation, the animals were anesthetized, and a median sternotomy was performed. The right pulmonary artery was clamped for 5 min followed by arterial blood gas sampling for isolated lung graft functional assessment.
Sample collection
Systemic blood samples were collected 6 h after reperfusion and then daily from a previously placed internal jugular vein indwelling catheter (9.5 Fr TPN Catheter set, Cook Medical, Bloomington, IN) for analysis of red blood cell count, white blood cell count, and differential, platelets, urea, creatinine, alanine transaminase (ALT), and aspartate transaminase (AST). One aliquot of the samples collected at days 1, 4, and 7 was centrifuged at 1,000 g, and the supernatant stored at −80°C for plasma cytokine analysis.
Lung biopsies were taken at day 7 post-transplantation, with one portion snap frozen in liquid N2 for cytokine analysis and another portion inflated and stored in 10% buffered formalin for 24 h for histopathological examination. The storage solution was then replaced with 70% ethanol and subsequently embedded in paraffin.
Cytokine assays
For tissue cytokine analysis, frozen lung tissue was homogenized as previously described. 10 Cytokine analysis was performed using enzyme-linked immunosorbent assay kits for human IL-10 and porcine IL-6, IL-8, IL-10, IL-1o, and interferon gamma (IFN-r; R&D Systems, Minneapolis, MN).
Histologic assessment
Sections were stained with hematoxylin and eosin and blindly assessed by a specialized lung pathologist (D.H.) using the International Society for Heart and Lung Transplantation (ISHLT) acute rejection scoring. 15 Sections were also blindly assessed for inflammation grading using parameters modified from Piedra et al., 16 which included peri-bronchovascular inflammation, alveolar septal inflammation, acute lung injury, and polymorphonuclear infiltration.
Proliferation assay
Mediastinal lymph nodes were harvested from the recipient at day 7, and cells were mechanically extracted with a cell strainer. These cells were labeled with CFDA-SE (CellTrace; Invitrogen, Life Technologies, Inc., Burlington, ON). Donor splenocytes were depleted of T cells after irradiation with 20 Gy and then used as stimulators. Responder cells were co-cultured with stimulator cells at a 1:1 ratio in triplicate. After 72 h, cells were harvested, washed twice, and re-suspended in binding buffer. Cell proliferation was assessed by flow cytometry (BD LSRII; Becton Dickinson, Franklin Lakes, NJ). Data were analyzed with FLOWJO software (Tree Star Inc., Ashland, OR).
Enzyme-Linked ImmunoSpot
Mediastinal lymph node cells (1.5 × 105), harvested at day 7 post-transplant, were co-cultured in a 1:1 ratio with medium alone, allogeneic irradiated splenocytes, or third-party splenocytes for 48 h using a Porcine IFN-γ Enzyme-Linked ImmunoSpot (ELISPOT) kit (R&D Systems). Plates were read using an ImmunoSpot analyzer, and results are expressed as number of spots/well.
Statistical analysis
All results are expressed as mean ± standard error of the mean. An unpaired Student oft-test and Mann–Whitney nonparametric test were used for comparisons between two groups whenever appropriate. For comparisons between groups at all time points, two-way repeated-measures analysis of variance (ANOVA) was used. Significance was considered whenever p ≤ 0.05.
Results
Ex vivo AdhIL-10 transfection provides effective transgene expression
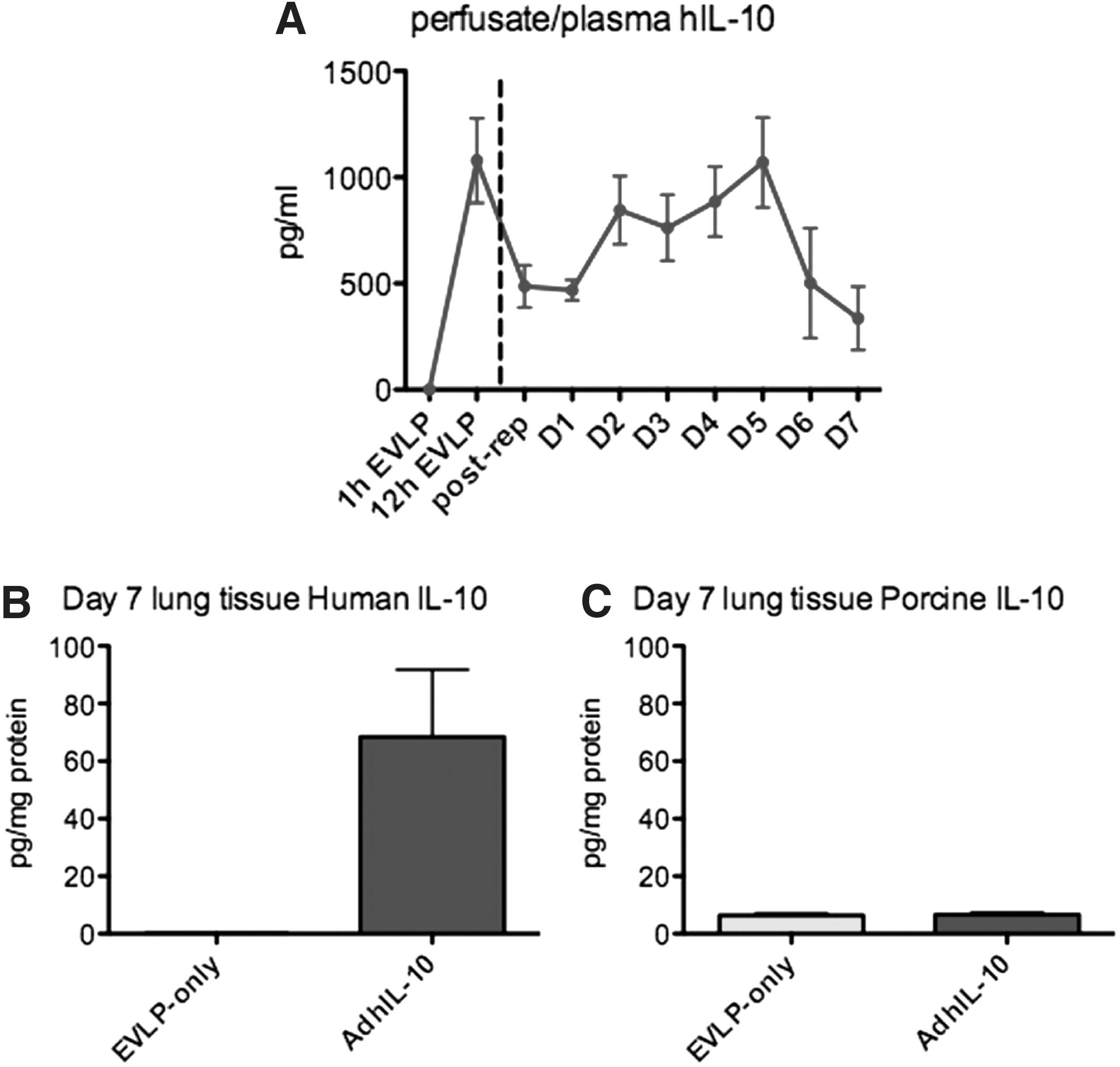
Human IL-10 was absent in perfusate samples taken at 1 h of EVLP. At 12 h, perfusate IL-10 levels increased to 998.9 ± 223.3 pg/mL (Fig. 1A). Post-transplant, the hIL-10 level in the plasma increased from approximately 500 pg/mL to a peak level of approximately 1,000 pg/mL at day 5, and decreased thereafter by day 7. As a negative control, hIL-10 was not found in the perfusate or in daily plasma samples in all other groups. Moreover, there was no significant difference in porcine IL-10 between AdhIL-10 and EVLP-only groups in the plasma (data not shown).
Ex vivo AdhIL-10 transgene expression. (
Local transgene expression was confirmed by positive levels of human IL-10 in lung tissue biopsies taken at day 7 post-transplantation. Again, hIL-10 was only detectable in the AdhIL-10-treated group (Fig. 1B); porcine IL-10 did not differ between AdhIL-10 and EVLP-only groups (Fig. 1C).
No evidence of systemic toxicity demonstrated with ex vivo AdhIL-10 gene delivery
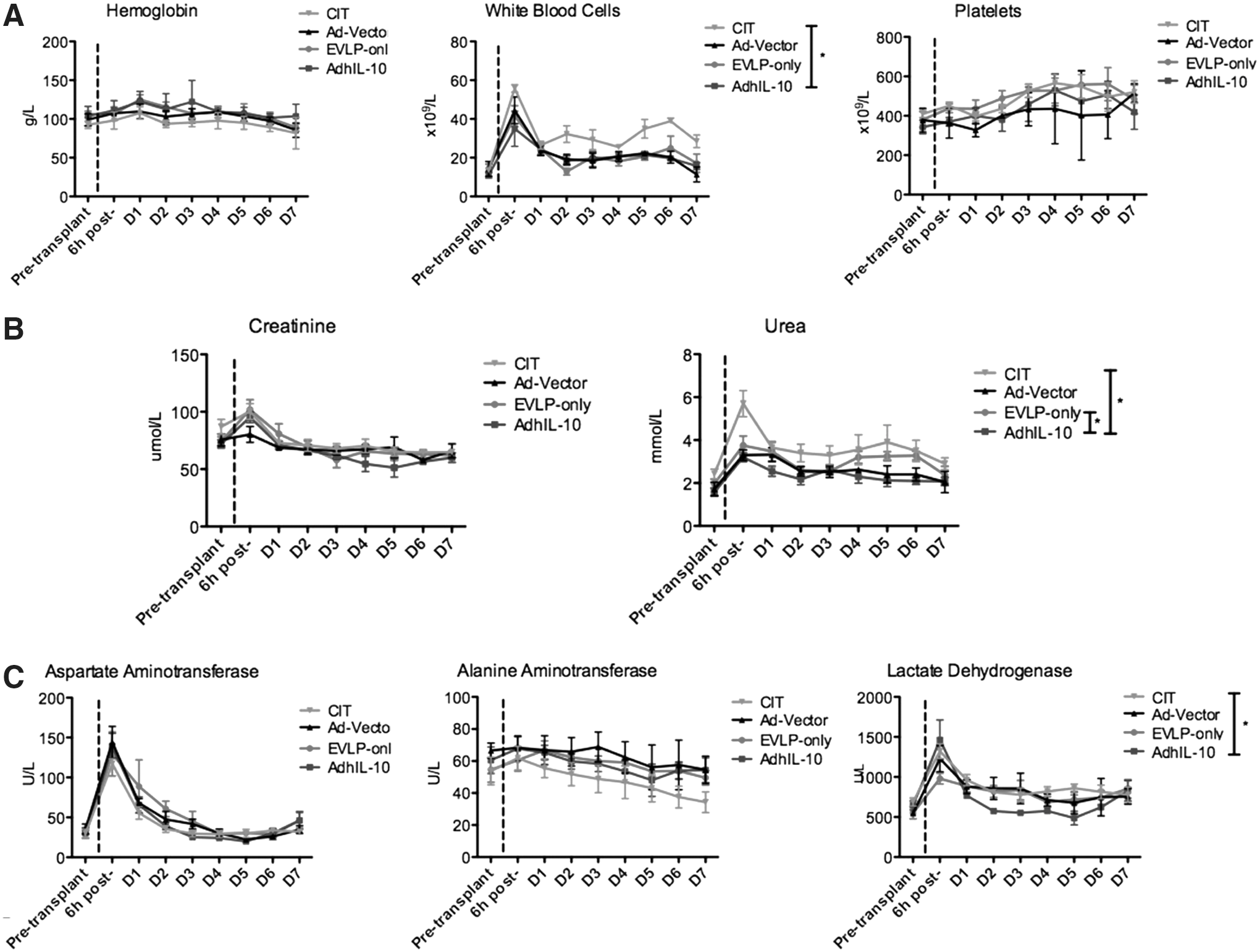
All animals remained healthy, presenting with normal activity and appetites throughout the 7-day period. There were no signs of hematological, renal, or hepatic toxicity observed in the AdhIL-10 group (Fig. 2A–C).
Recipient systemic toxicity profile of AdhIL-10 gene therapy. (
Donor lungs transduced with AdhIL-10 demonstrated superior lung function after transplantation
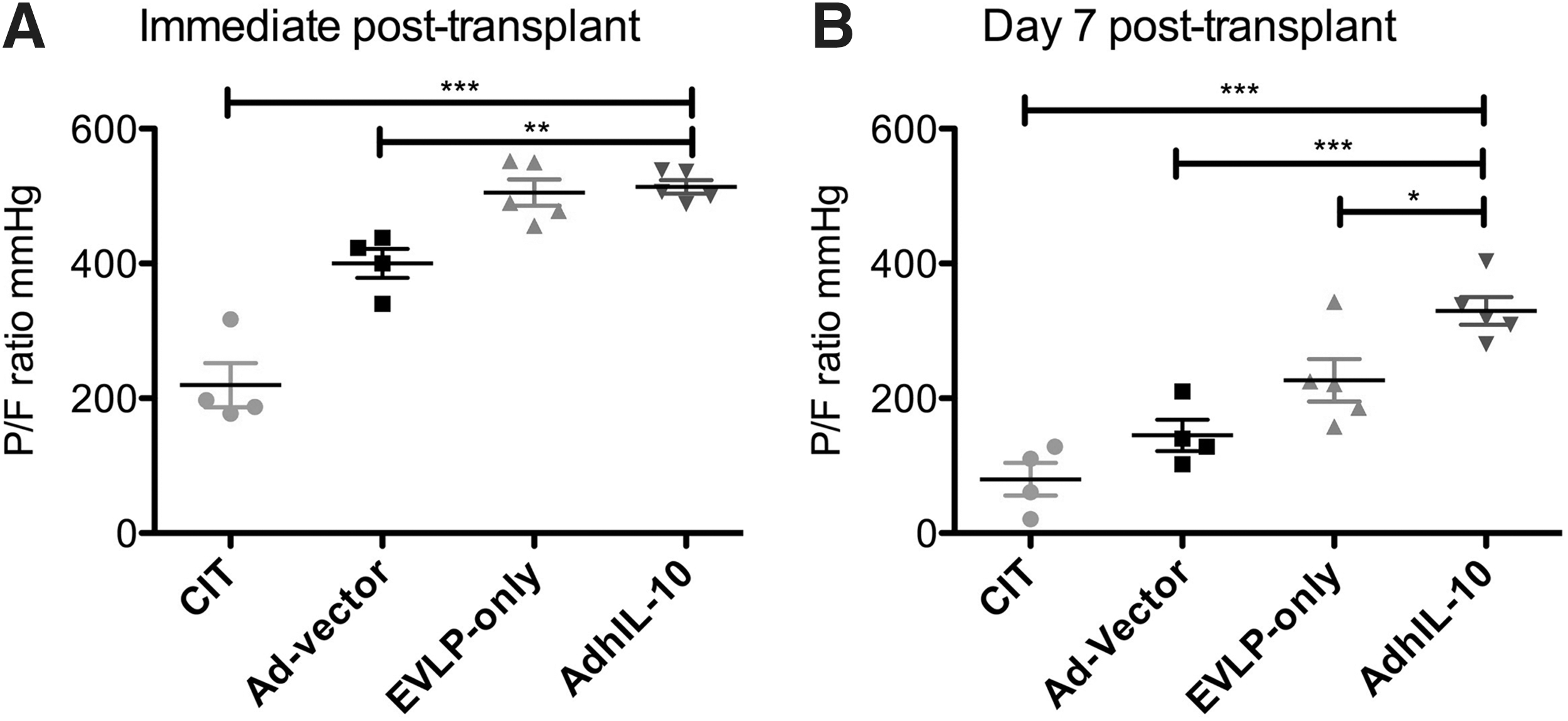
Early post-transplant graft function assessment is depicted in Fig. 3A. The oxygenation function of the lung graft is expressed as a PO2/FiO2 ratio. Transplanted donor lungs from the AdhIL-10 group (513 ± 9 mmHg) functioned significantly better than Ad-vector (400 ± 21 mmHg; p = 0.001) and CIT (219 ± 32 mmHg; p < 0.0001) groups. There was no significant difference between AdhIL-10 and EVLP-only (505 ± 19 mmHg; p = 0.711) groups.
Lung function following transplantation. (
On day 7 after lung transplantation, lungs from the AdhIL-10 group (329 ± 20 mmHg) showed significantly better gas exchange compared with all other groups (CIT 79 ± 24 mmHg, p < 0.0001; Ad-vector 145 ± 23 mmHg, p = 0.0006; EVLP-only 226 ± 31 mmHg, p = 0.025; Fig. 3B).
Donor lungs transduced with AdhIL-10 have decreased tissue inflammation 7 days after transplantation
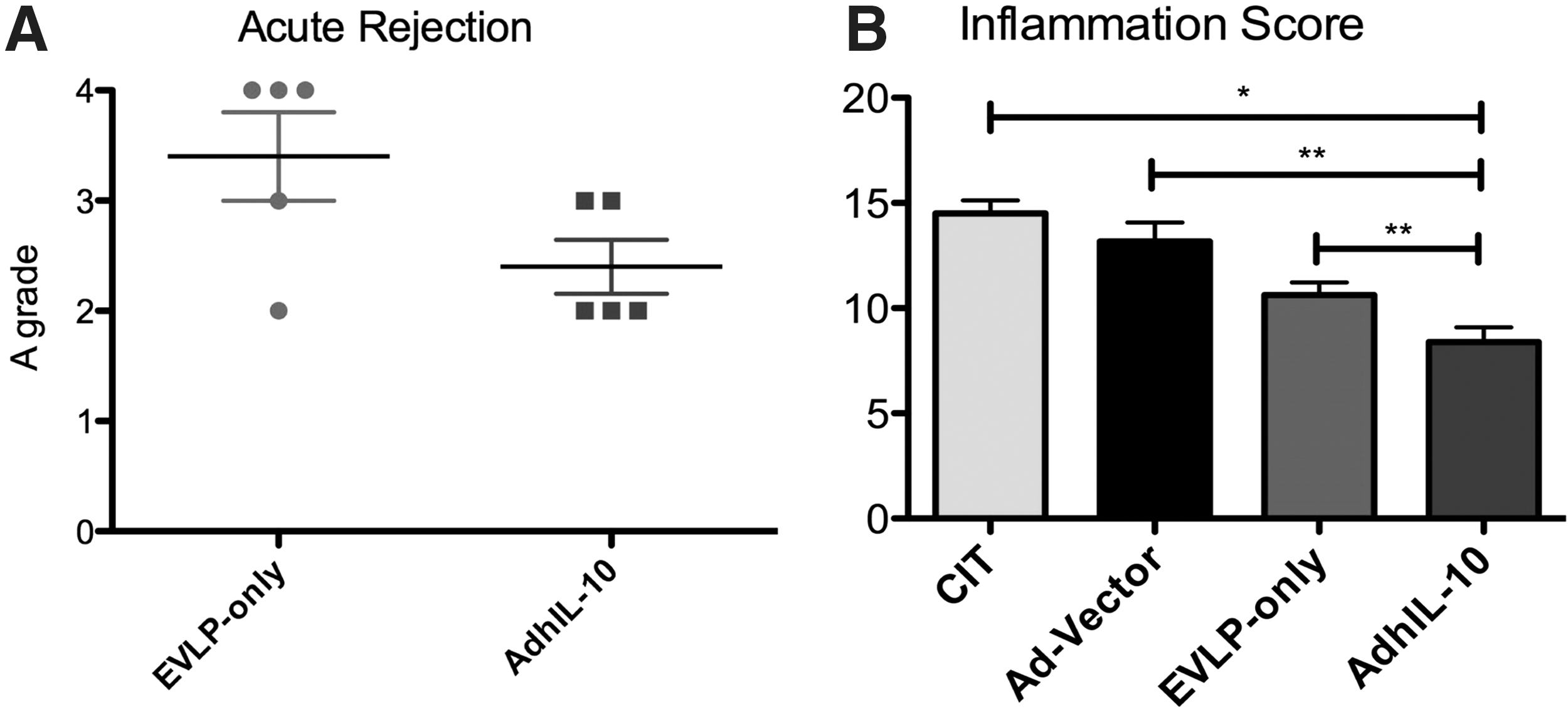
Acute rejection scoring using the ISHLT rejection grading score 15 revealed a trend toward decreased A grades in the AdhIL-10 group compared with the EVLP-only group (p = 0.06; Fig. 4A). There were no differences among these groups with regard to B grades (p = 0.24). The inflammatory score was significantly lower in the AdhIL-10 group (8.4 ± 0.6) when compared with all other groups (CIT 14.5 ± 0.6, p < 0.0001; Ad-vector 12.6 ± 0.8, p = 0.0009; EVLP-only 10.6 ± 0.6, p = 0.026; Fig. 4B). Lung tissue levels of pro-inflammatory cytokines were measured at day 7 post-transplantation. Comparison between AdhIL-10 and EVLP-only groups showed no significant difference in IL-1β (747.6 ± 206.8 vs. 862.4 ± 250.4 pg/mg protein; p = 1), IL-6 (36.8 ± 12.1 vs. 42.1 ± 25.4 pg/mg protein; p = 0.84), IL-8 (106.3 ± 32.5 vs. 102.2 ± 44.9 pg/mg protein; p = 0.69), and IFN-γ (254.8 ± 75.8 vs. 182.4 ± 31.5 pg/mg protein; p = 0.69). On examining the bronchial anastomoses at autopsy, no animals had any evidence of airway dehiscence at day 7.
(
Ex vivo AdhIL-10 decreases systemic levels of pro-inflammatory cytokines
A comparison among groups showed that at day 7, IL-1ong groups showed thatf pro-inflammatory cytokines any evidencep = 0.05; Supplementary Fig. S1A; Supplementary Data are available online at
Allograft specific response was attenuated by AdhIL-10
CD4+ T-cell proliferation was assessed by CFSE-dye dilution on co-cultured plates with donor irradiated splenocytes for 3 days. There was significantly less cell proliferation in cells from recipients in the AdhIL-10 group compared with the EVLP-only group (Fig. 5A and B).

Adaptive immunity evaluation. On mixed lymphocyte reactions, CD4+ cells harvested from mediastinal lymph nodes at day 7 after transplantation were co-cultured for 72 h with allogeneic splenocytes. (
The ELISPOT assay was used to assess donor-specific IFN-n in cells from recipients in the AdhIL-10 group compared s for 3L-10 and EVLP-only -only groups in the plasma (data not shown).of variance (ANOVA) was used. Signifewer spots in comparison with CIT (p = 0.02), Ad-vector (p = 0.03), and EVLP-only (p = 0.05) groups (Fig. 5C). Although the allo-specific response was attenuated in the AdhIL-10 animals, the third-party antigen response was preserved, as depicted in Fig. 5C.
Discussion
The success of clinical lung transplantation can be readily observed in the increasing number of procedures performed annually. 17 However, the number of procedures is plateauing, in part due to the shortage of available donor lungs. Since the lung is susceptible to injuries related to intensive care unit care and brain death, the utilization of lungs from multiple organ donors remains very low. 18 This fact is reflected in the considerable waiting list mortality observed worldwide. 19,20 Furthermore, PGD and chronic rejection are notable barriers that contribute to poor lung transplant outcomes in the short and long term, respectively.
Using a large animal survival model, the present study demonstrated the safety and effectiveness of leveraging an advanced organ preservation strategy—EVLP—for the delivery of AdhIL-10 gene therapy to provide better lungs for transplantation. While it has previously been shown that this strategy resulted in improved lung function up to 4 h after reperfusion, the current study suggests that these benefits are extended at least to 7 days. The allograft rejection response is attenuated and, more importantly, serial collections of peripheral blood did not detect any systemic toxicity reflected by normal hematological, renal, or hepatic functions.
The authors and others have focused efforts on gene therapy strategies to be applied to the donor lung to attenuate ischemia–reperfusion injury for more than a decade. 5 Although considerable success was demonstrated with AdhIL-10 transduction of donor lungs in a preclinical setting, important practical challenges to clinical translation still persisted. First, AdhIL-10 gene therapy required at least 6–12 h following delivery in order to achieve adequate tissue levels of human IL-10. 7 Second, as transfection of the lung during cold ischemic storage was shown to be inefficient, it was thus necessary to apply the viral vector before procurement, which, in clinical practice, would result in significant logistical challenges.
Both of these challenges have been overcome by the development of EVLP, a clinically proven technique to preserve metabolically active lungs stably at normothermia for prolonged periods outside the body. 11,13 As we have previously reported, EVLP proved to be the ideal platform for gene therapy delivery to the donor lung: intra-bronchial AdhIL-10 delivered during EVLP achieves adequate tissue levels upon reperfusion and effectively attenuates ischemia reperfusion injury. 9 Furthermore, a recent comparison between EVLP delivery versus in vivo delivery of AdhIL-10 has clearly shown the benefits of EVLP in further decreasing vector-related inflammation. 10 The present study is a critical next step toward clinical translation. Animals were recovered after transplantation and kept alive for 7 days. Importantly, the kinetics of hIL-10 in the systemic circulation was defined, and effective local transgene expression was achieved at the end of the experiments.
Ischemia and reperfusion injury induces a milieu of sterile inflammation in the graft. 21 In fact, this may be the earliest alloimmune-independent factor contributing to chronic lung allograft dysfunction, the main barrier to long-term survival after lung transplantation. 22 The link between PGD and enhanced allograft immunity has been further elucidated by Bharat et al., who reported an increased frequency of donor HLA class-II specific CD4+ T cells on IFN-n increased frequency of donor HLA clasde novo anti-HLA class II antibodies in recipients who developed PGD. 23 The same group has also shown an early pro-inflammatory trend in a cytokine analysis of patients who developed chronic rejection. 24 In the present study, by providing a less hostile environment in the peri-reperfusion period with ex vivo AdhIL-10, significantly better lung function was found in AdhIL-10 lungs compared with conventional cold preservation (CIT) and controls (EVLP-only or vector-only). Histologic examination has corroborated gas exchange findings and reinforced the significant protective and anti-inflammatory activity of IL-10. Moreover, intra-bronchial AdhIL-10 delivery was capable of decreasing allogen-specific immunity of recipient mediastinal lymph node T cells.
In the clinical setting, gene therapy has achieved considerable success with the use of retroviral vectors to treat severe combined immunodeficiency syndromes. 25 –27 Although efficacy was proven in 85% of treated patients, the small but real risk of development of T-cell leukemia related to insertional mutagenesis raised important biosafety concerns that need to be balanced considering the overall clinical benefit. 28,29 The lack of integration to host DNA, added to the high transgene expression efficiency, has contributed to the emergence of adenoviruses as the most widely used vectors in clinical gene therapy. 30 Nevertheless, the report of one death in the early experience with a Phase I gene therapy clinical trial, conducted for patients with ornithine transcarbamylase deficiency, raised a warning flag. 31 Massive innate immunity activation following intravenous vector delivery led to a systemic inflammatory response syndrome and multiple organ dysfunction. In view of some of these biosafety concerns, the current gene therapy strategy strongly favors minimal toxicity: (1) intra-bronchial as opposed to intravenous vector delivery is used; (2) EVLP has allowed for a diminished vector load requirement to achieve effective transgene expression (1 × 1010 pfu vs. 4 × 1010 pfu from previous studies) 8 ; (3) the ex vivo method means the organ has effectively been removed from the influence of most immune competent inflammatory cells with the absence of circulating leukocytes, thus preventing an enhanced inflammatory response 10 ; (4) the transgene is IL-10, an anti-inflammatory cytokine that has been shown, in a very similar model, to modulate the early inflammatory response during EVLP and after transplantation 9 ; and (5) most importantly, the organ is treated ex vivo before implanting it into the recipient rather than treating the recipient. Using this methodology, the previously reported systemic toxicity manifested as anemia, thrombocytopenia, and acute liver failure is theoretically less likely and indeed was not seen throughout the 7 days of follow-up in this survival study. 32,33 Furthermore, contrary to findings of increased systemic IL-6 in cases of adenoviral vector toxicity, 31 in this study, lower levels of this inflammatory cytokine were observed in the plasma of AdhIL-10-treated animals.
One of the limitations of this study was the absence of other pulmonary function assessments outside of the gold standard P/F ratios. However, assessments of lung mechanics can be cumbersome in single-lung transplantation models, as numbers are obtained from native and transplanted lung together—thus, not fully representing the graft function. Furthermore, as the primary purpose of this preclinical study was to determine the safety of ex vivo adhIL-10 administration, no significant toxicity was observed for every parameter evaluated.
In summary, the present study has demonstrated the safe and effective delivery of AdhIL-10 gene therapy to the donor lung using the Toronto EVLP strategy to modulate the innate and adaptive immune response after lung transplantation in a large animal survival model. This is an important step toward the ultimate clinical application of gene therapy to modify donor organs and improve their performance after lung transplantation.
Footnotes
Acknowledgments
T.N.M. was supported by Research Fellowships from the International Society for Heart and Lung Transplantation, the American Society of Transplantation, and the Canadian Institutes of Health Research (OOP #312227) during different periods of this study. This paper was originally presented and published as an abstract at the 93rd Annual Meeting of the American Association for Thoracic Surgery, Minneapolis, MN, May 2013.
Author Disclosure
XVIVO Perfusion (Denver, CO) provided Steen solution and disposable supplies for the ex vivo lung perfusion portion of these studies. S.K., M.C., and T.K.W. are co-founders of Perfusix Canada and Perfusix USA, and XOR Labs Toronto. M.L. is also a co-founder of XOR Labs Toronto.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.