
Abstract
Induced cell turnover (ICT) is a theoretical intervention in which the targeted ablation of damaged, diseased, and/or nonfunctional cells is coupled with replacement by partially differentiated induced pluripotent stem cells in a gradual and multiphasic manner. Tissue-specific ablation can be achieved using pro-apoptotic small molecule cocktails, peptide mimetics, and/or tissue-tropic adeno-associated virus–delivered suicide genes driven by cell type–specific promoters. Replenishment with new cells can be mediated by systemic administration of cells engineered for homing, robustness, and even enhanced function and disease resistance. Otherwise, the controlled release of cells can be achieved using implanted biodegradable scaffolds, hydrogels, and polymer matrixes. In theory, ICT would enable in situ tissue regeneration without the need for surgical transplantation of organs produced ex vivo, and addresses non-transplantable tissues (such as the vasculature, lymph nodes, and the nervous system). This article outlines several complimentary strategies for overcoming barriers to ICT in an effort to stimulate further research at this promising interface of cell therapy, tissue engineering, and regenerative medicine.
Introduction
M
Further, deleterious paracrine signaling and the aged tissue microenvironment (such as the SASP—senescence associated secretory phenotype) can impair the function of even the most pristine implanted cells. 2 A formidable barrier to truly efficacious stem-cell therapy is that administered cells die before stably engrafting due to a chemically inhospitable and/or overcrowded niche. Therefore, to optimize the function of rejuvenated tissues, the old cells must go.
“Science progresses one funeral at a time.”—Max Planck.
Ict As a Novel Therapeutic Modality in Biomedical Gerontology
A proposed intervention for age-related pathology (ICT) has recently been described, which consists of the coordination of targeted endogenous cell ablation with exogenous, patient-specific human pluripotent stem cell (hPSC)-derived cell administration, mediated in a gradual, multiphasic manner so as to effect the extrinsically mediated turnover of whole tissues and organs (Fig. 1).
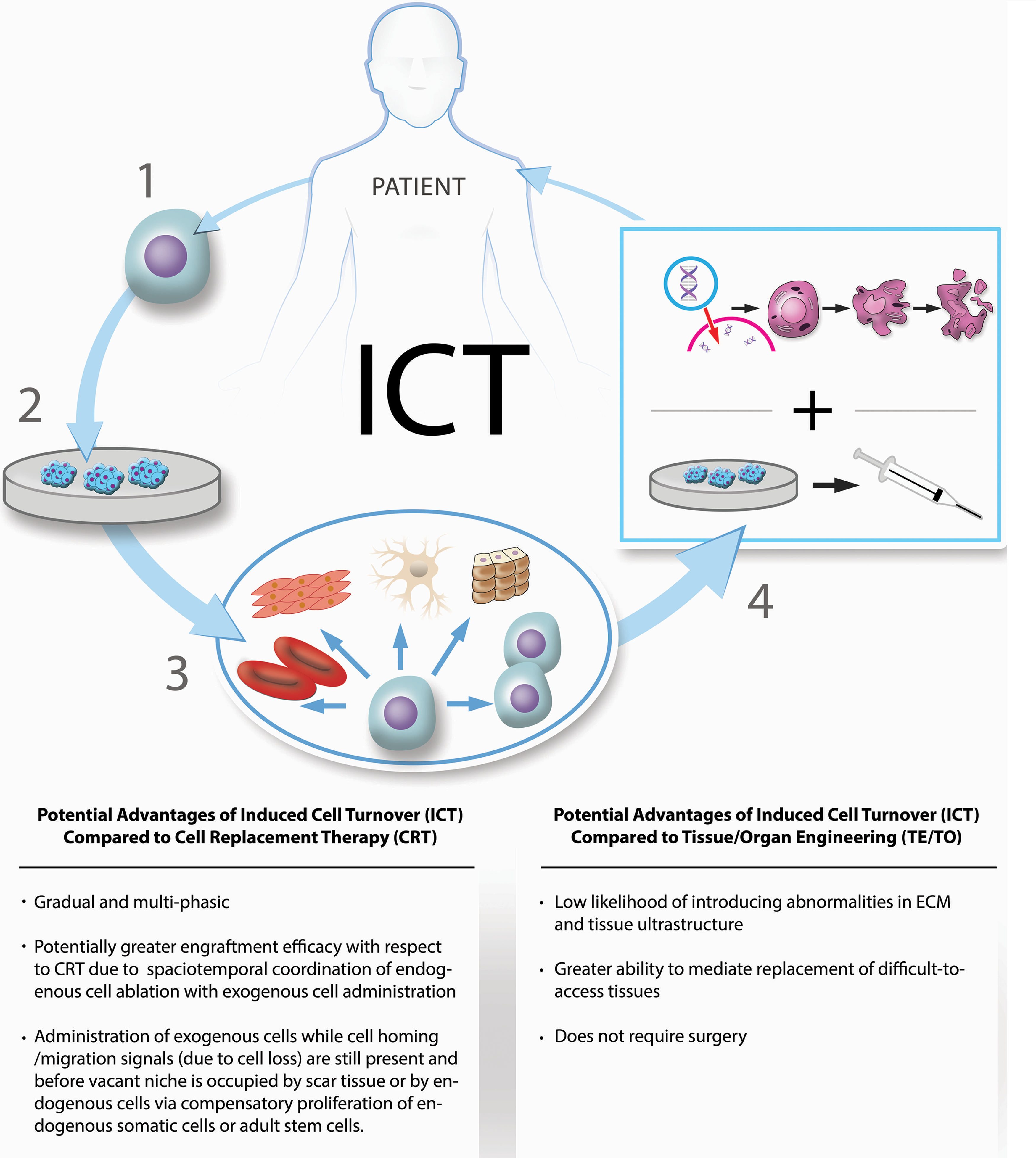
A highlight of the potential advantages of induced cell turnover (ICT) with respect to standard cell therapies (i.e., cell replacement therapy) and tissue/organ engineering, and a schematic representation of ICT. (1) Derivation of patient-specific human pluripotent stem cells (hPSCs). (2) Culturing of hPSCs to produce a sufficient quantity of exogenous cells. (3) hPSCs directionally differentiated into desired cell types. (4) Administration of directionally differentiated, partially differentiated or undifferentiated hPSCs (bottom panel) in coordination with suicide gene-mediated targeted cell ablation (top panel) at tissue-specific rates in a gradual, multiphasic manner so as to effect the extrinsically mediated turnover of whole tissues and organs. Reprinted and adapted with permission from Rejuvenation Research 19/4, published by Mary Ann Liebert, Inc., New Rochelle, NY. Color images available online at
The aim of ICT within the context of biomedical gerontology is the prevention and/or negation of several forms age-related cellular and intracellular damage (i.e., functionally deleterious phenotypic deviation), including telomere depletion, genomic DNA and mitochondrial DNA damage and mutation, replicative senescence, functionally deleterious age-related changes in gene expression, accumulated cellular and intracellular aggregates, and deleterious post-translationally modified gene products (e.g., glycated and carbonylated gene products). 3 The intervention was introduced in the context of biomedical gerontology, describing strategies to coordinate endogenous cell ablation with exogenous cell administration and to mediate cell type, tissue, and organ-specific ICT rates, addressing a variety of potential complications associated with the intervention (and proposed strategies for their deterrence where possible) and analyzing the potential therapeutic utility of ICT in the content of life- and health-span extension. The aim of the present review is to analyze the potential utility of ICT within the broader context of regenerative medicine and to give an overview of its potential to facilitate in situ whole-tissue and whole-organ replacement.
Any single phase of coordinated endogenous cell ablation and exogenous replacement cell administration is referred to as an ICT iteration, while the sum of ICT iterations comprising the multiphasic induced turnover of a whole tissue or organ is referred to as an ICT round. The use of hPSC-derived cells is specified on the basis that PSCs lack many of the forms of accumulated age-related damage that accumulate in adult somatic cells and adult stem cells. While a variety of options exist for sources of the exogenous PSC-derived cells used throughout a given ICT round, the use of patient-specific human-induced pluripotent stem cells (hiPSCs) generated via nuclear reprogramming or the use of immunologically matched hPSCs from existing hPSC banks is preferred so as to minimize concerns of immunogenicity and the possibility of rejection. To reduce the risk of oncogenesis, hPSCs may need to be differentiated (as far as necessary) along their respective cell-type lineages.
While a number of means exist for targeted endogenous cell ablation, the use of suicide genes is suggested, delivered using either cell type–specific delivery systems (e.g., drug delivery systems containing surface-incorporated homing motifs or liposome-conjugated antibodies) or tissue-tropic adeno-associated viruses (AAVs) carrying suicide genes under the transcriptional control of cell type–specific promoter regions, or a combination thereof, as the preferred means of targeted endogenous cell ablation due to their high level of use, availability, and characterization.
Alternatively, small molecules could be used to ablate cell types selectively by inhibiting the weak link in their survival-signaling network. For example, thrombocytes are known to rely upon BCL-xL, 4 an anti-apoptotic member of the BCL-2 family. Abbvie's chemotherapeutic Navitoclax (ABT-263) is limited by the induction of thrombocytopenia due to the molecule's affinity for BCL-xL. Administration of otherwise salutary senolytics—which selectively kill deleterious senescent cells (defined as p16 positive, senescence-associated beta-galactosidase [SA B-Gal] positive, and possessing a proinflammatory secretome), including BCL-inhibitors such as Abbvie's ABT-263 (Navitoclax), ABT-199 (Venetoclax), ABT-737, dasatinib, quercetin, and others 5 —is hampered by off-target effects in non-senescent cells. Generating more selective inhibitors is an intense area of drug development in oncology and can be repurposed for selective ablation of specific cell types. Specific cell types can be ablated because they depend on different nodes or “weak links” in their apoptotic program. For some cells, it may be Bcl-xL; for others, it may be survivin (BIRC5), NOXA, MDM2/p53, and so forth. Indeed, it should be possible to rank the importance of each cell type's apoptotic signaling protein using inhibitor screening, with each cell type possessing a unique “code” of vulnerable targets. Ultimately, a low dose of a specially optimized cocktail of compounds can be administered, locally or systemically, for selective ablation. This cocktail-based method is already a major area of oncology research. Small molecules tend to lack sufficient specificity, but a promising alternative is the use of peptide mimetics—those that interfere with apoptotic signaling have recently been shown to ablate senescent cells selectively via FOXO4-p53 signaling. 6
Cell type-, tissue-, and organ-specific ICT rates would be applied in accordance with a variety of parameters that affect the likelihood of preserving tissues' structural and functional integrity during the transient loss of a portion of their constituent cells. The extent with which a given cell type contributes to the structural and functional integrity of the tissue or organ determines how many cells can be transiently absent (as well as the spatial distribution of concomitantly absent cells that can be safely sustained by the tissue) without significantly decreasing the functional reserve of the tissue and without incurring substantial risk of acute tissue or organ failure. This varies among different cell types, tissues, and organs, and while ICT rates that are unlikely to result in acute tissue or organ failure can be approximated by referring to the extent with which a given cell type contributes to the structural and functional integrity of a tissue (with respect to its normal functional reserve, the normal homeostatic demands it is subject to, and the mechanical properties of the tissue), the actual optimal applied ICT rates and spatiotemporal distributions must be more confidently determined via preclinical studies measuring the actual effect of different ICT rates and spatiotemporal distributions upon the structural and functional integrity of tissues and organs. Optimal tissue-specific ICT rates and spatiotemporal distributions are also likely to be affected by the specific nature and function of the tissue. For example, it is likely that the kidney would be capable of sustaining a lesser ICT spatiotemporal distribution than other organs due to its specific function, in the sense that the loss of too many cells within too close proximity to one another would compromise the structural continuity of nephrons' tissues, leading to blood leaking out and filtrate leaking in. Thus, a tissue's or organ's ultimate size, gross anatomy and microanatomy, structural integrity, specific function, and functional reserve with respect to the homeostatic demands it is normally subject to must all be considered when determining tissue- and organ-specific ICT rates and spatiotemporal distributions.
While interventions employing aspects of ICT are routinely performed (e.g., bone-marrow transplants in a general sense 7 and the clearance of hematopoietic stem cell [HSC] niches prior to exogenous HSC administration as a preconditioning strategy for bone-marrow transplants in a more specific sense), 8,9 these interventions have yet to be applied to solid tissues and organs, and several fundamental components of ICT remain to be integrated into these techniques. These include the gradual clearance of cells coordinated with exogenous cell administration in a multiphasic fashion so as to limit the quantity of cells transiently absent at any one time in an attempt to maintain the structural and functional integrity of tissues and organs at all times throughout their induced turnover. The gradual, multiphasic coordination of targeted endogenous cell ablation with exogenous cell administration are the distinguishing characteristics of ICT, and are likely to be necessitated when applied to solid tissues and organs (i.e., tissues and organs in which the absence of a large-enough population of cells would have an immediate impact on the tissue's homeostatic integrity).
The levels of age-related cell loss and atrophy experienced by tissues and organs throughout development and aging attest to the fact that tissues and organs can sustain certain levels of cell loss before experiencing tissue and organ failure as a result. While the levels of transient cell loss necessitated by ICT would lead to a decrease in the reserve capacity of tissues and organs, it would not necessarily lead to acute tissue and/or organ failure, provided that the degree and spatiotemporal density of cell loss is sufficiently minimized by increasing the total number of phases comprising the cumulative procedure.
The therapeutic scope of ICT extends beyond the field of biomedical gerontology to potentially encompass a wider variety of diseases and conditions rooted in cellular and intracellular abnormalities that are traditionally viewed as targets of regenerative medicine. ICT aims to combine several of the features and therapeutic utilities of cell-based therapies, on the one hand, and tissue engineering, on the other, so as bridge the gap between these two main pillars of regenerative medicine.
Ict As a Novel Therapeutic Modality in Regenerative Medicine
Regenerative medicine comprises two main approaches to the maintenance and restoration of tissue function: cell therapy 10 –12 and tissue engineering. 13 –15 Like cell therapy, ICT aims to restore tissue and organ function by supplementing pathological cells with cells free of pathology and dysfunction. Similarly, like tissue engineering, ICT aims to restore tissue and organ function through the effective replacement of whole organs and tissues. However, unlike standard cell therapies, ICT aims to replace whole organs and tissues at the cellular level (rather than supplement the function of lost, diseased, and/or dysfunctional endogenous cells), and unlike tissue and organ engineering, it aims to replace whole tissues and organs in a gradual, multiphasic manner. By combining several features of these two pillars of regenerative medicine, ICT serves as a novel strategy to accomplish the aims of each respective approach—the restoration of function within damaged and diseased organs and tissues—while potentially remaining free of some of their respective drawbacks and inherent limitations.
ICT and tissue engineering
Tissue engineering faces several technical barriers that are absent from standard cell therapies. One such drawback is the need for surgery, which increases the necessary physiological stress placed upon patients. Another drawback in the specific case of engineered tissues and organs using exogenous and synthetic scaffolds at their current state of development is insufficient homology to the anatomy and tissue ultrastructure of the patient's removed endogenous tissue or organ.
In the case of decellularized and recellularized engineered tissues and organs, 16 –20 existing decellularization techniques are based upon cell lysis, which can allow cellular debris to absorb into the extracellular matrix (ECM), raising concerns of immunogenicity. Meanwhile, existing decellularization techniques are also known to degrade certain components of the ECM, 21 which introduce structural and mechanical abnormalities to the ECM that impact cell adhesion, and biochemical abnormalities in the ECM that could interfere with both cell–ECM signaling, as well as cell–cell communication. The decellularization efficiency varies between different decellularization protocols, and each approach affects the biochemical composition, tissue ultrastructure, and mechanical behavior of the decellularized ECM by varying degrees. 22
By contrast, ICT necessitates neither surgery nor an interim period during which the homeostatic functions of the removed tissue and organ are absent (Fig. 2). While the transplantation of many solid organs has become a routine procedure, this largely applies to solid organs that are not as intricately connected to other tissues, organs, and organ systems. In the context of distributed tissue systems and specialized tissues with more intricate connections with other proximal tissues, surgery poses more of a hazard in terms of reestablishing a functionally sufficient connection between the transplanted organ and other tissues, organs, and organ systems to which it is structurally and functionally connected. This is particularly true for distributed tissues, including the vasculature, lymphatic system, and skin. For example, rejuvenating the lymph nodes by surgically removing and implanting the ductal lymphatic system would be impractical. Selectively ablating and replacing different lymphatic cell types sequentially enables the repair of a distributed tissue system while minimizing functional impairment.
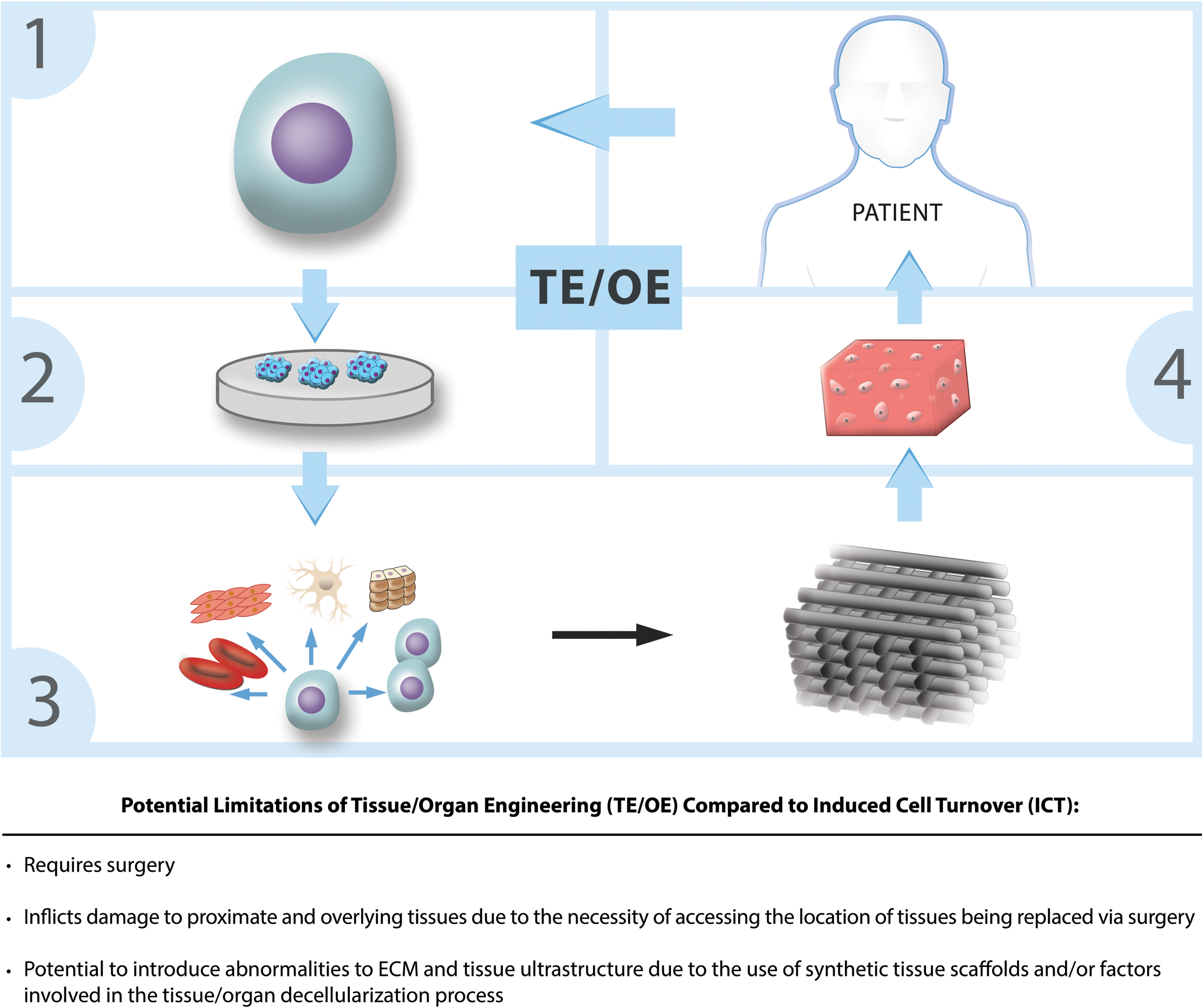
Comparison between ICT and tissue/organ engineering, and a schematic representation of tissue/organ engineering as applied for therapeutic purposes. (1) Derivation of hPSCs. (2) Culturing of hPSCs to produce a sufficient quantity of exogenous cells for use in seeding an engineered (i.e., synthetic) scaffold or a decellularized tissue or organ. (3) Seeding of directionally differentiated, partially differentiated, or non-differentiated hPSCs onto the synthetic or decellularized scaffold. (4) Transplantation of seeded scaffold into the patient. Color images available online at
Additionally, ICT is unlikely to be hampered by the potential problems of introducing biochemical, tissue ultrastructural, or mechanical abnormalities in the ECM because it utilizes induced apoptosis, a highly conserved and highly regulated (i.e., relatively clean) form of programmed cell death with minimal inflammation. Another potential limitation of engineered tissues and organs absent in the context of ICT is the fact that an engineered tissue's constituent cells are grown in an exogenous environment isolated from the recipient's circulatory and endocrine systems. In contrast, cells administered during the course of ICT would be exposed to the recipient's circulatory system from the beginning and may be more likely to proliferate, migrate, and integrate normally as a result.
ICT and standard cell therapies
Cell therapies suffer from low levels of long-term engraftment, 23,24 which among other factors is thought to result from a lack of niche vacancy. 8,25 –28 The levels of cell engraftment attainable by standard cell therapies are constrained by the existing degree of cell loss in the targeted tissue or organ, as well as by the proportion of vacancies (i.e., that have not become occupied by ECM or fibroblasts). This limits the clinical efficacy of cell therapies to the levels of long-term engraftment and retention they can achieve (i.e., by providing additional homeostatic function and support at the locations in which they can engraft) and to the extent with which engrafted cells can provide paracrine effects and trophic support on remaining in situ diseased and dysfunctional cells. 29 –31 By contrast, ICT aims to remove diseased and dysfunctional cells systematically so as to create vacancies in which administered exogenous cells can localize and engraft in a gradual, multiphasic manner such that the levels and spatiotemporal density of cell loss at any one time do not destabilize the structural and functional integrity of tissues to the point of acute tissue and organ failure (Fig. 3). Furthermore, historical instances of cell therapy have witnessed dramatically improved engraftment rates as a result of utilizing endogenous cell clearance, 8,32 substantiating the improved long-term engraftment efficacy reasonably presumed to also coincide with ICT. Cell engraftment efficiency in ICT may also be superior to standard cell therapy because exogenous cells are administered immediately after their cognate endogenous cells are ablated, thereby minimizing the time available for fibrosis or other processes that block engraftment long after tissue damage has occurred. 20,21
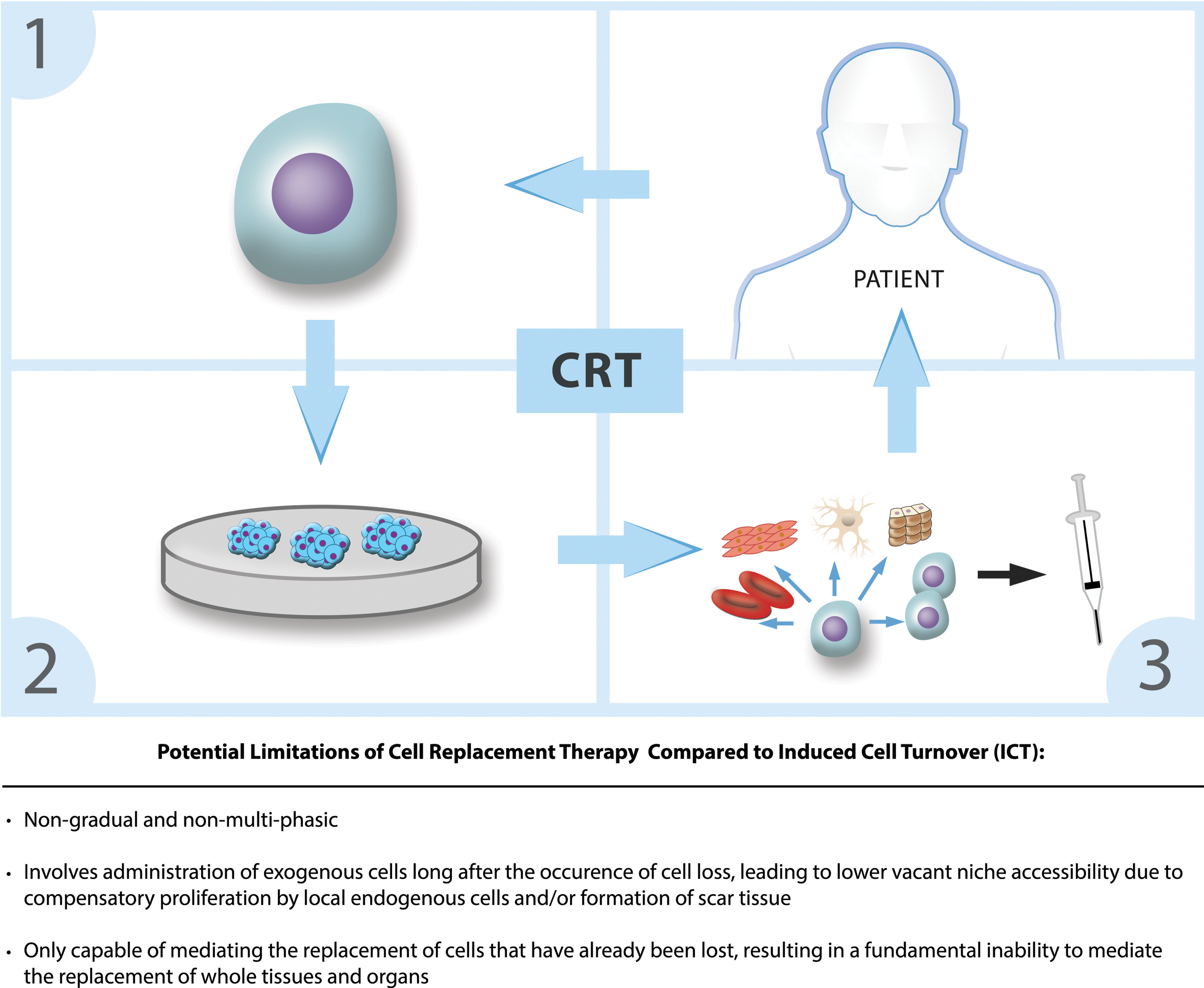
Schematic representation of standard cell therapies (i.e. cell replacement therapy [CRT]) and a comparison between ICT and CRT. (1) Derivation of hPSCs. (2) Culturing of hPSCs to produce a sufficient quantity of exogenous cells. (3) Administration of directionally-differentiated, partially-differentiated or non-differentiated hPSCs in a non-gradual and non-multi-phasic manner without quantitative and qualitative coordination of targeted endogenous cell ablation. Color images available online at
Inflammation, Necrosis, Hypoxia, and Fibrosis As Specific Barriers to Cell Engraftment in the Context of Ict
In the specific case of diseased and injured tissues, additional methodological strategies and approaches to the preparation of the exogenous cells administered each ICT iteration (cell preconditioning) as well as the diseased tissue or organ microenvironment (tissue preconditioning) could enhance the engraftment efficacy of cells administered in the context of ICT.
ICT in hypoxic and necrotic tissue microenvironments
Cell preconditioning strategies aim to increase cell survival and retention in hypoxic, necrotic, fibrotic, and inflamed tissue microenvironments. These broadly include exposing cells to sub-lethal insults, cell preconditioning mediators, and the use of specific pharmacological agents in vitro prior to in vivo administration. 33,34 Such strategies typically aim either to enhance the intrinsic homing, engraftment, and/or survival capacities of administered exogenous cells or to acclimate them to the hostile tissue microenvironment that they are likely to encounter. Cell preconditioning strategies that involve exposing cells to sub-lethal insults include simulated ischemia, hypoxia, anoxia, and nutrient deprivation, which have been shown to increase survival and paracrine factors in vivo in rats, 35 –43 as well as heat shock 44 and carbon monoxide exposure, 45 which have been shown to increase cell survival and trophic support via secretion of paracrine factors in rats. By contrast, treating cells with antioxidants (e.g., high-density lipoprotein 46 and curcumin) 47 has been shown to enhance exogenous cell survival by protecting cells from oxidative stress-induced apoptosis.
Additionally, preconditioning mediators, including hydrogen sulfide, 48 insulin-like growth factor 1, 49,50 fibroblast growth factor 2, 50 transforming growth factor alpha, and tumor necrosis factor alpha, 51 have been shown to increase cell survival, migration, and paracrine factors in rats. Enhancement of cell homing capacity and engraftment efficacy has also been demonstrated via the use of cell-conditioned media that incorporate components present in the targeted tissue microenvironment (e.g., fibronectin and laminin), 52,53 presumably acclimating them toward the recognition and successful interaction of such components in vitro prior to being exposed to them in the in vivo environment. The majority of the above cell preconditioning strategies have been shown in both preclinical and clinical settings to enhance cell engraftment and cell survival.
While many of the above-mentioned studies have focused on the use of preconditioned muscle stem cells using heart disease models due to the high prevalence of hypoxia and necrosis present in heart disease, it is likely that such preconditioning strategies would also prove useful as preconditioning strategies for other stem cell and progenitor cell types.
ICT in inflammatory and immunoreactive tissue microenvironments
The presence of inflammatory cytokines (e.g., interleukin-1α/β, tumor necrosis factor alpha, and SDF-1α) in inflamed tissue microenvironments also poses a unique barrier to cell engraftment, survival, and retention by promoting the destruction of administered PSCs by endogenous immunoreactive cells. An emerging strategy to combat barriers to cell engraftment, survival, and retention specific to inflammatory tissue microenvironments is the prior administration or co-administration of inhibitors and/or receptor antagonists to these immunological mediators with the aim of transiently decreasing their prevalence within the targeted tissue microenvironment during the homing and engraftment of administered cells. 54
ICT in fibrotic tissue microenvironments
In terms of unique barriers to cell engraftment posed by fibrotic tissue microenvironments, the administration of ECM-degrading factors such as matrix metalloproteinase 9 to the targeted tissue environment prior to exogenous cell administration has been shown to reduce fibrosis and to enhance engraftment efficacy in subsequently administered progenitor cells in mice, and could be used as a strategy to reduce the extent of the barrier to cell migration and engraftment posed by a fibrotic target tissue microenvironment in diseased and injured tissues in the context of ICT. 55 Additionally, local irradiation of the targeted tissue has been shown in animal models to reduce disease and injury-associated inflammation and fibrosis, 56 and ultrasound-target microbubble destruction has been shown in animal models to increase vessel permeability, 57 increasing cell engraftment and retention in both cases. The administration of growth factors to the tissue microenvironment prior to exogenous cell administration has also been shown to enhance cell survival and retention. 50
General strategies to enhance cell engraftment in the context of ICT
Homing enhancement has just begun to be explored (e.g., in the context of HSC transplantation in murine models), including the upregulation of cell adhesion molecules in transplanted PSCs and in the cells residing in the targeted tissue microenvironment, the upregulation of transplanted PSC homing molecules, and the upregulation of secreted chemotactic factors, so as to increase the homing and engraftment capacity of administered PSCs. 58 Additionally, recent efforts in screening for signal transduction modulators that enhance cell homing and engraftment (e.g., factors that increase surface expression of homing molecules that bind to intercellular adhesion molecule 1) represent an additional emerging cell preconditioning strategy to enhance cell homing and engraftment, 59 but have yet to be tested in a clinical setting. These broader strategies to enhancing PSC homing and engraftment represent an additional strategy to increase the homing and engraftment of PSC-derived cells administered in the context of ICT that are independent of any specific barriers to engraftment posed by hostile tissue microenvironments.
Potential Ict-Specific Complications and Logistical Challenges
While an overview of various potential complications and therapeutic challenges (and possible strategies for their deterrence) specific to ICT elsewhere (Table 1) has been given, several additional potential complications and therapeutic challenges unique to ICT are highlighted below that have not yet been adequately addressed elsewhere. These include: (a) strategies of coordinating the quantity of administered exogenous cells with the quantity of terminated endogenous cells during each ICT iteration; (b) strategies to overcome difficulties associated with the repeated administration of cells, suicide gene vectors for solid organs lacking easily accessible delivery routes; and (c) strategies to avoid overwhelming the patient's phagocytotic capacity due to the induced apoptosis of too large a quantity of cells during each ICT iteration.
Potential ICT-specific complications
ICT, induced cell turnover; hPSC, human pluripotent stem cell.
Quantitative coordination of exogenous cell ablation with endogenous cell administration
ICT necessitates that the quantity and cell type of ablated endogenous cells matches the quantity and cell type of administered hPSC-derived exogenous cells. The most detrimental possible consequence of failing to coordinate these two parameters would be to ablate more endogenous cells than are replaced via administered exogenous cells during each ICT iteration, potentially leading to cumulatively increasing levels of cell loss for each successive ICT iteration that is performed. Another possible detrimental consequence is the administration of more exogenous cells than is required to replace the endogenous cells ablated in each ICT iteration, although this would merely lead to those excess exogenous cells eventually undergoing apoptosis and/or phagocytosis by resident phagocytes.
In general, assuming levels of suicide gene transduction efficiency and exogenous cell engraftment efficiency approaching 100%, the mere coordination of the suicide gene dose delivered during each ICT iteration with the cell type and quantity of exogenous cells delivered during each ICT iteration would accomplish the quantitative and qualitative coordination of exogenous cell administration with endogenous cell ablation. In practice, however, both ablation efficiency and exogenous cell engraftment efficiency would not approach 100%, and would have distinct efficiencies that may vary among different tissues and cell types. Elsewhere, it has been proposed that if ablation efficiency and the exogenous cell engraftment efficiency were known (i.e., determinable via preclinical studies) for each distinct tissue and cell type, varying either the per-iteration dose of administered suicide genes or the per-iteration dose of administered exogenous cells could be used to match the two parameters quantitatively, despite non-negligible discrepancies between observed ablation efficiency and observed engraftment efficiency. 1
An alternative strategy would be to administer excess stem cells so that the ablation step is rate limiting—it is better to provide too many cells than to kill off too many. Such a strategy would at worst lead to an excess of exogenous cells, resulting in their eventual clearance. Furthermore, even in the absence of such strategies, in the case of mitotic cell types, it is possible that an excess of ablated endogenous cells with respect to the quantity of successfully engrafted exogenous cells would be compensated for via compensatory proliferation of local differentiated cell types and/or cognate adult stem cells within the resident tissue. For these reasons, the challenge of quantitatively coordinating the per-iteration quantity of ablated endogenous cells with the per-iteration quantity of administered exogenous cells is considered to be a surmountable therapeutic challenge, albeit one requiring further study into the observed efficiency of these two parameters and the feasibility of methods to coordinate these parameters in the face of observed discrepancies between them.
Another complimentary approach would be to determine the degree of cell ablation non-invasively, which would then be used to determine the dose of exogenous cells to be administered during that ICT iteration. Such an approach would be inadvisable due to the necessity to administer exogenous cells following suicide gene administration, update, and integration, and following endogenous cell ablation, rather than co-administering exogenous cells with the suicide genes being delivered during that particular ICT iteration or administering exogenous cells shortly before suicide gene administration. Doing so would prolong the period in which cells are required to be transiently absent within the tissue, and risks the potential for the loss of cells in the resident tissue to be compensated for by proliferation of either local differentiated mitotic cells or cognate adult stem-cell types within the resident tissue, before the administered exogenous cells have time to migrate toward their intended sites of engraftment and subsequently engraft in the vacated niches of their cognate ablated endogenous cell types. As such, we propose that the use of such a strategy poses undue risk with respect to the potential utility it might have in terms of matching the per-iteration quantity of endogenous cell ablation with the per-iteration quantity of exogenous cell administration and engraftment.
Minimizing difficulties associated with the repeated administration of cells, suicide genes, and reagents in solid tissues
The multiphasic nature of ICT enables gradual ablation and replacement. While this presents no problems for non-solid tissues such as blood, the repeated administration of cells and suicide gene vectors in solid tissues and organs, especially as it concerns solid organs lacking easily accessible delivery routes, presents unique therapeutic challenges. As discussed elsewhere, for these reasons, the systemic administration of suicide gene vectors and exogenous cells is preferred wherever possible. 3 In the case of differentiated cell types that are too large to pass through capillaries, the use of either undifferentiated hPSCs or minimally differentiated stem and/or progenitor cell types can be employed to circumvent the issue, provided that reasonably robust methods of preventing hPSC-associated tumorigenesis are also employed.
However, in order to account for instances where local administration is necessary, several strategies are outlined to enhance the feasibility of repeated local cell and suicide gene administration in solid tissues and organs. Specifically, it is proposed that the use of implanted delayed-release drug and/or cell encapsulation devices be employed to achieve sustained long-term release of both exogenous hPSC-derived cells and suicide gene vectors.
Live cell encapsulation devices are traditionally meant to facilitate the two-way transfer of cellular gene products (e.g., therapeutic proteins) to the exterior of the encapsulation device, and oxygen and nutrients between the interior of the encapsulation device and the surrounding tissue microenvironment, as well as to provide an immunological barrier to prevent the implanted cells from being terminated by the host immune system. 60 –65 As such, they are not traditionally envisioned as a means of releasing cells into the surrounding microenvironment at all. However, the application of sustained drug release technologies for the purpose of gradual, controllable, and/or sustained release of cells so as minimize the repeated administration of cells is, while certainly conceivable as a general area of future study and experimentation, almost completely lacking in clinical and preclinical precedent.
In the context of such a strategy, the implantation of a set of degradable (e.g., polymer) live cell encapsulation devices (hereafter referred to as cell carriers) is proposed, modeled after sustained biodegradable and/or bioerodable drug release devices, 66 –69 all carrying the same cell type(s) and all implanted within the same resident tissue for each distinct cell type in the tissue undergoing ICT. Distinct subsets would have different degradation and/or erosion rates, such that each successive subset releases their encapsulated cells at a later time following implantation than the previous subset. The degradation coefficient of degradable and erodible drug carriers is modifiable through a number of means, including the use of distinct encapsulation matrix thicknesses, the use of encapsulation matrixes composed of materials possessing distinct molecular weights, and the incorporation of materials within the encapsulation matrix that are known to slow its degradation rate. Such carriers would ideally be modeled after chemically controlled (i.e., biodegradable or bioerodable), as opposed to diffusion-controlled, osmotically controlled, or externally triggered (e.g., pH or temperature-controlled) sustained drug release systems.
It is important to note that the mode of release used by such cell carriers would be dissimilar to traditional modern-day sustained drug release devices. Most modern-day sustained drug delivery systems release drugs through either diffusion or polymer degradation, and in the latter case the drug is often homogeneously distributed throughout the encapsulation matrix to achieve continuous (i.e., non-pulsatile) drug release curves. However, the unique requirements of live cell encapsulation preclude both diffusion through the encapsulation matrix and homogenous distribution within the encapsulation matrix itself. For the purposes of sustained live cell release, the encapsulation matrixes should degrade or erode via bulk degradation or bulk erosion, wherein the encapsulation matrix is continuously degraded or eroded within the body until enough of the encapsulation matrix is degraded or eroded in order to permit the release of the encapsulated cells. This strategy would enable concentrated pulses of live cell release, wherein the cells in a given encapsulation device would be released approximately simultaneously. Another important consideration is the fact that the unique requirements of live cell encapsulation would necessitate modifications to the geometric design of the encapsulation matrixes, such as the use of thin non-erodible sections of the matrix that allow the constant diffusion of gases and nutrients across the encapsulation matrix, or the use of perforations within the matrix that allow for the diffusion of gases and nutrients but that are small enough to preclude the translocation of encapsulated cells through such perforations.
The use of dissimilar encapsulation matrix thicknesses (or other methods mentioned above, including the use of encapsulation matrix materials with varying molecular weights and/or the incorporation of materials known to prolong the normative degradation rate of the material otherwise comprising the encapsulation matrix) would permit differential lengths of time between implantation within the body and encapsulated live cell release for each distinct subset of each distinct tissue and cell type–specific set of cell carriers. Furthermore, the maximum attainable length of time it takes to erode the encapsulation matrix sufficiently can be made to be fairly high. In practice, sustained drug release using degradable and/or erodible polymer drug carriers has been achieved over a period of years (e.g., poly-ɛ-caprolactone [PCL] drug carriers have been observed to degrade over a period of 3 years in rats), 70 but theoretically could be expanded to an even greater period by modifying the size, thickness, molecular weight, and composition of the encapsulation matrixes employed.
The same general approach could be applied to the release of suicide genes and other reagents discussed above via sustained release gene delivery systems. 71 –75 However, it is important to note that the use of implanted sustained release drug delivery systems would be advantageous and, indeed, perhaps necessary in the context of the central nervous system, where in contrast to stem cells (e.g., neural and mesenchymal stem cells), which have been shown capable of crossing the blood–brain barrier (BBB), 76 the passage of other therapeutic agents is generally blocked. Alternatively, however, the use of approaches that have been shown to allow viral and non-viral gene vectors to cross the BBB could be employed to avoid the use of sustained gene delivery devices within the CNS, such as the use of transport vectors (including endogenous peptides, modified proteins, and/or peptidomimetic monoclonal antibodies) 77 and the use of recombinant AAVs modified via Cre recombination-based AAV targeted evolution. 78,79
Overwhelming the patient's endogenous phagocytotic capacity
Can the endogenous target cell die-off create cell debris (i.e., apoptotic bodies) sufficient to overwhelm endogenous phagocytes? The levels of endogenous cell death necessary to facilitate whole-tissue and whole-organ ICT depends on the applied tissue- and organ-specific ICT iteration frequency (i.e., the duration of time between two successive ICT iterations within the same tissue or organ), ICT iteration magnitude (i.e., the number of endogenous cells ablated during the same ICT iteration within the same tissue or organ), and ICT iteration spatial distribution (i.e., the spatial distribution of cells ablated during the same ICT iteration within the same tissue or organ) with respect to the maximum number of cells of a specific cell type that can be concomitantly absent from their resident tissue without reducing the functional and structural integrity of their resident tissue to the point of causing acute tissue or organ failure. A lack of enough phagocytes to sustain such levels of endogenous cell death could result in the inadvertent efferocytosis of the resulting apoptotic bodies by other non-phagocytotic endogenous cells, which could lead to detrimental consequences for those cells, such as a phenomenon that has elsewhere been referred to as an “inadvertent bystander effect,” whereby efferocytosis of the apoptotic bodies resulting from a given ICT iteration results in the uptake of either suicide gene products or components of the apoptotic cascade (e.g., caspases, cytochrome C, APAF-1, and pro-apoptotic BCL factors).
The avoidance of necrosis, necroptosis, or any form of cell death that causes a chain reaction of local cell death is absolutely critical. Elsewhere, several candidate solutions to the potential problem of an inadvertent bystander effect have been suggested, including: (1) co-administration of exogenous hPSC-derived phagocytes along with replacement hPSC-derived cell types administered during each ICT iteration, and (2) potentiation of the production of additional endogenous phagocytes via co-administration of mitogens carried by cell type–targeted drug delivery systems during each ICT iteration, which are targeted toward phagocytotic cell types. Furthermore, it has been estimated that approximately 50–70 billion cells die via apoptosis per day in the average adult human body. 80 Take the liver for example, which has been estimated to comprise roughly 361 billion cells. 81 If ICT were performed on the liver over the course of 40 ICT iterations (terminating approximately 0.9 billion cells each ICT iteration) and the quantity of hPSC-derived exogenous cells and suicide genes used throughout each ICT iteration over the course of a day was administered, this would result in the apoptosis of <2% of the lower bound of endogenous cells apoptosed that day (i.e., 50 billion cells) through normal tissue renewal according to the above estimate. However, terminating 1/40th of the cells comprising a given tissue or organ during a given ICT iteration is likely to result in a decrease in the homeostatic integrity of that tissue or organ by an amount that risks acute tissue or organ failure. This example illustrates the presumption that the termination of too great a quantity of endogenous cells during a given ICT iteration is likely to risk homeostatic collapse of that tissue or organ long before it is likely to risk overwhelming the endogenous phagocytotic capacity of the patient. Nonetheless, this is a potential complication that should be analyzed during preclinical and clinical studies to determine the actual likelihood and prevalence of this potential complication.
Conclusion
The promise of ICT has been illustrated, and it is hoped that further investigation has been inspired into its utility as a novel therapeutic modality in regenerative medicine and its utility in mediating in situ tissue replacement without the need for surgical transplantation. The novelty of ICT lies in the coordinated ablation and replacement of specific cell types, particularly in tissues that are not amenable to ex vivo production and surgical transplantation, in a gradual and multiphasic manner and at cell type-, tissue-, and organ-specific rates. Furthermore, a barrier to clinical application of senolytic interventions is the failure of old stem-cell niches to repopulate their tissue after senescent cell clearance. The risk of excessive ablation may be balanced by the provision of exogenous cell therapy, perhaps even with suprafunctional engineered cells. Complimentary lines of research on targeted apoptosis in oncology and senolytics may be coupled with impressive advances in cell therapy to yield a modality offering synergistic regenerative benefit to an aging global population.
Footnotes
Acknowledgments
The authors would like to thank João Pedro de Magalhães, PhD, Alex Zhavoronkov, PhD, Marios Kyriazis, MD, MIBiol, CBiol, and William Bains, PhD, for their critical reading of the manuscript, and Sandor Ligetfalvy for assistance in the preparation of the figures.
Author Disclosure
F.C. and G.S. have filed a patent application relating to the present article. No competing financial interests exist for S.A.