
Abstract
Patients with unresectable advanced soft-tissue sarcomas (STS) receiving radiotherapy or/and chemotherapy still have a poor prognosis. This study aimed to evaluate retrospectively the efficacy and safety of recombinant adenovirus-p53 (rAd-p53) gene therapy combined with radiotherapy and hyperthermia for advanced STS. A total of 71 patients with advanced unresectable STS treated at the authors' center from April 2007 to November 2014 were included. Of these 71 patients, 36 cases received rAd-p53 therapy combined with radiotherapy and hyperthermia (p53 group), while 35 cases received radiotherapy and hyperthermia alone (control group). Short-term therapeutic efficacies, long-term survival outcomes, and adverse events were evaluated and compared between groups. Compared to the control group, the p53 group had a significantly higher disease control rate (83.33% vs. 54.29%; p = 0.008) and a lower progressive disease rate (16.67% vs. 45.71%; p = 0.018). In addition, rAd-p53 treatment significantly improved the progression-free survival and overall survival of STS patients. Cox regression indicated that rAd-p53 treatment significantly reduced the risks for disease progression or death event for STS patients. Furthermore, there was no significant difference in all adverse events, except for transient fever, which occurred in 89% of patients with rAd-p53 therapy. rAd-p53 combined with radiotherapy and hyperthermia can effectively improve the therapeutic efficacy and survival outcomes in patients with advanced unresectable STS, providing a new therapeutic strategy.
Introduction
S
Currently, surgical resection is still the standard treatment for primary STS, while pre‐ or postoperative radiotherapy and chemotherapy are used as adjuncts to surgery for patients with locally advanced or metastatic disease. 6 However, even after optimal treatment with surgery alone or multimodality treatment, a significant proportion of patients with STS still develop disease recurrence. It has been shown that 10–20% of patients with extremity STS treated with radical resection and adjunctive radiation therapy still develop a local recurrence within 5 years after the initial treatment. 7,8 A large multicenter trial reported that STS patients receiving optimal local treatment (surgery with or without radiotherapy) still had a local recurrence rate of 24% at 5 years. 9 Local recurrence has been shown to be a crucial risk factor associated with decreased OS. 10 On the other hand, patients with unresectable STS should be treated with radiotherapy or/and chemotherapy. 11,12 Nevertheless, patients with unresectable advanced STS receiving radiotherapy or/and chemotherapy still have a poor prognosis. 13,14 This phenomenon may be attributed to the fact that STS is relatively resistant to irradiation and/or chemotherapy. 15 In addition, radiation damage to adjacent organs also limits the delivery of adequate-dose radiotherapy after resection of most retroperitoneal/visceral tumors. 16 Therefore, new and effective methods for the treatment of STS are urgently required.
p53 is a well-documented tumor suppressor gene encoding a nuclear phosphoprotein, which plays important cellular functions. 17 When the p53 gene is deleted or mutated, the cells are incapable of proliferation, DNA repair, and apoptosis, and eventually cancer is induced. 18 The mutation or deletion of p53 gene has been shown to play a crucial role in the tumorigenesis of a variety of malignancies. 19 In STS, the reported p53 mutation rates range from approximately 16% to 24%. 15,20 Furthermore, p53 mutation in STS has been shown to be associated with the occurrence of relapses and lymph node metastases. 15 These findings suggest that p53 plays an important role in tumorigenesis of STS, and could be a potential therapeutic target. Previous studies have demonstrated that recombinant adenovirus-p53 (rAd-p53) transduction can enhance the sensitivity of human cancer cell lines to both radiotherapy 21 and chemotherapy. 22 As for STS, Ganjavi et al. demonstrated that rAd-p53 transduction sensitizes STS cell line to chemotherapy, 23 indicating that rAd-p53 gene therapy may possess the capacity of improving the therapeutic outcome of radiation and chemotherapy for STS.
The clinical-grade rAd-p53 injection (Gendicine®) was developed by Shenzhen SiBiono GeneTech Co. Ltd., China, and was approved by the China State Food and Drug Administration (SFDA) in 2003 for intratumoral gene therapy for unresectable head and neck squamous-cell carcinoma (HNSCC). 24 Since then, a number of clinical trials have been carried out for gene therapy involving a variety of cancers. 25 Among these trials, gene therapy was combined with surgery, chemotherapy, and/or radiotherapy for patients with advanced or unresectable cancers, and satisfactory outcomes were observed in these clinical trials, that is, rAd-p53 treatment improved the overall response rates and survival rates. 25 Previous studies have shown that rAd-p53 combined with radiotherapy can improve local control and survival rate in patients with nasopharyngeal carcinoma and pancreatic cancer. 26 –28 However, the therapeutic efficacy of rAd-p53 gene therapy for STS remains to be investigated.
In the authors' hospital, rAd-p53 gene therapy has become a therapeutic option for unresectable advanced STS since October 2003. Hence, the purpose of this study was to evaluate the safety and efficacy of rAd-p53 gene therapy combined with radiotherapy and hyperthermia for unresectable STS.
Materials and Methods
rAd-p53 for gene therapy
rAd-p53 (Gendicine®, purchased from China Shenzhen SiBiono GeneTech Co., Ltd, China) is a recombinant replication-incompetent human serotype 5 adenovirus, in which the E1 region is replaced by a human wild-type p53 expression cassette. Its genome does not integrate into host genome DNA, and does not impair any normal cells. rAd-p53 was stored at −20°C at a concentration of 1 × 1012 virus particles (vp)/mL. The rAd-p53 solution was thawed and diluted moderately in physiologic saline according to tumor size 30 min before use.
Patients
A total of 71 patients with advanced unresectable STS treated at the authors' center from April 2007 to November 2014 were included in this study. The inclusion criteria were: (1) histologic diagnosis of STS; (2) primary or recurrent unresectable tumors with poor or no response to chemotherapy treatment; (3) aged 18–75 years; (4) initial treatment with radiotherapy and hyperthermia judged to be the accepted standard of care; (5) life expectancy of ≥6 months; (6) a Karnofsky performance score of ≥70; (7) adequate bone-marrow function (WBC count ≥4.0 × 109/L; hemoglobin ≥7 g/L; platelet count ≥70 × 109/L); and (8) adequate liver and renal function (aspartate transaminase [AST], alanine transaminase [ALT], blood ureanitrogen, and creatinine <1.5 times the upper limit of normal). The exclusion criteria were: (1) pregnant or nursing women; and (2) uncontrolled serious infections or serious heart and lung failure.
This study was originally designed as a randomized controlled trial. A total of 71 patients were recruited and randomized into the p53 group (n = 35) and the control group (n = 36). However, two patients in the p53 group refused p53 gene therapy due to the economic constraint, while three patients assigned to the control group insisted on receiving p53 gene therapy. Therefore, this study was a prospective, controlled non-randomized trial. Thirty-six cases receiving rAd-p53 therapy combined with radiotherapy and hyperthermia were designated as the p53 group, while 35 cases receiving radiotherapy and hyperthermia alone were designated as the control group. This study was approved by the Institutional Review Board of the authors' hospital. Written informed consent was obtained from all the patients.
rAd-p53 gene therapy
Among the 36 patients in the p53 group, 34 received rAd-p53 by intratumoral injection at multiple sites at a dose of 1 × 1012 vp/2 mL under the guidance of ultrasound or computed tomography (CT). The other two cases were administered with rAd-p53 by intracavitary perfusion to pelvic-cavity tumors at doses of 1 × 1012 vp and 2 × 1012 vp. All patients were administered once a week (every Friday).
Radiotherapy
Patients in the p53 group started to receive radiotherapy 3 days (the next Monday) after rAd-p53 treatment. The radiotherapy was also started in the control patients 3 days after the gene therapy of the p53 group. For both groups, the same irradiation technique was administered, using three-dimensional conformal radiotherapy (3D-CRT) or intensity-modulated radiotherapy, with the conventional fractionation of 2 Gy by high energy (6 MV or 10 MV) accelerator photons, once a day, 5 days a week, Monday to Friday.
Hyperthermia therapy
All 71 patients received hyperthermia therapy after radiotherapy. Patients with superficial tumors received hyperthermia at 43–44°C using a 915 MHz microwave machine, while those with deep-seated tumors received hyperthermia at 42–43°C using a 41 MHz radiofrequency machine for 40–60 min, once a week
Tumor assessments and data collections
Each patient's performance status was evaluated by the Eastern Cooperative Oncology Group (ECOG) scale. 29 Tumor assessments by CT or magnetic resonance imaging scans were performed before treatment, at 2 months post treatment, and then at intervals of 3 months within 3 years post treatment, and thereafter at intervals of 6 months. Treatment response was assessed according to the Response Evaluation Criteria in Solid Tumors (RECIST) v1.1. 30 Briefly, a complete response (CR) was defined as disappearance of all target lesions. A partial response (PR) was defined as at least a 30% decrease in the sum of diameters of viable (enhancement in the arterial phase) target lesions, taking the baseline sum of the diameters of target lesions as the reference. Stable disease (SD) was defined as neither sufficient shrinkage to qualify for PR nor sufficient increase to qualify for progressive disease (PD), taking as reference the smallest sum diameters while on the study. PD was defined as an increase of at least 20% in the sum of the diameters of viable (enhancing) target lesions, taking the smallest sum of the diameters of viable (enhancing) target lesions recorded since the treatment started as the reference.
OS was calculated from the initially diagnostic date to the date on which the patient died or the date of the last follow-up. Progression-free survival (PFS) was calculated from the first day of radiotherapy to the date of disease progression, the date of the last follow-up, or death.
Adverse event determinations
Patients were monitored for adverse events. Adverse event determinations were conducted weekly according to the Common Terminology Criteria for Adverse Events (CTCAE) v4.0. Toxic and adverse events were assessed as light (grade 1), mild (grade 2), serious (grade 3), and life-threatening (grade 4). Particular attention was paid to body temperature.
Statistical analysis
The distributions of age and tumor size, AST, and ALT were skewed or without assumed normality. Therefore, these variables were presented as median (interquartile range), while radiotherapy dose and hyperthermia times were presented as mean ± standard deviation. All continuous data were compared with the Mann–Whitney U-test. Categorical data between groups were examined with either the chi-square test or Fisher's exact test if cell expected values of <5 were found. PFS and OS were analyzed using the Kaplan–Meier survival function and compared by the log-rank test. Predictors associated with PFS and OS were investigated by both univariate and multivariate Cox regression models and indicated with a hazard ratio (HR) and its 95% confidence interval (CI). All calculations were performed using IBM SPSS Statistics for Windows v20.0 (IBM Corp., Armonk, NY). A p-value of <0.05 was considered to be statistically significant.
Results
Demographic and clinical characteristics
All patients with primary or recurrent tumors with sizes ranging from 3.4 cm × 2.6 cm to 15.2 cm × 9.7 cm. The demographic and clinical characteristics of patients are summarized in Table 1. There were no significant differences in age, sex, ECOG scales, tumor site, tumor stages, tumor size, histologic subtypes, pretreatment status, or ALT and AST values between the p53 and control groups (p > 0.05). Regarding radiotherapy, the p53 group received a mean total radiation dose of 56.3 ± 9.0 Gy (36–70 Gy) in 18–35 fractions, while the control group received a mean total radiation dose of 58.1 ± 8.9 Gy (40–72 Gy) in 20–36 fractions. There was no significance in the mean total radiation dose between the two groups (p = 0.276; Table 1). The mean total times for hyperthermia therapy were also similar between the two groups (9.0 ± 4.08 [4–29] vs. 9.2 ± 2.96 [5–16]; p = 0.510; Table 1). These results suggest that the two groups were comparable. The mean total time for rAd-p53 gene therapy for the p53 group was 8 ± 2.1 (4–18). In this study, most patients (n = 24) received eight rounds of gene therapy (total dose = 8 × 1012 vp), while seven patients received four to seven rounds of gene therapy due to economic constraints. Three patients received 9, 10, and 18 rounds of gene therapy. Both cases undergoing intracavitary perfusion received eight rounds of gene therapy, but the total doses were different (8 × 1012 vp vs. 1.6 × 1013 vp).
Clinical characteristics
ECOG, Eastern Cooperative Oncology Group scale.
Short-term therapeutic efficacies
The short-term therapeutic efficacies were evaluated by RECIST criteria at 2 and 6 months post treatment. As shown in Table 2, 4 (11.1%) and 18 (50%) patients in the p53 group achieved CR and PR at 2 months, respectively, and 5 (13.89%) and 19 (52.78%) in the p53 group achieved CR and PR at 6 months, respectively. No significant difference was found in CR, PR, and SD between groups (p > 0.05). However, the p53 group had significantly lower PD at 2 months (16.67% vs. 45.71%; p = 0.032) and 6 months (8.33% vs. 34.29%; p = 0.036) compared to the control group.
Response at 2 or 6 months post treatment, n (%)
p-Values were adjusted by Bonferroni correction.
Long-term survival outcomes
Long-term survival outcomes were evaluated. The median duration of follow-up was significantly longer in the p53 group than it was in the control groups (36 months [range 18–120 months] vs. 15 months [range 16–116 months]; p = 0.001). Kaplan–Meier survival analysis showed that the p53 group had a significantly longer PFS than the control group (median = 12 months vs. 5 months; p = 0.009; Fig. 1). In addition, the OS was significantly longer in the p53 group than it was in the control group (median 36.5 months vs. 16 months; p = 0.023; Fig. 2). These results suggest that rAd-p53 treatment significantly improved the PFS and OS of STS patients.
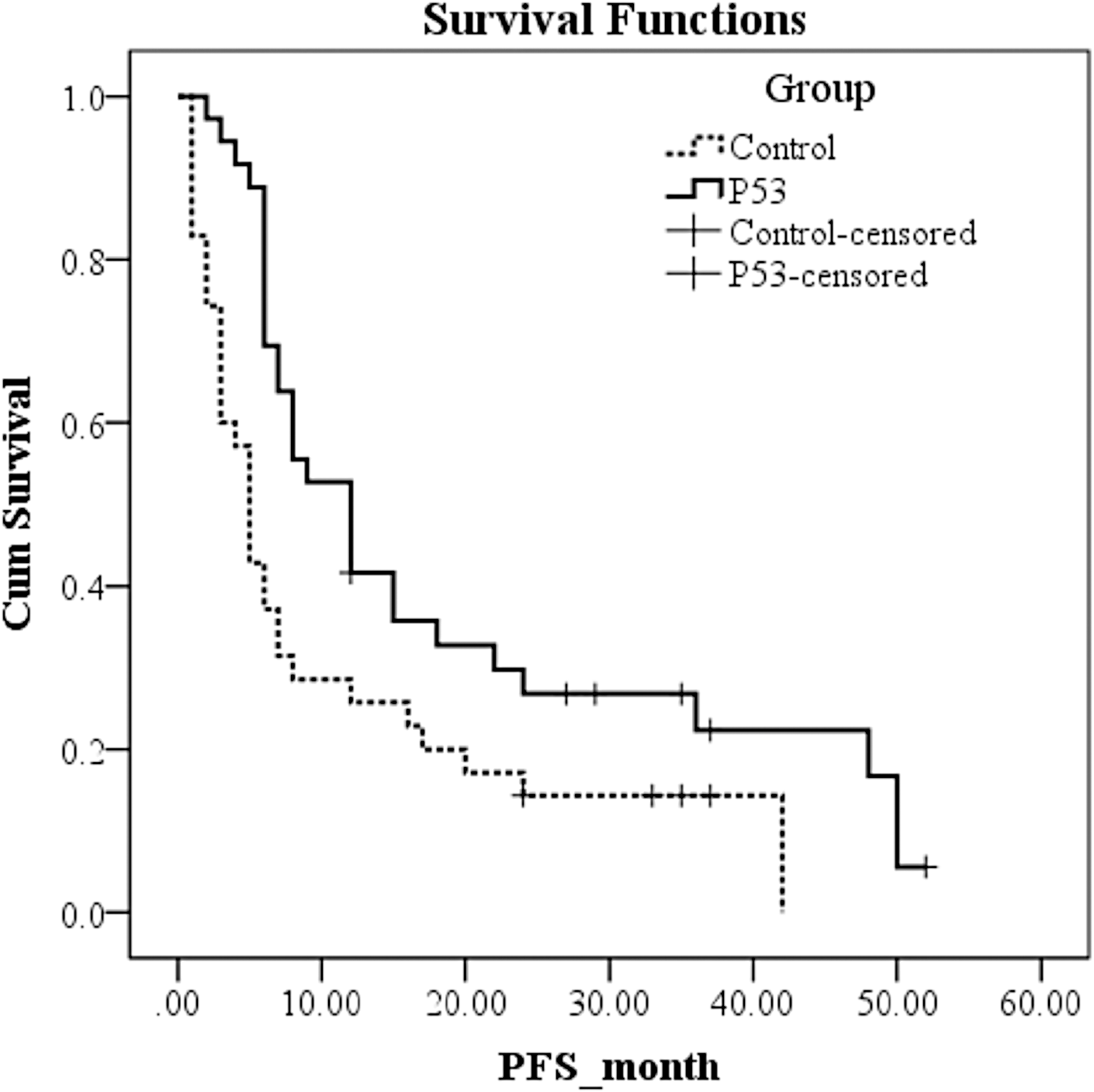
Kaplan–Meier curves for progression-free survival.
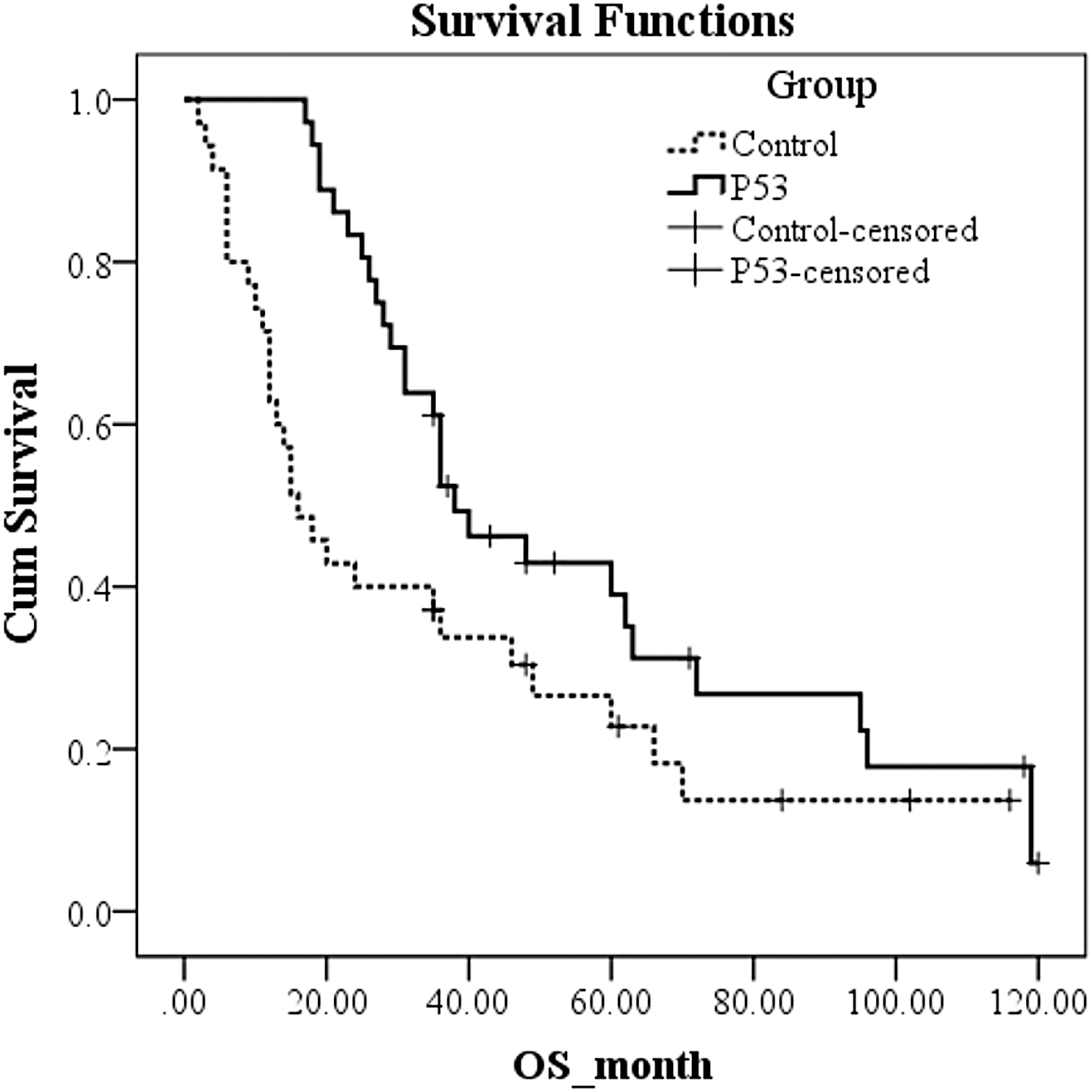
Kaplan–Meier curves for overall survival.
Influence factors associated with PFS or OS
Next, Cox regression models were used to analyze the influence factors with PFS or OS of STS patients. After adjusting for age, sex, ECOG scale, tumor sites, tumor stages, pretreatment status, and histological subtype, group was the only significant factor associated with PFS (HR = 0.40, 95% CI 0.22–0.71; Table 3) and OS (HR = 0.40, 95% CI 0.23–0.71; Table 4) in both univariate and multivariate Cox regression models (p < 0.05). These results indicate that rAd-p53 treatment significantly reduced the risk of progression or death for STS patients.
Predictor associated with progression-free survival
The variables with significance in the univariate analysis and the important covariate that need to be controlled were included in the multivariate Cox analysis.
HR, hazard ratio; CI, confidence interval.
Predictor associated with overall survival
The variables with significance in the univariate analysis and the important covariate that need to be controlled were included in the multivariate Cox analysis.
Therapeutic adverse events
Before and after treatment, the results of blood, urine, and stool examinations were all normal in both groups. Meanwhile, both groups had normal liver, renal, lung, and heart functions. The serum levels of pretreatment and post-treatment ALT and AST were both within normal ranges in both groups (p > 0.05). Among patient undergoing rAd-p53 treatment, 32 (89%) patients had a transient and self-limited fever, including grade 1 fever (47.2%) and grade 2 fever (41.8%). Development of fever was observed as early as approximately 3 h after rAd-p53 injection, which lasted about 4 h and then disappeared spontaneously. Fever occurred most frequently after the fourth round of gene therapy. Nevertheless, fever did not occur at each gene therapy after the fourth round.
There was no significant difference in the other adverse events, including nausea (16.7% vs. 14.3%), vomiting (8.3% vs. 11.4%), diarrhea (8.3% vs. 11.4%), and pain (8.3% vs. 5.7%) between the p53 group and the control group (p > 0.05).
Discussion
Gendicine® is the first approved commercial-use gene therapy vector. Since 2003, tens of thousands of cancer patients have received Gendicine® administration in clinical trials for many cancers with favorable outcomes and safety. 25,31 However, its efficacy on STS is still unknown. This study investigated the efficacy and safety of rAd-p53 gene therapy for patients with unresectable STS. The results show that compared to radiotherapy and hyperthermia alone, rAd-p53 gene therapy combined with radiotherapy and hyperthermia significantly improved the disease control rate and reduced the PD rate. In addition, Kaplan–Meier survival analysis shows that rAd-p53 significantly improved the PFS and OS of STS patients. Cox regression analysis shows that group was the only significant factor associated with PFS and OS, indicated that rAd-p53 treatment significantly reduced the risks for disease progression or death for STS patients. Furthermore, there was no significant difference in any adverse events, except for transient fever. These results suggest that rAd-p53 gene therapy combined with radiotherapy and hyperthermia could improve both short-term therapeutic efficacies and long-term survival outcomes in patients with unresectable STS compared to radiotherapy and hyperthermia alone. To the best of the authors' knowledge, this is the first study reporting the therapeutic efficacy and safety of rAd-p53 gene therapy for STS.
In the present study, there were 62 (87%) patients with stage III and nine (13%) patients with stage IV STS. All were advanced unresectable diseases, which were expected to be associated with poor prognosis. The data show that conventional treatment of a combination of chemotherapy and hyperthermia resulted in poor therapeutic efficacies and survival outcomes. Nevertheless, rAd-p53 gene therapy significantly improved all of the evaluation indicators of therapeutic efficacy and survival outcomes, except for the response rate, including disease control rate (from 54.29% to 83.33%), PD rate (from 45.71% to 16.67%), PFS (from 5 to 12 months), and OS (from 16 to 36.5 months). The difference in response rate between groups did not reach significance, which may be attributed to the small sample size of this study. These results indicate that rAd-p53 gene therapy is capable of effectively sensitizing advanced unresectable STS to radiotherapy and hyperthermia, and could be considered as a treatment option. These observations are consistent with several previous studies on other cancers. For example, rAd-p53 therapy can improve OS in nasopharyngeal carcinoma 32 and unresectable pancreatic carcinoma. 27 As for adverse events, transient fever was the most frequent complication of Gendicine® administration according to previous reports. 32 –34 Consistently, the present study showed that transient fever was founded in 89% of patients with rAd-p53 administration, and no severe adverse events were observed. Fever is a common adverse event in patients receiving gene therapy with different kinds of adenovirus vectors due to the adenovirus-induced immune response. 35
Regarding the dose of gene therapy, previous studies have shown that cancer patients receiving four to eight rounds of rAd-p53 gene therapy can achieve a good outcome, and that more than eight rounds of the treatment does not improve the therapeutic efficacy further. 26 –28 In this study, most patients (n = 24) received eight rounds of gene therapy (total dose = 8 × 1012 vp). Correlation coefficient analysis showed that the dose of gene therapy (the number of rounds of gene therapy) had no significant correlation between any of the outcomes, including response at 2 months, progression, and death (R = −0.193 to 0.188; p > 0.05). The timing of the administration of recombinant virus is crucial for rAd-p53 gene therapy. It has been documented that after the intracellular rAd-p53 injection, ectopic p53 protein starts to express at 3 h after administration, peaking at 72 h, followed by maintaining the expression for 5–6 days and stopping expression after 7 days. 36,37
In this study, rAd-p53 was administered once a week (every Friday), and radiotherapy was started at the peak of p53 protein expression (72 h after rAd-p53 administration, the following Monday), which maximized the beneficial effect that p53 sensitized STS to radiotherapy, resulting in a favorable therapeutic efficacy. In addition, hyperthermia or radiotherapy should be avoided within 2 h after rAd-p53 administration because the administered adenovirus would be directly inactivated by heat or radiation, leading to failure of p53 gene transfer.
There were still some limitations to the current study. First, the sample size was relatively small. Nevertheless, the preliminary results still provide evidence to support the efficacy and safety of rAd-p53 gene therapy for unresectable STS. In addition, this is a retrospective study. A well-designed prospective study with large sample size is required to validate the findings of this study. Moreover, the molecular mechanism underlying the therapeutic efficacy of rAd-p53 gene therapy in STS was not investigated further. All these limitations should be addressed in a following study.
Conclusion
This study showed that rAd-p53 gene therapy combined with concurrent radiotherapy and hyperthermia can significantly improve the therapeutic efficacy and survival outcome of patients with advanced unresectable STS. The findings provide a new therapeutic strategy for unresectable STS.
Footnotes
Acknowledgments
We thank Dr. Jiayong Liu and Chujie Bai at our hospital for their help. This study was supported by a grant from the National Science Committee.
Author Disclosure
The authors declare that there are no conflicts of interest.