
Abstract
Many promising cardiovascular gene therapy approaches have failed to fulfill expectations in clinical trials. However, 20 years of research and method development has laid a solid groundwork for future therapies, and the need for new treatment options still exists. The safety of gene therapy has been established with various viral vectors, transgenes and delivery methods. Improving success in clinical settings requires careful consideration of the translational process. This requires both improving animal models and preclinical end points, and new approach in patient recruitment and selection of clinical end points. This review focuses on bidirectional translationality from bench to bedside and back and proposes ways to improve the process. Developing a highly complex new therapy has taken an enormous amount of work and resources, but perhaps now after the hard lessons cardiovascular gene therapy is ready become a clinical reality.
Introduction
T
Further improvement of the method and success in clinical setting requires even more careful considerations of preclinical disease models, study settings, and endpoints in both preclinical and clinical settings. We should not expect to see more in patients than we have seen in controlled laboratory settings, but often these studies have very different viewpoints, expectations, and even methods. The gap between preclinical and clinical trials should be bridged from both ends. Animal models and preclinical study settings should be designed to mimic the clinical target population and treatment goals better, and clinical disappointments could be better utilized by more careful analysis of responders and non-responders. The reasons for unsuccessful clinical trials often remain speculative. Factors associated with poor outcomes in clinical trials could be reproduced in the experimental setting, and the contribution of individual factors could be more carefully analyzed.
This review focuses on the current status of cardiovascular gene therapy with emphasis on myocardial gene therapy targets and trials. The value of bidirectional translationality from bench to bedside and back is emphasized, and novel approaches to fulfill the clinical demand better for novel therapies are suggested. Central points are summarized in Table 1 and Fig. 4.
Checklist to improve translationality of gene therapy approaches
Choosing Treatment Strategies for Cardiovascular Gene Therapy
The majority of cardiovascular diseases are part of a life-long process of atherosclerosis and its complications. Genetic factors, life-style choices, and environmental factors contribute to a gradual structural and functional destruction of the vasculature, usually remaining asymptomatic for decades. Finally, vascular pathology progresses to a point when the metabolic needs of the tissues are no longer met, resulting in ischemic damage and organ dysfunction. The gradual development of a multifactorial disease produces a genetically and clinically heterogeneous patient population with different grades of disease manifestations and complications. 7 The late manifestation of symptoms also means that the majority of patients have other diseases, medications, and aging-related issues. 8 Modeling such a multifactorial disease is challenging and requires careful interpretation of preclinical findings. 9,10 Defining a clear therapeutic target and setting strict and objectively measurable inclusion and exclusion criteria are therefore essential, and would deserve more consideration in clinical study design. Choosing a (relatively) uniform patient population with clearly defined treatment goal is a perquisite for observing a treatment effect short from a miracle.
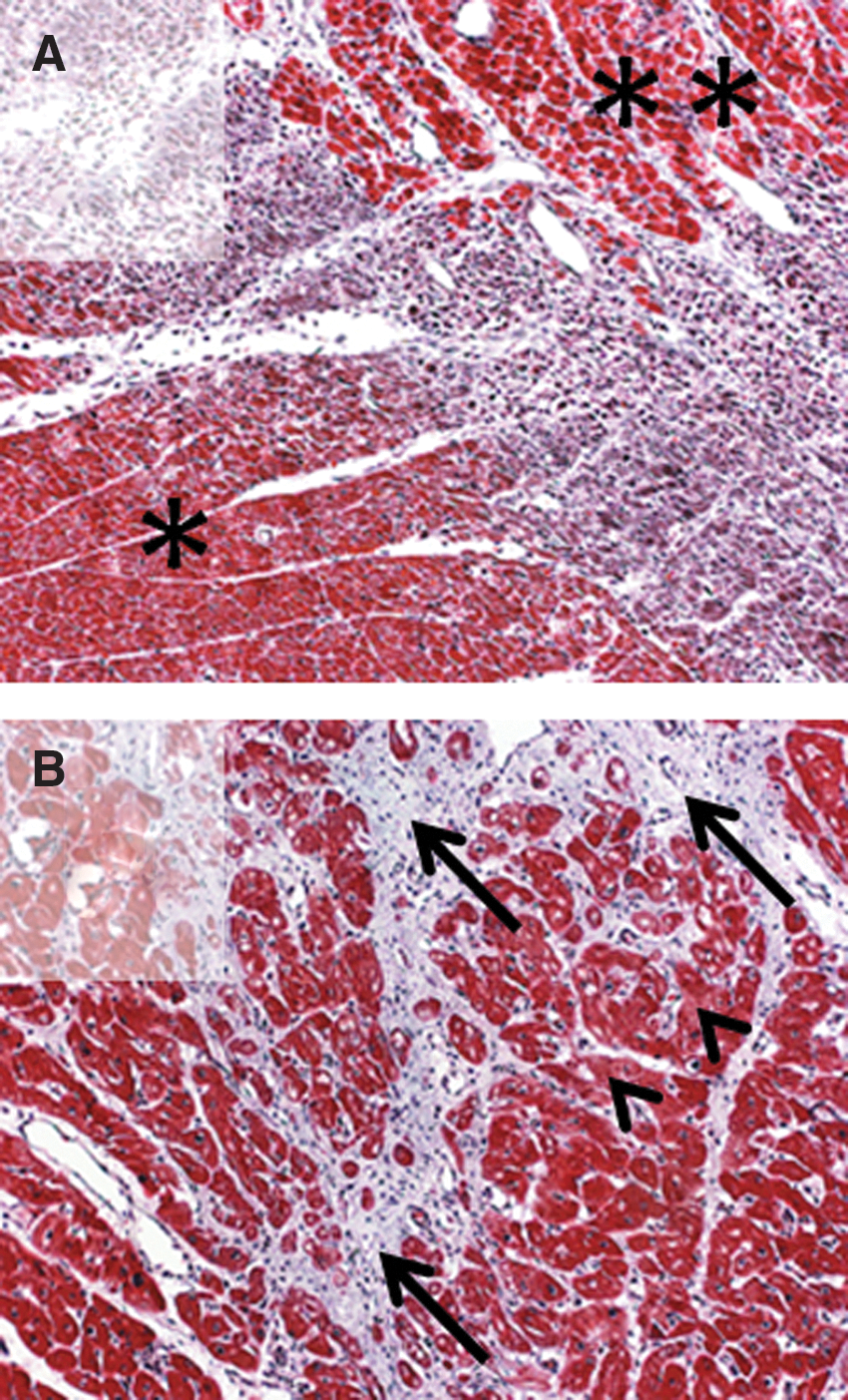
Choosing a uniform and scientifically sound treatment target reaches beyond choosing the patients with similar symptoms or even clinical findings. Preclinical studies often focus on molecular and cellular level events in highly reproducible in vivo and in vitro models, often modeling only one aspect of a multifactorial disease. 10 Patients are diagnosed based on symptoms, clinical findings, and various imaging methods. Different molecular level disease processes can lead to similar clinical outcomes. Acute myocardial infarction in a relatively normal mouse heart is a completely different treatment target compared to acute infarction in a chronically ischemic human heart (Fig. 1). Successful translation of preclinical findings to clinical settings therefore requires careful consideration of therapeutic potential of the preclinical findings, and identifying the patients with similar type and stage of disease process for the clinical trials or conversely, developing animal models that more precisely model the condition intended to be treated.
Defining therapeutic targets. Clinical study population and recruitment criteria have to be defined carefully. Patients with similar clinical symptoms, exercise capacity, and even a similar degree of myocardial damage in the acute setting can be very different targets for gene therapy.
The progressive nature of the disease is also reflected in its manifestations. Mild, exercise-induced ischemia, unstable angina, infarction, and ischemic heart failure are symptoms of different stages of the same disease process. Nevertheless, atherosclerosis, ischemia, and heart failure are often considered separate therapeutic targets, and different therapeutic genes are used. 1 In the earlier stages of the disease, the focus has been on induction of neovessel growth, 11 while in the heart failure setting, the goal has been to improve cardiomyocyte function. 12 Functionally, these two targets cannot be separated. Functional cardiomyocytes require sufficient blood flow, and functional blood vessels are useless without cardiomyocytes to nourish. One option to improve the outcomes in clinical trials would be to consider the heart function on a broader perspective, and combine different treatment strategies to improve organ function more efficiently. 13
Due to the chronic and progressive nature of ischemic heart disease, the potential benefits of the treatment should be evaluated both at the time of expected maximal effect and at longer time points. Preclinical data often describes the acute, maximal effects of a therapeutic approach, and therefore similar time points should be used to show the efficacy of gene therapy approaches conceptually. However, successful treatment of a chronic condition requires beneficial long-term effects, and functional endpoints in particular should be evaluated later. 14 Longer time points may also reveal other, indirect effects of the treatment. A treatment may not improve heart function dramatically in the acute setting, but it may prevent further damage and adverse remodeling in the long run and improve prognosis. 15
Pharmacological management of early stages of the disease and operative management of acute complications are well established. 16,17 Gene therapy approaches are therefore often aimed at treating the late complications and most severely affected patients. 1 These “no-option patients,” who either have already undergone all standard treatment options or are too sick to undergo them at all, 18 also likely have reduced regenerative capacity due to aging and multiple comorbidities. 19 This increases heterogeneity of the patients enrolled in clinical trials, and likely explains at least in part the weak responses. To some extent, this is a reality that has to be accepted in the early stages of a new therapy. As every patient has the right to receive the best possible standard care, gene therapy has to be developed as either an adjuvant to existing treatments or a treatment for situations where no other treatment options are available. 20 Refractory angina and diffuse ischemia affecting multiple vessels and microvasculature of the heart are such targets. 11 In these challenging patient groups, the expectations should be set realistically. In order to induce tissue regeneration, viable tissue and regenerative capacity must exist in the treated area. If functional endpoints are pursued, the capacity for functional improvement must be evaluated as a part of the patient recruitment process.
Setting Expectations
The reason for disappointing results in clinical trials is likely multi-faceted. Multiple small differences, all skewing the results in the same direction, add up and translate to disappointing outcomes in clinical settings (Fig. 2). However, the relative contributions of the various factors affecting the efficiency of specific therapies are largely unknown. Aging, comorbidities, polypharmacy, and diminished regenerative capacity are clinical realities in patients suffering from cardiovascular diseases, especially when gene therapy is developed for no-option patients most urgently in need of novel therapeutic approaches. Methodological issues such as transduction efficiency, pre-existing viral antibodies, and non-sensitive and unspecific endpoints may further dilute the treatment effect, especially in small trials. 14
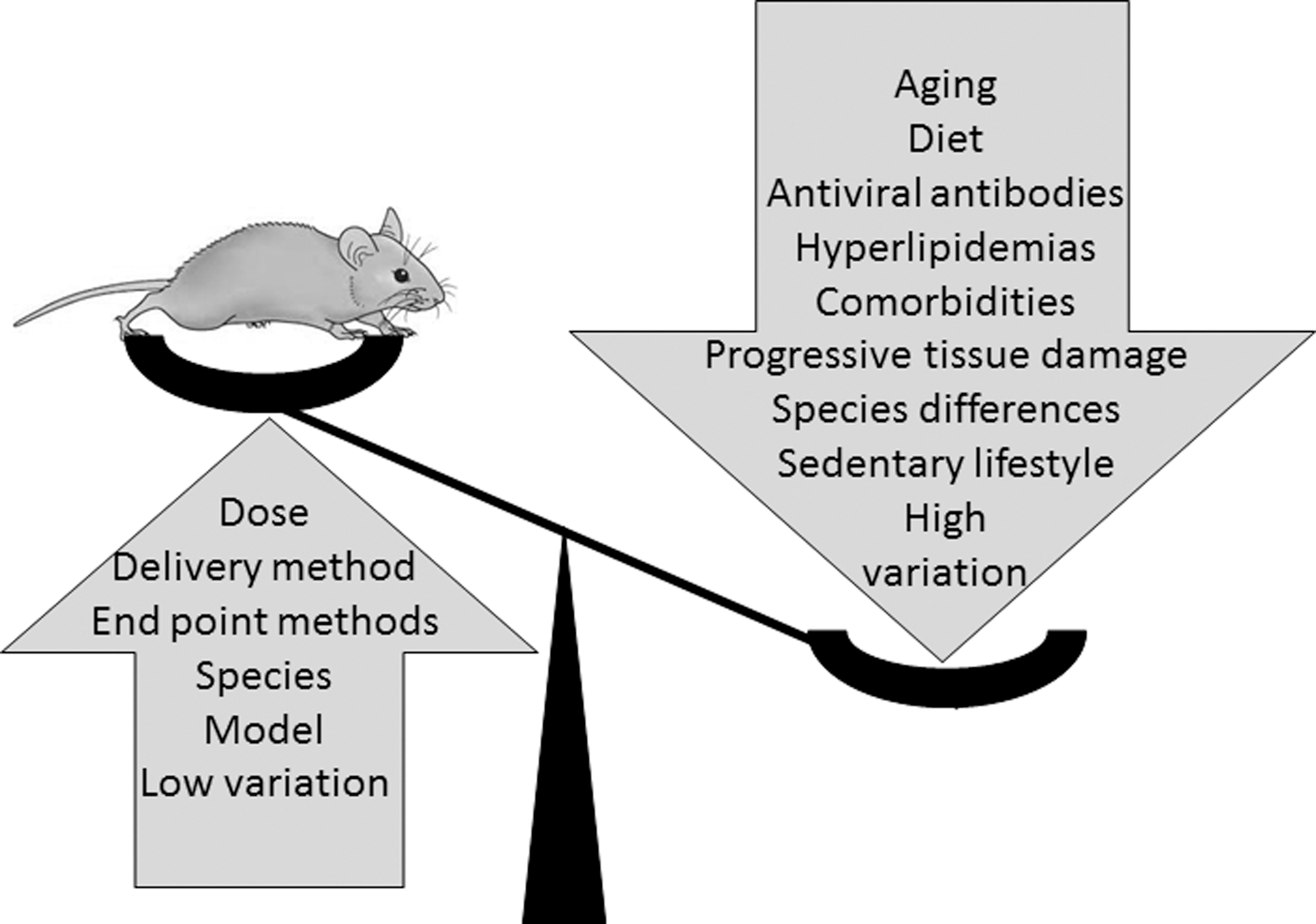
Multiple factors contribute to the dilution of preclinical findings in clinical trials. Experimental animals are usually young, rodents in particular have better regenerative capacity than humans, and genetic variation in experimental animal populations is small. Animal models have low variation in baseline characteristics, and time points are identical in all individuals. Delivery methods are often different from clinical settings, and too often viral doses exceed those used in clinical trials. Endpoint methods in preclinical studies are sensitive and often focus on molecular level effects. All these characteristics highlight even small differences between treatment groups.
Some falsely promising results in preclinical settings are likely due to fundamental differences in animal models and target patient populations. Experimental animals are usually young and healthy, and due to both age and species differences have better regenerative capacity than aging humans with several comorbidities. 21,22 This translates to plasticity, proliferative capacity, and functional physiological responses such as vasodilation often required in tissue regeneration. Variation is often minimal in preclinical settings compared to the human population. In rodent models in particular, uniform genetic background and identical environmental conditions provide an optimal setting for bringing out differences in treatment groups, but it does not reflect the degree of variation in clinical populations. This conundrum cannot be completely eliminated but has to be taken into account in power calculations and study design.
Other differences between preclinical and clinical studies are easier to resolve. Preclinical data are often derived from much simpler animal models, and bold extrapolations have been made when the treatment strategy has been tested in clinical settings. For example, myocardial ischemia is often modeled in otherwise healthy, young animals. The tissue environment is completely different in an acutely ischemic but otherwise healthy heart and in chronically ischemic fibrotic myocardium. This can affect all stages of the therapeutic approach: cells available for viral transduction, capacity to produce the transgene, cell types available to respond to the therapeutic molecule, and regenerative capacity (Fig. 1). The molecular environment possibly altering the transgene function is different, and systemic responses such as inflammatory reactions and the regulation of blood pressure may be different. This may produce very different outcomes, even with the same therapeutic molecule and dose (Fig. 3). Physiological characteristics also modify local responses, for example neovessels only persist in ischemic tissue where the vessels are needed, whereas vascular pruning trims capillary network in normoxic tissues. 23 Some approaches may even be detrimental in dysfunctional tissue. For example, increasing myocardial contractility in poorly perfused myocardium may only lead to the depletion of limited metabolic resources and further tissue damage. Careful experimental design and choice of animal models are therefore essential for realistic evaluation of the therapeutic potential of a gene therapy approach.
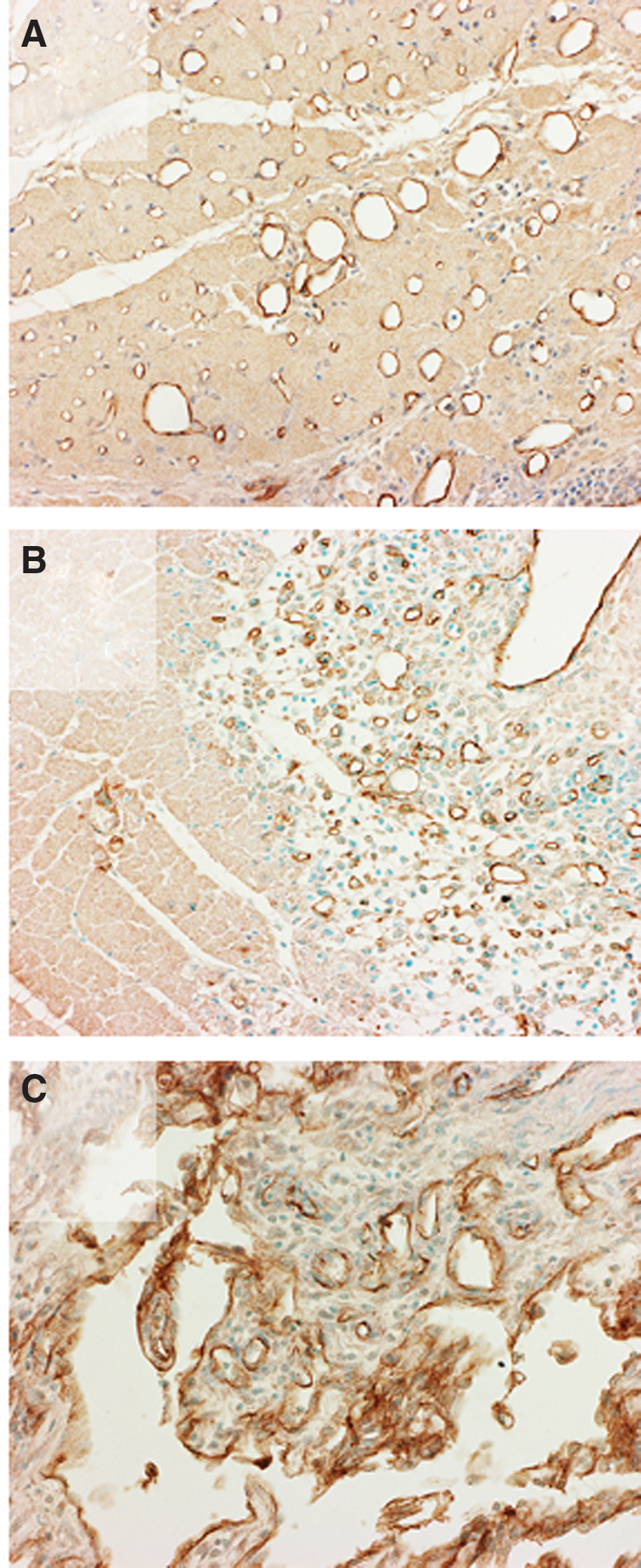
Targeting gene therapy. The same vector, therapeutic gene, and dose in different areas of the same heart. Adenoviral delivery of vascular endothelial growth factors can produce very different effects, depending on gene transfer area.
Advances in animal models and imaging methods have brought the clinics and laboratories gradually closer to each other. Myocardial ischemia models have developed from surgical coronary ligation models to sophisticated, minimally invasive models, where duration and severity of ischemia can be controlled. 24 More widely available, more sophisticated imaging methods allow more precise patient selection and provide more functional data of the target tissue in animal models as well. Tools are therefore available to match the preclinical animal models and patients recruited in clinical trials better and more precisely, and to target gene therapy to the right tissue environment.
The differences in regenerative capacity and plasticity of the cardiovascular system are largely only estimations, and systematic side-by-side comparisons have not been conducted. Replicating a clinical study setting in a relevant animal model, from delivery methods to endpoint measurements, would be possible in large animal models, and would provide valuable information of translationality of the chosen approach. No animal model is a perfect reflection of a patient, and identifying patient characteristics that predict a poor or beneficial outcome of a treatment would allow the modeling of these characteristics in preclinical studies. Patient recruitment could also then be adjusted to rule out patients who are unlikely to benefit from the treatment strategy, or preferably, to be able to choose the patients most likely to gain clinical benefit. Post hoc analyses of clinical trials have helped to guide the patient selection process. The AWARE trial was designed based on the results from AGENT trials, revealing that women >55 years of age were the most likely to benefit from intracoronary infusion of Ad5FGF-4. 25 However, the efficacy of this strategy remains to be tested.
Measuring Efficacy
In order to achieve a therapeutic effect, the dose and duration of transgene expression have to be sufficient. Delivery methods and especially viral doses used in preclinical and clinical studies are often very different. 26 In rodent models in particular, very high viral doses are feasible, and total viral doses often grossly exceed the doses used in large animal models and clinical trials. Systemic delivery results in transduction of various organs according to vectors tropism, and high protein production can be achieved in non-target organs. It is therefore essential to mimic the intended clinical study setting as closely as possible in preclinical studies in order to obtain a realistic view of the transduction efficiency and protein production in target organs.
Differences in animal models and patient populations are an obvious culprit, but another explanation is a mismatch between preclinical data and clinical expectations. Therapeutic benefit has largely been assessed differently in preclinical and clinical studies. 11 In animal models, the emphasis has been on easily quantifiable endpoints, such as blood vessel number and gene expression, while in clinical trials, the endpoints have been more elusive and subjective, such as exercise tolerance. 1 A positive result in a study requires a statistical difference between the treatment groups. In a strictly controlled preclinical study setting, variation can be minimized, and smaller differences can lead to significant results. Endpoints such as exercise tolerance are dependent on multiple factors—heart function, overall fitness level, and mental factors to name but a few. The more variables there are, the harder it is to bring out differences between treatment groups. This problem is evident in trials with a limited number of participants. These types of endpoints are also more susceptible to placebo effects often observed in gene therapy trials. The endpoints also measure completely different things: increase in blood vessel number does not necessarily correlate to better perfusion, to better organ function, and even less so to better exercise tolerance, ability to function, or mortality. 27
Both types of endpoints are needed to develop successful therapeutic approaches. Methods such as histology, gene expression analysis, and protein expression provide invaluable information on the mechanisms and effects of gene therapy in preclinical studies. Quantitative endpoints such as local perfusion and locally measured myocardial viability are important to assess the efficiency of the gene transfer, and functional endpoints are needed to assess if the local effects are sufficient to improve overall function. Functional endpoints are the most meaningful for the patient. A local increase in perfusion is a methodological success, but in the end, the goal is to alleviate perceptible symptoms and to improve the patient's ability to function and quality of life. Methodology should therefore be unified in preclinical and clinical studies. This would both provide mechanistic, proof-of-concept data from clinical studies and would help to design both patient inclusion criteria and study endpoints to match the preclinical data better (Fig. 4).

Translationality from bench to bedside and back. The preclinical data have to be interpreted carefully in order to set realistic goals and endpoints in clinical trials. Too liberal extrapolation and over-interpretation of preclinical results only leads to unrealistic goals and wrong endpoints in clinical settings. If cardiomyocyte viability and neovessel formation were studied in animal models, it may not be realistic to expect improvement in perfusion or exercise capacity. Patients for the clinical trials have to be chosen to match the actual preclinical model used, and inclusion criteria should include methods that are able to characterize the disease process, not just the clinical and functional outcome of the disease.
Translating Basic Science to Clinical Practice
A key to clinical success is to understand both strengths and weaknesses of gene therapy. The approach is so different from standard clinical methods that conveying this information to the clinics performing the clinical trials is essential. 28,29 This requires close collaboration between the units performing the preclinical and clinical phases of development. This would improve both translating basic science to clinical practice and preclinical testing.
Achieving sufficient transduction efficiencies and effective concentrations of therapeutic molecules in the treated tissue often requires local delivery of the vector. Locality can be both a strength and a weakness. Locality means fewer systemic (side) effects, and for strategies such as induction of neovessel formation, less risk for unwanted effects, such as induction of neovessel growth in undiagnosed or dormant tumors, or systemic vasodilation interfering with regulation of blood pressure and perfusion distribution. However, locality also means that the therapy must be correctly targeted in order to achieve therapeutic effects. Increasing perfusion in healthy tissues to a super-physiological level is less likely to improve heart function, and can even reduce perfusion in ischemic areas due to a steal effect. 14 Conversely, transducing scar tissue is not effective, as protein production and tissue regeneration require living, functional cells in the gene transfer site. Gene transfer in ischemic myocardium therefore has to be delivered to a relatively small, clearly defined area where beneficial effects can be expected. Recently, elegant strategies have been developed to target the gene transfer better where it is needed. In ischemic myocardium, a combination of electromechanical mapping and positron emission tomography perfusion imaging has been utilized to identify the viable but poorly functional myocardium. 29,30 In addition, this local, quantitative, baseline information can be used to follow up the perfusion in the gene transfer site after treatment.
A local effect can also be a downside if a large transduction area is required to achieve a therapeutic effect. Lower limb ischemia is one such application, and therapies aiming to improve myocardial function would also require a significant portion of the cardiomyocytes to be transduced to improve cardiac function. Using viral vectors with high tropism to target tissue and secreted soluble therapeutic molecules can be used to overcome this problem. 31
Gene therapy is usually delivered as a single treatment. From the patient's perspective, this is an advantage compared to long-term pharmacological treatments. However, this means either that the therapeutic effect should be achieved in a relatively short time, or that long-term expression with integrating vectors is used. Exposure to viral vectors usually leads to the production of neutralizing antibodies, and repeated dosing of vectors with a short gene expression time is not a feasible option at the moment. 32 On the other hand, integrating vectors raise more safety concerns due to possible activation of oncogenes and deleterious effects of prolonged gene expression. 33
Recent Advances and Future Perspectives
Better clinical success can likely be achieved by improving the specificity and efficacy of gene therapy. Local gene transfer methods allow efficient local transduction of ischemic myocardium and selected sections of vascular wall. 34,35 High transduction efficiencies in the heart have been achieved with intravascular delivery methods, but the efficacy in clinical settings remains to be demonstrated. 31,36 Different characteristics of healthy and diseased tissue can also be used to target gene therapy and improve its safety. For example, vector constructs or therapeutic molecules selectively active in hypoxic environment can be used. 37
Viral vectors have been developed to target the therapeutic effect to specific cell types and tissues either by modifying the tropism of the vector or by limiting the transgene expression to desired cell types by choosing a cell- or condition-specific promoter. 2 The challenge of these approaches is that when specificity increases, the efficacy usually decreases, and therapeutic concentrations may not be reached. Adenoviruses and adeno-associated viruses have been tested in various clinical trials and have been shown to be suitable for cardiovascular applications. 27,38 Novel delivery methods such as exosomes, nanoparticles, and microRNAs are explored as potential new tools to deliver a wide selection of different types of therapeutic constructions to target tissue. 39 –41
Currently, the focus is shifting from single therapeutic genes to more complex regulation of gene expression. The aim is to develop therapies that more closely mimic endogenous responses and repair mechanisms. The selection of therapeutic molecules has expanded from protein-coding genes to various regulatory RNA molecules. 42
Another option is to combine gene therapy approaches to surgical and endovascular procedures and cell therapies. 20,43 This augmentation treatment approach would also allow enrollment of less severely ill patients, with possibly better regenerative capacity and better chance of improvement of heart function.
Previous clinical trials have provided valuable information to develop gene therapy approaches further. The regulatory pathway for gene therapy products has been established, many clinical centers have experience with gene therapy trials, and the safety of several vectors and transgenes has been studied. Despite early disappointments, several gene therapy trials have reported positive results, and new trials are underway. 27 The first gene drugs have been approved for clinical use in the Western world, 44 and the route for new basic science innovations to clinics has been charted. In the future, continued dialogue between basic science laboratories and clinical centers should be maintained and strengthened to improve clinical study design, patient selection criteria, selection of appropriate endpoints, and preclinical animal model development. Developing a highly complex new therapy has taken time and an enormous amount of work and resources, but perhaps now all the groundwork will bear fruit in the near future.
Footnotes
Acknowledgments
This review was supported by the Finnish Academy Center of Excellence in Cardiovascular and Metabolic Diseases ERC Advanced Grant and EATRIS (National Virus Vector Laboratory).
Author Disclosure
No competing financial interests exist.