
Abstract

Introduction
S
While appreciating the enormous potential of gene transfer technology, the scientific and medical community has always recognized the possible limitations toward clinical translation in terms of feasibility, safety, economical constraints, and ethical issues. The establishment of treatments involving gene transfer technology is analogous to that of any biological products in that it is translational in essence, ranging from experimental and preclinical research to product manufacture and clinical trials and development (Fig. 1). Gene therapy can only reach its true potential if advances can be achieved in technology on both the safety and efficacy sides. It also requires adequate resources, including high-level training of personnel and sustained funding of projects in the long run. When referring to pharmaceutical drug development, a minimum of 10 years is required, while monoclonal antibodies have entered the clinic more than two decades after introducing the concept and showing its targeting potential in vitro. Successful development of gene therapy is therefore complex, which also encompasses three additional salient issues in this particular area: first, regulatory policies for gene therapy medicinal products, in particular since vectors can be derived from defective viruses or integrate in the genome of the host target cells or might elicit an immune response; second, related ethical issues, noticeably addressing the decision on when to “go” or “no-go” to the clinic; and finally, patenting certain processes, while several technologies are intricate and need to be combined toward clinical implementation. Because of this complexity, sustained exchanges of ideas, concepts, data, methods, and material are pivotal to the advancement of the field that gave birth to the European Society for Gene and Cell Therapy (ESGCT)28 and, later on, to its companion EC-DG research network of excellence, the CliniGene-NoE. 29
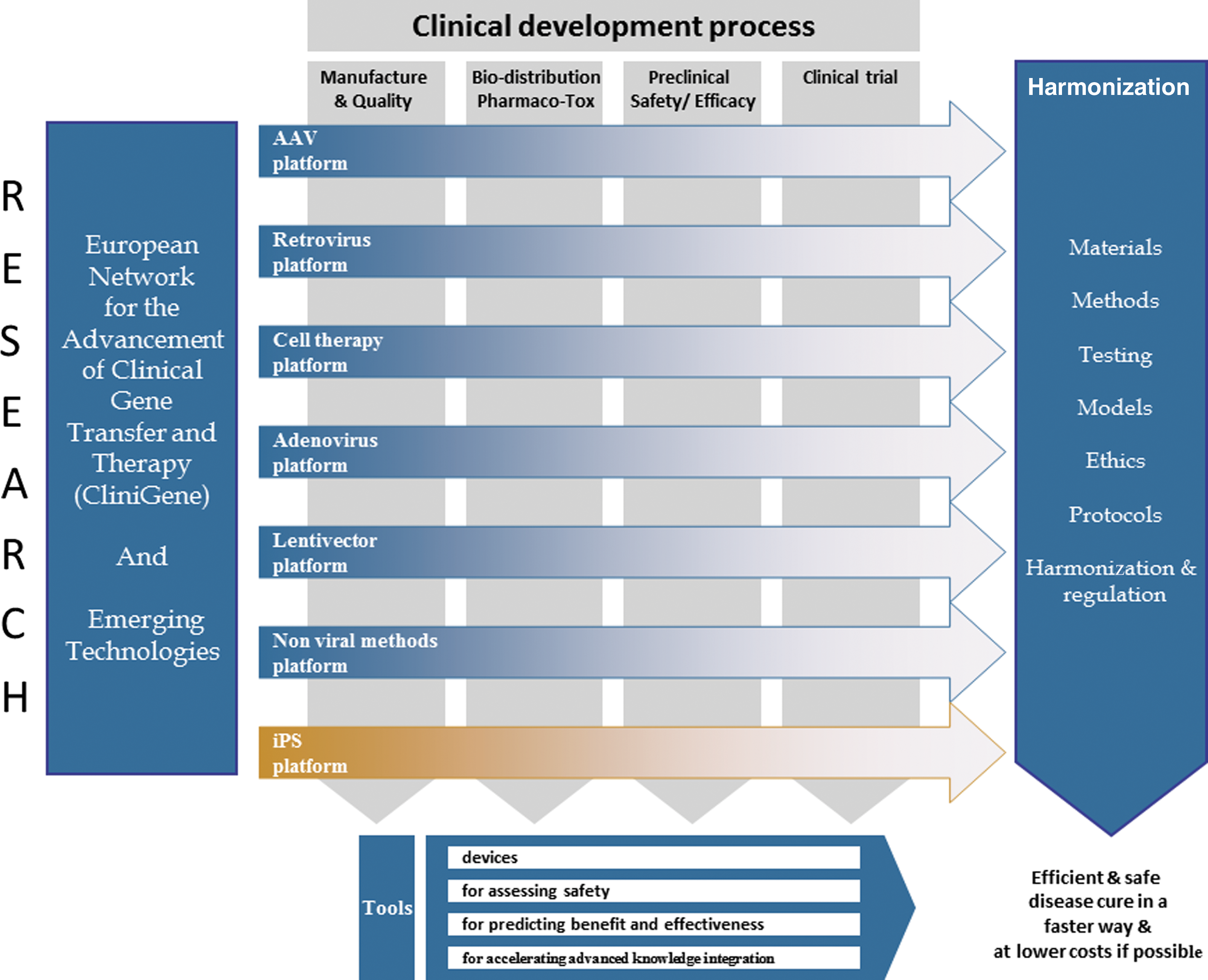
Clinical development of gene therapeutics: from the basic science of gene regulation through gene transfer vectors, experimental research to clinical translation of products qualifying for use in human patients.
A Historical View: the First Learned Society On Human Gene Transfer and Therapy
First international workshop on human gene transfer
The first international symposium on gene therapy in Europe took place in April 1991, a year after Michael Blaese's team carried the first gene therapy clinical trial in a monogenic disorder, ADA-SCID, at the National Institutes of Health. This meeting, hosted by Michel Boiron and Odile Cohen-Haguenauer, was held in April 1991 at the Chateau de Montvillargenne, which gathered >250 participants. The meeting focused specifically on two areas in which gene transfer is particularly relevant to medicine: (1) the transfer of human genes to experimental animals, with the aim of understanding the regulation of gene expression and creating models of human diseases, including via homologous recombination, as pioneered and presented by Mario Capecchi 30,31 ; and (2) the introduction of genes into human somatic cells, with the ultimate aim of treating human diseases. Progress presented on this occasion was particularly gratifying. In a powerful experimental system, Claudio Bordignon reported that genetically immunodeficient mice can be made immunocompetent by the infusion of genetically engineered lymphocytes from children with ADA-SCID. 32
The symposium of Montvillargenne had given a wonderful overview of the current “state of the art” in gene transfer and a think tank on what to do next. 3,4 It soon became evident that expertise and synergies were needed across disciplines in order to help solve burning issues discussed during the symposium, ranging from ethical and safety concerns, gene regulation, and gene delivery methods, calling on virology, molecular modeling, and chemistry, as well as routes and schedules of administration according to the disease to treat. Since a multidisciplinary approach is needed to allow fruitful exchange between clinicians and researchers in basic science, it was to meet this need that the European Society for Gene and Cell Therapy was founded, as the first in the field worldwide.
Launching the ESGCT
The European Working Group on Human Gene Transfer and Therapy, later to be called the ESGCT, was officially founded in January 1992.
33
The Society's main goal was to develop and coordinate clinical and scientific research in the area of gene transfer and gene therapy in Europe. The Society aimed at disseminating coordinated information and exchange of technology, material, and human expertise, which it did in the following ways: • The annual meeting provided a forum for the exchange of information and the presentation of peer-reviewed data; • A scientific directory was established, which described the details of both the area of interest and the expertise of each member's team; • A European Union (EU)-wide record of gene transfer and therapy clinical protocols was established; and • A quarterly newsletter was released by the scientific secretariat in order to foster interaction between members and circulate information from the Board. Each issue included an update of clinical protocols and a section dedicated to ethical and regulatory issues (ELSA).
The Society was founded with the initial support of the European Haematology Association (EHA) established by Michel Boiron. Lucio Luzzatto's support and commitment were also critical. The first meeting was held on October 17, 1992, at Chateau de Maffliers, where the first elected Board was formed, gathering Claudio Bordignon as president, Erwin Wagner as vice-president, and the following members: Olivier Danos, Jean-Michel Heard, Stephen Russell, Dinko Valerio, Thierry Velu as Treasurer, and Odile Cohen-Haguenauer as Scientific Secretary based in Paris, France. The Society bylaws were registered in Belgium as a European nonprofit association. By 1996, this unique group had achieved the federation of all major European teams working in the field and included >550 members, including company personnel from 18 countries, including Israel, Eastern Europe, North America, and Asia, as Associate Members.
The Society faced difficult times when major adverse events showed in clinical trials, first in 1998 in the United States, with the tragic death of a young boy infused systemically with an adenovirus-derived vector, and later in 2001, when a first case of leukemia developed in a X-SCID infant treated in France as a direct consequence of the integration into the host cell genome of the gammaretrovirus vector carrying the otherwise therapeutic gene, which triggered enhancer-mediated genotoxicity and uncontrolled proliferation of gene-modified cells. 34
During this complicated period for the field in general, Bernd Gänsbacher took over as president in 1999 and remained extremely active in reshuffling and reshaping the Society during five consecutive years up until 2004. With his action, the ESGCT started to recover and progressively upgrade again both in membership and in the quality of the yearly meeting, which currently stands as an international reference.
Focusing On Scientific Expertise: Yearly Meeting and Education
ESGCT yearly meeting
Since its inception, the ESGCT holds an Annual Congress in October or November of each year. The communication of utmost recent data and the participation of young scientists are encouraged. The ESGCT meeting is now well established (
The venue moves between different European countries so as to encourage interactivity, the recruitment of new members, and outreach. In fact, through its Annual Congress, the ESGCT has been proactive in facilitating scientific exchange, disseminating knowledge, and increasing the awareness of gene and cell therapy among scientists, including numerous other learned societies and the general public at large.
The first meetings received support from the DG research (DGXII) of the European Commission (Human Genome Area, FP4-Biomed 2 Programme). Since then, a number of EC-DG research funded programs have followed the pace initiated by the Euregenethy thematic network and the CliniGene-NoE in organizing their dissemination programs at the ESGCT yearly meeting, thereby allocating their matching budget to the ESGCT.
Educational sessions
Considering the complexity of the field, embracing cutting-edge and rapidly evolving technologies, biosafety issues related to the use of genetically engineered viruses and human cells, a broad range of potential applications, and key ethical issues, the establishment of a strong network inside the scientific and medical community had to streamline the spreading of the best validated knowledge. It was first Zelig Eshhar and later Fulvio Mavilio who took over the organization of an education day. It was decided that this multidisciplinary event would be held before the opening of the general meeting. In fact, leading scientists give a high level of in-depth lectures, which provide the necessary background in order to capture important new data communicated during the main meeting to follow.
Scientific developments and first clinical trials have attracted leading top scientists to the EU
Because the Society was fostering scientific exchanges and spreading enthusiasm, it probably played a part in attracting leading experts to the EU, such as: Luigi Naldini 5 and Thierry VandenDriessche, who were later to become presidents of the Society; Zsuzsanna Izsvak and Zoltan Ivics, who have been acting as leaders in the development of transposon-derived gene transfer vectors and developed collaborations with Marinee Chuah and Thierry VandenDriessche 35 ; and, more recently, Federico Mingozzi, whose contribution pioneered the elucidation of immune reactions related to adeno-associated virus mediated gene transfer. 36,37
Scientific Expertise and Regulation of Advanced Therapy Medicinal Products for Gene Therapy At the European Medicines Agency
The development of promising new medicines to address unmet medical needs is challenging from a scientific and regulatory point of view. Early consultation and scientific advice with regulators and other healthcare decision makers is key to ensuring that data are generated to the standards required for regulatory approval and market access.
European centralized regulation
As an inaugural event, in December 1994, the Committee for Proprietary Medicinal Products approved a final draft of the guideline addressing “Gene therapy products: quality aspects in the production of vectors and genetically modified somatic cells” (DGIII/3477/92). These products would be subject to a centralized procedure for marketing authorization issued by the European Medicines Evaluation Agency (EMEA; later to become the European Medicines Agency [EMA] in 2011). Since then, many position papers, reflection papers, and guideline documents have been issued by EMA's Committee for Advanced Therapies (CAT) in particular, following in each instance a phase of consultation seeking for comments from established expert scientists in the field of interest. 38
Over the past year, the EMA and its scientific committees have been working on a number of initiatives aimed at further supporting development with a view to accelerating patients' access to medicines that address unmet medical needs. With the development of gene- and cell-based prospects for the treatment of human disorders, the EMA set up a CAT in charge of the evaluation of so-called advanced therapy medicinal products. Fast-tracks have been set in place for the evaluation of orphan drugs addressing rare diseases and more recently the Scientific Advice Working Party (SAWP) and the PRIME procedure. The latter is a scheme that has been developed to reinforce early dialogue and regulatory support to stimulate innovation, optimize development, and enable accelerated assessment of PRIority MEdicines (EMA/CHMP/57760/2015).
The field was fortunate that a prominent, outstanding figure, Klaus Cichutek, was initially in charge at the level of the regulatory authorities and also a renowned scientist acting with a wonderful spirit of collaboration with the ESGCT.
Scientific advisory body
The ESGGT and its Ethics and Regulation Committee (ELSA) were prepared to act as a scientific advisory body for the review of guidelines, scientific programs, clinical protocols, and so on, and were asked to act in this capacity by the EC DGIII pharmacy and DGXII research. This officially materialized with the allocation of a dedicated seat for a Society representative at EMA-CAT as the Committee was established in 2010.
Moving back at the time where major adverse events occurred in the field, it became obvious that ethical, legal, social, and regulatory issues (ELSA) had to be taken up as a never so salient and strong a component in the field of gene therapy. While the Society's Board was focusing on establishing the yearly meeting, Euregenethy 1 was created by members of the ESGCT ELSA Committee as an FP4 EC-funded undertaking coordinated by Odile Cohen-Haguenauer. Euregenethy 2 followed as an enhanced project, a thematic network under the EC fifth framework program. Robust and sustained interaction with regulatory authorities, an active Web site, publications, and meetings gathering all stakeholders in the field led the thematic network to expand into the capacity of funding collaborative research in a way that was meant to encourage synergies. Indeed, the EC-FP6 CliniGene-NoE was officially launched in 2006 as the European network for the advancement of clinical gene transfer and therapy. From Euregenethy 2 to CliniGene, both endeavors have negotiated with the EC to act as major funding supports to the ESGCT, contributing >€300,000 from 2004 to 2011.
Scientific Developments: EU DG Research Funding
With the fourth framework program of the EC-DG research (DGXII), somatic gene therapy was registered for the first time as a priority in both the Biomed 2 and Biotechnology programs. This represented a significant step forward, because up until 1994, official recognition of this field by the European Parliament and the Commission of the European Union was strongly disputed. Both the acting president and scientific secretary of the Society initiated action from 1992 onward to convince members of the European Parliament and decision makers at EC DGXII research that gene therapy was not meant to modify the inherited genetic make-up of the human race but rather to provide innovative options and hope for lethal diseases, many of which were orphan or rare disorders affecting infants and children. Since then, a number of EC-funded projects have markedly helped advancement of the field, as stated by Draghia-Akli. 39
Created with the main objectives of bottom-up and overcoming fragmentation, the CliniGene-NoE EU DG research funded program acted as the ESGCT companion in ELSA, bridging with the industry sector and expanding the scope through funding of experimental research with a 6-year budget of €12 million. The main goal of CliniGene was to integrate multidisciplinary research in order to identify the “critical path” to accelerate the transit phase from preclinical to clinical stage by integrating expertise and generating new knowledge that can lead to improved safety and clinical efficacy of gene transfer and therapy. Indeed, safety is of germane concern, since in the event where the treatment would be proven safe, it could be administered early enough in the course of the disease to achieve a genuine cure so that clinical gene transfer may be called therapy.
While encompassing a broad range of technologies and their potential applications, the NoE has succeeded in establishing intensive networking, which crosses the boundaries between technology platforms, including emerging technologies and a human induced pluripotent stem cells (iPS) platform. This challenge has been successfully fulfilled, with the NoE achieving integration and translating into the facilitation and multiplication of clinical trials initiatives with as many as 29 clinical trials, while the initial target was in the range of 10 at the most, among which first clinical successes have been in ADA-SCIDs, Leber congenital amaurosis, Parkinson's disease, and X-linked adrenoleukodystrophy, with the first clinical use of lentivectors in the EU. 29
Central to these successes and their acceleration was the constant development of cutting-edge technology, with the implementation of both the Emerging Technologies platform and the General Biosafety platform. The Emerging Technologies platform funded competitive start-up international collaborative projects and exchange of personnel (Fig. 2), with >90 projects targeting novelty between 45 laboratories and companies. The mechanism of flexibility funds through so-called flexifunds involved 20% of the NoE total budget. The General Biosafety platform focused on the translational aspects addressing safety and efficiency of current and newly developed systems in vitro and in vivo with two main focuses: (1) transgene integration, with Christof von Kalle and Eugenio Montini in charge; and (2) immunotoxicology, with David Klatzmann in charge, in collaboration with Federico Mingozzi who was still in the United States at that time.
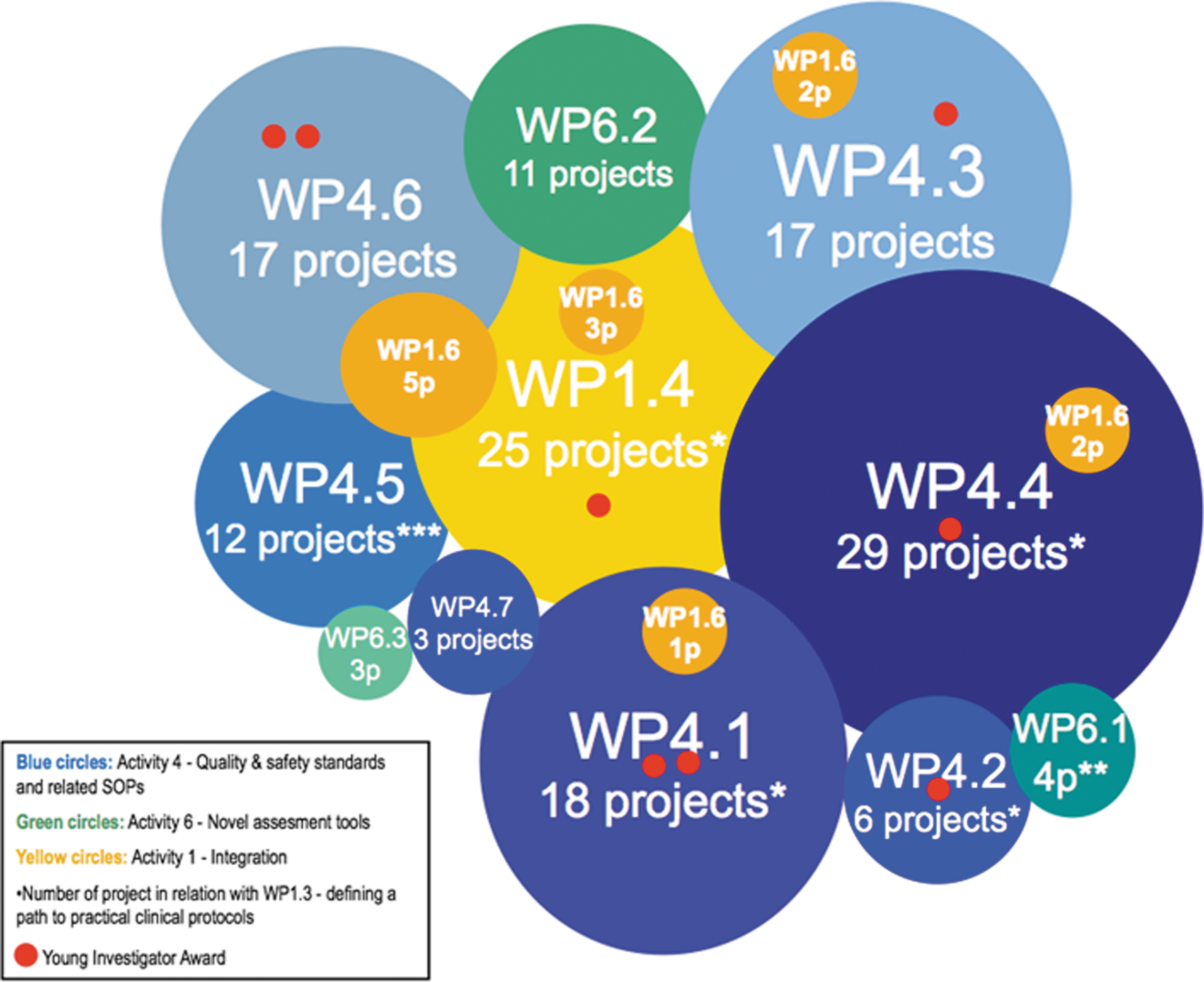
Funding and integration of emerging technologies through the CliniGene-NoE “flexifunds” international collaborative program including short term exchanges of personnel and young investigators awards. WP1 stands for integration; WP4.1 to WP4.6 relate to the six gene transfer vector platforms (4.1: AAV; 4.2: gammaretrovirus; 4.3: lentivirus; 4.4: gene-modified cells; 4.5: adenovirus; 4.6: non-viral) and WP4.7 to iPS; WP6 represents general biosafety and novel assessment tools.
In order to streamline the clinical translation of the most advanced technologies, this joint research program developed and concentrated on five main directions: (1) Preclinical evaluation of a new generation of safer and more efficacious gene transfer vectors, whether viral or non-viral, including transposon-derived non-viral integrating vectors, and comparing them to available technologies. (2) Safety and efficacy improved integrating vectors, since predicting and ultimately controlling the fate of transgenes integration is a major priority in the field.
34,40
Progress in this regard is likely to pave the way for the treatment of numerous conditions, noticeably accessible by ex vivo gene manipulation of stem cells, whether intended at repairing cell defects such as with hemoglobinopathies, Wiskott–Aldrich syndrome, or Fanconi's anemia, or with a view to enzyme replacement therapy such as with adrenoleukodystrophy or ADA deficiency. A stem cell and iPS technology platform was created in the fourth year of the program, addressing induction of iPS together with characterization, expansion, and differentiation of stem cells and their genetic modification. (3) Improvement of the therapeutic index of viral and non-viral vectors noticeably via direct in vivo administration routes is another key issue in gene therapy related to the immune responses directed at the vector particles, the transduced cells, and/or the therapeutic proteins themselves, which can curtail long-term gene expression. The risk of inadvertent immune responses can be minimized in avoiding vector uptake and gene expression in antigen-presenting cells, including modified administration routes. This can also be based on targeting of cell entry and tight transcription regulation taking advantage of miRNAs. (4) Ethics and regulation. The field of gene transfer research is one of the first among novel biologics to have thoroughly considered the ethical issues that arise in first-in-human trials. Key issues include determining how much and what type of preclinical information supports moving to human studies and who should be the first subjects. These issues raise questions of both research design and research ethics.
41,42
(5) Bridging with the industry sector: establishing the industry meeting as a satellite to the ESGCT yearly meeting, Seppo Ylä-Herttuala played an important role in that regard.
Installing Industry Workshops As Satellites of the ESGCT Annual Congress
The CliniGene industry workshops held as satellites of the ESGCT Annual Congress provided unique opportunities to gather professionals from the private sector and academic centers of excellence. These meetings had a positive feedback, with their attendance growing from one year to the next. The first meeting took place in Rotterdam on October 31, 2007, and was entitled “Gene therapy and gene transfer: from basic research in centres of excellence to industry development.” The second meeting was held in Brugge on November 16, 2008, with two main sessions: (1) a regulation round table, and (2) a “freedom-to-operate” workshop. On the occasion of the third meeting in Hannover on November 24, 2009, the theme was “GMP manufacture of gene therapy vectors and genetically modified cells: present status and future needs.” The fourth meeting took place during the ESGCT Congress in Milan on October 25, 2010, and was dedicated to “Bottlenecks in the industrial development of cell and gene-based therapeutics,” addressing five main topics: (1) R&D—how the industry can cooperate with academic research and clinical centers of excellence; (2) intellectual property issues in gene transfer research; (3) GMP manufacture and development of common standards: usefulness of a pan-European Infrastructure; (4) regulation—fostering simplification and accuracy; and (5) models for industry development—financing the development of gene and genetically modified cell therapies. The fifth meeting took place at the ESGCT Congress in Brighton on October 31, 2011, and was dedicated to “Industry–academic centres of excellence collaboration in challenges for early-phase clinical trials,” which focused on the following issues: (1) how academia and industry collaborate and on which ground it is maintained; (2) the main bottlenecks—research, intellectual property, timelines, management, regulatory issues, and so on; and (3) suggestions to improve these collaborations in the future.
In fact, these first attempts, along with first evidence of clinical successes, have now materialized into a major involvement of the private sector into the gene therapy field. Of note, the issues that were initially considered still hold in so far as collaboration between academic centers of excellence, cutting-edge technologies, and ethical issues in their clinical translation are concerned. While the private sector is pivotal to the clinical development of gene therapeutics, it is not the appropriate place to overlook and regulate all of the above-mentioned issues.
Integrating Ethics and Regulation With Science and Clinical Translation
Education, policy development, advisory ethical review, information sharing through conferences, publications, and public education that combines ethics and science and involves all relevant stakeholders in a comprehensive advisory role, as developed in CliniGene with enlightening views provided by Nancy King, hold the potential for complementing that of the regulatory authorities. This is to ensure early dialogue, robust accountability, high levels of transparency, open, clear, and timely flow of communications, and clarity of decision-making roles, all of which represent key values for safe clinical trials and, ultimately, effective gene and cell therapy medicinal products (GCTMPs). 41 –43 Indeed, research on GCTMPs must be translational, that is, coordinated across the development of technologies, assays, and materials, and from preclinical through clinical trials, rather than simply focusing on research with human subjects.
In order to foster safe and high-quality clinical gene transfer treatments, the CliniGene-NoE approached the definition of key criteria resulting from interesting preclinical results, which enable the decision as to whether it is a “go” or a “no-go” to the clinic with a reasonable enough margin of confidence toward foreseeable success. 41 Patient advocates have been involved all along, providing pivotal added value. The Clinigene-NoE has aimed to: (1) avoid the reproduction of Phase I trials asking the same questions; (ii) prevent predictable failures from entering the clinical phase; and (iii) deliver practical results, opening new opportunities for funding research and clinical development, thereby favoring the expansion of a high-tech industry sector.
Prospective Vision for a Sustained European Society On Gene and Cell Therapy
Whatever the interest raised by gene therapy and its innovatory potential, the relevance of this approach constantly needs to be carefully considered in terms of feasibility, economical constraints, and ethical issues and confronting alternative treatments such as targeted drugs. When considering a specific disease, the schedule of conditions to achieve therapeutic benefit must be scrutinized. Indeed, there might be alternative or complementary approaches to gene and cell therapies, constituting its own therapeutic armamentarium, the review of which belongs to the relevant clinical communities.
The raison d'être of a Society for gene and cell therapy therefore lies first in the technology and the knowhow to design its specificity and safety, whatever the application under consideration. In fact, the life-science community at large owes a lot to the gene transfer community, as mentioned by the ESGCT President in his recent letter: “The development of powerful technologies for efficient and safe gene transfer with minimal impact on target cell biology, regulated transgene expression and precise genome editing are just some examples of our legacy to the daily work of countless investigators and laboratories.”28
Because of the CliniGene program and actions, the necessity of streamlining experimental research and overcoming fragmentation has become evident. 44 The creation of a Pan-European resource for gene transfer vectors toward clinical application has emerged. 29,45 A nonprofit initiative, a EU-funded infrastructure would be well positioned to respond quickly to the changing demands of this rapidly developing area of science. This would provide the opportunity not only to incorporate novel scientific and technical possibilities, but also to create the appropriate ethical, regulatory, and public communication frameworks necessary to secure public endorsement to legitimate clinical gene transfer and cell therapy research. In structuring a distributed infrastructure with integrated governance, coordinated services, one-stop-shop access to services, the objectives are the following: (1) to build up a Pan-European infrastructure of vector engineering facilities providing state-of-the art gene transfer vectors toward preclinical developments of gene therapy and stem-cell engineering; (2) to serve a community of users in providing advice on the best system and accompany their project in providing prototypes and material; (3) to develop efficient and safer emerging technologies relying on multidisciplinary expertise in a coordinated manner; and (4) to provide access to complementary skills in order to answer the needs of the scientific community addressing a wide scope of applications and conditions. This infrastructure will help harmonize practices and quality in the design and production of vectors and genetically modified cells, thereby favoring the expansion of a high-tech industry sector through appropriate technology transfer. In fact, once proof of efficacy is gathered, technology can be transferred to the private sector, which is the appropriate channel to take over further phases of development toward marketing authorization (Fig. 3).

Added value of a non-profit EU-infrastructure: (i) integration through the European Society for Gene and Cell Therapy including a strong Ethics and Policy component; (ii) funding of innovative experimental research and emerging technologies; (iii) fostering technology transfer and clinical translation in collaboration with the private sector.
The EC-DG research has been approached with view to launching a specific line of call. A European gene and cell therapy infrastructure is likely to expand the scope of the Society, with a capacity to fund experimental and ethical research toward accelerating clinical translation of cutting-edge technology. Such a prospect is particularly relevant at a time where (1) multiple companies are currently entering the field, a significant move that requires strong reference material, methods, and ethical standards; and (2) CRISPR-Cas9 and other systems pertaining to homologous recombination toward precise genome editing are currently revolutionizing the field, with the added advantage of being immediately applicable to dominant as well as recessive inherited genetic diseases. 46,47 For therapeutic purposes, such technology still needs to be accurately shuttled to the nucleus of target cells, calling on the expertise of the gene therapy community in so far as targeting, safety, and efficacy constraints are concerned.
Conclusion
Behind the disease and the tentative therapy, there is first and foremost the patient. Patients are the most concerned with innovative therapies, which they might perceive as hope for a miracle to happen. The community has a responsibility to move ahead and at the same time convey to patients measured and concerted expectations. Multidisciplinary interaction only makes fruitful exchanges possible between investigators in basic science and clinicians in order to help overcome the many bottlenecks and draw a critical path between basic genetic discovery and clinical implementation. This has been the basis for the creation of the ESGCT and later of CliniGene as its professional companion in the ethical and regulatory field and experimental arm funded by the EC. It will soon be inevitable that a continuation of the CliniGene-NoE 48 actions will be necessary, taking from Inder Verma's (Chair of the Clinigene International Committee) word of wisdom : “In science, we build up on what already exists, learning from others. Creativity comes from the ability to see the data, integrate them and extrapolate from them. You multiply by sharing: share your reagents, share your ideas openly and freely because science is a collaborative effort: no single person can do everything” (Vilcek Prize, 2008). The prospect of building up a strong nonprofit European infrastructure also warrants the robust expansion of a high-tech industry sector, with best possible ethical landmarks.
Footnotes
Acknowledgments
The author would like to thank Pr Michel Boiron, Pr Lucio Luzzatto, Didi Jasmin (ESH-EHA), Pr Klaus Cichutek (President, PEI), Fernand Sauer (EC-DG Sanco), Octavi Quintana-Trias (EC-DG Research), Dr Fatiha Sadallah (EC-DG Research); Celia Tunc and Nicolas Creff, the wonderful CliniGene managers.