
Abstract
In 2003 in China, Peng et al. invented the recombinant adenovirus expressing p53 (Gendicine) for clinical tumor virotherapy. This was the first clinically approved gene therapy and tumor virotherapy drug in the world. An oncolytic herpes simplex virus expressing granulocyte-macrophage colony-stimulating factor (Talimogene laherparepvec) was approved for melanoma treatment in the United States in 2015. Since then, oncolytic viruses have been attracting more and more attention in the field of oncology, and may become novel significant modalities of tumor precision imaging and radiotherapy after further improvement. Oncolytic viruses carrying reporter genes can replicate and express genes of interest selectively in tumor cells, thus improving in vivo noninvasive precision molecular imaging and radiotherapy. Here, the latest developments and molecular mechanisms of tumor imaging and radiotherapy using oncolytic viruses are reviewed, and perspectives are given for further research. Various types of tumors are discussed, and special attention is paid to gastrointestinal tumors.
Introduction
M
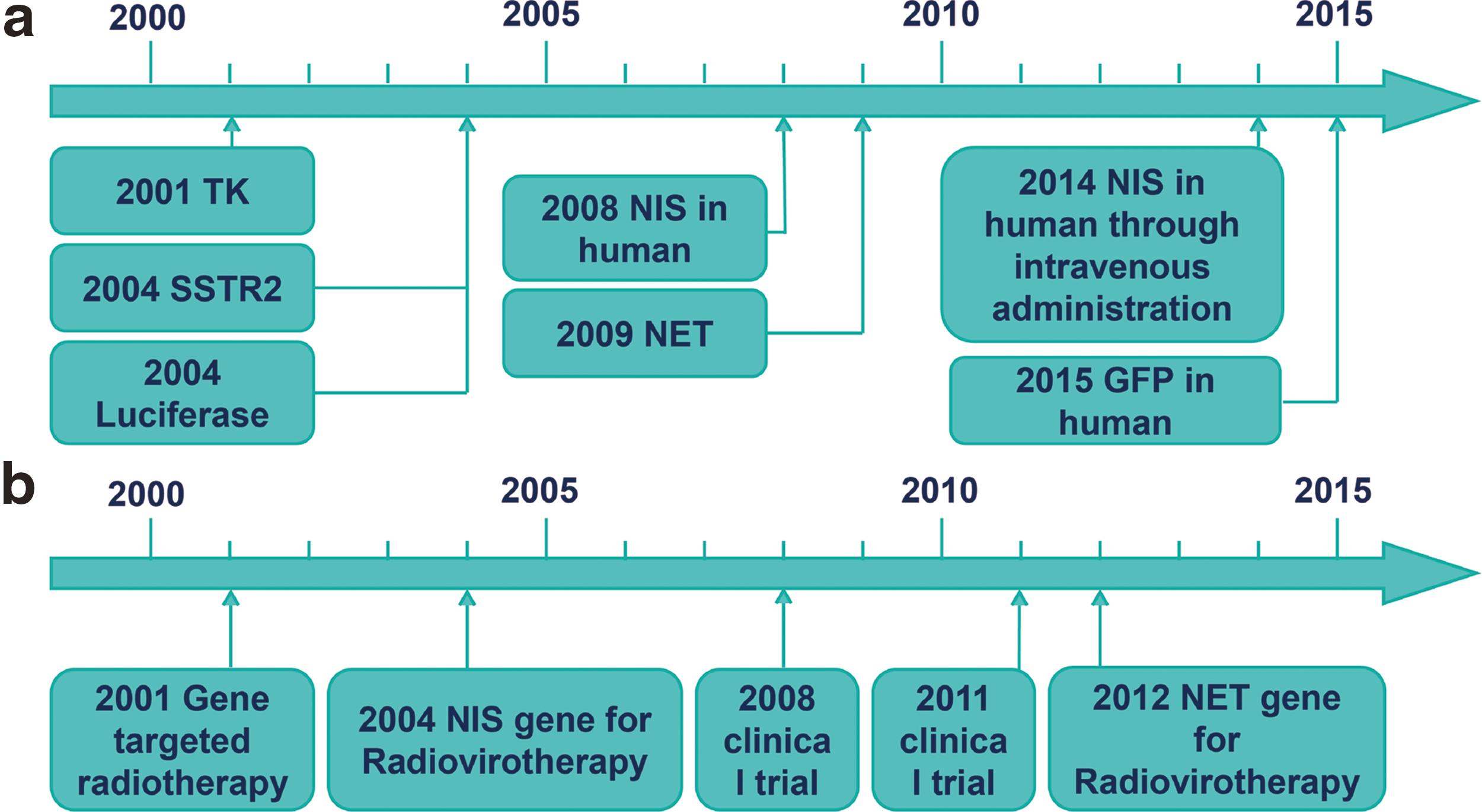
The important events of tumor imaging and radiotherapy using oncolytic viruses.
Here, current tumor imaging using oncolytic viruses is reviewed in the following four areas: (i) optical imaging, (ii) nuclear medical imaging, (iii) magnetic resonance imaging (MRI), and (iv) ultrasonic imaging (Table 1). The recent findings regarding radiotherapy using oncolytic viruses are also reviewed (Table 2). Oncolytic virus mediated imaging and radiotherapy in gastrointestinal tumors is summarized.
Experimental evidence and mechanism of imaging using oncolytic viruses
Ad5, adenovirus serotype 5; Ad5/3, adenovirus serotype 5/3; ADV, adenoviruses; BLI, bioluminescence imaging; CT, computed tomography; eGFP, enhanced green fluorescent protein; FDG, fluorodeoxyglucose; FEAU, 2′-fluoro-2′-deoxyarabinofuranosyl-5-ethyluracil; FI, fluorescence imaging; FIAU, 5-iodo-2′-fluoro-1-beta-D-arabinofuranosyluracil; HSV, herpes simplex virus; MOI, ratio of viral plaque forming unit to cancer cells; MRI, magnetic resonance imaging; MV, measles virus; ODTI, optoacoustic deep tissue imaging; PET, positron emission tomography; SPECT, single-photon emission computed tomography; TK, thymidine kinase; VSV, vesicular stomatitis virus; VV, vaccinia virus.
Experimental evidence and mechanism of radiotherapy using oncolytic viruses
vvDD, double-deleted vaccinia virus; Chk1, checkpoint kinase 1; PFU, plaque-forming units.
Tumor Imaging Using Oncolytic Viruses
Optical molecular imaging
Due to high sensitivity and simple operation, optical molecular imaging has become an essential technique to study tumor imaging using oncolytic viruses (Table 3).
The comparison between different tumor imaging technologies mentioned in this review
Bioluminescence imaging
Luciferase is a biocatalyst that converts chemical energy into light energy using adenosine triphosphate (ATP) and luciferin as reaction substrates. The luminescence intensity is proportional to the amount of ATP and luciferase. After being infected with the luciferase-expressing oncolytic viruses, cancer cells generate luciferase (Fig. 2). Following injection of the exogenous luciferins, the bioluminescence detector of corresponding imaging equipment forms images by detecting the bioluminescence released from the oxidation. There are many luciferases, including Firefly luciferase, Renilla luciferase, and Gaussia luciferase. The firefly luciferase gene is the most commonly used for in vivo imaging. Bioluminescence imaging has recently been successfully used in mouse models for evaluating the oncolysis kinetics of oncolytic HSV, 7 determining the combination therapy effects of oncolytic virotherapy and immune checkpoint blockade, 8 and tracking the replication of oncolytic parvoviruses, adenoviruses (ADV), HSV-1, vaccinia virus (VV), measles virus (MV), and vesicular stomatitis virus (VSV) 9 (Table 1).

The mechanism of tumor imaging and radiotherapy using oncolytic viruses.
Fluorescence imaging
Green fluorescent protein (GFP), found in jellyfish and other invertebrate marine animals, is widely used to detect tumor growth, invasion, and metastasis. When stimulated by ultraviolet or blue light, GFP emits green light efficiently and stably (Fig. 2). This protein and its enhanced fluorescent protein have been expressed in mouse models by most of the oncolytic viruses, including Newcastle disease virus (NDV), VSV, HSV-1, MV, ADV, and VV, 9 to evaluate the oncolytic viral therapy efficiency directly 10,11 or to evaluate the effects of other novel imaging technologies as a control. 12,13 Fluorescence-guided surgery (FGS) has also been studied for accurate surgical navigation in mice. For example, Kishimoto et al. used a GFP-expressing ADV for FGS in a disseminated colon and lung cancer model. 14 Yano et al. used a red fluorescent protein (RFP)-expressing ADV in a lung-tumor mouse model. 15 Although FGS has not been tested in humans until now, these animal studies show that it is reasonable to use FGS in patients in the future. Moreover, a Phase I clinical trial using GFP-expressing VV (GLV-1h68) has been completed, demonstrating its effectiveness of monitoring viral delivery and patient safety through intravenous administration (Tables 1 and 4).
The ongoing clinical trials investigating tumor imaging and radiotherapy using oncolytic viruses
Photoacoustic imaging
Photoacoustic imaging is based on the photoacoustic effect. When target tissue is irradiated by a short-pulse laser beam, the light absorption in the tissue is translated into heat, which increases thermoelastic expansion. Finally, heat energy and mechanical energy within the organ or tissue propagate ultrasound waves, which are used for imaging. 16 The image contrast is related to the light absorption, and the light absorption is correlated with the endogenous molecules such as melanin, oxygenated and deoxygenated hemoglobin, and exogenous contrast agents such as nanoparticles. 17 Based on this principle, Stritzker et al. used oncolytic VV strain GLV-1h68 as carriers of key genes of melanogenesis, tyrosinase (Tyr) gene, tyrosinase-related protein 1 (Tyrp1), and tyrosinase-related protein 2 (Tyrp2) gene to treat tumor-bearing mice. They provide evidence that the expression and accumulation of melanin by oncolytic viruses can be used as a diagnostic mediator in photoacoustic imaging (Table 1). 18 However, melanin overproduction inhibited viral replication. Therefore, in a further study, a doxycycline-regulated inducible system was used to decrease this inhibition effect. 19
In conclusion, prominent advantages in optical imaging include non-ionizing radiation, its noninvasive nature, its high sensitivity, its low cost, and the fact that it can be detected in real time. However, compared to other imaging technologies, the main limitations of optical imaging are the shallow light penetration, light scattering, and absorption in tissue (Table 3). 20 The prospective development direction of optical imaging is to conquer the limitation of imaging depth through combining endoscopic optic technology and intraoperative imaging. The association of optical imaging with multimodal imaging can also accelerate the clinical application.
Nuclear medical imaging
Since began in 1950s, nuclear medical imaging, especially radionuclide imaging, has been widely used, and the development and application of the targeted radioactive tracer laid the groundwork for molecular imaging. 3,21 Radionuclide imaging has high sensitivity (Table 3). Picomolar to nanomolar concentrations of radiotracers can be detected by nuclear medical equipment such as scintigraphic scanners, γ-cameras, positron emission tomography (PET) scanners, and single-photon emission computed tomography (SPECT) scanners. The tissue resolution of PET and SPECT has been significantly improved by the combination of nuclear medicine equipment and traditional medical imaging technology such as computed tomography (CT) and MRI (e.g., PET/CT, SPECT/CT, and PET/MRI). PET/CT can provide not only anatomical information, but also information about metabolism, receptor distribution, and expression level. Oncolytic viruses express reporter genes in tumor cells, which gather exogenous radionuclides detected by the equipment (Fig. 2). Three widely used reporter genes are focused on below, and less reported reporter genes are also summarized (Table 1). It is believed that there will be clinically approved oncolytic viruses for radionuclide molecular tumor precision imaging in the future.
Human sodium–iodine symporter gene
The human sodium–iodine symporter gene (hNIS) is one of the most mature nuclear medicine reporter genes. 9,22,23 hNIS protein naturally exists in the thyroid, salivary gland, gastric mucosa, and mammary gland. 24 hNIS is expressed on the cell membrane surface (Fig. 2). hNIS transfers various kinds of gamma-emitting radioisotopes such as radioiodine (123I, 124I, 125I, and 131I), technetium in the form of anionic pertechnetate (99mTcO4−) and perrhenate (186, 188Re) into the cells. 9,25 hNIS has been cloned into MV, VSV, ADV, and VV for tumor imaging, viral replication, and biodistribution in animal models (Table 1). 9
Among the completed clinical trials using oncolytic viruses and hNIS, the majority of adverse events were mild (grade 1–2), and no dose-limiting toxicities or serious adverse events were observed (Tables 1 and 4), demonstrating their safety. 26,27 Barton et al. used an oncolytic ADV-hNIS to treat prostate cancer patients through intraprostatic injection, and found that the viral replication, detected by SPECT imaging, peaked 1–2 days post virus administration and lasted up to 7 days, demonstrating the feasibility of ADV-hNIS mediated imaging in human gene therapy. 27 Among all 12 patients in this research, 98% of the adverse events were grade 1 or 2, with grade 3 lymphopenia occurring in two patients due to the prodrug therapy and grade 3 genitourinary adverse events occurring in one patient due to the radiation. In 2015, Galanis et al. used an oncolytic MV-NIS to treat ovarian cancer patients intraperitoneally. They observed NIS expression in tumors of three patients by the absorption of 123I on SPECT/CT among 13 patients treated at the viral dose of 109 TCID50. 26 Most common adverse events in this research were grade 1 or grade 2, but one patient experienced grade 2 hypotension, grade 2 fever, grade 3 direct bilirubin increase, and grade 3 neutropenia, probably due to an allergic reaction. Infectious etiology was ruled out, and the Vero cell-based virus production methodology used in this patient was suspected to be the reason for the allergic reaction because those who administrated the virus generated by HeLa cell–based methodology did not experience an allergic reaction. Russell et al. evaluated the tumor targeting of oncolytic MV-hNIS in two myeloma and multiple plasmacytoma patients through intravenous infusion, 28 and showed clear tumor imaging by MV-hNIS in both patients. Interestingly, it was found that the sizes of lesions in hNIS-mediated SPECT/CT imaging were different from those in normal fluorodeoxyglucose (FDG) PET imaging. The authors concluded that the difference may have been caused by variable uptake of 131I by lesions due to the heterogeneity of viral replication. Both patients became febrile, tachycardic, and hypotensive 2 h after virus infusion. A superficial venous thrombosis was detected in one patient and then dissolved within 1 week, and there were no evidences documented that thrombosis was due to virotherapy. However, the NIS imaging system was not always successful in the clinical trial due to the oncolytic viruses, the viral dose and administration routes, the patient type, and even the sensitivity of the PET and SPECT scanners. 25 Rajecki et al. failed to image the replication of an oncolytic adenovirus expressing the hNIS gene in a cervical carcinoma patient with metastasis due to inefficient native E3 promoter driving hNIS. 29 Risk management of oncolytic virotherapy is a focal point in clinical research, and close attention has been paid to this. There are at least three major origins of risk. First, oncolytic viruses can cause adverse events, for example nausea, flu-like symptoms, transaminitis, and fatigue. Apart from that, the potential pathogenicity of viruses should not be ignored. For example, HSV-1 causes gingivitis, keratoconjunctivitis, and encephalitis; ADV causes respiratory tract infections; MV causes measles. 30 Fortunately, under the conditions where relevant viral genes have been modified to ensure safety, such potential adverse events have rarely been reported in clinical research. Second, exogenous genes are potentially toxic for humans. Third, the drugs used for different imaging technology may result in side effects in humans. For example, radioiodine can be absorbed by normal organs that express hNIS, and then it will disturb the tumor signal and injure normal cells. Therefore, it is recommended that L-thyroxine or other exogenous iodine is administered before radiovirotherapy in order to decrease radionuclide absorption by normal tissues.
A search was made for clinical trials in China (
Human type 2 somatostatin receptor gene
Somatostatin (SST) is a multifunctional peptide produced by neuroendocrine cells and many other cells in the brain, pancreas, gastrointestinal mucous membrane, kidney, and peripheral nervous system. 31 The human type 2 somatostatin receptor gene (hSSTR2) is localized on the cell membrane of targeted tumor cells, and shows high affinity for natural SST and radioactive nuclide labeled synthetic analogues such as pentetreotide, octreotides, and lanreotide (Fig. 2). 32 However, one hSSTR2 protein can bind only one radiolabeled ligand on the cell membrane. Thus, the amplification for the intracellular downstream signal is not as significant as hNIS (Fig. 2). McCarty et al. successfully used oncolytic VV-hSSTR2 for tumor imaging in nude mice with 111In-pentetreotide (Table 1). 33 As with other reporter genes, naturally occurring hSSTR2 and hSST may potentially disturb the imaging, and so combining hSSTR2 with other reporter genes may resolve the problem. 23 In 2016, Wang et al. reported in the Journal of Nuclear Medicine that oncolytic VV-NIS-hSSTR2 showed improved imaging with 99mTc-pertechnetate and 111In-octreotide, and improved therapy with 131I radionuclide in vivo in mice (Table 1). 34
Thymidine kinase gene
The HSV-1 thymidine kinase (HSV1-TK) gene, a non-mammalian TK, can phosphorylate its radiolabeled nontoxic pro-drugs such as purine nucleoside derivatives and acyclovir derivatives and trap the toxic drugs in tumor cells for the purpose of imaging and therapy (Fig. 2). 22,35 Jacobs et al. first demonstrated the feasibility of using oncolytic viruses with TK for tumor imaging in vivo noninvasively in a tumor-bearing animal model in 2001 (Fig. 1). 5 In 2011, Abate-Daga et al. successfully used a novel oncolytic adenovirus expressing human immunodeficiency virus transactivator 8 (Tat8)-TK fusion protein in the tumor-bearing mouse model for PET imaging and antitumor therapy (Table 1). 35,36 However, in clinical research, oncolytic HSV1716 was used to treat patients with malignant glioma by intratumoral injection, but 123I-FIAU and SPECT imaging showed no difference before and after treatment. 37 The author concluded that the limited expression of the TK gene and the insufficient extent of viral replication may be the reasons that led to low 131I-FIAU concentrations in tumors. Moreover, the sensitivity of 123I-FIAU and SPECT imaging may be not enough to differentiate the 123I-FIAU absorption of the tumor from the background signal. The interference of the high background signal is the main limitation for tumor imaging using the TK gene in patients, 38 indicating that oncolytic viruses with more powerful TK gene expression and imaging systems with higher sensitivity such as PET are needed for clinical application. In another recent clinical trial (NCT03029871), an oncolytic ADV-TK, Ad5-ycd/muttksr39rep-ADP, is being tested for its PET imaging and therapy effects in non-small-cell lung cancer patients (Table 4).
In addition, an oncolytic vaccinia virus expressing human norepinephrine transporter (hNET) was successfully used for both tumor therapy and tumor deep-tissue imaging (Table 1). 39
Magnetic resonance molecular imaging
Compared with the traditional magnetic resonance imaging (MRI), magnetic resonance molecular imaging (MRMI) has higher imaging specificity and sensibility due to the contrast agent and molecular probes, and can be used to investigate the function of molecules in cells under normal or pathologic conditions in vivo and noninvasively. Since Reimer et al. used ultra-small superparamagnetic particles of iron oxide (USPIO) coated with arabinogalactan targeting asialoglycoprotein receptors for liver imaging in 1990, 40 MRMI has become a rapidly developing and important field (Table 1).
Reporter gene
There are many reporter genes in MRMI, including tyrosinase (Tyr), β-galactosidase (β-gal), transferrin receptor (TfR), creatine kinase (CK), and ferritin genes. Some of these genes and other new techniques of MRI have been applied in oncolytic viruses for tumor imaging (Table 1).
The level and activity of Tyr were positively correlated with the amount of melanin synthesis in human melanoma cells. Melanin has a high affinity for many kinds of metal ions, and forms chelate with paramagnetic iron ions to reduce T1 relaxation times and thus enhance the T1 signal of MRI (Fig. 2). 41 Stritzker et al. successfully used an oncolytic VV-Tyr for MRMI in mice, suggesting that melanin overexpressing oncolytic viruses are worth testing in clinical trials for tumor MRMI (Table 1). 18 The chemical exchange saturation transfer (CEST) effect in MRI has also been used for oncolytic virus mediated tumor imaging. Farrar et al. used an oncolytic HSV expressing lysine-rich protein (LRP) to infect glioma-bearing rats, and demonstrated the ability of LRP reporter to enhance CEST and MRMI of tumors (Table 1). 42
Other novel imaging methods
Almstatter et al. assembled oncolytic virus particles with magnetic nanoparticles (MNPs), and found that the local magnetic field becomes uneven through the MNPs, which influences the detected motion of hydrogen protons (Table 1). 13 Hemminki et al. used MRMI and magnetic resonance spectroscopy (MRS) to detect the antitumor effects of an oncolytic adenovirus expressing human GM-CSF gene, and found that there were different image characteristics in different phases in the MRMI and MRS (Table 1). 43
MRMI can be used not only to detect specific proteins, but also to obtain anatomical and functional information. The tissue resolution of MRI has reached micron level, which is an advantage for MRI compared to other imaging technology (Table 3). However, with low imaging sensitivity, current research on oncolytic virus mediated MRMI is still at the early and preclinical stage. With the development of modern sensitive MRI equipment and advances in molecular biology technology, MRMI should go a step further in tumor imaging using oncolytic viruses.
Ultrasound molecular imaging
In recent years, with the development of ultrasonic microbubbles and ultrasonic testing technology, contrast-enhanced ultrasound is no longer confined just to obtaining the information of blood perfusion from the tissue, but it is also applied to ultrasound molecular imaging. 44 The use of targeted ultrasound contrast agents such as targeted microbubbles for ultrasound molecular imaging has attracted increasing attention from researchers. Unfortunately, ultrasound molecular imaging has not been used for oncolytic virus mediated tumor imaging. The possible reason may be that research for oncolytic virotherapy needs more mature imaging modality such as nuclear medical imaging and optical imaging. The advantages of ultrasonic imaging are very obvious, such as it being safe, convenient, noninvasive, and inexpensive compared to other diagnostic imaging methods. It is predicted that ultrasound molecular imaging will play an important role in tumor imaging using oncolytic viruses in future.
Radiotherapy Using Oncolytic Viruses
About half of cancer patients receive radiotherapy. 45 The mechanism of radiotherapy is to induce DNA damage in the tumor cells, 46 including pyrimidine or purine lesions, single-strand breaks, and, the most deleterious, double-strand breaks. 47 However, radiotherapy can cause radio-resistance of tumor cells and damage to the surrounding normal cells, leading to significant side effects, which may be reduced using charged particles such as high-energy protons and carbon ions, 48 targeted radiotherapy, 49 and radiotherapy combined with other treatment modalities. The excellent tumor selectivity of oncolytic viruses improves therapy effects and side effects of radiotherapy. The combination of tumor radiotherapy and virotherapy may be classified into three aspects: (i) oncolytic viruses combined with standard external beam radiotherapy (EBRT) as a radio-sensitizer; (ii) oncolytic viruses used for tumor targeted radionuclide therapy; and (iii) oncolytic viruses combined with EBRT and radionuclide therapies (Table 2).
Oncolytic virotherapy combined with EBRT
In both preclinical and clinical studies, the combination of oncolytic virotherapy and radiotherapy showed synergistic therapeutic effects for tumor treatment. On the one hand, the uptake, gene expression, and replication of oncolytic viruses can be increased by radiation. On the other hand, the oncolytic viruses can act as a radiation-sensitizing agent to enhance the effect of radiotherapy. 6 In a recent clinical trial, Markert et al. used a combination of a mutant HSV-1G207 and radiotherapy to treat nine malignant glioma patients, demonstrating its safety and potential clinical effects (Table 2). 50 Undue toxicity was not produced by this combination treatment, and most adverse events were grade 1 or grade 2. Though this was a Phase I study and there were no controls due to the limited patient numbers, positive radiographic responses occurred in two patients who were HSV-1 seronegative, and stable disease or partial response occurred in 6/9 patients. In a Phase II clinical trial in 2014, an oncolytic adenovirus combined with intensity modulated radiation therapy was used to treat 44 prostate cancer patients (Table 2), demonstrating a better therapeutic efficacy than radiotherapy alone, while most adverse events (98%) were grade 1 or grade 2. 51 Different Phase I and Phase II clinical trials using a combination of oncolytic virotherapy with EBRT have been published with similar promising results in recent years. 50,52,53 In particular, the first clinically approved tumor virotherapy drug, Gendicine, proved to act synergistically with radiotherapy. 54
Radiovirotherapy: oncolytic viruses used for targeted radionuclide therapy
The concept of radiovirotherapy was first defined by Dingli et al. in 2004 as the combination of tumor virotherapy and virus mediated radionuclide therapy (Fig. 1). 55 After cancer cells were selectively infected by oncolytic viruses engineered to express exogenous genes (such as hNIS), radionuclides (such as 131I) from local or intravenous administration were enriched in the cancer cells, thus enhancing therapeutic effects and reducing the side effects of radiovirotherapy (Fig. 2 and Table 2, and section above on the hNIS gene).
Synergy between viral oncolysis and radiotherapy was observed in most studies. However, some issues need to be studied further (Table 2). Penheiter et al. used oncolytic MV-NIS to infect mice with human pancreatic cancer xenografts and treated mice with different doses of 131I. Then tumor development and mouse survival were monitored. It was found that radiovirotherapy achieved delay in tumor growth but did not prolong survival compared with 131I alone or MV-NIS alone due to the uneven virus distribution. 56 Reiecki et al. found that radiovirotherapy was no better than virotherapy alone due to the lack of extra iodine administered before radiovirotherapy, the rapid 131I efflux, and the lack of a high early activity promoter. 57 Reddi et al. compared the therapeutic effects between the MV-NIS + 131I and MV-NIS alone for anaplastic thyroid cancer, and no statistical difference was observed in tumor volume between these two groups due to inappropriate dosage of 131I administration and low radiosensitivity at 2 mCi dose level of KTC-3 xenografts. 58 These results suggest that many uncertain factors might influence the effect of radiovirotherapy. Trujillo et al. studied some factors that are relevant to the efficacy of radiovirotherapy, such as viral dose and spread, radioiodine uptake, and efflux, and indicated that radioiodine efflux and viral spread played a major role in the outcome of radiovirotherapy. 59
Apart from the hNIS gene, other genes have also been used for radiovirotherapy (Table 2). In an in vitro radiovirotherapy experiment with oncolytic VV-hSSTR2, no statistical difference was observed in the growth of MC-38 cells between radioactive drugs and radiovirotherapy, though both resulted in decreased growth. 60 A persuasive in vivo experiment is planned. Sorensen et al. used oncolytic HSV-NET (HSV1716) and radiolabeled noradrenaline analog 131I-metaiodobenzylguanidine (131I-MIBG) to treat human tumor xenografts, and showed that combination treatment resulted in less tumor volume than each monotherapy, and sequential administration, in which HSV1716 was injected 24 h before the injection of 131I-MIBG, achieved higher survival than simultaneous injection. 61
In addition to these preclinical studies, clinical trials have also been performed (Tables 2 and 3). An oncolytic ADV-hNIS had been tested in six prostate cancer patients for radiovirotherapy, whereby 200 mCi of 131I was administrated after the viral injection, but the mean absorbed dose was only 7.2 ± 4.8 Gy, which is far below the standard dose that can elicit the effect of radiotherapy. 62 The authors believe that the viral dosage and the ability of viral propagation may not have been enough for radiovirotherapy. Although all adverse events in this research were transient, it is noteworthy that incidence and severity of adenovirus therapy related adverse events were increased in the group of higher virus dose, including flu-like symptoms, transaminitis, and fatigue, indicating that more attention needs to be paid to the toxicities of radiovirotherapy when using a higher viral dose. A Phase I clinical trial of targeted radionuclide therapy is now under way to show the side effects and best viral dose with radioiodine for prostate cancer patients (NCT00788307).
These preclinical and clinical studies indicate that before the clinical application of radiovirotherapy, some issues should be resolved (Table 2). Some important future directions and perspectives for improvements include: (i) the dosage of virus and radionuclides should be enough for radiovirotherapy, and the best dosage should be tested in different tumor models; (ii) the most suitable interval time between the administration of oncolytic viruses and radionuclides should be tested 61 ; and (iii) the ability of viruses to be replicated and the expression level of radiotherapy genes are vital for the therapeutic effects, 62 and therefore robust replicative oncolytic viruses, viral replication promoting agents such as cyclophosphamide (CPA), 63 and the active promoter of radiotherapy genes such as the ubiquitous cytomegalovirus promoter 27 might be good improvements; (iv) administrating L-thyroxine or other exogenous iodine before radiovirotherapy should be considered in order to decrease the radionuclide absorption of normal tissues 64 ; (v) human thyroid peroxidase gene together with the hNIS gene might lead to longer retention of radioiodine 65 ; and (vi) concomitant use of agents to prevent the DNA repair after radiation damage such as specific checkpoint kinase 1 inhibition. 66
Radiovirotherapy combined with EBRT
This modality includes three antitumor therapies: oncolytic virotherapy, radionuclide therapy, and EBRT. Touchefeu et al. used not only the combination of these three therapies, but also a checkpoint kinase 1 (Chk1) inhibitor SAR-020106 to block DNA damage repair pathways, and indicated that radiovirotherapy combined with EBRT is more effective than single therapies. 66 This result suggests that multiple therapies using radiovirotherapy combined with EBRT may be a promising approach for clinical tumor therapy.
Imaging and Radiotherapy of Gastrointestinal Tumors By Oncolytic Viruses
Some unique pathological characteristics exist in gastrointestinal cancers, including the communication of digestive system with the external environment and the shallow location of gastrointestinal cancers. Due to these unique advantages, oncolytic virus mediated FGS and fluorescence endoscope imaging for gastric cancer have been used in animal models, and bright-field laparoscopy undetectable tumor nodules can be identified by a GFP fluorescence endoscope (Table 1). 67 Deep-tissue imaging can also be used in gastric cancer. In recent studies, an oncolytic vaccinia virus GLV-1h153, which expresses both GFP and hNIS, was used successfully for the visualization of gastric tumors and colorectal peritoneal carcinomatosis in nude mice (Tables 1 and 2). 12,68 Moreover, they can also be a therapeutic agent, killing gastric cancer cells. It is foreseeable that oncolytic virus directed fluorescent imaging will facilitate the progression of FGS and endoscope imaging for precision imaging and therapy of gastrointestinal cancer.
Several distinctive radiovirotherapy research studies have been reported (Table 2). The hSSTR2 gene was shown to suppress C-38 murine colon adenocarcinoma cells in targeted radionuclide therapy. 60 The hNIS gene was applied in colorectal cancer animal models, and the tumor volume was significantly reduced when oncolytic ADV-hNIS and 131I were administrated compared to hNIS-negative VV and virotherapy alone. 69 Moreover, a complete treatment regimen including MV-NIS, targeted 131I radiotherapy, EBRT, and Chk1 inhibitor showed better effects in colorectal xenografts models than each monotherapy or other combination therapies with three or two treatments of the whole treatment regimen. 66 This four-pronged regimen may represent future development, and these preclinical studies set the stage for future clinical research of radiotherapy using oncolytic viruses.
Concluding Remarks
This article has reviewed recent progress in tumor imaging and radiotherapy using oncolytic viruses. Current publications indicate that oncolytic viruses may be used not only for antitumor treatment, but also for tumor imaging through different molecular imaging techniques, and the combination of oncolytic virotherapy with radiotherapy may produce better antineoplastic effects. It is strongly believed that these new imaging methods and treatment approaches will accelerate the clinical application of oncolytic viruses, and provide new opportunities for both researchers and patients to fight cancer. On the one hand, oncolytic viruses have excellent specificity for the infection of tumor cells. To this end, they can be used as carriers for both tumor precision imaging and radiotherapy. On the other hand, due to oncolytic effects, the viruses may kill tumor cells when used for tumor imaging and generate synergistic effects when combined with radiotherapy. In addition, oncolytic viruses can be engineered according to the need of researchers for different functions.
In the field of diagnosis, different imaging techniques have different advantages. Multimodal imaging will combine the advantages of different imaging techniques. Therefore, it is important to investigate oncolytic viruses with the aid of multimodal molecular imaging in the future. In the field of therapy, the safety and efficiency of the radionuclide therapy using oncolytic virus followed by EBRT deserves more preclinical and clinical studies. It is hoped that oncolytic viruses will play a more important role in tumor precision imaging and radiotherapy, and promote the development of novel diagnostic and antineoplastic agents.
Footnotes
Acknowledgments
We thank Hubei province for funding to H.W.X. as a Chutian Scholar Distinguished Professor (20160527), and Yangtze University for funding to Z.J.W. as a graduate scholarship winner.
Author Disclosure
We declare that none of the authors have any financial or personal relationships with other people or organizations that could inappropriately influence the quality of the work presented in this manuscript. There is no professional or other personal interest of any nature or kind in any product, service, and/or company that could be construed as influencing the position presented in, or the review of, this manuscript.