
Abstract
The adoptive transfer of chimeric antigen receptor (CAR)-modified T cells is attracting growing interest for the treatment of malignant diseases. Early trials with anti-CD19 CAR T cells have achieved spectacular remissions in B-cell leukemia and lymphoma, so far refractory, very recently resulting in the Food and Drug Administration approval of CD19 CAR T cells for therapy. With further applications and increasing numbers of patients, the reproducible manufacture of high-quality clinical-grade CAR T cells is becoming an ever greater challenge. New processing techniques, quality-control mechanisms, and logistic developments are required to meet both medical needs and regulatory restrictions. This paper summarizes the state-of-the-art in manufacturing CAR T cells and the current challenges that need to be overcome to implement this type of cell therapy in the treatment of a variety of malignant diseases and in a greater number of patients.
The Principle of CAR T Cell Therapy
O
CAR T cells are medicinal cell products with the capability to migrate, to amplify, to release bioactive substances, and to execute specific effector functions toward cognate cells. The therapeutic activity against tumors is dependent on the functional capacity of the CAR T cells, which is defined by a number of variables, including the modular CAR composition, the cognate antigen, the binding affinity, the signaling moieties and the T cell maturation and proliferative capacity. In this context, the production procedure itself has a substantial impact on the fitness of the final CAR T cell product, involves a number of steps that are crucial to its clinical efficacy, and has to be performed according to the regulatory requirements for clinical applications. 3,4
The Growing Number of CAR T Cell Trials
Clinical trials with CAR T cells for the treatment of malignant diseases constitute a fast-growing field. In May 2016, about 100 ongoing trials were listed,
5
while there are now >200 trials that are registered with
CAR T cell therapy is becoming ever more established with the growing number of trials performed at different centers. Although remissions are induced by CAR T cells, the success rate still varies greatly between the trial centers; relapse rates of 21–45% have been reported for ALL. 17 –19 Discussion of the trial data is even more complex, since a number of technical variations and modifications of the CAR design make direct comparisons of clinical efficacy almost impossible. These variations include the modular CAR composition, CAR T cell production, the genetic modification procedure, patient pretreatment, and the CAR T cell dose, among others. A meta-analysis of CD19 CAR T cell trials revealed that lymphodepleting preconditioning and the CAR T cell dose are key factors for a favorable prognosis in the treatment of B-cell neoplasia. 17 Treatment of solid cancer lesions, for instance by targeting CEA 20 or Her2, 1 likely follows the same rules.
Production of CAR T Cells for Clinical Use
The increasing number of CAR T cell studies has initiated a process of continuous improvement in manufacturing under the conditions of good manufacturing practice (GMP). In most trials, the patient's peripheral blood mononuclear cells are harvested by leukapheresis, stimulated via TCR/CD28 and interleukin (IL)-2, virally transduced with the vector encoding the CAR, and expanded to clinically relevant numbers. The entire manufacturing process requires 7–22 days, usually 12 days. 13,21 Rigorous quality control management accompanies the process and governs the starting material, the entire production process, and the final product after harvesting. Apart from bulk T cell preparations, defined T cell subsets have also recently been used as starting material, and specific stimulation protocols are applied to promote the development of the cells into a preferred maturation stage. 22 –24 The apheresis product can be processed using various devices, such as Haemonetics Cell Saver5+, COBE2991, and Fresenius Kabi LOVO. Terumo Elutra and Biosafe Sepax deplete monocytes and isolate lymphocytes based on cell size. The CliniMACS device positively or negatively enriches T cells or subsets through antibody-coupled beads. The apheresis product is shipped to the manufacturing GMP facility under temperature control, fresh or cryopreserved. The subsequent CAR T cell manufacturing procedure includes T cell activation, viral transduction, expansion and, in most cases, cryopreservation, in a step-by-step process (Fig. 1). The patient's own immune cells are generally used as starting material. However, allogeneic donor T cells have also been engineered with a CAR and depleted in TCR expression, 25 which would overcome some limitations related to using patient's own T cells, such as poor cell counts, quality, and functional capacity due to the strong chemotherapeutic pretreatment. CD3+ T cells are most commonly used for CAR engineering. Isolated CD4+ and CD8+ T cells, 24 naïve T cells, 26 central memory, 27 or memory stem cells 28 have also been explored in some trials. So far, the most commonly used activation process involves super-paramagnetic beads coated with anti-CD3, anti-CD28 antibodies, such as Dynabeads, or polymeric nanomatrix Miltenyi MACS GMP TransAct CD3/CD28 beads coupled to agonistic anti-CD3 or anti-CD28 antibodies. 29 –31 Paramagnetic beads must be removed at the end of the manufacturing process, while the Miltenyi MACS GMP TransAct CD3/CD28 beads are biodegradable and do not require removal before further processing. A recent development by Juno Therapeutics uses a soluble T cell stimulating reagent, Expamer, for T cell activation prior to viral transduction. 32,33 The use of a soluble anti-CD3 antibody OKT3 and IL-2 supplementation is also reported for activation and expansion of a patient's CAR T cells. 13,34
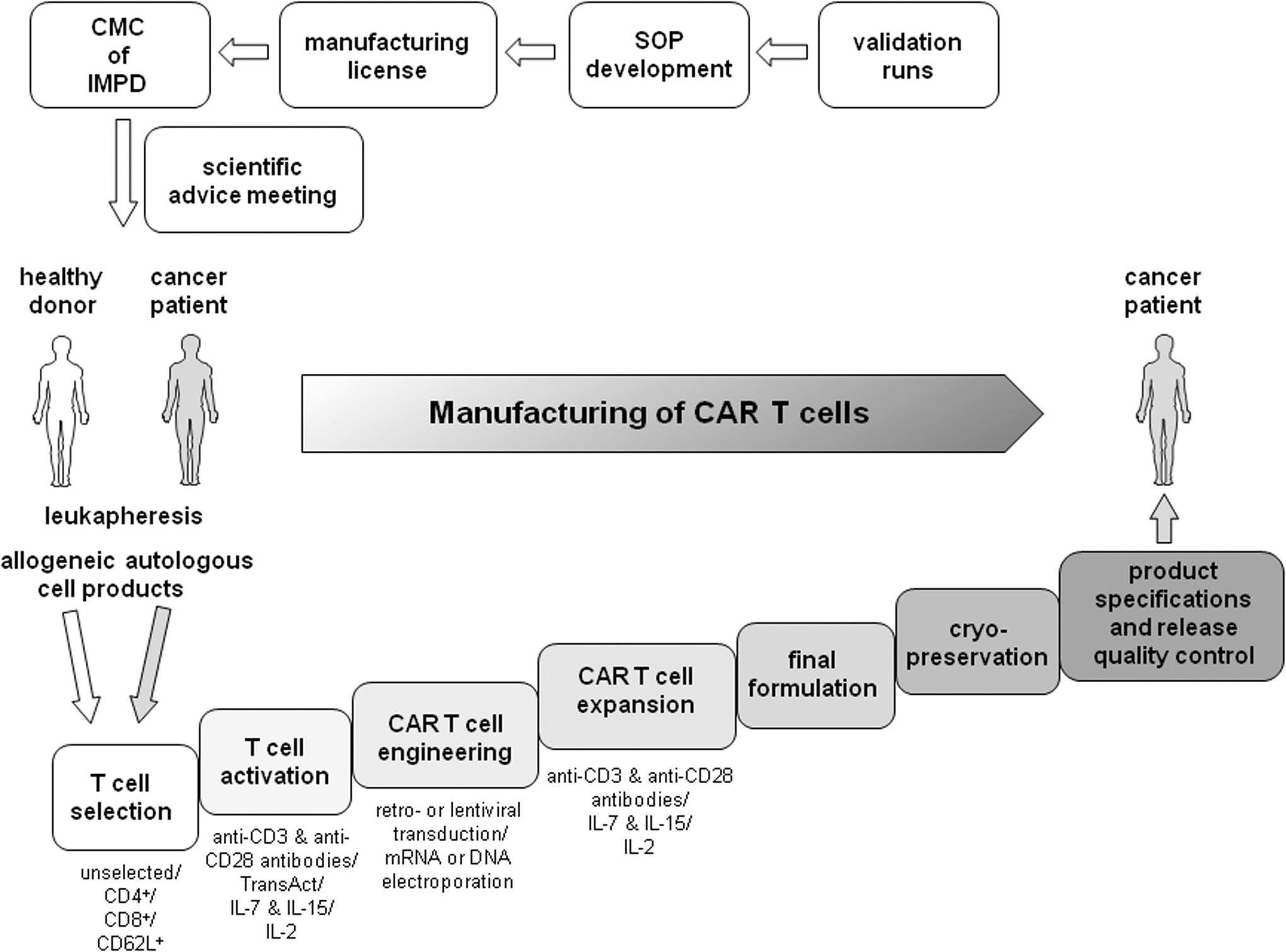
Good manufacturing practice (GMP)-compliant manufacturing of chimeric antigen receptor (CAR) T cells. A major technical obstacle to the widespread application of CAR-expressing T cells in cancer is the overall complexity of the GMP-compliant manufacturing process. In order to enter clinical trials, the relevant corresponding Standard Operating Procedures need to be generated, validation runs are required, and the application for manufacturing licenses has to be granted. Both the manual and automated processes for manufacturing CAR T cells from the patient or healthy donor include the isolation, activation, engineering, expansion, the final formulation, and cryopreservation of the cell product, as well as the definition of product specifications and the final release quality control.
The expansion of the T cell population is generally carried out after gene transfer and in the presence of IL-2 or, preferentially, in the presence of IL-7 plus IL-1535 in order to amplify the genetically modified T cells, but can also be performed prior to genetic engineering. 4,36 The entire process, so far, is a hands-on manufacturing procedure and is performed in bags, for example PermaLife®, Flexsafe®, Cellbag®, and VueLife®, on a rocking baseplate, allowing both media perfusion and efficient gas exchange. GE WAVE bioreactors with a rocking platform (GE Healthcare Life Sciences) are used as an alternative for the production of anti-CD19 CAR-modified autologous T cells (CTL019). 37 –39 The perfusion of the WAVE bioreactor allows for automatic feed and waste removal. These cell culture platforms are widely used by academic centers in early-phase trials. 37,40 The newly established G-Rex (Wilson Wolf) system with gas permeable membranes allows, in particular, the amplification of cells from low starting concentrations and the growing of cells in an incubator. 41,42
T cells are generally engineered with the CAR by viral transduction, and some trials have used DNA electroporation to modify cells. Replication-defective, transducing viral vector is prepared from supernatants of plasmid transfected producer cells, mostly HEK293T cells. 43 The plasmids for engineering the producer cells are usually (1) a plasmid encoding the viral structural protein (gag) and polymerase (pol), (2) a plasmid like VSV-G (env) for vector particle pseudotyping, (3) a vector encoding the Rev accessory protein, and (4) the plasmid harboring the CAR expression construct and regulatory elements. Commonly used vector systems are designed to prevent the generation of replication-competent virus particles by recombination during the production process. Virus stocks are harvested, multiple sub-batches are produced, impurities are removed, and the virus vector is finally purified, subjected to sterilizing filtration, and stored in vials under cryopreservation. The most common vectors are based on γ-retroviruses 44 –48 and lentiviruses, 49,50 with both vectors requiring mitogenic T cell activation for highly efficient transduction. Lentiviruses infect cells during activation and more easily infect nondividing cells than γ-retroviruses. 37 Other protocols use electroporation or a nucleofector device (Lonza) for T cell engineering with plasmid DNA that encodes the CAR.
For viral transduction, bags are coated with substances that facilitate virus aggregation, for instance, with GMP-grade human recombinant fibronectin fragments (e.g., Takara Bio). Other centers conduct viral transduction in tissue culture plates or flasks, often with centrifugation and without coating. The manufacturing processes themselves differ in multiple parameters, including the media used for T cell amplification (e.g., X-Vivo 15®, AIM V®, and TexMACS GMP®). A number of release specifications and in-process controls are implemented during and after the manufacturing process, including T cell number, cell viability, phenotypic characterization, CAR or other transgene expression, and impurity measurements. Finally, sterility, mycoplasma, and endotoxin recordings are made. Although the generation of replication-competent virus particles is highly unlikely with the vectors that are currently used, 51 replication-competent retrovirus/lentivirus testing using quantitative polymerase chain reaction is conducted throughout the entire production process. After CAR T cell application, the Food and Drug Administration (FDA) recommends patient follow-up for 15 years for the documentation of any potentially vector-related adverse events. 52 In early-phase trials, flow cytometric quantification of the CAR expression by the T cells in the final cell product is thus far accepted as an indirect potency assay. Validated functional assays will be mandatory for trials in advanced phases, such as cytokine secretion of the CAR T cells and cytotoxicity assays on the relevant target cells, to provide information on the functional capacities.
While CAR T cell manufacturing for early-phase trials is currently provided by some specialized academic centers, large-scale manufacturing is mostly carried out in partnership with companies, for example Molmed Milano with GSK, Tel Aviv Sourasky Medical Centre and National Cancer Institute with Kite Pharma/Gilead, Baylor College of Medicine with Cellmedica, University of Pennsylvania and Fraunhofer Institute of Cellular Therapeutics and Immunology Leipzig with Novartis, and Seattle Children Hospital, St. Jude, Fred Hutchison Cancer Center, and Memorial Sloan Kettering Cancer Center with Juno Therapeutics. In August 2017, Novartis was the first company to receive FDA-approved marketing authorization for Kymriah™ (tisagenlecleucel), shortly followed by Kite Pharma/Geliad for Yescarta™ (axicabtagene ciloleucel), both CD19-redirected CAR T cell products for the treatment of pediatric B-ALL and adult large B-cell lymphoma, respectively.
Recent Achievements Toward a Fully Automated Manufacturing Process
Due to the rapidly increasing number of patients who need CAR T cell therapy, there is a growing challenge in relation to producing cell products for each individual patient and standardizing the production and treatment procedure for multiple centers. With reference to manufacture, this includes both harmonized production protocols and automation platforms that allow reproducible and rapid production of cells, with every step strictly documented. An example of this is the Octane Cocoon™ cell culture and tissue engineering system, which is a patient-scale cell therapy platform as a central core of a series of cell and tissue therapy production systems and allows multiple manufacturing processes to run in parallel. Another example for automated and supervised manufacturing is CliniMACS Prodigy (Miltenyi Biotec), which allows T cell activation, transduction, amplification, and final harvesting of CAR T cells, with high transduction frequencies and high cell numbers in the same device and aims at integrating and fully controlling the multi-step process through a flexible programming suite and allows in-process sampling. 53 –55 CAR T cells were produced by lentiviral transduction using the CliniMACS Prodigy in quantities suitable for clinical applications. 56 While Mock et al. 55 started CAR T cell production with a portion of the leukapheresis product, Priesner et al. 54 used CD62L+-selected T cells in order to obtain a high number of naïve and central memory T cells for transduction with a lentiviral vector. Both groups reported an expansion rate of T cells of >30-fold after 2 weeks, which is in line with the step-by-step manufacturing protocols that are currently routinely used. MACS GMP TransAct CD3 and CD28 reagent was used for T cell activation. TexMACS™ GMP medium was supplemented with IL-7 and IL-15, and human serum was removed after the entire manufacturing process. The fully automated system was clearly time-saving in comparison with the hands-on handling process and provided an anti-CD19 CAR T cell product with ex vivo properties and an overall yield that were similar to those obtained with conventional processes. On the day of harvesting, Priesner et al. 54 used Composol® PS (Fresenius Kabi Ltd.) for the final formulation. In addition, using the CliniMACS Prodigy, Lock et al. 57 produced similar data for CAR T cells redirected against CD20, starting with CD4 and CD8 T cell selection; the CD4/CD8 ratio was maintained over the entire expansion process. The CAR T cell manufacturing process was further shortened and optimized, reducing the process to 6 days. 58 Very recently, Piscopo et al. 59 proposed some solutions to challenges that remain during the manufacturing process, including the use of alternative biomaterials, synthetic biology, metabolic engineering, process control, and automation. The achievements are clearly a step toward a harmonized and automated manufacturing protocol, and companies are currently anticipating treating several thousand patients per year. However, other barriers include insurance cover and contracting and site certification, among others.
The Regulatory Landscape for CAR T Cells in Europe and the United States
There are substantial regulatory differences in relation to CAR T cell therapy in the United States and in Europe due to the fact that CAR T cells are complex medicinal products that combine the properties of being a cell product, genetically modified and applied as a cellular immunotherapeutic product (Table 1). There is one regulatory body in the United States, the FDA, while the European Medicines Agency (EMA), together with the national authorities of each Member State and, finally, the local-state authorities, are responsible for regulatory affairs in the European Union (EU). Based on their biological and pharmacological complexity, CAR T cells are regulated by the German local-state authorities as substantially manipulated cells. In the EU, CAR T cells are classified as an Advanced Therapy Medicinal Product (ATMP). The legal framework is based on Directive 2004/23/EC, and subclassified as a Gene Therapy Medicinal Product (GTMP), which has to be manufactured in accordance with GMP. The so-called Tissue and Cells Directive defines the “standards of quality and safety for the donation, procurement, testing, processing, preservation, storage and distribution of human tissues and cells.” 60 In addition, Directives 2006/17/EC 61 and 2006/86/EC 62 provide amendments for starting materials. Regulation 1394/2007/EC as well as Directive 2001/83/EC 63 provide the overall framework for ATMPs, defining the centralized procedure for marketing authorization. Finally, Directive 2009/120/EC, the so-called ATMP Directive amending Directive 2001/83/EC, provides technical requirements and definitions for GTMP, as well as combined ATMPs. 64 In November 2017, the EU published a risk-based approach, taking into account the complexity of the respective ATMPs 65 and providing more flexibility in the manufacturing process, which predominantly depends on the risk related to decentralized processing, automation, and in-process controls, with traceability data also included. Finally, the standards for the quality control of medicinal products and of the substances used during the development, production, and marketing processes are listed in the European Pharmacopoeia (Ph. Eur.). 66
Comparison of regulatory aspects in the EU and United States
EMA, European Medicines Agency; EU, European Union; FDA, Food and Drug Administration; ATMP, Advanced Therapy Medicinal Product; HCT/Ps, human cellular therapy products
GMP-compliant manufacturing of CAR T cells remains challenging due to the high variability of the starting cell material as a consequence of the patient's intensive pretreatment and often poor immune cell status. Moreover, the transduction efficiency, the copy numbers of transmitted expression vectors, the level of CAR expression, the phenotype and maturation of CAR T cells, as well as the capacity of cells to respond to external signals are relevant factors that substantially impact the reproducibility and robustness of the manufacturing process and the performance and safety of the final cell product. Given the complexity in ATMP manufacturing, EU Directive 2001/20/EC aims to harmonize the regulation of clinical trials. However, some differences still exist between the EU Member States, including the classification as a genetically modified organism in some states, which requires an environmental risk assessment. Finally, the revision of the current regulatory system for clinical trials in academic centers 67 and the new EU Clinical Trials Regulation (EU Regulation No 536/2014) aim to harmonize the regulatory process and to avoid delays in clinical investigation.
A comparison of the regulatory situation in the United States and in the EU is difficult, since the processes are basically regulated in a different manner (Table 1). For instance, EU countries require current GMP (cGMP) compliance that is certified by a qualified person, while cGMP compliance in the United States is assessed by paper review. In the United States, CAR T cells are regulated as human cellular therapy products under 21 CFR 1271. The regulation is based on the statutory authority, granted to the FDA in section 361 of the Public Health Service Act, to prevent the spread of communicable disease. The general and permanent rules and regulations are published in the Federal Register by the executive departments and agencies of the U.S. federal government 68,69 ; 21 CRF 1271 defines general provisions and requirements for the registration and listing, donor eligibility, current Good Tissue Practice, and adverse-event reporting, as well as inspections and enforcement. 70,71 For excipients, USP <1043> refers to ancillary reagents, ancillary products, and process reagents and is classified into four tiers according to their risk factor. 72
Remaining Challenges
How can we produce an individualized cell product for a growing number of patients?
With an increasing number of patients being subjected to CAR T cell therapy, a centralized cell manufacturing facility needs to deliver the individualized products to various hospitals. The manufacturing process is currently based on manual procedures, mostly performed at academic centers or by specialized GMP units, which needs to be translated into an automated process run by specialized centers. Manufacturing by a few specialized centers that distribute the product to hospitals requires expedient transportation of the apheresis product from the patient to the manufacturing center and of the CAR T cell product from the center to the patient. Good distribution practice rules apply during transportation to prevent mismatches between the product and patient. To this end, an unambiguous tracking system was developed by the CARAT consortium. In contrast, decentralized production centers would require access to local GMP facilities with the appropriate equipment and trained personnel for cell manufacturing and virus production. Decentralized manufacturing in the relevant hospital would make the logistics easier. However, this still requires a broadly accepted level of standardization of the manufacturing process, and local production is likely associated with varying degrees of compliance with regulations.
A fully automated device for genetic cell engineering and T cell amplification would allow “in-house” and decentralized production of CAR T cells. Finally, the origin, traceability, composition, and certification must be accessible and harmonized in order to guarantee the quality and safety of CAR T cell products and to administer consistent treatment to patients.
How can we guarantee the quality of the cell product?
Given the complexity in the manufacturing process and clinical management of heavily pretreated patients, the scaling up from an academic institutional process for single patients in a highly specialized center to a process for hundreds of patients in various hospitals is challenging. The clinical success of CAR T cell therapy is strongly dependent on the effective coordination and standardization of the manufacturing and treatment processes. T cells obtained from leukapheresis display enormous patient-to-patient variability with respect to function and maturation; isolating CD4+ and CD8+ or CD62L+ T cells aims to provide more reproducibility in production and clinical efficacy. 28,73,74 CD4+ and CD8+ T cells are separately engineered with the CAR, amplified, and finally combined at a 1:1 ratio prior to application, aiming to ensure a more defined cell product. 24 However, the ratio of CAR T cells will alter shortly after infusion, and T cell maturation will progress, in particular after repetitive encounters with the target antigen, demanding additional strategies to keep the cells in a specific stage of maturation. Further critical quality criteria are the CAR T cell numbers, the level of CAR expression, and the functional capacities, such as cytokine release, target cell killing, and phenotypic markers of exhaustion. To ensure a uniform cell product, at minimum, these criteria need to be controlled during the entire manufacturing process.
Will “off-the-shelf” T cells provide a cell product for every patient?
T cells from each individual patient are currently engineered and amplified for treatment, which demands individualized cost- and labor-intensive production. So-called universal T cells, which can be applied to a number of patients independently of their major histocompatibility complex, would make a priori production of CAR T cells possible. Efforts are underway to use allogeneic CAR T cells, which are disrupted in their TCR α-chain locus in order to minimize allo-reactivity. 9,25,75,76 Further engineering is likely required to reduce the risk of immune destruction by the host immune response. However, such a universal CAR T cell would allow off-the-shelf delivery of cell products, providing more flexibility in the clinical management of patients. The option of using off-the-shelf CAR T cells is of relevance, since most cancer patients in advanced stages of the disease experience immune suppression with partial deficiencies in immune cell functions, which may result in poor T cell numbers from the leukapheresis product, insufficient T cell activation for viral transduction, or ex vivo amplification of engineered T cells. Indeed, a patient recently received an allogeneic CAR T cell product without severe alloreactivity, 25 demonstrating the basic feasibility of the strategy.
Will other immune cells be efficiently redirected toward tumors?
Cells of the innate immune system can also be specifically redirected toward target cells by an engineered CAR. 77 –82 Natural killer (NK) cells isolated from the peripheral blood are engineered with a CAR by retroviral transduction, and the established NK92 cell line can likewise be engineered with a CAR. 83 –85 While the amplification of primary NK cells to clinical doses is challenging, the use of CAR-modified NK92 cells has the advantage of off-the-shelf manufacturing and cell banking. CAR NK92 cells are irradiated before use, persist in the short term after application, and require repetitive administration.
Will there be CAR T cell products for the treatment of diseases other than cancer?
While all CAR T cell trials are currently exploring the treatment of malignant diseases, CAR T cells can also be used to target infected cells displaying viral antigens, including hepatitis B, 86 hepatitis C, 87 cytomegalovirus, 88 and human immunodeficiency virus. 89,90 Anti-Dsg3 antibody-producing B cells, which are pathogenic for pemphigus vulgaris, can be eliminated by CAR T cells. 91 Even T cells with auto-reactivity against auto-antigens can be eliminated by CAR T cells. 92,93 CAR-redirected regulatory T cells are aimed at controlling auto-immune diseases and graft-versus-host disease in the long term. 94 –97 Other applications can be envisaged, underlining the central role of manufacturing a CAR T cell product in a robust, reliable, and timely manner.
Footnotes
Acknowledgments
H.A. and U.K. are members of the “CD20 CARTime” consortium funded by a grant from the German Federal Ministry of Education and Research within the funding program “innovations for individualized medicine” (Fkz 01EK1507A-C). Work in the laboratory managed by H.A. was supported by grants from the Deutsche Forschungsgemeinschaft, Bonn, Deutsche Krebshilfe, Bonn, Bundesministerium für Bildung und Forschung, Berlin, Deutsche José Carreras-Leukämie Stiftung, München, Wilhelm Sander-Stiftung, München, Else Kröner-Fresenius Stiftung, Bad Homburg v.d.H., the German-Israeli Foundation, Jerusalem, and the Fortune Program of the Medical Faculty of the University of Cologne. Work in the institutes that U.K. is associated with was supported by grants from the German Ministry of Education, Berlin, the Integrated Research and Treatment Center Transplantation (IFB-Tx), the Deutsche Forschungsgemeinschaft, Bonn, the Alfred and Angelika Gutermuth-Stiftung, Berlin, as well as the Adolf Messer-Stiftung, Königstein.
Author Disclosure
H.A. serves on the Scientific Advisory Board of Miltenyi Biotec. U.K., S.A., and A.H. have no competing financial interests.