
Abstract
Previously, results at 2 years after subretinal injection of a recombinant adeno-associated virus vector expressing RPE65 (rAAV2-CB-hRPE65) in eight adults and four children with retinal degeneration caused by RPE65 mutations were reported. Now, results at 5 years after treatment in 11 of these subjects are reported. Subjects received a subretinal injection of rAAV2-CB-hRPE65 in the poorer-seeing eye, at either of two dose levels, and were followed for 5 years after treatment. The primary safety outcomes were ocular and non-ocular adverse events. Efficacy outcomes included changes in best corrected visual acuity, static perimetry hill of vision measurements for the central 30° (V 30), and total (V TOT) visual field and kinetic perimetry visual field area. The only adverse events reported during years 3, 4, and 5 were minor intercurrent illnesses. Pediatric subjects had improvement in visual acuity and static perimetry in the treated eye, sometimes with a smaller improvement in the untreated eye, during the first 2 years of the study that persisted during years 3–5, with no consistent changes in kinetic perimetry during the study. Most adult subjects had no consistent changes in visual acuity or static perimetry during the study. Three adult subjects with markedly abnormal baseline kinetic visual field area had improvement in the treated eye during the first 1–2 years after treatment, but the absolute magnitude of the improvement was small and was not sustained at subsequent visits. There were no clinically significant adverse events. Visual acuity and static perimetry testing results suggest that treating patients at a younger age is associated with better visual function outcomes during 5 years after treatment.
Introduction
L
The safety and benefit of gene replacement using recombinant adeno-associated virus (AAV) vectors have been conducted in murine 9,10 and canine 10 –15 models of RPE65 deficiency and in human patients, in whom RPE65 gene replacement has successfully restored cone and rod sensitivity, improved visual fields, and in some cases improved visual acuity. 16 –25 A randomized, controlled Phase III trial of an AAV2-RPE65 vector (voretigene neparvovec) demonstrated significant improvement in the ability of treated patients to perform multi-luminance mobility testing. 26 These findings led to recent Food and Drug Administration (FDA) approval of the therapy for treatment of patients >1 year of age with biallelic RPE6-associated retinopathy and evidence of viable cells. 27
Previously, results at 2 years after gene therapy were reported in 12 patients with RPE65-deficient LCA and SECORD. 25 Here, results at 5 years after gene therapy in 11 of these patients are reported.
Methods
Study design
Details of the study design have been reported previously. 25 In brief, 12 subjects at least 6 years of age with biallelic RPE65 mutation-associated retinopathy, best corrected visual acuity (BCVA) not better than 20/60 and not worse than hand motion in both the treated and fellow eye, and visible photoreceptor (outer nuclear) layer on an optical coherence tomography scan in the region of the retina where study agent administration was planned were recruited into the study. After signed informed consent was obtained from all subjects (and a parent for children), each subject received a subretinal injection in one eye of an AAV-RPE65 vector produced according to Jacobson et al. 28 Ten subjects (subjects 201–210) were enrolled at Casey Eye Institute, and two (subjects 301 and 303) at the University of Massachusetts Medical Center. All subretinal injections were performed by a single surgeon (one at each site).
During the first 2 years of the study, subjects underwent assessments of visual function at 14 specified visits, as described previously.
25
During the subsequent 3-year, long-term follow-up (LTFU) period, subjects were scheduled for an annual visit, which could be performed at the original study site or by the subject's local ophthalmologist in consultation with study personnel (see Supplementary Data; Supplementary Data are available online at
Statistical methods
Details of data analysis methods have been reported previously. 25 In brief, BCVA results were reported as the ETDRS letter score and log of the minimum angle of resolution (logMAR). Each of the 12 subjects had two pretreatment visual acuity tests performed for each eye. The coefficient of repeatability was determined using the method of Bland and Altman 33 for all eyes and for 19 eyes after excluding five eyes that had an ETDRS letter score of 0. The repeatability coefficient was logMAR = 0.145, equivalent to seven ETDRS letters for all eyes, and logMAR = 0.164, equivalent to eight ETDRS letters for the 19 eyes that had an ETDRS letter score >0 on one or both pretreatment test.
Each of the 12 subjects had three pretreatment (baseline) kinetic and static perimetry tests performed for each eye. Kinetic perimetry results were reported as the total area in square degrees for each target size (V4e, III4e, II4e, and I4e), and the mean of the total area with each target was determined for the three pretreatment tests and compared to the result at each subsequent visit and to values in 15 normal subjects. 25
Static perimetry data were analyzed using the Visual Field Modeling and Analysis method, 34 and results were reported as the total volume of the entire hill of vision (V TOT) and the central 30° portion of the hill of vision (V 30). The limits of agreement among baseline V 30 and V TOT tests for all subjects were calculated pairwise between each of the pretreatment tests, incorporating data for both eyes for all subjects. For each subject, the difference between the average pretreatment value and each post-treatment value for that subject was determined and compared to the upper and lower limit of agreement as the criteria that would represent a statistically meaningful change for a subject. 35 Results for 6/72 baseline tests and 7/168 post-treatment tests that had a false-positive rate >25% were excluded from this analysis. The limit of agreement for all baseline retinal sensitivity results was −3.50 to +3.12 db-sr for V 30 and −9.73 to +8.17 db-sr for V TOT. In 13 normal subjects, average values were 95.2 ± 9.0 db-sr for V TOT and 26.0 ± 1.4 db-sr for V 30. 25
Results
Twelve subjects aged 6–39 years with confirmed mutations in RPE65 were enrolled, two at the University of Massachusetts (subjects 301 and 303) and 10 at the Casey Eye Institute, between July 2009 and September 2012. Subjects 301, 303, and 201 to 204 received a lower dose of the vector (1.8 × 1011 vector genomes per eye) and subjects 205 to 210 received a higher dose of the vector (6 × 1011 vector genomes per eye). The 5-year follow-up visits were completed in September 2017. One subject (subject 201) was lost to follow-up after the year 2 study visit. Eleven subjects completed the LTFU questionnaire at years 3, 4, and 5 after study agent administration, but five of these had incomplete collection of other information during the LTFU period.
Safety information
During LTFU, there were no serious adverse events and no adverse events considered possibly related to the study agent or the procedures used to administer the study agent. The only adverse events reported were intercurrent illnesses (conjunctivitis and otitis in subject 205 and sinusitis and vertigo in subject 206).
One subject (subject 206) became pregnant approximately 4.5 years after study agent administration. She gave birth to a healthy baby boy in February 2017 (5 years and 3 months after study agent administration).
Ophthalmic examinations
All subjects had abnormalities on indirect ophthalmoscopy examination, characterized by a varying degree of retinal pigmentary changes, pallor of the optic disc, and attenuation of retinal vessels (Supplementary Tables S1 and S2; Supplementary Data are available online at
Visual acuity
Visual acuity results for six subjects who completed the LTFU visits and had baseline visual acuity in the treated eye of 25–62 ETDRS letters (logMAR 1.20–0.46) are provided in Fig. 1 and Table 1. The four pediatric subjects (subjects 202, 203, 204, and 210) had improvement in visual acuity in the treated eye during the first 2 years of the study that persisted during years 3–5. In two of these (subjects 202 and 210), visual acuity in the untreated eye also improved during years 3–5 compared to year 2.

Changes in visual acuity in six subjects with baseline acuity better than 20 Early Treatment of Diabetic Retinopathy Study (ETDRS) letters. Each subject's pretreatment visual acuity in the treated and untreated eye is in parentheses after the subject's study number. Blue diamond symbols are for treated eyes; red square symbols are for untreated eyes. Subjects 202, 203, 204, and 210 are pediatric subjects.
Average change from baseline visual acuity in subjects with baseline acuity better than 20 ETDRS letters
Values are average EDTRS letter score at baseline and average change from baseline for all visits during the period from month 2 to month 24 and month 2 to month 60.
EDTRS, Early Treatment of Diabetic Retinopathy Study; T, treated eye; U, untreated eye.
One adult subject (205) with baseline visual acuity of 31 ETDRS letters had little change in the untreated eye but had dispersion of subretinal pigment within the subretinal bleb during study agent administration 25 that was associated with persistent reduction in BCVA during the first 2 years, with little change in either eye over the next 3 years. Adult subject 208 with baseline visual acuity of 25 ETDRS letters had worsening of visual acuity in both eyes during the first 2 years that was more severe in the worse (treated) eye and then changed little over the next 3 years.
Five adult subjects with baseline visual acuity of count fingers (CF) or hand motion (HM) in the treated eye (subjects 301, 303, 206, 207, and 209) had little or no change in their visual acuity in the treated eye during the first 2 years of the study (Table 2). Four of them had progressive loss of visual acuity in one or both eyes during years 3–5. Subject 301 progressed from five letters to HM in the untreated eye, subject 303 progressed from 6.5 letters to CF in the untreated eye and 2.5 letters to HM in the treated eye, subject 206 progressed from CF to light perception (LP) in the treated eye, and subject 209 progressed from HM to LP in both eyes.
Visual acuity changes in five adult subjects with extremely poor baseline visual acuity
Values are ETDRS letter score, with a description of visual disability in parentheses if the letter score was 0. The pretreatment value is the average of the screening and baseline visits. The last visit at which visual acuity was tested was year 3 for subject 303, year 4 for subjects 301 and 207, and year 5 for subjects 206 and 209.
10/400 tested by Snellen chart.
CF, count fingers; HM, hand motion; LP, light perception.
Kinetic perimetry results
Kinetic perimetry results were available for 10 subjects during the LTFU period. The four pediatric subjects had normal or near normal kinetic fields with the V4e target at baseline (67–102% of normal in the treated eye and 64–107% of normal in the untreated eye). All four had no consistent change from baseline with the V4e target for either eye during 5 years after treatment (Supplementary Fig. S1 and Supplementary Table S3). Baseline values with the III4e and II4e targets were lower (13–83% of normal in the treated eye and 27–93% of normal in the untreated eye with the III4e target and 7–70% of normal in the treated eye and 10–49% of normal in the untreated eye with the II4e target). Three pediatric subjects had no consistent change in the visual field area in either eye with the III4e or II4e targets. One (subject 210) had a substantial and sustained increase in visual field area in the treated eye with the III4e target (from 13% of normal to ∼50% of normal) and II4e target (from 7% of normal to ∼50% of normal) at all time points from month 6 through year 5, with little change in the untreated eye (Supplementary Fig. S1). However, two of three baseline values with the III4e and II4e targets were much lower than the third baseline values (Supplementary Table S3), which may have exaggerated the magnitude of the increase after treatment.
One adult subject (subject 208) had normal kinetic fields with the V4e target at baseline (99% of normal in the treated eye and 95% of normal in the untreated eye). Baseline values were lower with the III4e target (77% of normal in the treated eye and 74% of normal in the untreated eye) and with the III4e target (58% of normal in the treated eye and 40% of normal in the untreated eye with the II4e target). This subject had inconsistent results during the follow-up period with the V4e, II4e, and II4e targets (Supplementary Fig. S2 and Supplementary Table S3).
Five other adult subjects had markedly abnormal kinetic perimetry results with a V4e target at baseline, ranging from 0.4% of normal in the treated eye for subject 206 to 9% of normal in the treated eye for subject 209. Only one of these (subject 205) had detectable visual fields with the III4e or II4e target (<1% of normal in each eye). Results with the V4e target during 5 years after study agent administration are shown in Table 3 and Supplementary Fig. S2. Subject 301 had an approximate doubling of visual field area in the treated eye during the first 2 years after treatment that was not sustained at year 4. Subject 303 had a decrease in visual field area in the untreated eye to <50% of the baseline value and a modest increase in visual field area in the treated eye during the first 2 years after treatment, but by year 3 the visual field area in the treated eye had also declined to <50% of the baseline value. Subject 206 had an increase in her visual field area in the treated eye during the first year after treatment that was not sustained at the year 2 visit. At the year 5 visit, she had no detectable response in the treated eye, and the visual field area in the untreated eye was decreased compared to the baseline value. Subject 205 had fluctuating results, but many values were less than baseline at all post-treatment time points. Subject 209 had a marked decrease in visual field area in the treated eye at all post-treatment time points, with no decrease in visual field area through year 3, but by year 4 the visual field area in the untreated eye had also decreased substantially. Subject 207 had an increase in visual field area in both eyes during the first 2 years after treatment and had no perimetry testing after the year 2 visit.
Changes in kinetic visual fields area after treatment in five subjects with markedly abnormal baseline values
Values are visual filed area (deg 2 ) tested with a V4e target at the indicated time points before and after treatment. Normal values are ∼14,000 ± 1,000. 25 Baseline values are mean (SD) of three values.
—, not tested or not reliable; SD, standard deviation.
Static perimetry results
Results for the eight subjects who had static perimetry obtained during LTFU are provided in Fig. 2 and Supplementary Table S4 for V TOT and in Fig. 3 and Supplementary Table S5 for V 30.
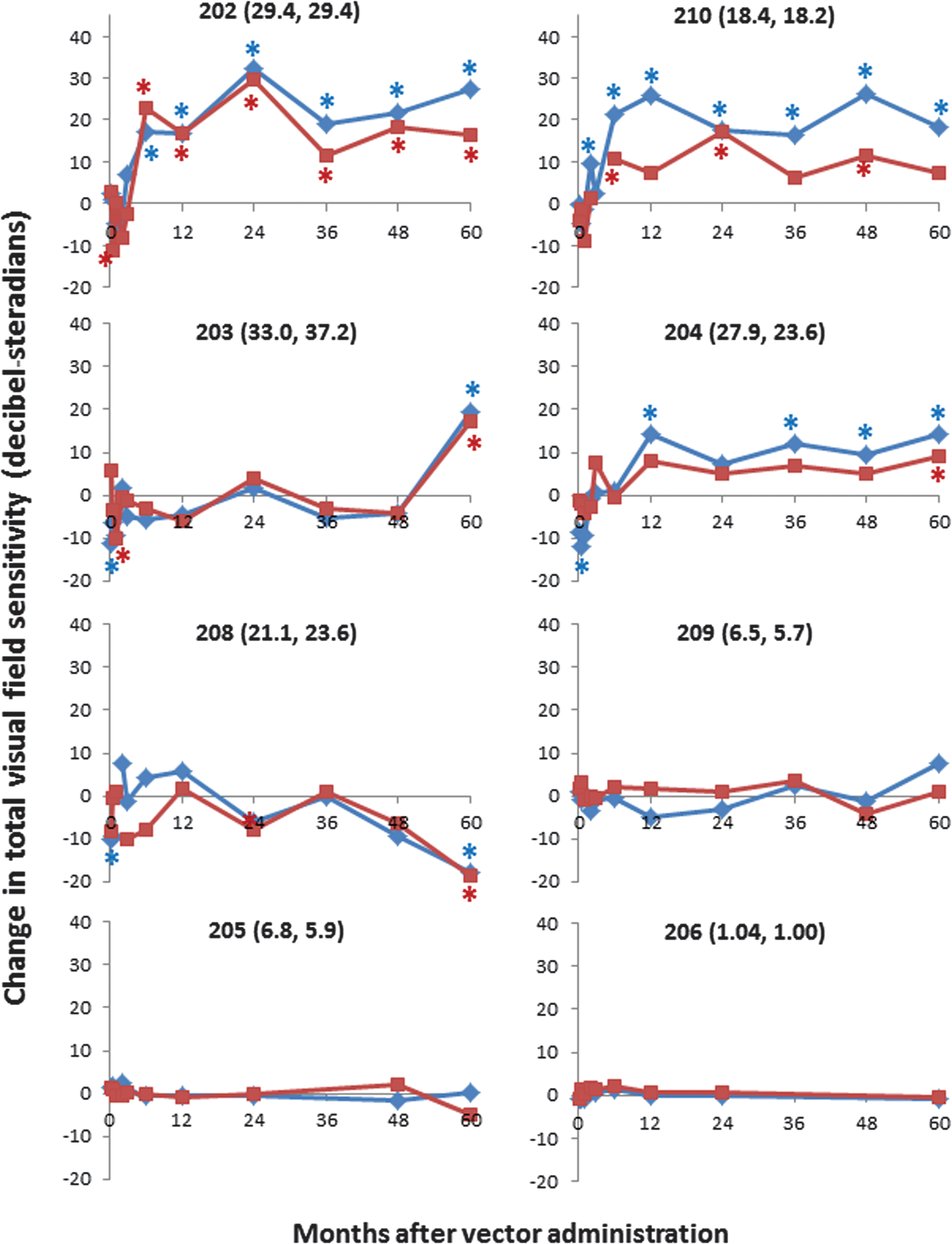
Total visual field hill of vision (V TOT) changes from baseline. The mean baseline V TOT values (decibel-steradians) in the treated and untreated eye are listed after each subject number. Asterisks indicate changes greater than the limit of agreement of pretreatment values for all subjects (−9.73 to +8.17 decibel-steradians). Subjects 202, 203, 204, and 210 are pediatric subjects.
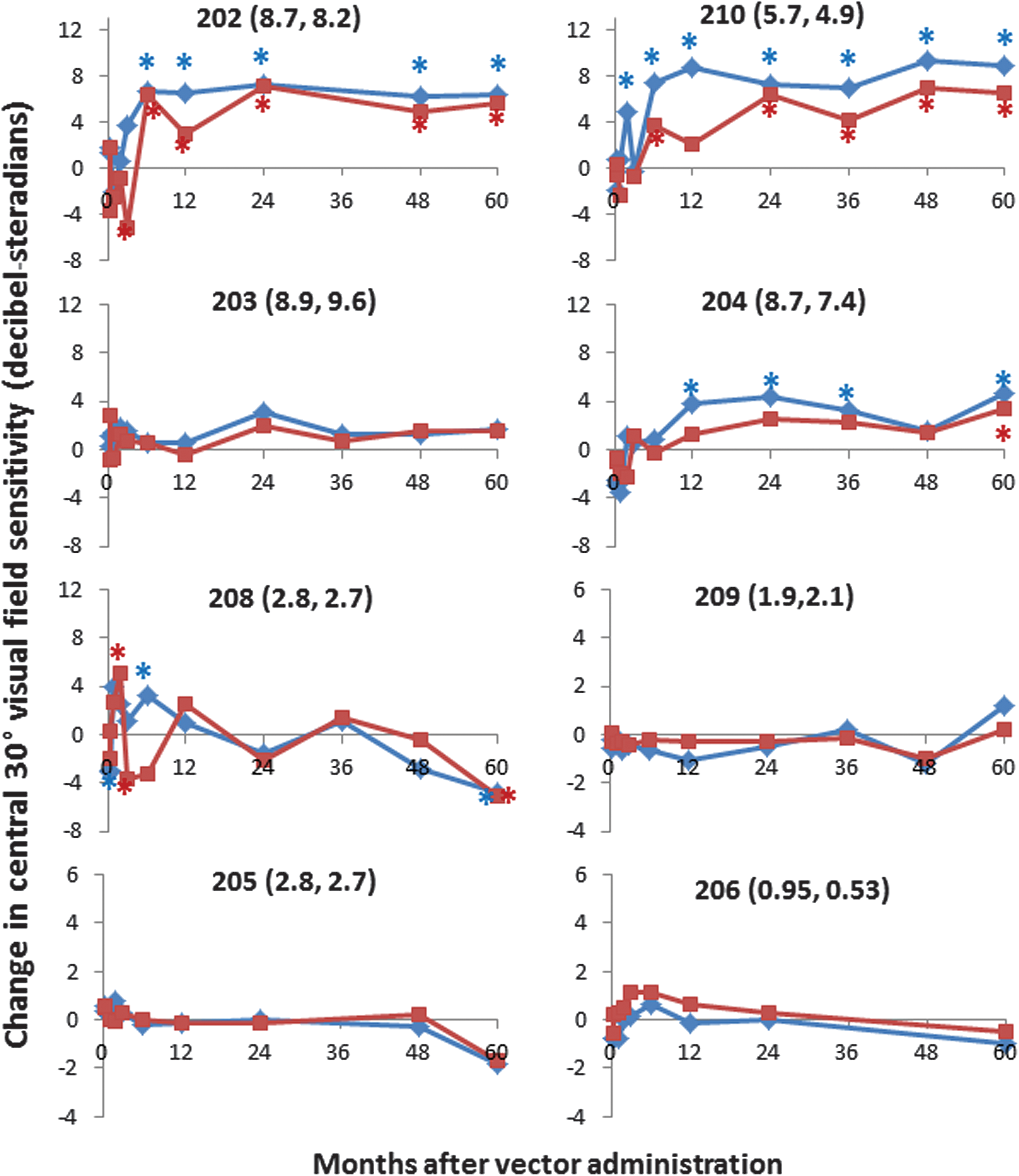
Central 30° visual field hill of vision (V 30) changes from baseline. The mean baseline V 30 values (decibel-steradians) in the treated and untreated eye are listed after each subject number. Asterisks indicate changes greater than the limit of agreement of pretreatment values for all subjects (−3.50 to +3.12 decibel-steradians). Subjects 202, 203, 204, and 210 are pediatric subjects.
The four pediatric subjects had a median baseline V TOT that was between 17% and 41% of normal and median baseline V 30 that was between 19% and 37% of normal. Three of these subjects (subjects 202, 204, and 210) had improvement in the total hill of vision in the treated eye at multiple visits during the first 2 years of the study that persisted during years 3, 4, and 5. The fourth pediatric subject (subject 203) had no significant changes during the first 4 years of the study but had an improvement in both the treated and untreated eye at the year 5 visit (Fig. 2).
Changes in V 30 paralleled the changes in V TOT. Three pediatric subjects (subjects 202, 204, and 210) had improvement in the total hill of vision in the treated eye at multiple visits during the first 2 years of the study that persisted during years 3–5. The fourth pediatric subject (subject 203) had small increases in V 30 that did not reach statistical significance (Fig. 3).
Among the four adult subjects with data obtained at LTFU visits, subject 208 had a median baseline V TOT that was approximately 22% of normal, with little change during the first 4 years of the study. However, there was a marked decrease in V TOT at year 5 to 3% of normal in the treated eye and 5% of normal in the untreated eye. Subjects 205 and 209 had more advanced disease, with a mean baseline V TOT that was approximately 6–7% of normal, and subject 206 had a mean baseline V TOT that was <2% of normal. Subject 209 had little change in V TOT during the study. Subject 205 had little change in V TOT during the first 4 years of the study, but at the year 4 visit there was a marked decrease in V TOT in the untreated eye to 1% of normal, with no change in the treated eye, and subject 206 had almost total loss of V TOT in both eyes at the year 5 visit (Fig. 2). Changes in V 30 paralleled the changes in V TOT (Fig. 3).
Discussion
Results from the first 2 years of this clinical trial showed that AAV2-mediated RPE65 gene replacement therapy was not associated with serious adverse events, and improvement in at least one measure of visual function was observed in 9/12 subjects, with the trend for improvement being clustered in the younger subjects. 25 Results from years 3, 4, and 5 identified no safety issues and continued to provide evidence that treatment at an early age may improve visual function and prevent progression of photoreceptor degeneration. Because of the large variation in baseline visual function and small number of subjects per group, it is not possible to draw meaningful conclusions about any potential dose-related differences in safety or efficacy.
Changes in visual acuity during LTFU were markedly influenced by the age and baseline status of subjects. Five adults with extremely poor baseline visual acuity had little or no change in visual acuity during the first 2 years after treatment, and four of the five had progressive loss of vision in one or both eyes during years 3–5. In two adults who had baseline visual acuity in the treated eye of 25 or 31 ETDRS letters, visual acuity was lower than baseline in the treated eye at year 2, with little change in either eye during years 3–5. In contrast, pediatric subjects had improvement in visual acuity in the treated eye, and a smaller improvement in the untreated eye, during the first 2 years of the study that persisted during years 3–5.
Changes in visual fields measured by static perimetry were also influenced by the age and baseline status of subjects. Three of four pediatric subjects had statistically significant improvement in V TOT and V 30 in the treated eye at most time points from year 1 to year 5 after treatment, and the fourth pediatric subject had improvement in V TOT in the treated eye only at the year 5 visit and small improvement in V 30 at most time points that did not reach statistical significance. At several visits, there was also a statistically significant improvement in V TOT and V 30 in the untreated eye in these younger subjects. As hypothesized previously, this could be related to a dampening in nystagmus after treatment of the eye with worse visual function, which would be expected to produce an increase in foveal fixation time and a concomitant increase in viewing stability at the locations of visual field testing in each eye. 25 This might also contribute to the improvement in visual acuity in the untreated eye during years 3–5 compared to year 2 in subjects 202 and 210. One adult subject had little change in V TOT or V 30 in either eye after treatment, but three adult subjects had marked worsening of static perimetry in both eyes during the study.
Improvements in BCVA and static perimetry in some subjects in this study are similar to short-term results from other studies. In a Phase I study evaluating subretinal administration of an AAV-RPE65 vector, Maguire et al. reported an eight or more ETDRS letter increase in BCVA in 8/12 subjects and a more than eight letter decrease in 2/12 subjects at 1 year after vector administration. 22 Five subjects followed for 3 years after treatment showed persistent improvement in BCVA in both the treated and untreated eyes and stable improvement in visual field area by kinetic perimetry testing. 36 In a Phase III study using the same vector, Russel et al. reported an average increase of eight or nine ETDRS letters in the treated eye versus an average increase of 1.6 letters in the untreated eye at 1 year after vector administration. 26 In a Phase I study of the same vector used in our study, Jacobson et al. reported an average increase of six EDTRS letters in the treated eye and 2.5 letters in the untreated eye, and improvement in retinal sensitivity detected by static perimetry testing in the treated area in 11/12 subjects. 37 The improvements in retinal sensitivity persisted at follow-up 3 years after treatment, 38 but three subjects followed for 4.5–5.5 years had a decline in the magnitude of the improvement in retinal sensitivity. 39
The results contrast with the results of Bainbridge et al. 24 who reported transient improvement in static perimetry in 6/12 subjects aged 6–19 years during the first year after treatment, with a return to baseline at the year 2 or year 3 visit. Differences in the potency for RPE65 expression in the two vectors may have contributed to the more sustained efficacy that was observed in pediatric subjects in the present study, and the Bainbridge group are developing an improved vector by codon optimization of RPE65 sequence and optimizing the promoter sequence. 40
Changes in visual fields measured by kinetic perimetry were more difficult to interpret. The four pediatric subjects had normal or near-normal visual field areas with the V4e target in both the treated and untreated eye at all time points, and one of these had improvement in the visual field area with the III4e and II4e targets in the treated eye but not the untreated eye. Three adult subjects with markedly abnormal baseline visual field area with the V4e target had improvement in the treated eye during the first 1–2 years after treatment, but the absolute magnitude of the improvement was small and was not sustained at subsequent visits, indicating that the efficacy benefit in these subjects was lost over time. One other adult (subject 209) had progressive loss of visual field area with the V4e target in both eyes that appeared earlier in the treated eye, and one (subject 205) had some loss of visual field area in both eyes during LTFU, indicating disease progression in these subjects. One (subject 208) had inconsistent results of testing, which is not uncommon in patients with advanced retinal degeneration.
Most Phase I/II clinical trials of inherited retinal diseases treat only one eye and use the fellow eye as an untreated control. However, because the eye with worse baseline function is generally the treated eye, caution must be exercised in interpreting results. Improvement in the treated eye but not the untreated eye suggests a treatment benefit, but if the outcome for the treated eye is worse than the untreated eye, this could be due to either toxicity from the study agent or the procedure used to administer the study agent, or could be the result of faster disease progression in the eye that had more advanced disease at the time of treatment. Phase I/II studies are also limited by the small number of patients who are treated and the lack of an untreated control group.
In summary, during LTFU evaluations there were no clinically significant adverse events detected and no clinically important new findings detected on ophthalmic examinations in subjects treated in one eye with a rAAV2-RPE65 gene therapy product. Visual acuity and static perimetry testing results suggest that treating patients at a younger age is associated with better visual function outcomes during 5 years after treatment. Outcomes beyond 5 years have not been determined.
Footnotes
Acknowledgments
This study was registered at
Author Disclosure
J.D.C. is an employee and shareholder of AGTC and has a conflict of interest to the extent that this work potentially increases his financial interests. K.N.B. is an employee of AGTC. OHSU in the name of R.G.W. holds U.S. patent no. 8657446, method and apparatus for visual field monitoring, also known as Visual Field Modeling and Analysis or VFMA, which was used for the volumetric assessment of the static perimetry. The other authors declare no conflicts of interest.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.