
Abstract
DNA vaccines can elicit both humoral and cellular immune responses in mice. However, their poor immunogenicity is a major obstacle toward clinical applications. Improving the efficiency of delivery of DNA vaccines has become a key issue. Vaccination via microneedles penetrating the epidermis can dramatically enhance the stimulation of immune responses. This study showed that by using microneedles to deliver DNA vaccines, gene expression and corresponding immune responses were greatly improved compared to conventional needle injection. The quantitative analysis of gene expressions was made at 6, 24, 72, and 144 h after the DNA delivery. DNA expression levels increased in a time-dependent manner and were substantially greater than with syringe injection after 6 h and 24 h. This elevated expression was followed by markedly enhanced immune responses, with 6–10 times higher levels of antibody and T-cell responses.
Introduction
DNA
Recently, another vaccine delivery technology, transcutaneous immunization (TCI), has emerged in the field as an alternative. TCI takes advantage of a noninvasive microneedle technique in which immunologically active skin is used as the route of delivery. It has already been demonstrated that TCI is a promising alternative DNA vaccine delivery technology that enhances vaccination efficacy. 12 Furthermore, microneedle vaccination may be administered by less-trained personnel, or even by patients themselves. 13 It has additional advantages, including inexpensive manufacturing, thermo-stability, and small physical size for logistics and storage. 14 The enhanced immune response is believed to be due to resident antigen-presenting cells (APCs) under the skin, such as Langerhans and dermal dendritic cells. 15 Although the delivery of DNA vaccines by TCI has been well documented, the mechanisms underlying the improved immunogenicity remain to be further investigated.
Given the advantages of microneedles, it was hypothesized that delivery of a DNA vaccine into the skin by microneedles would improve immune response by enhancing protein expression of encoded gene. This hypothesis was tested by investigating the expression and immunogenicity of antigen when delivered into the skin as DNA either by microneedles or by syringe. This study provides solid evidence that delivery of DNA vaccines into the skin via microneedles can be superior to conventional syringe injection in respect of both antigen expression and immunogenicity.
Materials and Methods
Animal, cell line, and reagents
Female C57BL/6 mice (6–8 weeks of age) were purchased from Beijing Vital Laboratory Animal Technology Company Ltd. (Beijing, China) and kept in specific-pathogen-free conditions. All animal experiments were approved by the Experimental Animals Committee of SHMC. HEK 293T cells were purchased from ATCC (Manassas, VA). Lipofectamine™ 2000 was purchased from Invitrogen (Carlsbad, CA). OVA protein was from Sigma–Aldrich (St. Louis, MO). pVAX1-OVA was constructed and preserved in this laboratory. All antibodies for cell subset identification and cytokine detection were purchased from eBioscience, Inc. (San Diego, CA) and BioLegend (San Diego, CA).
Plasmid preparation
Plasmids pEGFP-N3 (Clontech, Mountain View, CA) and pVAX1-OVA were prepared as midi-preps from DH5a cultures, purified by EndoFree Plasmid Maxi Kit (Qiagen, Hilden, Germany), and endotoxin was <30 EU/mg by limulus amebocyte lysate test.
Characterization of the microneedles
The microneedle holder and microneedle arrays were purchased from Suzhou NaTong Biological Nano Technology (Suzhou, China). The array of microneedles was observed by 1.0 kV scanning electron microscopy and showed a square of 2.6 mm × 2.6 mm, with each array containing 36 needles (6 × 6).
Injection of DNA vaccine
One microliter of plasmid DNA (8 mg/mL) was dropped onto the microneedles and spread evenly. The loaded array was then applied against the surface of a shaved mouse ear pinna or dorsal skin, with the holder set for 30 s vibration. After 24 h, quantitative analysis of subsequent protein expression in the vaccinated site was performed by placing an ear on the platform of a confocal microscope (Leica TCS SP5) or in dorsal skin by in vivo imaging (IVIS Lumina K). Controls received phosphate-buffered saline (PBS) in parallel. Syringe injections were delivered using a standard intradermal tuberculin syringe and needle.
Measurement of humoral immune responses by immunoglobulin G titration
Enzyme-linked immunosorbent assay (ELISA) was used to measure the antigen-specific antibody production induced by the DNA vaccine, as previously described. 16 Briefly, 96-well plates were coated with 2 μg/mL of OVA (in 50 mM of carbonate-bicarbonate buffer, pH 9.6) at 4°C overnight and blocked with 5% bovine serum albumin in PBST (0.05% Tween 20 in PBS) at 37°C for 1 h. The plates were incubated with diluted serum from different immunization groups for 1 h at 37°C. Antibodies were detected with horseradish peroxidase (HRP)-conjugated goat anti-mouse immunoglobulin G (IgG; Southern Biotech, Birmingham, AL). After the enzymatic reaction was developed, the OD values were read at 450/620 nm with an ELISA plate reader (Bio-Rad, Hercules, CA).
Measurement of delayed-type hypersensitivity
OVA-encoded plasmid DNA was delivered by microneedle or syringe into C57BL/6 mice (100 μg/mouse) four times in a 2-week interval. Delayed-type hypersensitivity (DTH) to DNA vaccine was determined by re-challenging with OVA protein on a footpad (10 μg/injection) and measuring the net increase in footpad thickness (swelling) at 48 h.
Assessment of T-cell responses by multicolor flow cytometry
A multicolor antibody panel was set up comprising anti-CD8, anti-interferon (IFN)-γ, and anti-tumor necrosis factor (TNF)-α. Splenocytes were re-stimulated in vitro by OVA for 24 h, and then blocked with monensin for a further 6 h. Splenocytes were stained with surface CD markers at 4°C for 20 min. After surface staining, intracellular staining was carried out after 4% paraformaldehyde/PBS fixation and 0.2% Triton X-100 permeabilization. Data were collected with a BD LSR Fortessa flow cytometer (BD Biosciences, Franklin Lakes, NJ) and analyzed by Flowjo (Tree Star, Ashland, OR) and GraphPad Prism (GraphPad Software, Inc., La Jolla, CA).
Statistics
Statistical analysis performed by using GraphPad Prism v6.0 (GraphPad Software, Inc., La Jolla, CA). An unpaired Student's t-test was used in one- or two-way data analyses. A p-value <0.05 was considered statistically significant.
Results
Characterization of the microneedles loaded with plasmid DNA
Inspection of the 6 × 6 array of microneedles by scanning electron microscopy revealed that each needle had a pyramid shape 220 μm high on a 180 × 180 μm square base (Fig. 1A). The microneedle holder/applicator is shown in Fig. 1B.

Characterization of the microneedle system used to deliver plasmid DNA.
To examine whether the microneedles penetrated the stratum corneum and delivered substances effectively, trypan blue was used as a delivery indicator. Two microliters of trypan blue was applied onto the microneedle array, which was then gently pressed against a mouse ear for 30 s with vibration turned on. As depicted in Fig. 1C, 36 dyed pinholes were observed in the treated ear. On the opposite ear, 8 μg of plasmid pEGFP-N3, encoding green fluorescent protein (GFP), was delivered in the same manner. Expression of GFP was examined by confocal microscopy 24 h later. As shown in Fig. 1D, the DNA plasmid was effectively delivered and resulted in efficient expression of GFP.
Microneedles facilitate DNA delivery
It was previously found that conventional syringe injection of DNA vaccine achieved poor antigen expression and stimulated a lower level of humoral response when compared to injection of protein. This study tested if microneedles could improve the protein expression that resulted from intradermal delivery of DNA vaccine. Plasmid DNA encoding GFP was applied at a dose of 8 μg by the microneedle array onto a mouse ear or dorsal skin, and the expression level of GFP was measured 24 h later by confocal microscopy or by an in vivo imaging system. Compared to the syringe injection, the microneedle delivery gave a 18.6-fold higher level of GFP expression in the ear by fluorescence microscopy (Fig. 2A and B) and more than fourfold higher in dorsal skin by the live imaging analysis (Fig. 2C and D).
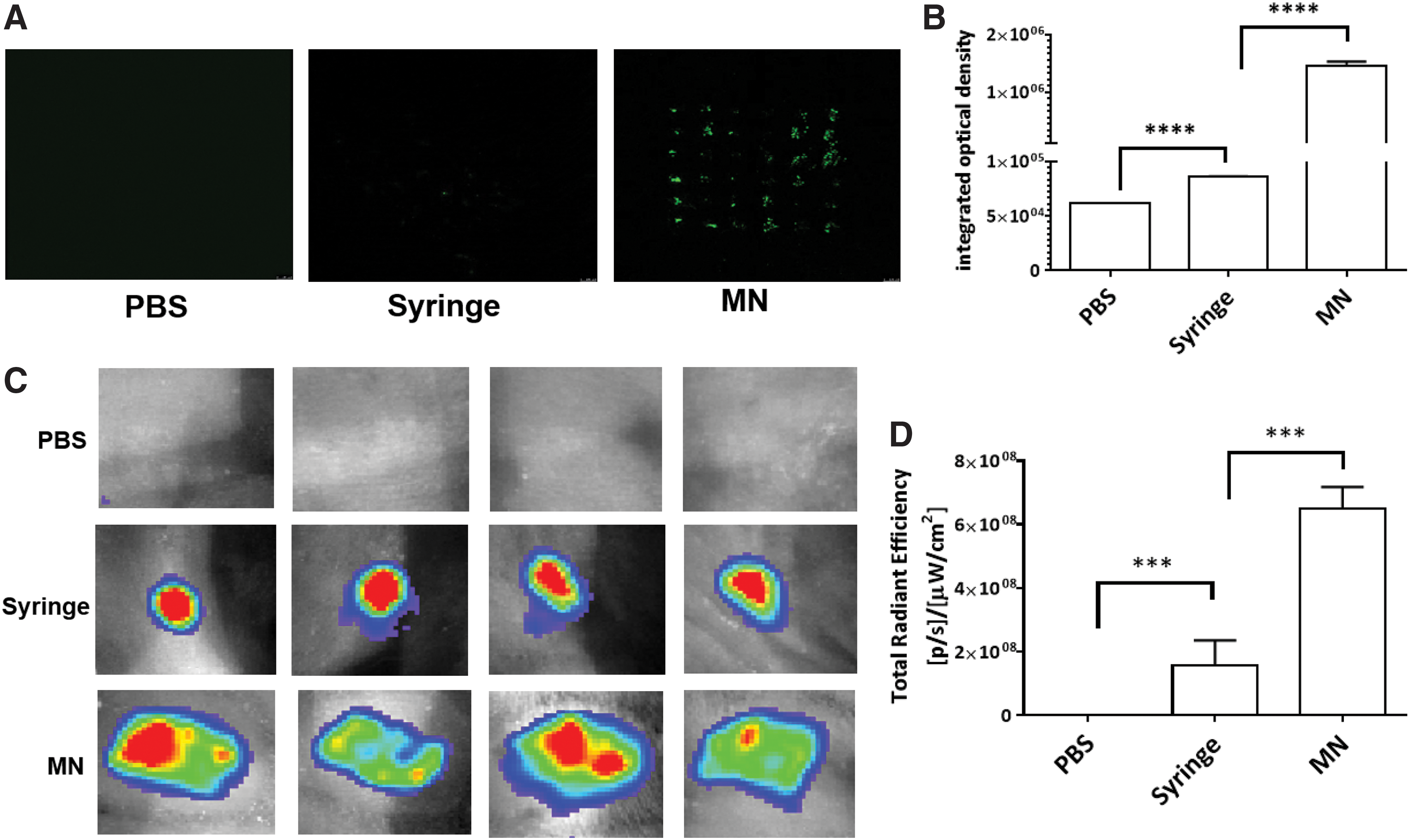
Microneedles improve protein expression from a DNA vaccine. GFP-encoding plasmid DNA (8 μg) was delivered by microneedle or syringe injection into the mouse ear or dorsal skin, and the tissues were inspected 24 h later. The expression of GFP in the ear was detected
Microneedle delivery and the duration of protein expression from the DNA vaccine
Protein expression was monitored and quantified at 6, 24, 72, and 144 hours by either confocal microscopy (ear skin; Fig. 3A) or in vivo imaging (dorsal skin; Fig. 3B). Expression was evident as early as 6 h after the microneedle injection, and up to 24 h, it was significantly higher than after delivery by syringe (Fig. 3B and D). A plateau was apparent between 24 and 72 h, and expression returned close to the baseline by 144 h. Detection of greater protein expression from microneedles even at 144 h by the more sensitive fluorescence microscopy method suggested that microneedles not only facilitated DNA delivery efficiency, but also may have prolonged the expression compared to the syringe injection. However, this difference was not statistically significant.

Duration of protein expression from DNA vaccination. GFP (8 μg) was delivered by microneedle or syringe into the mouse ear or dorsal skin and examined as described in Fig. 2. Expression was quantified at 6, 24, 72, and 144 h later.
Microneedle delivery facilitated host immune responses to DNA vaccination
To evaluate if the immune responses were enhanced by the microneedle modality of DNA vaccine delivery, mice were vaccinated with 60 μg of DNA vaccine encoding an OVA antigen four times biweekly by either microneedle delivery or syringe injection. The antigen-specific antibody titers, DTH, and CD8 T-cell responses were monitored.
Serum samples were collected 2 weeks after the final immunization and used to measure antigen-specific antibody responses by ELISA. Total antigen-specific IgG titers in mice that received the syringe injections were significantly lower than those in mice that received microneedle delivery (Fig. 4A). IgG1 subtype responses were at similar levels after microneedle and syringe administrations (Fig. 4B). Levels of IgG2c antibody, an indicator of cell-mediated response, was 11-fold higher after microneedle than after syringe administration (Fig. 4C). The ratio of IgG2c/IgG1, which reflects T helper type 1 (Th1) versus Th2 biased immune response, was significantly higher in the group that received microneedle immunizations compared to the syringe-immunized group (Fig. 4D).

Microneedle delivery enhanced both humoral and cellular immune responses to a DNA vaccine. Naïve C57 mice were immunized four times at 2-week intervals with 60 μg of OVA DNA by microneedle (MN) or by intramuscular (IM) syringe injection to dorsal skin. Two weeks after the last immunization, anti-OVA immunoglobulin G (IgG) antibody titer
When cellular immune responses were measured as DTH, it was evident that the groups immunized via microneedles gave stronger DTH reactions than those given syringe administration (Fig. 4E). The levels of IFN-γ- or TNF-α-producing CD8 T-cell responses were significantly higher in the microneedle-immunized animals compared to the syringe-immunized group (Fig. 4F and G).
Discussion
Here, it is reported that administration of a DNA vaccine by a microneedle array can effectively enhance the expression of the encoded antigen and greatly improve immunogenicity. The level and duration of antigen expression were markedly higher and longer than obtained by the traditional syringe injection. Consequently, there were both enhanced antigen-specific antibody production, and significantly higher levels of antigen-specific DTH reaction and CD8 T-cell responses. The enhanced immune responses might be a result of a greater number of Langerhans cells being impacted through a larger area of skin disturbed by multiple microneedle penetrations. Uptake of the delivered DNA by more Langerhans cells would in turn result in more antigen being presented highly effectively to the host immune system to generate Th1 cellular immunity. This would be consistent with the higher level of expression of IFN-γ and TNF-α cytokine production that was observed. The authors concur with the view that fewer APCs were likely engaged in antigen presentation after syringe injection. 17
Higher immunogenicity of DNA vaccines has also been achieved by using in vivo electroporation and gene gun delivery. 18,19 However, these approaches require special equipment that may cause discomfort during vaccination. In recent years, researchers have sought alternative delivery methods. The TCI modality is proving particularly attractive due to its convenience to use and reduced pain for recipients. 9,13,15,20,21 Different formats of antigen, including influenza, human papillomavirus-like particles, and naked DNA delivered by microneedle, have been shown to elicit both humoral and cellular immune response. 22 –24
The target tissue and depth of delivery can have major effects on the efficiency of microneedle delivery where there is shallow dermis penetration. 25 Short microneedles suitable for mouse skin were used, and gene expression levels were compared via the routes of the ear and dorsal skin. It was observed that ear delivery by microneedle achieved higher levels of gene expression by either route when compared to the syringe injection. Others have reported that humoral and cytotoxic T cell–mediated immune responses after DNA vaccination via syringe injection into the ear pinnae were 10 times stronger than after intramuscular injection. 26,27 Such findings suggest that DNA uptake and expression by typical target cells, including keratinocytes, Langerhans' cells, and dermal dendritic cells (DCs) in the skin, may result in more efficient presentation of the antigen to the immune system than uptake by muscle cells. After expression or uptake of the antigen, DCs can mature and migrate to local lymph nodes where antigens are presented to B and T cells and result in the initiation of a variety of immunological responses. In the present comparison, the best humoral immune response was obtained in the microneedle administration group at about 10 times higher titer for IgG2c than that in the syringe-injected group. Similarly, the DTH and cellular immune responses were about sixfold higher by the microneedles than the syringe injection.
The quantity of DNA delivered into skin cells by microneedles has not been accurately assessed, but about 25% of the DNA was lost while loading onto the microneedles (unpublished data). Any improvement of loading onto microneedles will further enhance this modality. Additionally, the use of materials such as dissolvable polymer to encapsulate the DNA vaccine on the array of microneedles should make it even more effective.
This study has demonstrated the successful cutaneous delivery of DNA vaccines via microneedles that resulted in robust antigen expression and duration. The antigen expression was much greater than that achieved by comparable syringe injection and induced much higher antigen-specific immune responses. This study has thus indicated that microneedles may provide an important advance in DNA vaccinology, not least because the strong cellular immunity that was elicited points toward application in novel therapeutic vaccination strategies against cancer and chronic infectious disease.
Footnotes
Acknowledgments
We are grateful to Ms. Shuhui Sun from the Flow cytometry facility of Fudan University for kindly providing helpful support and to Mr. Zhonghuai He from Advaccine (SuZhou) Biopharmaceuticals Co. Ltd. for fermentation and purification of plasmids. We also thank Ms. Xiaoyu Zhou and Ms. Yue He for their experimental technique support. This work was supported by grants from the National Key Research and Development Program of China (2017YFD0502301-2) to Dr. Gan Zhao and in part by support from the Natural Science Foundation of China (81672016) to Dr. Bin Wang.
Author Disclosure
The authors declare no conflicts of interest.