
Abstract
Hematopoietic stem cell transplantation has been studied for several decades now, mostly as a treatment for malignancies and hematological diseases but also for genetic metabolic disorders. Since many diseases that could be potentially treated with this approach develop early in life, studies of cell transplantation in newborn mice are needed, especially for gene therapy protocols. However, the small size of pups restricts the possibilities for routes of administration, and those available are normally technically challenging. Our goal was to test different routes of administration of Lin− cells in 2-day-old mice: intraperitoneal, intravenous through temporal vein (TV), and intravenous through retro-orbital (RO) sinus. Routes were evaluated by their easiness of execution and their influence in the biodistribution of cells in the short (48 h) and medium (30 days) term. In either 48 h or 30 days, all three routes presented similar results, with cells going mostly to bone marrow, liver, and spleen in roughly the same number. RO injection resulted in quick distribution of cells to the brain, suggesting better performance than the others. Rate of failure was higher for the TV route, which was also the hardest to execute, whereas the other two were considered easier. In conclusion, TV was the hardest to perform and all routes seemed to demonstrate similar results for cell biodistribution. In particular, the RO injection results in quicker biodistribution of cells to the brain, which is particularly important in the study of genetic metabolic disorders with a neurological component.
Introduction
Hematopoietic stem cell transplantation (HSCT) has been very effective for several hematological and metabolic conditions, including those with neurological impairment. Owing to the capacity of cells to migrate throughout the body and, under certain conditions, to reach the central nervous system (CNS) and differentiate into microglia, HSCT is being extensively studied for inherited metabolic diseases. 1 In these conditions, early intervention is primal for good outcomes as disease progression can only be prevented, but not reverted by treatment. 2 Minding this issue, preclinical studies aiming at transplantation in the early stages of life have been increasing, mainly using mouse models of diseases.
One of the main limitations of mouse models of transplantation is the animal size, especially if the procedure has to be performed in the newborn period. Mice pups have ∼3.5 cm and weight ∼2 g on day 2 postnatal. This is a major issue when intravenous administrations have to be performed, as the volume of injection is limited, and the vessels caliber is very tiny. Considering all difficulties for administering cells in newborn mice, the literature is very heterogeneous about routes of administration.
Intraperitoneal (IP) route is widely used to inject pharmacological drugs and viral vectors for gene therapy, 3,4 though it is also frequently used to inject mesenchymal stem/stromal cells (MSCs). 5 –7 The administration of cells in the peritoneum has results similar to intravenous administration, especially for cells with strong tropism for certain tissues or conditions—as MSCs that migrate to injured/inflamed tissues 6 —or cells that act by paracrine mechanisms. 7 This via tolerates well up 10–30 mL/kg body weight (although bigger volumes can be used in specific circumstances upon ethics committee approval). 8 IP injection is the easiest to perform but may cause significant animal distress if they are manually restrained. 9
For intravenous routes of administration, options for pups are different from those for adults. Although unpractical in newborns, the lateral tail vein is commonly used for intravenous access in adult mice. It is an effective systemic route, though some studies 10 –13 consider it relatively hard to access, requiring trained personnel to avoid multiple venepuncture attempts that may lead to animal discomfort and distress. If multiple administrations are required, scarring of the tail can occur, making the last injections even more difficult to perform. 12 Another option is the retro-orbital (RO) sinus—a venous complex situated in the retrobulbar space. Contrarily to the lateral tail vein, this route is accessible in newborn mice, even though the eyelids are shut in the first few days postnatal. 14 Comparison between these two routes normally favors the RO route, which is easier to perform and leads to equivalent results—although repeatedly being cited in the literature as aesthetically unpleasant to execute. 10 –13 In pups, however, there is another intravenous access: the lateral temporal vein (TV), a small vessel that is visible in both face sides in the first postnatal days. 15 It is widely used for all sorts of different treatments, 16 –18 although it seems to have more limitations—it is considerably harder to perform after 4 or 5 days postnatal as the skin thickens and pigmentation increases (especially in black strains), thus interfering in the visualization of the vessel. In addition, some techniques require two trained people. 19
Up to date, there are few studies comparing administration routes considering cell biodistribution, easiness of manipulation, and animal discomfort, 5,7,10,20 but none performed on newborn mice. Upon difficulties faced by our research group in assessing the best route for hematopoietic cell transplantation in newborn mice aiming at future studies, here we describe our experience with three routes—IP, intravenous through RO sinus, and intravenous through lateral TV. Our goal was to determine which route was the easiest to perform while allowing effective cell distribution.
Methods
Animals
This research project was approved by the ethics committee for the use of animals of Hospital de Clínicas de Porto Alegre under number #16-0260. C57BL6-GFP (herein referred as GFP) and 129/SV mice (herein referred as WT) were used as donors and recipients, respectively. The choice of a different strain (129/SV) was based on availability of mice in the animal facility. Animals from both genders were used. After weaning at 21 days of age, animals from the same litter were kept in appropriate cages with a maximum of five animals per cage in a controlled environment (temperature 20–24°C, 40–60% relative humidity, and air exhaust systems) with cycles of 12 hours of light and 12 hours of dark, standard commercial feed for the species, and water ad libitum.
Experimental design
Up to five animals per group were analyzed, as indicated in each figure legend. Recipient mice were assigned to three major groups according to the administration routes to be tested: IP, intravenous through RO sinus, and intravenous through lateral TV. Animals from the same litter were assorted randomly to each group and front paws were marked with subcutaneous injection of nontoxic ink for posterior identification. Since the goal was to provide an idea of cell distribution among various tissues (and not only hematopoietic organs), with special focus in the brain, and verify whether there would be a major difference between the routes tested rather than analyzing long-term engraftment, the endpoints chosen were 48 h and 30 days post-transplantation (Fig. 1A) (considered short term and medium term, respectively). 19 Other than in the brain, results are descriptive and are shown as the average and standard error of the mean from the three animals in each group. Another experiment following the same design was performed in mice without preconditioning with busulfan, and representative results from this experiment are shown in Supplementary Fig. S1. In addition, 10 animals were treated with busulfan only, without cell transplantation—3 mice were euthanized 48 h after busulfan injection for histological analysis of bone marrow (Supplementary Fig. S2) and 7 mice were kept for 30 days as controls for the conditioning treatment.

Experimental design and routes of administration.
Bone marrow collection and Lin− cells isolation
Hind legs were collected, and femurs and tibias were dissected from 6 to 8 week-old GFP+ mice. The bone marrow was flushed with Dulbecco's modified Eagle's medium containing 1% penicillin/streptomycin and 20% fetal bovine serum (all from Gibco), using a 27-gauge needle attached to a 3 mL syringe (BD). Flushed cells were homogenized by gentle up-and-down pipetting and filtered in a 70 μm Falcon cell strainer (Fisher Scientific) to remove cell clumps and bone particles. Cells were spun at 300 g for 5 min and then resuspended at a concentration of 1 × 106 cells/mL, plated in 6-well treated plates (Nest, China), and incubated in a humidified atmosphere at 37°C, 5% CO2, for 2 h, so that adherent cells (as macrophages and mesenchymal stromal cells) could attach to the plate. Upon completion of incubation, nonadherent cells were collected, pelleted, and resuspended in MACS buffer (Miltenyi Biotec, Germany). Lineage positive cells were depleted using MiniMACS Lineage Cell Depletion Kit (No. 130-090-858; Miltenyi Biotec, Germany), according to manufacturer's protocol. For each donor adult mouse, the yield of Lin− cells was approximately 5 × 105 (data not shown); therefore, for each pup, cells were collected from two donors, on average. Purity of lineage-depleted population was assessed by flow cytometry using antimouse Lineage Cocktail (BioLegend), which showed >90% of Lin− cells in each cell preparation (data not shown).
Busulfan conditioning
Newborn mice (∼24–48 h after birth, when weighting >1.5 g) were treated intraperitoneally with 20 mg/kg of busulfan (Busilvex, Patheon Manufacturing Services) in a maximum volume of 20 μL. This dose partially ablates the bone marrow, as determined by previous experiments from our research group (pilot study; data not published). The day chosen to initiate the treatment regimen was based on pup's size and weight (>1.5 g), as different litter sizes influence the pup's growth. After busulfan injection, pups were then placed back to the dam's cage.
Procedure for Lin− cells transplantation
Pups were transplanted 24 h after busulfan administration, ultimately varying from 2 to 3 days postnatal. Each pup received 1 × 106 Lin− cells suspended in 50 μL of saline solution 21 and cell suspension was kept on ice until the moment of injection. All procedures were performed in anesthetized mice, regardless of the route of administration. Newborns were removed from the dam's cage one by one and placed in a heated bench to induce vasodilation. Anesthesia was induced with isoflurane 3–4% (Isoforine; Cristalia, Brazil) vaporized in oxygen flow (300 mL/min) (Takaoka, Brazil). In the absence of motor reflex upon digital pinching, isoflurane concentration was reduced to 1–2% to maintain absence of reflexes. In the TV and RO groups, isoflurane flow was temporarily interrupted while performing the injection (up to 15 s). All injections were performed with a 6 mm 31-gauge needle (BD Ultrafine II, Brazil).
For intravenous injections through TV, animals were positioned in lateral decubitus, with thoracic members kept close to the thorax (Fig. 1C). The needle was inserted in the TV in the cranial–caudal direction. Elapsed injection time was ∼5 s. The injection was considered a success when no extravasation of solution was observed in the adjacent tissues and when the vessel recovered its dark color right after the end of the infusion (though before removing the needle). Hemostasis was achieved by light pressure with a cotton swab in the injection site upon needle removal.
For intravenous injections through RO sinus, pups were held in a vertical position, facing the executioner. Needle was inserted in the medial aspect of the shadow produced by the ocular globe (Fig. 1D), with the tip pointing to the orbit. The injections were considered successful when no extravasation of solution was observed in the adjacent tissues, no occurrence of ocular globe protrusion was observed, and nostrils were free of liquid.
For IP injections, we used the same procedure for injections in the peritoneal space for both cells and busulfan. Pups were placed in dorsal decubitus and the needle was introduced in the inferior right quadrant of the abdomen, in a 15° angle in an attempt to puncture skin and abdominal layers in different sites, thus reducing the reflux of liquid through the injection site upon needle's removal. In addition, mice were kept under anesthesia for 2 min after completion of injection for liquid settling. Liquid extravasation, including during the recovery of spontaneous movements, was considered as a failure of the procedure.
Animals were warmed and placed in oxygen flow after injection and only placed back to the dam's cage when spontaneous movements were fully recovered. In the few cases of failure of the procedure, mice were immediately euthanized by decapitation under deep anesthesia with isoflurane.
Euthanasia
Euthanasia was performed by isoflurane overdose and confirmed by cervical dislocation. In treated animals, blood was collected from heart puncture and stored at −20°C. Heart, liver, lungs, kidneys, spleen, cortex, and hind legs were also collected. For DNA extraction, one fraction of each tissue was frozen at −20°C, except for the bone marrow cells that were stored in phosphate-buffered saline solution collected by flush from the femur. For the immunohistochemistry (IHC) analysis, the remaining fraction of tissues and one hind leg were fixed in buffered formalin followed by paraffin processing according to routine techniques. The formalin fixed leg also went through 14% EDTA decalcification for 1 week immediately before being processed.
Immunohistochemistry
To evaluate the cell biodistribution and morphology, the IHC technique was performed using anti-GFP antibody to detect cells from the GFP+ donor. Collected organs were processed in paraffin blocks, cut in thin sections, and incubated for 1 h at 75°C. After dewaxing, antigen retrieval was performed by incubation with 10 mM citrate buffer pH 6 for 35 min at 94°C. Slides were incubated with primary anti-GFP antibody (1:600 dilution; rabbit polyclonal IgG from Santa Cruz Biotechnology) overnight at 4°C in a dark camera. Finally, slides were incubated with peroxidase-conjugated goat antirabbit IgG (1:200; Santa Cruz Biotechnology) secondary antibody for 90 min at room temperature on a dark camera and then developed through the DAB Kit (Dako) through chromogen 3-3′-diaminobenzidine (DAB). After IHC, slides were analyzed using ImageJ software, by means of the Color Deconvolution plugin, resulting in percentage of area occupied by GFP+ cells in the field, analyzing three fields of each organ. GFP+ tissues for positive controls and WT tissues and secondary antibody only for negative controls were run in all experiments.
Quantitative PCR
Genomic DNA was extracted from frozen tissues by the salting out method: small tissue fragments were homogenized with sterile pestles and incubated overnight in a bath shaker at 65°C, 350 rpm with 5 μL Proteinase K (10 mg/mL; Invitrogen) and 400 μL of digestion buffer (100 mM TRIS pH 8.3, 10 mM EDTA pH 7.5, 200 mM NaCl, 1% SDS). Upon complete dissolution of tissue, 100 μL of 5 M potassium acetate was added. Samples were spun 18,000 g at 4°C for 20 min, supernatant was collected, and 250 μL of ice-cold isopropanol was added. DNA was pelleted after 10 min centrifugation at 18,000 g and washed with 1 mL of ethanol 70%. Samples were resuspended in 49 μL of TE buffer and 1 μL of RNase A (ThermoFisher Scientific), incubated at 37°C for 1 h and quantified by Nanodrop (ThermoFisher Scientific). Purity ratios 260/280 and 260/230 were ∼1.8/2.0 for all samples.
Reactions in standard mode were carried out using PowerUp SybrGreen MasterMix (ThermoFisher Scientific), primers forward 5′ TGACGGGAACTACAAGACGC 3′ and reverse 5′ CCTCCTTGAAGTCGATGCCC 3′ (RefSeq NC_025025.1) at 0.2 μM each, with the following cycling conditions: 50°C 2 min; 95°C 2 min; 40 × 95°C 15 s, 55°C 15 s, 72°C 1 min; followed by dissociation curve in QuantStudio 3 and StepOne equipments (Applied Biosystems). Samples were run in triplicates, with 100 ng of DNA each.
In addition, amplification of the reference gene β-actin was conducted to control DNA input in brain samples. Primers used were forward 5′-CAAGATCATTGCTCCTCCTGAG-3′ and reverse 5′- GACTCATCGTACTCCTGCTTGC-3′.
For the absolute quantification, the 5.3 kb pIRES2-EGFP plasmid (Clontech) was used to create the standard curves, where a regression line was obtained plotting the logarithm of the number of copies versus the Ct. Correlation coefficients R 2 were >0.97 in all reactions. As positive and negative controls, samples from GFP+ and WT mice, respectively, were analyzed. No amplification was detected in WT samples neither in nontemplate controls, whereas amplification was positive in all GFP+ samples. Melting curves were obtained and confirmed the presence of single amplicons, and amplification efficiency was determined at every reaction, being ∼90% in all experiments. Absolute number of GFP molecules was calculated using the linear equation obtained from the standard curve. Each sample was analyzed in triplicates.
Results
Cell distribution
The presence of transplanted cells was assessed 48 h and 30 days after injection, both by IHC and quantitative PCR (qPCR) (Figs. 2 –5). qPCR was used as a quantitative method, whereas IHC was used mostly to evaluate the localization of cells within the tissue and their morphology, as the last is not as sensitive as the first. Since cells are supposed to engraft in the bone marrow, results are presented both using raw numbers (absolute number of GFP copies in qPCR or percentage of GFP+ area per field in IHC sections) or as relative numbers, considering the bone marrow at each time point as 100%.
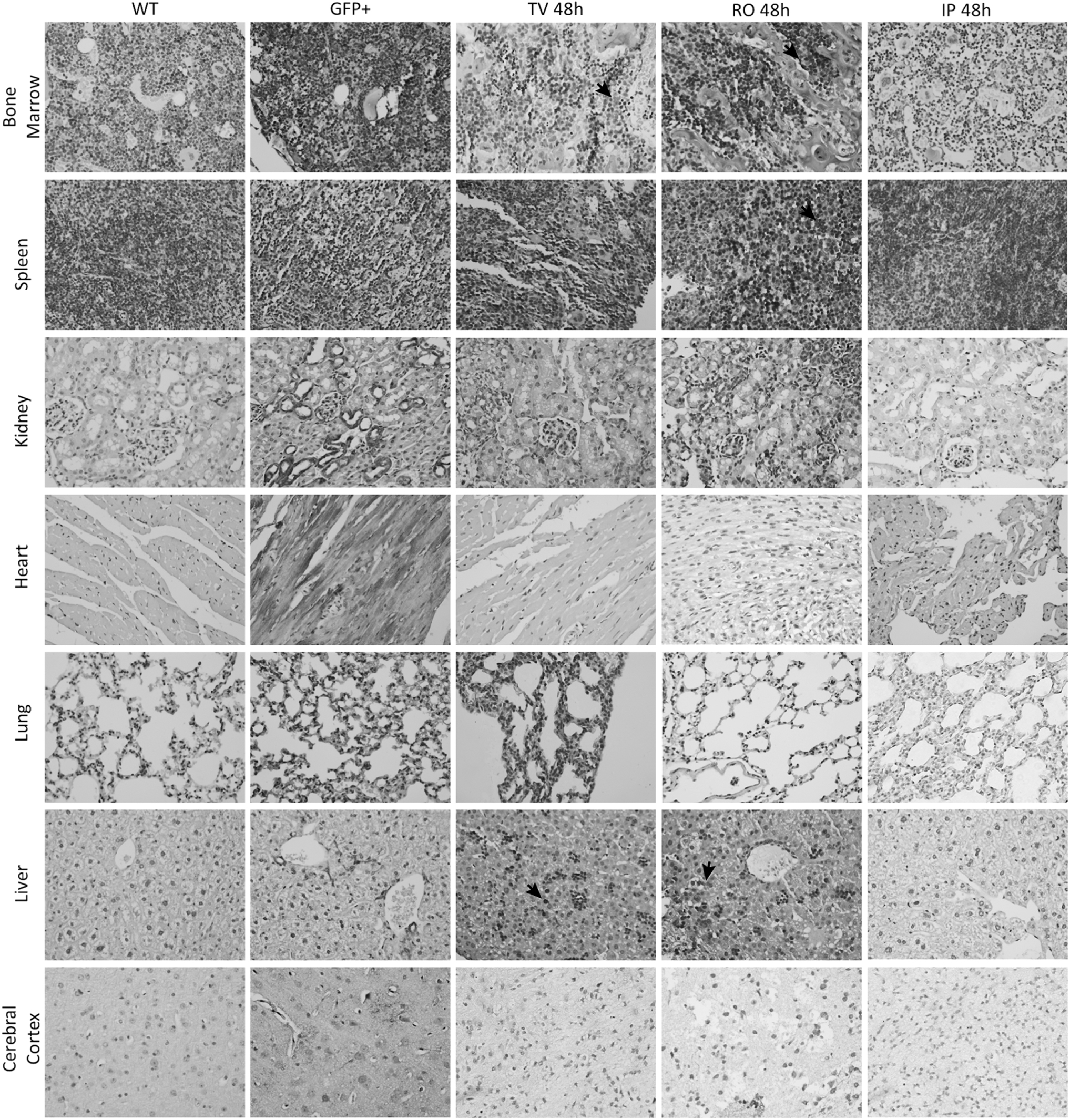
IHC for GFP+ cells in all organs analyzed at 48 h post-transplant of Lin− cells. Histological sections from positive and negative controls were obtained from adult mice. In 48 h, bone marrow, liver, lungs, and spleen were the tissues that presented more GFP+ cells in the TV route and in the RO route. Heart and kidney were almost negative, and few cells could be found in the brain of one mouse in the RO group. IP route had negative sections for all organs analyzed. Magnification 400 × . n = 3 per group. IHC, immunohistochemistry.

IHC for GFP+ cells in all organs analyzed at 30 days post-transplant of Lin− cells. Cells were found mainly in the hematopoietic organs bone marrow and spleen, but also in lungs, liver, heart, and kidney. In the brain, only the RO route presented few cells, with morphological characteristics of microglia cells. Representative GFP+ cells are pointed by black arrows. Arrows point to Kupfer cells in the liver, alveolar macrophages in lungs, and microglia-like cells in the brain. Negative and positive controls are the same as used in Figure 2. Magnification 400 × . N = 3 per group.

Quantitative results of GFP content in different tissues. Each color represents a different route of administration. Bars were plotted according to the left y-axis and represent the absolute number of GFP copies (qPCR: top plots) or GFP+ area (IHC: bottom plots); whereas symbols were plotted in the right y-axis and represent the percentage of GFP in the organ comparing with the bone marrow at each time point, assuming the latter is 100%. Standard error mean is shown above each bar. N = 3 per group in all organs but the brain, which is 5 per group. qPCR, quantitative PCR.
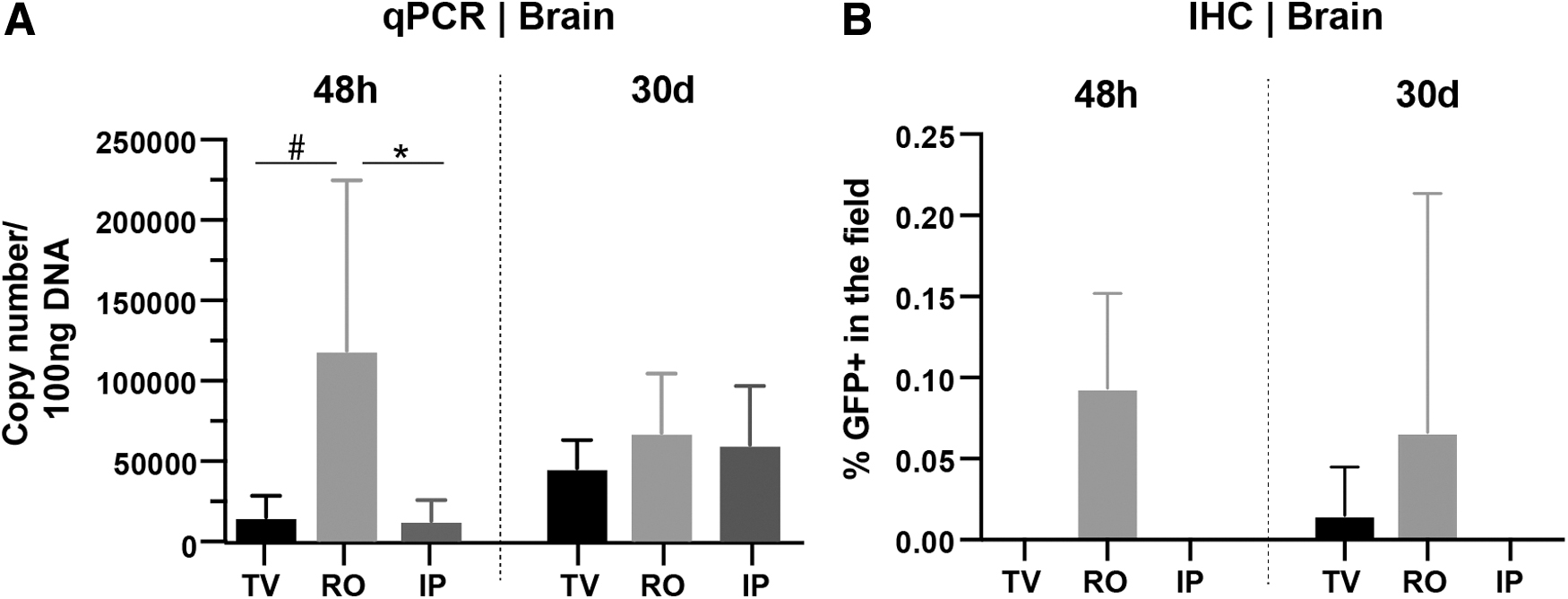
GFP quantification in brain.
At 48 h, in the IP group, GFP copies were seen mainly in the bone marrow, whereas in other tissues, the number of copies was very low (Fig. 4). By IHC, only the bone marrow presented positive cells (Fig. 2), reinforcing the result obtained by qPCR. This may suggest that cells migrate rapidly to the bone marrow when using the IP route. On the contrary, cells injected through the RO and TV routes were observed in tissues such as the spleen, lungs, and specially the liver, not only in the bone marrow (Fig. 2).
As expected, after 30 days, qPCR results showed that most cells migrate to the bone marrow, followed by spleen and liver. All three routes performed similarly in the medium-term assays. More importantly, all organs presented increased number of GFP copies when compared with 48 h results, which could be an indication that the cells were able to proliferate in the recipient.
In summary, the organs that retain most transplanted Lin− cells in 48 h are the liver and the bone marrow. In 30 days, cells home to the bone marrow and seem to be proliferating there, as the GFP+ detection increased in both qPCR and IHC. Following bone marrow and liver, cells also migrate to spleen and lungs, where the proportion of cells compared with bone marrow decreases over time (except for IP, where it increases from almost null to 30% in the spleen). Heart, kidney, and blood present similar number of cells and the proportion is roughly kept throughout time. Although the number of cells in blood seemed to increase, the proportion reduced in all routes at 30 days, which was expected as cells probably homed to the hematopoietic organs.
Brain had undetectable GFP+ cells in IHC assay for most samples (except from one mouse each time point from RO and one from TV 30 days). In the mouse from RO 30 days, GFP+ cells had the aspect of glial cells, not macrophages nor monocytes (Fig. 3), which could suggest engraftment and differentiation of transplanted hematopoietic cells. In qPCR at 48 h, number of GFP copies was lower in TV and IP than in the RO route (p = 0.023 for IP and p = 0.085 for TV) (shown in Fig. 4 for comparison with other organs and detailed in Fig. 5). Accordingly, at 30 days, mice transplanted through RO also presented higher number of copies than the others. Surprisingly, all five mice transplanted IP had detectable levels of GFP, with mean number of copies even higher than the TV route, though statistical significance was not observed. Overall, this could suggest that the RO route addresses the brain quickly and more efficiently than the others, although the variability was high in all groups (Fig. 5).
Easiness of procedure
All transplantations were performed by two veterinarians and one nurse. All three professionals are very experienced with injections in adult mice (ranging from 5 to 15 years of experience), but none had expertise in handling newborn. All performed injections by the three routes and here we describe their impressions exclusively regarding the injection procedures.
The TV route is the hardest to perform, as the hand has to be perfectly steady, requiring more and continuous practice. If the volume of administration is high (in case of hydrodynamic injections, e.g.), the difficulty increases as the syringe's piston is farther and another person is required to push it. In contrast, it is the only route that the executioner is completely sure of success, as it is possible to observe the administered solution inside the vessel and the recovery of blood flow when the injection procedure is over.
The RO route does not require as much training as the TV route. However, the executioner must estimate the needle's deepness and the site of puncture, requiring anatomy knowledge. It is possible to assess the success of injection if there is no swelling in the applied region or presence of liquid in the nostrils, although it is not as perfectly visible as for TV route.
Finally, the IP route is by far the easiest and does not require prolonged training. The needle has to be very thin, 30-gauge or more, otherwise the liquid will flow back through the puncture site and the pup has to be anesthetized during and after the injection to avoid reflux caused by their movement. In neonates, the skin is considerably translucent, and it is possible to visualize when viscera are pushed by the injected liquid without evident lesions. Therefore, veterinarians considered this route as easier to determine the success of the procedure compared with RO route, but not as well as TV route in this parameter.
The mortality rate solely due to the injections was null, although the success of the procedure varied between groups. TV showed ∼a 20% failure, mostly due to liquid extravasation in the subcutaneous skin layer, whereas no adverse events or consequences were observed in successful TV injections. For RO, one case of edema occurred immediately after injection, considered as failure. For IP, failure (liquid reflux) occurred in 10% of injections. Adverse events after successful injections occurred for RO and IP only. From all 12 animals injected through the RO route, we had one case of abscess in the injected site (Supplementary Fig. S3A) and one case of corneal clouding. In the IP route, we had one case of microphthalmia and growth retardation (Supplementary Fig. S3B), possibly due to complications of the transplant (as graft rejection or acute graft-versus-host disease) rather than due to the injection. As myeloablation control, seven pups were injected with busulfan only and were accompanied for 30 days. Five of these fully recovered from the partial myeloablation whereas the other two died at 48 h and 20 days after busulfan injection.
Discussion
When planning a project that involves newborn treatment, one might not consider how challenging it could be to administer a treatment to a mouse pup. Without experience, our research group has failed many times when trying to perform the first intravenous injections in 2-day-old mice, and some of these times were particularly frustrating as the treatments were expensive and/or laborious. The literature does have several systemic administration routes described, such as TV, 15 jugular vein, 19 RO sinus, 14 and so on, but evaluation of distinct routes using hematopoietic cells in newborn mice was not performed before. Most studies about administration routes of hematopoietic cells only evaluate engraftment in hematopoietic organs, as bone marrow and spleen, while we were interested in seeing cell distribution as a whole, including the CNS, as this is an important target for several conditions that could be treated with HSCT. 1,2 Intrahepatic injection is, possibly, the most common route for transplantation of hematopoietic cells in newborn pups, especially human CD34+ in humanized mouse models. 22,23 However, there is evidence that cells transplanted in the liver do not reach the brain 24 —thus our interest for systemic routes.
The ability of hematopoietic stem cells to home and engraft can vary considerably depending on the source of the cells. In humans, it is well known that cells derived from umbilical cord blood, bone marrow, or mobilized peripheral blood engraft differently—umbilical cord blood cells have the highest risk of graft failure, followed by bone marrow and peripheral blood. 25 Besides the cell source, age-related differences in engraftment have also been described: for example, hematopoietic cells derived from young mice (up to 4 months old) can prevent aging-related processes, whereas cells from older donors cannot. 26,27 The transplant outcome also depends on the recipient—cells derived from adult mice engraft better in adults than in newborns. 28 In this study, we used 6–8 weeks old mice as cell donors for newborn recipients, which may have influenced the engraftment and distribution of cells, although this diminished activity of adult cells occurred to all experimental groups, making the observations still valid.
Both qPCR and IHC techniques were used as they complement each other. The absolute quantification method detects the presence of DNA, which is independent from GFP expression; whereas IHC provides the localization and morphology of GFP+ cells in the tissue, thus making it possible to observe whether there are donor-derived round-shaped monocytes, differentiated ramified microglia-like cells, or tissue macrophages, for example. IHC also excludes the possibility of positive cells detected by qPCR being located only in remnants of blood in tissue vessels.
IHC results were all based on percentage of GFP+ area in the field. They could not be compared with their correspondent GFP+ control tissues because the expression and intensity of GFP largely varies between different organs, possibly due to different promoter activation. 29 Even though tissues were cut symmetrically upon collection (half for each method) and multiple fields were analyzed per slide, IHC results are still not representative of the whole. This may explain why many tissues had absent GFP staining while presenting high number of GFP copies by qPCR. As results from both techniques showed high variability, we calculated the correlation between them (Supplementary Fig. S4). Correlation scores were R 2 > 0.4 for most tissues, which is an indication that there is some correlation. Nevertheless, IHC was very useful to analyze the morphology of transplanted cells in different tissues. Despite the rare possibility of differentiating in other cell types (including hepatocytes, 30 e.g.), the majority of Lin− cells resembled monocyte-derived cells, as Kupffer cells in the liver, alveolar macrophages in the lungs, and microglia-like cells in the brain (Figs. 2 and 3).
At first (based on 48 h results), Lin− transplanted cells go mainly to the liver when using RO and TV routes. This could be explained by high vascularization and/or because the liver is the primary source of hematopoietic cells during the embryonic development, with the last colony-forming progenitor cells migrating to the bone marrow in the first few days after birth. 31 Besides the liver, in 48 h, a good portion of cells home to the bone marrow, where they seem to engraft and proliferate, as they were also detected at 30 days in even higher numbers in all routes (as seen in both IHC and qPCR). It is important to highlight, however, that this configuration is not necessarily final, as the transplanted cells only achieve a steady state 8 weeks post-transplant, and the effect of reconstitution performed by long-term hematopoietic stem cells can only be analyzed after 16 weeks in vivo and after serial transplantations. 32 Furthermore, spleen showed the third biggest GFP content; other organs, such as heart, kidney, lungs, and brain had fewer cells and in comparable number (Fig. 6).
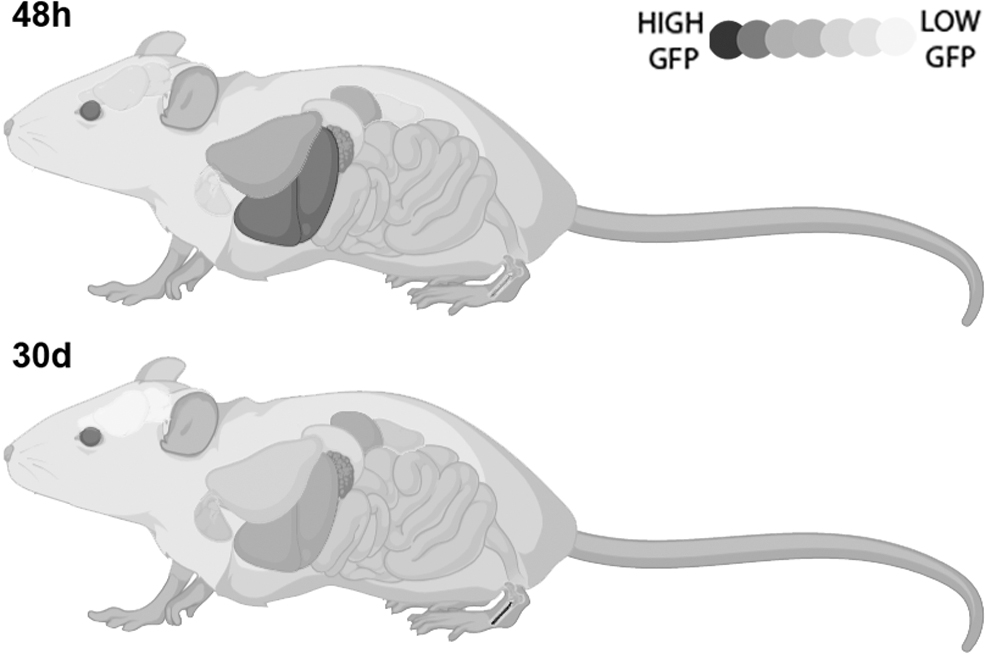
Distribution of Lin− cells in mouse. Summary of distribution of Lin−cells considering all three routes of administration and both qPCR and IHC techniques. In 48 h post-transplant, cells are mainly found in liver, but bone marrow, lungs, and spleen also have a moderate number of cells. Kidney, heart, and brain present very few cells. At 30 days post-transplant, however, cells home to the bone marrow, where they engraft and proliferate. Spleen and liver have significant number of cells, followed by kidney and heart. Very few cells migrate to the brain and presumably engraft there, being barely detectable.
At 30 days, cell distribution resembled that observed at 48 h, except that in the later point the bone marrow had much higher GFP+ copies. In all tissues analyzed, it is possible that cells are proliferating, as the absolute number of GFP copies and/or GFP staining increased in all 30 days groups when compared with 48 h groups, even though the content of GFP in some tissues may seem lower if compared proportionally with the content in the bone marrow. This ability to migrate to and/or proliferate in different organs together with the thorough distribution of cells in systemic administrations (as in the RO route that even seems to facilitate cell migration to the CNS, at least in one mouse) is extremely helpful when one thinks about long-term treatments.
Hematopoietic cells migration activity is increased to the CNS in cases of injury and neuropathology, 1 which was not the case and could explain why not many cells were seen in this tissue. Busulfan conditioning also is supposed to help cell engraftment in the CNS, 33,34 but it may not occur when partial myeloablation is achieved as compared with full myeloablation with lethal doses. It has been suggested that few transplanted cells migrate to the brain soon after conditioning, as the myeloablative regimen affects resident microglia cells and facilitates the influx of circulating myeloid cells to the brain. However, this is not correlated with the bone marrow engraftment and only few cells do engraft in the brain parenchyma, proliferating in the tissue if necessary, rather than recruiting more cells from circulation. 33 Nevertheless, we observed positive cells in the brains of few mice, two of them from the RO route. IHC from 48 h did not show well-defined cells, but qPCR presented 10-fold more copies than other individuals in other groups. Moreover, the mouse analyzed at 30 days presented several microglia-like cells in IHC assay, with multiple visible ramifications (Fig. 3). As targeting the brain was one of our main goals, we performed the analysis in five mice per group and included a DNA input control in the qPCR, by amplifying the reference gene β-actin in every run. In all samples analyzed, variations in β-actin amplification were <5% between samples, confirming that the robust variation observed in number of GFP copies is solely due to the treatment (Supplementary Fig. S5).
Although the small number of mice does not allow us to reach robust conclusions on this subject, better performance of the RO route over the TV route aiming at the CNS was already described by Gruntman et al., 21 when they compared both routes for adeno-associated viral vectors injection and observed higher transduction of brain and retina with the RO administration—although the authors discussed that the volume administered (50 μL) might be too much for this route, which could cause a hydrodynamic effect and increase efficiency. Surprisingly, the IP route performed similarly to the RO route at 30 days (Fig. 5), although this should be further investigated with larger sample size and longer time periods.
The mouse that developed microphthalmia and had growth retardation was transplanted through IP and was euthanized at 30 days (Supplementary Fig. S3B). This mouse had the highest content of GFP in all organs seen in both qPCR and IHC, compared with the others in the same group. These manifestations are characteristic of acute graft-versus-host disease, in which the transplanted immune cells proliferate indefinitely and attack the host's tissues. The acute response in mouse models typically arises at 14–28 days post-transplantation and usually deceases the mouse within few days. 35 Unfortunately, phenotypical analysis of immune cells was not performed to confirm this hypothesis.
If we consider the easiness of execution and the less distress caused to animals, the IP route would definitely be the unanimous choice. It had fewer failures and only one adverse event, although it was not related to the procedure itself but probably due to graft-versus-host disease. The possibility of local effects at the site of injection was not analyzed in our study, but if present, they do not seem to last long term. 36 Lin− cells were distributed in a similar manner in visceral organs in IP as other routes, with even better results in the brain than TV route. RO injections were also easy to perform but unpleasant; it was the route that seemed to yield higher GFP content in most organs and, more importantly, the route that reached the CNS the most in our sample. Lastly, the TV route was the hardest to master, with many failures and discarded animals throughout the study. As a bright side, this route seemed to have the most homogenous results among groups—possibly because it was easier to notice the failure of injections than it was in the others. Finally, the best route of administration of Lin− cells depends on the goal, personnel, and resources available.
Footnotes
Acknowledgments
The authors would like to thank Dr. Marina Siebert and Flavia Giusti for their assistance with qPCR and IHC experiments.
Author Disclosure
No competing financial interests exist.
Funding Information
Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq), grant number 141702/2017-6; Fundo de Incentivo à Pesquisa e Eventos do Hospital de Clínicas de Porto Alegre (FIPE-HCPA), grant number 16-0260.
Supplementary Material
Supplementary Figure S1
Supplementary Figure S2
Supplementary Figure S3
Supplementary Figure S4
Supplementary Figure S5
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.