
Abstract
Gene therapy and gene editing technologies are complex and it can be difficult for the public to understand their possible benefits or side effects. However, patient and public support is critical for the successful adoption of any new technology. Given the recent advances in gene therapy and gene editing, their potential clinical benefits, and the significant attention that has been given to the first-known successful attempt at permanent and heritable changes to the human genome, a systematic review was performed to assess beliefs and attitudes toward gene therapy and gene editing for human use, and to highlight the factors that influence acceptability. A systematic search following Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) guidelines was undertaken in April 2018 to identify articles examining opinions and attitudes regarding the acceptability of gene therapy and gene editing. Overall, 1,561 records were retrieved from 4 databases (Ovid Medline, PsycINFO, Scopus, and Web of Science). Duplicates were removed, and titles and abstracts independently screened, leaving 86 full-text articles assessed for eligibility. Following full-text review, 33 were included, with 5 articles added after forward/backward searching. An additional three articles were added following an updated search in March 2019 (total n = 41). Findings from the studies were integrated according to common themes: the impact of demographics; risks versus benefits of success; treatment specifics (e.g., medical vs. other reasons; disease severity and status; somatic vs. germ line; and mode of delivery); moral or ethical issues; and changes with time. In general, perceptions were positive, particularly for medical reasons and fatal diseases, but were also influenced by perceived risk. Somatic therapies had higher levels of acceptability than germ line therapies. While available in various forms, limitations exist in the measurement of perceptions of gene therapy and gene editing. Treatment acceptability is essential for future clinical trials, so it is important for scientists and clinicians to be clear about the risks and benefits of these technologies, and how these are communicated to the public, while encouraging education about genetic therapies to a broad range of individuals.
Introduction
Genetic diseases are conditions caused by one or more mutations in the genome, and are ideal targets for gene therapy or gene editing; treatments designed to correct the function of the abnormal gene. 1 Gene therapy achieves this by adding a correct copy of the gene into the genome of the cells in the target organ or tissue, while gene editing alters the genome at a specific location to correct or alter the genetic sequence. 2 The premise of both these therapeutic approaches is that the presence of the modified gene enables the expression of a correctly functioning protein, eliminating the cause of the disease and improving whole-organ function.
Gene therapy and gene editing are ideally suited to monogenic inherited disorders in which mutations in a single gene are responsible for causing disease. They are also typically targeted at rare diseases for which effective treatment options are not available, and for which premature death occurs (e.g., hemophilia and cystic fibrosis [CF]). Gene therapy typically uses a vehicle—termed a gene vector—to transfer a correct copy of the gene of interest into target cells. Viral and nonviral gene vectors have been developed over the last 30 years to treat a range of intractable diseases, including severe combined immunodeficiency (SCID), 3 hemophilia, 4 Wiskott–Aldrich syndrome, 5 metachromatic leukodystrophy, 6 spinal muscular atrophy, 7 and CF. 8,9 Recently, Luxturna (Spark Therapeutics) became the first Food and Drug Administration (FDA)-approved prescription gene therapy, treating Leber's congenital amaurosis (LCA), an inherited retinal disease caused by mutations in the RPE65 gene. Others such as Strimvelis (GlaxoSmithKline) for SCID and Glybera (UniQure) for hereditary lipoprotein lipase deficiency have been marketed, but have faced challenges due to cost. 10,11 While ex vivo gene editing approaches have been developed for diseases such as hemophilia 12,13 and immunodeficiencies, 14 few successful in vivo techniques have been reported, primarily due to challenges associated with the delivery of the gene-editing reagents to the target cells. 15
While gene therapy and gene editing offer real hope for lasting benefit or a cure for these diseases, the delivery process and the potential for permanent changes to the host cell genome do have potential or actual risks. A 1996 gene therapy clinical trial for X-linked SCID—a disease characterized by a lack of the IL-2 receptor that results in an impaired adaptive immune system—used a γ-retroviral vector to deliver the IL-2 receptor gene, and resulted in improved long-term immune reconstitution and correction of the primary immunodeficiency. However, 25% of patients developed T cell acute lymphoblastic leukemia, 16,17 an unexpected consequence of the vector inserting itself upstream of the proto-oncogene, LMO2, resulting in its expression. 17 Gene vector designs have improved in the last 15 to 20 years, and these adverse events are now better understood and deemed extremely unlikely. However, risks remain and there are still some uncertainties about the actual risk involved. For example, Hampel et al. noted that “both the chances and the risks of this technology are still relatively hypothetical.” 18 In contrast, risk in other areas of medicine such as organ transplantation and stem cell therapies has become more acceptable, 19 likely because the risks involved in those procedures are better understood. This suggests that the overall risk is a combination of actual and perceived risks.
There are also several ethical and philosophical issues related to gene therapy and gene editing. Both can be targeted to the somatic cells, any cell other than the reproductive cells, or to the germ line cells, the reproductive cells that pass their genetic material onto their progeny. Any risks and consequences arising from somatic cell gene transfer are restricted to that particular individual. Germ line gene transfer differs in that it permanently alters the sex cells of the organism. Germ line alterations would be passed onto future generations, and these therapies might therefore have a much wider impact than just the treated individual. 20 Many researchers consider germ line alterations to be an ethical line that should not be crossed. 21 While rare and intractable diseases are the main target of gene therapies, a future use might be functional enhancement. For example, in the future it may be possible to add or alter genes responsible for strength, endurance, speed, longevity, intelligence, hair or eye color, or other physical traits, for nontherapeutic benefit. However, the ethics of these modifications remains questionable. As such, the ethical and moral implications of genetic therapies are likely to influence people's perceptions toward gene therapy and gene editing.
Overall, gene therapy and gene editing technologies are complex processes and it can be difficult for the public to understand their mechanisms, possible benefits, and side effects without education and clear communication. 22 However, both patient and public support are critical for the successful adoption of a new technology. Since gene therapy can produce permanent genetic changes, carries some inherent risks, and would ultimately be delivered to children and young patients, it is important to comprehensively assess the acceptability of gene therapy and gene editing for human use. Understanding the perceptions that people broadly hold regarding the potential risks of gene therapy and gene editing for human use is critical to consider the future viability of these treatments. In addition, patients themselves are integral stakeholders to the uptake of emerging genetic medicines. Thus, an understanding of specific factors that might influence perceptions of these technologies (e.g., mode of delivery and how therapeutic efficacy is assessed) is also essential.
Researchers have previously reviewed attitudes to biotechnology, 23 gene therapy, 24 and gene editing, 25 however, given the recent and rapid advances in these fields, and their increasing potential to provide substantial clinical benefit, a comprehensive systematic review was deemed essential to assess the beliefs and attitudes toward gene therapy and gene editing for human use. The aim of this systematic review was to provide a broad understanding of the perceived acceptability of gene therapy and gene editing for human use and to highlight factors that influence acceptability.
Methods
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement was followed. 26 The research question, search strategy, and selection criteria were all predefined. Critical appraisal of the articles and methods for data analysis and synthesis are outlined below.
Search strategy
A systematic search was undertaken on April 17, 2018, and updated March 6, 2019, to identify articles that examined opinions and attitudes regarding the acceptability of gene therapy and gene editing. The focus was on examining perceptions of gene therapy within a broad population, with a specific focus on the “public,” and exploring views on gene therapy and gene editing, including perceptions, attitudes, and acceptability. A search strategy was developed in consultation with a Health Sciences Librarian to increase search sensitivity. The following search string was adapted across the four core databases: ((public OR lay OR popular* OR countr* OR communit* OR patient* OR carer* OR caregiver* OR “care giver”* OR personal OR parent*) NEAR/10 (attitude* OR accept* OR opinion* OR perception* OR view* OR belief*)) AND ((gene OR genes OR genetic* OR gene-based) NEAR/1 (addition OR edit* OR therap* OR treat* OR transfer* OR repair* OR replace* OR medicine*)). Databases used were Ovid Medline, PsycINFO, Scopus, and Web of Science.
Selection criteria
Studies were included if they were full-text, peer-reviewed articles that presented data on people's perceptions, attitudes, opinions, or views on the acceptability of gene therapy or gene editing for human use. Qualitative, quantitative, and mixed-methods studies that presented primary data were included to gain a greater understanding of the research in this area. Articles from broad samples (e.g., the general population, parents, students, or those in STEM-related jobs) as well as ones that examined gene therapy in health, medical, and cosmetic settings, were included. Studies were excluded if they were not peer-reviewed or available in English; if they did not measure perceptions, views, opinions, or attitudes regarding gene therapy for humans; or if they focused solely on stem cell therapy, genetic testing, sex selection, or genetic enhancement without gene therapy. Studies that examined perceptions or attitudes toward gene therapy solely for agricultural purposes or animals were excluded. No date restrictions were applied.
Study selection
Overall, 1,561 records were retrieved from searches on Medline (n = 376), PsycINFO (n = 33), Scopus (n = 745), and Web of Science (n = 407); see Fig. 1 for PRISMA diagram. Duplicates (n = 678) were removed and two authors (I.P., M.D.) independently screened the titles and abstracts of the remaining 883 records according to the stated inclusion and exclusion criteria. A further 797 articles were removed, and 86 full-text articles were assessed for potential eligibility. Based on the full-text review, 50 were excluded with reasons recorded (Fig. 1), and 33 from the initial search and a further 3 from the updated search were included (see Appendix Tables A1–A3 for a summary of all included articles). Forward and backward reference searches were carried out on all included studies, and an additional 5 articles were identified, resulting in a final total of 41 studies.
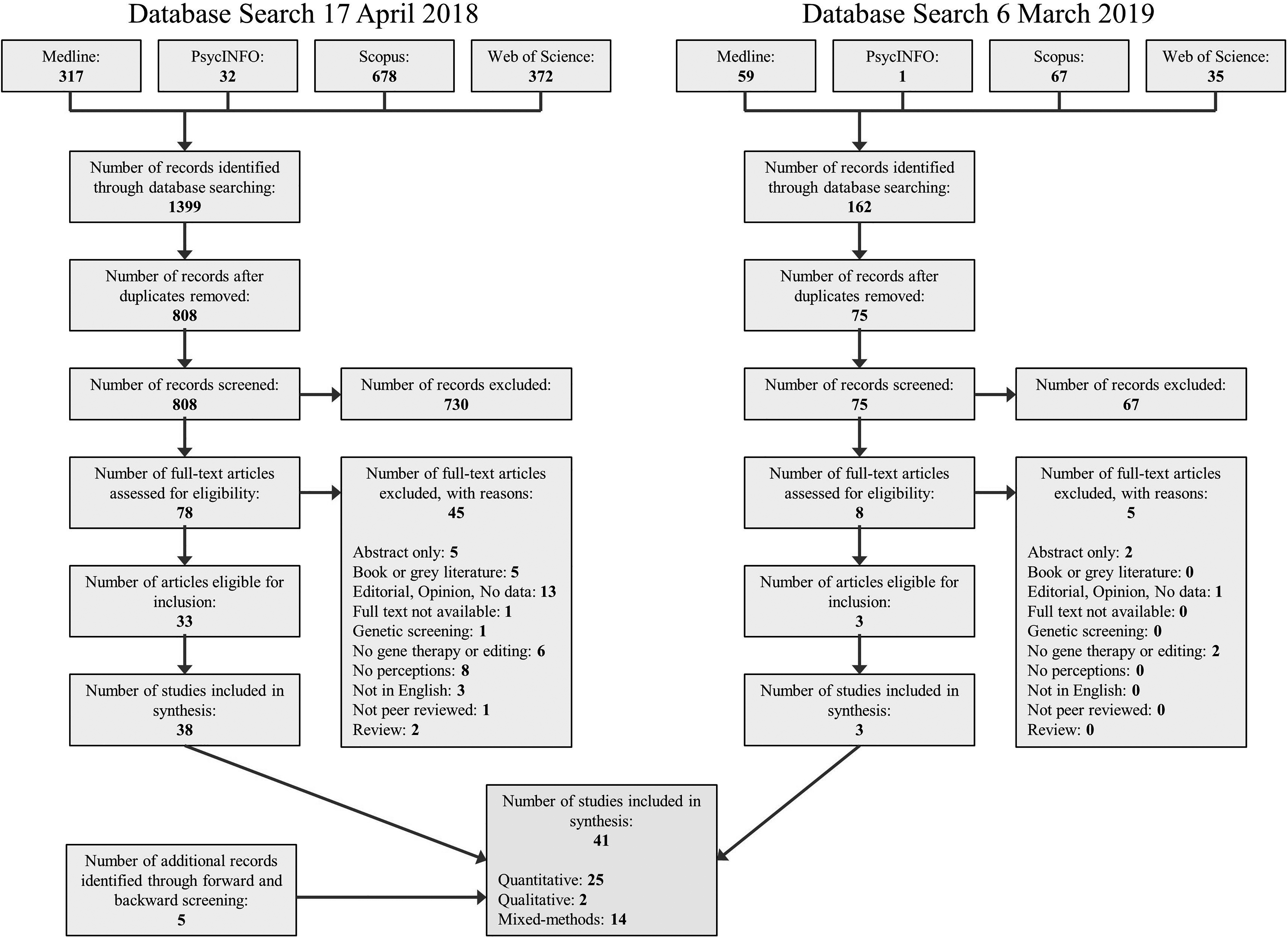
PRISMA flow diagram of study selection. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Critical appraisal and data synthesis
All included studies were critically appraised by two independent researchers for methodological quality using the Standard Quality Assessment Criteria for Evaluating Primary Research Papers from a Variety of Fields. 27 Where applicable, this was supplemented with items from the Evaluation Tool for Qualitative Studies. 28 Average quality rating scores were calculated for each study (score range 0–1). Articles with scores ≤0.5 were considered low quality, with a substantial number of unfulfilled checklist criteria. Articles with scores between 0.51 and 0.8 were considered medium quality, and those with a score >0.8 were considered high quality. Studies were not excluded or weighted in the results based on the allocated quality scores.
Results
Study characteristics
Forty-one studies were included in the review (25 quantitative, 2 qualitative, and 14 mixed-method). Studies were not excluded based on the weight of evidence provided, as it was deemed essential to provide a current and complete picture of all of the evidence to date. Methodological heterogeneity was high across all of the included studies. Studies were conducted in a range of locations, with the United Kingdom (11), the United States (10), Australia (6), and Japan (6) featuring most commonly. Articles were published from 199229 to 201930: 5 studies 29,31 –34 were published before 2000, 14 18,19,35 –46 between 2000 and 2010, and a further 23 30,47 –67 from 2011 onward, demonstrating the increasing level of awareness, scientific interest, and financial support for these recent advancements in gene therapy. The number of participants in each study varied from 2238 to a large public opinion poll of 13,201 people in China. 62
Participants in the studies were from a range of sources, including participants involved in gene therapy trials, 32 international samples, 30,47,55,57 national samples, 18,39,40,42,43,60,62 –65,67 people recruited from the general public, 34,35,38,51,52,59,63 students, 33,38,45,49,52,53,56 conference or public scientific engagement event attendees, 35,58,59,66 teachers, 54 patients, 36 –38,41,44,46,61 parents of children with a disease, 19,38 and health practitioners. 36,46,48,52 Five of the studies utilized online data collection methods. 50,51,55,63,65 Ten studies (all from 2016 onward) specifically examined gene editing. 30,55,57 –60,63,64,66,67
The majority of articles were rated as being of medium quality (n = 24), with 11 studies rated as high quality, and the remaining 6 rated as low quality. Insufficient information regarding study design and data analysis procedures was the main reason for low-quality study ratings.
Findings from all the studies were integrated such that perceptions toward gene therapy/editing were synthesized and discussed according to common themes (Appendix Table A4). These were the impact of demographics; treatment specifics; risks versus benefits of success; ethical or moral issues; trust, fears, or concerns; and changes over time.
Impact of demographics
Demographics impacted the overall acceptability of gene therapy, with studies investigating the impact of knowledge/education, gender, religion, and age.
Knowledge/education
Twenty-four studies examined the impact of knowledge of gene therapy on levels of acceptance. Ten studies compared clinician/scientist/biology or medical student perceptions with those of the general public, 29,31,33,35,43,48,52,53,62,66 8 measured differences in self-reported or tested genetic knowledge, 18,39,49,54,60,64,65,67 and a further 10 examined differences in self-reported education levels. 39,40,42,47,51,53 –55,62,63
The impact of career was mixed, with four studies finding that science-oriented careers were a significant predictor of greater levels of acceptance of gene therapy, 29,31,35,62 while six studies found little to no relationship. 33,43,48,52,53,66 In a recent study, Ganne et al. also reported no difference in the acceptance of genetic research among eye care professionals, optometry students, and the general public, reporting an average 70% approval rate across all three samples. 52
Self-reported and tested knowledge of genetics was found to positively impact the acceptance of gene therapy. For example, Cebesoy and Öztekin reported that preservice teachers with a high self-reported level of knowledge had greater levels of acceptance toward gene therapy. 54 Similarly, Črne-Hladnik et al. demonstrated that female students with higher scores on a genetics knowledge test were more likely to perceive both somatic and germ line gene therapies as useful. 49 However, in contrast, Evans et al. found that self-reported knowledge of genetics did not predict acceptance of gene therapy for a variety of applications. 39 Chen and Raffan noted that positive attitudes do not necessarily indicate that students have better knowledge of biotechnology, but rather that they are not aware of the risks. 33 In relation to gene editing, Uchiyama et al. found that despite self-reported low public awareness and inadequate understanding about gene editing, respondents thought that targeting disease-related genes was acceptable. 67
In relation to education levels, increased education levels were found to be a significant predictor of greater levels of gene therapy support in seven studies, 40,47,51,54,55,62,63 while two studies found no relationship 39,53 and one reported a negative relationship. 42 For example, Weisberg et al. reported that individuals with high school as their highest education level were less accepting of gene therapy than those with a college degree or higher. 63 In contrast, Barnett et al. found that both education level and attentiveness to issues around genetics were significant negative predictors of perceptions toward gene therapy. 42
Gender
Eighteen studies examined the impact of gender. Of those, a total of 14 articles determined that women were less approving of gene therapy. 18,34,39,42,45,47,49,53 –55,57,63 –65 For example, Napolitano and Ogunseitan found that 58% of men and 40% of women supported somatic therapy, while 23% of men and only 16% of women expressed support for germ line therapy. 34 Although Napolitano and Ogunseitan did note gender-based differences for somatic and germ line therapies, they did not detect an association of gender with acceptability toward specific applications. 34 The study by Liu et al. determined that gender did not impact acceptability within their cohort of oncology physicians and nurses, 48 and a further two publications mirrored the sentiment that gender had no significant impact upon gene editing. 30,66 Only a single study found women to be significantly more accepting of gene therapy compared with men. 62 However, this was context dependent, with the applications being (1) therapy in children with an inherited disease and (2) germ line modification.
Religion
Religious affiliations of respondents were considered in 10 studies. 18,39,46 –48,51,53,55,60,64 Religiosity was found to be a negative predictor of acceptability of gene therapy in eight of these studies. 18,39,46,47,51,55,60,64 For example, Scheufele et al. determined that respondents with no religious affiliation reported greater support for gene therapy treatment applications compared with those with religious beliefs. 60 Similarly, both Hudson and Orviska, and McCaughey et al. found religious status to be a negative predictor of the acceptance of gene therapy for a variety of applications. 47,55 In contrast, both Xiang et al. and Liu et al. reported that religion was not related to attitudes toward genetic applications. 48,53
Age
Overall, 26 of the 41 studies contained data on age, 18,31,34 –38,40,43,45,47,49,51 –55,57,59,61 –67 but only 9 specifically reported on its relationship with perceptions of gene therapy. An inverse relationship between age and acceptability of gene therapy was noted in four of the studies, 47,55,63,64 with younger participants being more accepting of gene therapy than older age groups. In contrast, one study found that older participants (31 years and older vs. 18–30 years) had a more positive attitude toward gene transfer than younger participants, describing it as “amazing.” 61 The remaining four articles that examined age indicated that it had no effect on attitudes toward either gene therapy 42,48 or gene editing. 57,66
Disease status
Weisberg et al. found no differences in levels of gene therapy acceptance in those affected with a genetic disease or with a family history of genetic disease. 63 Similarly, Iredale et al. found no difference in the levels of support for gene therapy for medical applications between the public and those with CF, but noted that families of those with CF were qualitatively more enthusiastic in their support of germ line gene therapy (i.e., “Once it is gone you would be glad to see the back of it. I would be in favour of that”). 38
Treatment specifics
This theme examined a range of factors related to treatment, and how they affect people's perceptions. These included the following: medical versus nonmedical applications of the technology, disease severity and status, acceptability of somatic and germ line gene therapy, and mode of delivery.
Medical versus nonmedical reasons for gene therapy or gene editing
A total of 21 studies specifically examined people's perceptions of gene therapy for medical (i.e., treatment or risk reduction) reasons in direct comparison with nonmedical (i.e., appearance related or enhancement) applications. 30,31,34,35,38 –40,43,50,51,53 –58,60,62,64 –66 Overall, 15 studies asked respondents their opinion on whether generalized medical versus minor physical versus appearance/enhancement applications should be accepted. 30,31,35,38,39,43,50,55 –58,60,62,64,66 Six studies compared the perceptions of gene therapy for specific applications: debilitating medical conditions (e.g., CF, cancer, HIV, neuromuscular disease, LCA, Parkinson's disease, and sickle cell disease), mental illness (e.g., depression, schizophrenia, and attention deficit disorder), minor physical conditions (i.e., cleft palate, diabetes, and obesity), and nonmedical reasons (intelligence enhancement, physical attributes, and individual characteristics). 34,40,51,53,54,65
Across almost all 21 studies, in general there was substantially less support for the use of gene therapy for nonmedical purposes compared with medical applications. For example, Napolitano and Ogunseitan investigated 13 different applications for gene therapy, finding greater support for treating a variety of medical and mental health issues (heritable diseases: 70%; mental retardation: 78%; and delayed physical deformity: 77%), compared with both personality- and appearance-related applications (baldness: 11%; hyperactivity: 29%; and obesity: 32%). 34 Robillard et al. found that 93% of respondents believed it was acceptable to use gene therapy for LCA (severe blindness at birth), compared with only 35% who believed it should be used to enhance memory. 51 Wang et al. reported greater acceptance of gene therapy for the treatment of fatal diseases from both clinicians and the public (83% and 88%, respectively) compared with gene therapy for enhancement purposes (32% and 39%, respectively). 62
One qualitative study was conducted using semistructured interviews to examine the differences between medical and enhancement purposes for gene therapy. Iredale et al. found that people were more strongly opposed to the use of gene therapy for enhancement purposes, stating comments such as “scientists have better things to do than to waste time on that.” 38 These opinions were echoed in more recent studies on the perceptions of gene editing; for example, Scheufele et al. found 59% of respondents expressed support for human gene editing to treat human medical conditions, compared with 33% who expressed support for using these techniques to enhance or improve human abilities. 60 Furthermore, Gaskell et al. reported that 75% of respondents reported positive evaluations of gene editing technology for adult therapy (e.g., it would lead to “improvements to quality of life”), and only 26% of respondent comments were positive for the use of gene editing for adult enhancement. 57
Only 3 of the 21 studies found little indication of public discomfort with using gene therapy for what is deemed to be genetic enhancement/improvement of humans. An early study by Macer et al. reported that more than 50% of participants from both India and Thailand supported enhancement of physical characteristics in humans. 31 More recently, van Lieshout and Dawson asked two small samples of Australian high school students (sample 1, n = 22; sample 2, n = 19) their position on somatic gene therapy to fight serious diseases (both samples), minor diseases (sample 1), or to enhance humans (sample 1). For sample 1, 36%, 50%, and 59% were in favor of somatic gene therapy to fight serious diseases, minor diseases, and human enhancement, respectively. In sample 2, 73% were in favor of somatic gene therapy to fight serious diseases. 56 Only one other text, Robillard et al., found some support for the use of specific applications of gene therapy for human enhancement, reporting a 77% approval rate for the enhancement of normal memory function. 50
Disease severity and availability of alternative treatments
Overall, 20 studies examined opinions toward gene therapy to treat fatal or debilitating diseases compared with minor physical conditions or benign conditions. Many found that disease severity had a direct impact on acceptance of gene therapies for diseases such as incurable heart disease, 37 deformity, 34 neuromuscular diseases, 65 Schizophrenia, 40,54,58 Alzheimer's, 50,51,62 Parkinson's, 41 and cancer. 29,31,43,48,53,54 More support was found for somatic therapy of fatal and debilitating diseases over less severe diseases for adults 35,40,55,62 and children. 55,62 Xiang et al. found that a large proportion of respondents were accepting of gene therapy for complex and potentially severe diseases such as breast cancer (63.73%) and congenital heart disease (60.28%). However, this proportion reduced with decreasing disease severity, falling to 44.38% for hypertension and 40.59% for attention-deficit/hyperactivity disorder (ADHD). 53 Similarly, 93% of respondents approved the use of gene therapy for LCA, compared with 45% for ADHD. 51 Contrastingly, Kim et al. found that within their sample of participants with Parkinson's disease, those who had milder symptoms seemed to be more willing to participate in gene therapy research compared with those with more debilitating symptoms. 41
As the severity of the disease increased, so too did the acceptability of gene therapy. Evans et al. noted a 41% acceptability for a “death sentence” genetic defect. 39 Hendriks et al. found that 85.2% of individuals would accept somatic gene therapy for a serious disease, such as a neuromuscular disorder, only decreasing to 66% when considering germ line modification instead. 65 The same was found for severity within a specific disease, with 52% of cardiac surgery patients willing to enroll in a gene therapy trial for cardiovascular disease, and a further 33% if the heart disease was otherwise incurable. 37 Liu et al. observed increased acceptability with severity through comparison of early diagnosed cancer (63.1%) versus late-stage cancer (85.1%), 48 while Uchiyama et al. found support for therapies when the disease would either shorten life or result in long-term care. 67 In contrast, van Lieshout and Dawson reported that adolescents were more likely to be in favor of somatic gene therapy for minor (50%) in comparison with serious diseases (36%). 56
Four studies evaluated gene therapy versus alternative treatments. 32,36,39,54 In a cohort of 16 CF patients, all indicated that they had a preference for gene therapy as an alternative therapy over conventional heart and lung transplantation. 32 Holm and Jayson found that oncology staff deemed gene therapy (48.9%) to be a safer cancer treatment option than chemotherapy (7%), with patients (26.7%) also agreeing that gene therapy was safer than chemotherapy (6.7%, with 66.7% neutral). 36
Somatic cell gene transfer versus germ line transgenesis
Seventeen articles compared the attitudes of participants toward somatic cell gene transfer, germ line transgenesis, or embryonic editing as three modes of therapeutic intervention. 30,31,34,35,38,40,45,49,55,56,58,60,62,64 –67 There was a noteworthy difference in the acceptability of somatic gene therapy, and its benefits were largely accepted (range: 4534–98% acceptance 66 ). In contrast, the use of germ line transgenesis was more divisive, with many articles reporting participant wariness toward this type of therapy, resulting in a lower level of acceptability 34,35,38,40,45,49,56,58,62,64,65 (range: 1634–71% 35 ).
Exceptions to the view of somatic transgenesis being more favorable were by Macer et al., who only found a small difference in acceptability 31 ; and both Scheufele et al. and McCaughey et al. who reported similar levels of support for both somatic and germ line therapies. 55,60 Iredale et al. noted differences in the willingness to personally use gene therapy for somatic (95.5%) over germ line transgenesis (54.4%). 38 This same cohort was divided when comparing the ethical differences between the two modes of therapy, with 40.9% expressing that there is no ethical disparity between somatic and germ line gene therapies, and 36.4% stating that the two therapies are distinct.
Mode of delivery and assessment
Overall, four studies examined perceptions toward either the mode of gene therapy delivery or how effectiveness would be assessed. 32,37,44,61 Cardiac surgery patients expressed a preference for catheter-based delivery of a gene therapy product over surgical gene transfer (94% vs. 80%, respectively). 37 In that same study, adenovirus was considered an acceptable gene transfer vector by 73% of patients, although the study did not assess the acceptability of other types of gene vectors. 37 Hemophilia patients clearly had a preference for subcutaneous administration (76.3%), with intramuscular and intravenous routes also considered positive alternatives (66.2% and 60.1%, respectively). 44 Bone marrow transplantation was the least favored administration modality, with 66.4% of patients declaring this method “not acceptable.” 44 Individuals with sickle cell disease indicated increased apprehension upon discovery that chemotherapy would be used before the infusion of stem cells that had been treated with a modified HIV vector containing the therapeutic β-globin gene. This apprehension was due to both the chemotherapy and resultant side effects, and also with the use of the HIV vector as the delivery vehicle for transfer of the therapeutic gene, with individuals describing its use as “scary.” 61
A single study analyzed acceptability and assessment of gene therapy efficacy. This study used a single nasal application of DNA liposomes in CF patients and noted that 9 of the 16 participants found the invasive nasal brushings, biopsies, or daily potential difference measurements to be tedious and unpleasant. These methods of outcome assessment subsequently had a direct negative bearing upon attitudes toward gene therapy. 32
Risks of gene therapy versus the potential benefits of success
This theme examined the risks and benefits of treatments and balanced these with the likely expectations that treatments would be successful. A total of 22 studies specifically examined a range of risks and benefits, 18,19,29,31 –33,41,43,44,47,49 –51,53,54,57,59,61 –63,65,67 and many noted that acceptability of gene therapy or human genetic manipulation was very closely related to the risk of the intervention. 50,62,65 In general, there was broad support for the benefits of gene therapy for human use, however, potential risks were also important to consider. For example, Robillard et al. 51 found that 75% of a general sample of people from the United States thought that gene therapy would have positive impacts on society, 74% agreed that gene therapy would possibly provide cures for many diseases, and 54% thought that the benefits of gene therapy outweigh any harms. In a large European Union survey, Hudson and Orviska 47 found that the majority of participants thought gene therapy was useful to society, however, they also had risk-related concerns. Gaskell et al. examined the public's view of gene editing, with 75% of respondents giving a positive evaluation of gene editing technology for adult therapy. Participants frequently thought gene editing would lead to “improvements to quality of life”; it would enable “curing dementia”; and that the “benefits outweigh[ed] the risks.” 57
When participants identified risks they included unacceptable health risks 65 and the possibility of “things going wrong” due to mistakes such as the production of leukemia in SCID trials, 47 or potential negative future consequences. 61 For example, in a study of patients with sickle cell disease, participants indicated that the risk of developing cancer following gene therapy meant they would be trading sickle cell for a potentially more serious disease. 61 Although their disease might impact their life and reduce their life expectancy, many thought it was better to continue their current treatment rather than risk developing a life-threatening condition. Others identified the risk of deliberate human germ line alterations that would impact future generations. 47 Together these results suggest that it is important to understand the level of such off-target effects that participants would find acceptable for each disease. 65
Furthermore, some participants voiced disapproval that gene therapy was unnatural, 31,43 with others saying diseases have a purpose in life. 65 In a German study, Hampel et al. found that only one-third of the people they interviewed thought that the risks of genetic engineering outweighed the chances of success. 18 In addition, over half of the preservice teachers in one study either agreed or strongly agreed that “changing a person's genes is too risky, whatever the benefit might be.” 54 However, these feelings were countered in an earlier gene therapy trial reported by Blair et al., which stated that participants generally assumed that “doctors would not put them at risk.” 32 Furthermore, in a Chinese sample, 41% of respondents disagreed with the statement, “It is too risky to try to change people's genes,” and 41% were neutral (remainder unknown). 53 The willingness of participants to take part in a gene therapy trial also appeared to be related to their risk perception, with those who were more willing to participate also more optimistic about the potential benefits of gene therapy. 41
In a CF gene therapy safety trial using liposomes for delivery—where the vector is regarded as being safer than viral vectors—almost all patients thought that they had placed themselves at no risk whatsoever by taking part, 32 although this was before the SCID trials that identified the risks of genotoxicity. In contrast, although cancer induction is a minor risk for gene therapy, more than half of a group of patients with hemophilia thought that the long-term perceived risk of cancer development was a major concern. 44 Kim et al. also found that participants who were willing to participate in gene therapy trials for Parkinson's disease perceived less risk than those not willing to participate and were also more optimistic about the benefits to society. 41
Demographics
The interdependent relationship between risk and acceptability also varies based on demographic factors. Hampel et al. noted that men were more accepting of gene therapy, and perceived fewer risk than women. 18 In another study, women were significantly more likely to agree with the statement, “It is too risky to try to change people's genes,” 53 while men were found to have higher levels of confidence in safety. 47
Risk perceptions did not vary greatly with ethnicity with the exception of one Chinese survey, which found that only 31% of respondents agreed with the statement that: “The benefits of gene therapy will be greater than the harm it may cause.” 53 However, the authors did note that the greater concern of the Chinese population about gene therapy may be caused by an absence of understanding and media coverage in China. 53
Potential ethical or moral issues
The application of genome engineering requires significant ethical and moral consideration and this was a primary theme across over half of the included articles, with 24 articles discussing these issues when determining levels of acceptability. 19,29,31,32,34 –36,38,39,43,45 –47,49 –51,53,56 –58,60,62,64,65 The most common ethical concern was that genetic modification was interfering with nature (unnatural) 29,31,32,38,45,46,49,50,53,62,65 and that it was “playing God,” 29,31,36,46 although some religious leaders considered it “preservation and advancement of life.” 46 As expected, gene therapy for diseases was found to be significantly more morally acceptable compared with enhancement. 35,38,39,50,51,57,60,62,64 Slovenian students considered somatic gene therapy as ranking highly in terms of usefulness and moral acceptability. 45,49 As previously discussed, the acceptability of germ line transgenesis is generally lower, with the potential for inadvertent germ line transmission demonstrated to be of ethical concern. 50
Some of the moral concerns at a societal level include the impacts of increased longevity, 51 the accompanying exponential population growth resulting from the decreased incidence of disease, 51,53 and the potential for uneven distribution of resources. 50 Further ethical considerations were related to the reduction in human diversity 56,65 and the lack of natural selection. 43,56 Techniques that are perceived as substantially less risky are considered more “morally acceptable” and “useful to society.” 47,49 Further moral considerations included the perception that natural abilities would not be unique if people use gene therapy for enhancements 56 and may even threaten the integrity of the human species. 34,56 There could also be a risk of losing a sense of self (personal identity), particularly in the context of gene therapy for the brain, or changes in sexual orientation as a result of gene therapy. 50,51 In contrast, those not opposed to germ line transgenesis for improved intelligence cited that it would allow users to contribute more to society, and they had concerns of falling behind if others instigated its use first. 65
A significant recurring ethical concern was whether a parent has the right to decide on the use of gene therapy, either somatic or germ line, for their child. Some studies suggested that parents had no right to modify their unborn child's genes using germ line therapy, 44,49,56,65 while others discussed the treatment of children as a parental right or duty, 38,57 or even a moral imperative toward one's offspring by not withholding the opportunity for therapy and subsequent improvement in quality of life. 65 Ninety-nine percent of respondents thought it was ethically sound to administer a gene therapy for CF to children (aged 6 months–17 years), on the condition that safety was the priority. 19 The administration of gene therapy in utero or to a child for a fatal or debilitating disease also scored highly by the public, indicating general agreement of these uses. 62 Five other studies were in agreement with using gene therapy on children, 29,31,34,38,43 with two showing more support for gene therapy in children than adults. 29,31 Several studies showed support for in utero gene therapy for health-related reasons that would not result in germ line transgenesis, 34,40 ones that would result in germ line modification, 55,65 or ones that were embryonic but did not specify germ line transgenesis. 30,64,66
In some instances, the ethical division was less clear with 61% of individuals in agreement that parents could use human germ line genome editing for the purpose of having a child if there was no other means to do so. This decreased to 45% when used to reduce the risk of a serious disease as opposed to being a treatment for it. 58 Iredale et al. found support for the statement that parents have the right to obtain gene therapy for their children (73%), but less support for in utero gene therapy where 55% agreed with the statement that “children had the right to be born with the genetic makeup they had at conception,” while 27% were in disagreement, and 18% felt unsure. 38
Another interesting topic of ethical debate was the selection of participants who would be enrolled in gene therapy trials 46,51 and the ethical responsibility to ensure accurate information for consent when participating in high-risk research. 46,51 Participants in various studies also determined that gene therapy had the scope for generating genetic discrimination and injustice. 50,53 The high cost of gene therapies was cited as a concern 53,62 with the associated ethical apprehension being the creation of different classes of individuals based on who could afford gene therapy for modification purposes, 51 or therapy being a privilege only for the wealthy and powerful. 53
When given the opportunity to discuss controversial scientific topics, such as gene editing, communication with a panel of topic-specific experts was shown to have no impact on the level of ethical concern for gene editing or the belief that this sort of therapeutic intervention would progress humankind. Instead, such discussions were found to significantly affect the belief that gene editing is morally acceptable, with agreement increasing following such panel discussions, 59 a trend supported by others. 40
Trust, fears, or concerns
A total of 21 studies raised the topic of trust, fears, and concerns related to the use of gene therapy or gene editing. 18,29,31,32,35 –37,41,42,44,46,47,50,51,56,57,61 –63,65,67 Most fears could be grouped into medical or trial participation concerns. Concerns related specifically to medical outcomes included infections, 32,41,44 cancer, 41,44,61 inflammation, 41 thrombosis, 44 bleeding, 41 infertility, 61 fear of chemotherapy, 61 reactions to anesthesia, 41 and contracting hepatitis 44 or HIV. 61 More generally, participants expressed concern about misuse, 31 safety, 62 unacceptable health outcomes, 29,31,47,65,67 adverse medical side effects, 50,51,62 their current disease getting worse, 41 or unknown or unpredictable long-term consequences such as undesirable mutations. 32,37,41,50,56,57,63,65 The acceptability of additional treatment side effects has been shown to correlate with the potential cure rate, highlighting a trade-off between side effect/therapeutic benefit of a gene therapy treatment. 36 Participants also had concerns over being excluded from other clinical trials, 41 and racial and social disparity leading to recruitment bias for clinical trials. 46 A lack of adequate information about gene therapy before a trial was also cited as a worry. 50,51 Surprisingly, the fear of eugenics was only mentioned twice 31,63 and does not appear to be a significant cause for concern in those considering the application of gene therapy.
Many fears and concerns were accompanied with an inherent lack of trust. These issues centered around mistrust of research, 46 scientists, 18 the medical system, 46 and government rules and those in charge. 42 Ng et al. determined that respondents were most trusting of international regulatory bodies such as the World Health Organization, for regulatory oversight, while scientific organizations and ethics committees were deemed less favorable. 35 Religious organizations, trade unions, and political parties rated lower still in terms of trust, from a regulatory perspective. 35 Scientists expressed issues of trust surrounding the control on techniques to ensure protection from misuse 29 leaving scope for change and improvement.
Changes over time
Although the gene therapy and gene editing fields have rapidly advanced over the last decade, only two articles specifically looked at changes in attitudes toward gene therapy over time. 35,43 Both reported on public attitudes to gene therapy in Japan based on opinion surveys. Macer et al., covered surveys conducted from 1991 to 2003, 43 finding that levels of optimism toward gene therapy for a serious or fatal disease remained relatively consistent over that time period. They also reported that there was little difference in attitudes toward gene therapy between the public and scientists. 43 Ng et al. reported on a subset of the same surveys from 1991 to 2000. 35
Discussion
The purpose of this article was to synthesize the research to date on people's perceptions of gene therapy and gene editing for human applications, and to highlight factors that influence acceptability. Key points are summarized below along with a series of recommendations to advance the work in this field.
Impact of demographic factors
Demographic factors are known to play a substantial role in influencing public perceptions relating to genetic modification. Generally, younger individuals, males, those with lower religiosity, better (self-reported) knowledge, and increased trust in scientists were shown to have more support for both gene therapy and gene editing technologies. Specifically, most studies found that younger participants were more accepting of gene therapy, possibly due to an increase in concern by older individuals and reduced exposure to the development and use of these modern technologies. Only a single study found that women were more accepting of gene therapy than men. 62 One explanation for these gender-associated differences in acceptability could be the concern that women have toward science and technology, and the increasing control that technology has over our lives suggested by some researchers. 68 While it has been shown that women are generally more risk averse than men, 69 it is possible that the perceived risks of gene therapy may be more acceptable to women in certain situations, for example, when confronted with the reality of a serious or debilitating disease affecting one's offspring or children in general compared with gene therapy as a whole for adults. These differences also call for improved gender-specific educational programs to address the specific concerns more often associated with women.
Knowledge and education levels were generally significant predictors of the level of support for these technologies; however, some findings were mixed. While it has been suggested that negative perceptions of gene therapy can be attributed to a lack of knowledge, the issue is more complex. Mixed results regarding the relationship between knowledge and perceptions could be due to the inconsistent way that knowledge is measured, for example, through career choice or education. Self-reported and tested knowledge on genetics was found to have the most consistent results; however, there remains a need for research to unify measurements of knowledge for consistency, clarity, and comparative analyses. Strong et al. also suggest that participant engagement over time might give opportunities to provide education; answer questions, address misconceptions, and allow participants to better weigh up the risks and benefits of treatment. 61 They also recommend the use of education materials containing a combination of visual and numerical information, along with patient experiences. 61
Perceptions based on treatment specifics
Overall, there was substantially less support for the use of gene therapy for nonmedical (i.e., enhancement) purposes compared with medical applications. Acceptance was lowest for nontherapeutic enhancement procedures, driven strongly by concerns such as “playing God,” “going against nature,” and also societal concerns such as disparities in resource allocation or access to procedures based on socioeconomic standing that could lead to discrimination or inequality. Gene therapy was also more acceptable for serious or fatal diseases rather than debilitating diseases (e.g., Alzheimer's or Parkinson's). This is likely due to the perception that gene therapy carries some risks, so the risk/benefit ratio is perceived to be inversely proportional to the severity of the disease. For some participants, the health risks were unacceptable due to the possibility of “things going wrong,” and that for patients with less severe conditions it was better to continue their current treatment rather than risking development of a life-threatening condition.
Importantly, in cases of disagreement for genetic modification for health-related applications, an absence of a complete understanding of the technologies themselves and their accompanying potential risks was cited as contributing to apprehension to their use as opposed to the actual genetic modification itself. 30 Adequate education of participants about these aspects will be of fundamental importance to its broader uptake and acceptance.
Acceptability was inversely related to the invasiveness of the delivery technique or assessment of therapeutic efficacy, however, increased discomfort or side effects arising from a gene therapy were considered acceptable for a fatal disease if there was potential for that therapy to provide a cure. An important element of patient acceptability was the description of the mode of gene delivery (i.e., the gene vector). Describing the delivery vehicle for transfer of the therapeutic gene as an “HIV vector” had a direct negative bearing upon attitudes toward gene therapy. 61 It is possible that if it were instead described as a “lentiviral gene vector,” then it would be less confronting, and lead to greater acceptability. However, it should be noted that this level of technical detail and the implications of using these different vector delivery methods may not be easily understandable by everyone. Education consisting of simple explanations that clearly outline the points of differences between the vector delivery systems may aid understanding to enable the public to accurately assess each therapy.
Risks versus benefits
The importance of scientists and medical personnel clearly explaining the possible risks and benefits of genetic therapies is becoming more obvious. In many studies, knowledge of gene therapy was intertwined with perceptions of its risks and benefits. For example, participants in one study remarked that including the percentage likelihood of risks was helpful for them to form their own opinions about gene therapy. 61 Willingness to take part in clinical trials was also closely related to personal risk perceptions and optimism about the potential benefits. Hudson and Orviska found that people who were more educated and had greater knowledge about gene therapy viewed it as less risky. 47
Jaffé et al. noted that they did not explicitly describe the risks of gene therapy in their study, and that providing more information to participants may have resulted in them being less accepting of risk. 19 In support of this notion, when the potential risks and side effects of a gene therapy were explicitly explained to patients with sickle cell disease, they perceived the treatment less favorably. 61 Weisberg et al. also found that the support for human germ line modification was slightly lower when the risks were made more explicit. 63 However, perceptions of risk and benefit are not necessarily inversely related, 59 highlighting the need for open discussions with stakeholders for each application and therapy as they may have variable risk profiles.
Trust, fears, concerns, and ethical and moral issues
Fear and concern stem mainly from the misuse of these technologies, unacceptable health outcomes, adverse medical side effects, a current disease getting worse, or unknown or unpredictable long-term consequences such as undesirable mutations. For example, participants considered germ line genetic modifications such as introducing HIV resistance “a slippery slope toward other applications deemed morally unacceptable.” 65 These applications have recently become a public focus due to the use of CRISPR by Chinese Scientist Dr. Jiankui He to alter the genome of human embryos before implantation to confer HIV resistance in two infants (November 2018). This news received swift international condemnation, with the medical field saying it is irresponsible to proceed with clinical germ line editing at present. 70 This type of rogue research and media attention creates mistrust of research, scientists, the medical system, government rules, and those in charge.
While there was little empirical research related to cost as a concern, anecdotally, this topic is rapidly becoming one of the most frequently mentioned aspects of the gene therapy debate in public forums. As such, it is an important avenue for future research. Future research should aim to compare actual real-world costs and people's perceptions of costs for gene therapy relative to alternative therapies. It would also be interesting to assess the influence of gene therapy cost and payment models (e.g., public versus private health insurance and outcome- versus value-based pricing) on people's perceptions and acceptability.
For some people, there are ongoing ethical and moral issues surrounding gene therapy and gene editing. It is therefore a moral obligation of all those involved in the development and implementation of therapeutic therapies, from scientists to policy makers, to ensure that due diligence is performed with regard to the safety of these therapies, and to ensure that complex information is relayed in an understandable and transparent manner to regain trust and mitigate these current fears and concerns. The issues of mistrust among particular populations, especially some minority groups, also need to be addressed as they form a barrier for the recruitment of these groups into clinical trials. 46
The complex relationship between the use of gene therapy and its moral and ethical considerations should be at the forefront of all discussions involving genetic modification, with personal, societal, and environmental implications balanced against the potential benefit of genome modification. Continuous conversations between patients, the public, scientists, clinicians, and policy makers need to be built and maintained to deliver resolutions/agreements on how to move forward with these therapies and what would be considered “right” at a particular point in time for the world's population.
Changes over time
More than half of the articles in this review were published in the last 8 years, likely owing to the maturity of the gene therapy field as a whole and also more media attention and discussions around the topic with the public. This demonstrates the increasing focus that the scientific community is placing on this type of work as a viable treatment option for a range of different complex diseases, and the importance of understanding people's perceptions toward this technology. However, since 2007, none have looked at changes in perceptions over time. Collectively, from the studies reviewed, it appears that there is an upward trend in acceptability of gene therapy as a treatment alternative when looking at the percentage of people who were accepting, particularly for medical purposes. Some views have also changed over time based on other medical advances. For example, participants in 1999 viewed gene therapy for HIV as acceptable if it could prolong lives. 33 In 2018, a different study reported that germ line modification to produce HIV resistance was not considered necessary due to the low risk of acquiring HIV, 65 and the likely availability of other acceptable and effective treatments.
While the general trend for medical somatic therapy shows an increase in acceptability over time, germ line modifications remain contentious and a heated source of ethical debate. Deviations from the status quo have been vehemently frowned upon with He Jiankui's editing of human embryos sparking international outcries 71 that have culminated in the Chinese government immediately tightening up regulations against germ line editing. 72 Numerous cell and gene therapy committees have rebuked the act and have subsequently called for an international moratorium on the use of germ line genetic modifications. 73 The expansion of gene therapies into the medical arena, coupled with increased media exposure, is likely to change current perceptions. It will be critical to understand how the public's perception is tracking with these advancements and how much of an impact the recent gene therapy successes have had on the public's perception and willingness to participate in gene therapy clinical trials and whether there are still additional barriers that need to be overcome in the future. Future research could usefully track potential changes in perceptions over time via longitudinal methods, or by examining current versus retrospective accounts of perceptions among different samples.
Limitations and future research directions
Limitations exist with all forms of research, and the research presented in this field is no exception. To provide a comprehensive review, all relevant studies were included. However, it was clear that a number of misconceptions surrounding gene therapy and gene editing still exist, both among researchers and the public. For example, there were suggestions it could change sexuality, 50 demonstrating that some of the studies reviewed did not understand the true purpose, capabilities, and/or reasonable applications of current gene therapy and gene editing techniques. It is likely that these misconceptions are driven by the media and sensationalized in movies (e.g., Gattaca). As such, it is essential for future research in this space to be performed by multidisciplinary teams of gene therapy experts—including clinical researchers, basic scientists, social scientists, bioethicists, and patient advocacy groups—to ensure a comprehensive understanding of perceptions of gene therapy and gene editing.
Overall, the measurement of perceptions of gene therapy and gene editing was inconsistent and there is a need for future research to use standardized and validated forms of measurement to draw firm conclusions. In addition, concepts such as “risk” with regard to gene therapy have not been clearly defined within the literature, and as such, this term was used in a variety of contexts. These included general nonspecific risks, 57 actual risks posed by gene therapy, 65 negative consequences, 61 or greater philosophical risks pertaining to humankind. 34,56
While the studies reviewed reported on data from a wide range of samples, relatively little research has been done on specific consumer groups. Future research should address this by examining the perceptions of individuals who are closely associated with different diseases. Finally, only two studies (that drew from the same data set) specifically reported on changes over time. 35,43 As such, any findings related to changes should be considered with caution.
Recommendations and future directions
Public engagement can improve knowledge and change risk and benefit perceptions, but the relationship between these factors remains complex. 59 Based on the studies we reviewed, we have created the following list of recommendations and directions for future research to improve public perceptions of gene therapy.
Improve the standard of informed consent
Clear and consistent communication between patients, clinicians, and clinical trial managers is integral to fostering a sense of trust and empowerment to patients choosing to undergo genetic therapy. In particular, it is important to design informed consent documentation specifically for gene therapies, being mindful of the phrasing of content, terminology, and the amount of detail provided. 51,61 Information should be engaging with complex ideas preferably portrayed with images and videos for clarity. 37 Specific attention should be given to accurately convey messaging that is often portrayed fallaciously within the media (e.g., the generation of eugenics or designer babies). Future research should obtain insight from focus 52 and patient advocacy groups to determine any potential miscommunication of information before broader dissemination.
Use minimally invasive procedures
While invasive procedures remain the only mode of delivery for many potential gene therapies, technological advances are likely to bring about less invasive methods of delivery, and with that an expected increase in acceptability. Given the direct negative correlation between invasiveness and acceptability highlighted above, 32 there must be a continuing drive to provide innovative ways to combat the current hurdles associated with noninvasive delivery of some gene therapies when alternatives may be possible.
Develop greater trust
To gain public trust, it is critical to deliver information to the public and potential patients that is understandable, relatable, unambiguous, and reliable. 62,65 Greater emphasis needs to be given to the development of public engagement tools for scientists and clinicians to feel adequately equipped to engage with the public and build long-standing and honest relationships built on trust. A recent 2019 study went so far as to note that sharing visuals of scientists themselves versus innate laboratory objects was enough to change perceptions and garner increased trust by humanizing scientists on social media. 74
Furthermore, information should be relayed frequently for the public to remain updated and feel empowered by new developments with the gene and cell therapies. 46 It is important to address any shortcomings in understanding or inaccuracies with reliable scientific content to prevent negative perceptions toward genetic therapies based on misinformation. 46,61 It is likely that increased exposure and a continuous track record of transparency between scientists and the public would significantly improve issues of trust.
Develop appropriate policy frameworks for gene therapy regulation
Patients need to know that new therapies are being correctly regulated and that policy decision-makers are provided with enough up-to-date scientific insight and public participation 57 to drive these therapies forward while keeping safety a priority. Pairing current expert knowledge with a clear understanding of past errors has already provided improved guidelines for regulating gene therapies, but there is still scope for international clarity and consensus for many of their uses. Public confidence can be developed and maintained through instigation of more dynamic and open communication between the regulatory agencies that are drafting guidelines and implementing policies. This has become a realization with the recent notice by the FDA requesting formal input into their draft guidelines for the enhancement of diversity of clinical trial populations, enrollment practices, eligibility criteria, and trial designs. 75 This method of consultation and transparency specifically for gene therapy is highly recommended to improve the quality of the guidelines through constructive collective consultation and improve public trust in health agencies. It will also be essential to include postsuccess analyses in any future research looking at perceptions of somatic gene editing changes.
The implications of genetic modification are not always well understood or even known scientifically, so we should continue to tread with caution while continuing to engage in global discussions on what is defined as acceptable. There is an urgency to gain international regulatory control over the use of these therapies for the right purposes, to avoid inappropriate application of genetic therapies. Currently, this is largely regulated by the FDA in the United States who are increasing the number of clinical reviewers for the evaluation of cell and gene therapies, and the European Medicines Agency Advanced Therapy Medicinal Product who have recently completed their consultation period (July 2019) for guidelines of cell and gene therapies. Ideally, interagency consultation and a unified global regulatory framework should be established to streamline the regulatory process and determine which applications are deemed ethically, morally, and scientifically safe and acceptable for clinical use across geographical boundaries.
Provide better gene therapy education to the public and stakeholders
The rapidly changing biomedical landscape is demanding more in-depth science and biotechnology teaching, even at high school level. This shift is driven by a need to improve basic science and biotechnology knowledge 54 and bioethical principles 49 for teachers and students. Gaps in knowledge should be addressed before subsequent delivery of information to ensure good foundational science understanding. 56 Clinicians in relevant fields must stay up-to-date with the most current and ground-breaking gene therapy research and practice spanning oncology, ophthalmology, hemoglobinopathies, immunodeficiencies, and lysosomal storage diseases. Furthermore, knowing the factors that can influence people's perceptions will be critical to assist clinicians to act as a bridging point between patients and those developing gene therapies, and assist them to garner acceptance from patients for clinical trials.
There is an increased need and desire for the public to know more about these new and exciting genetic therapies. Opportunities to instigate multidirectional communication between the public, scientists, clinical staff, and policy decision-makers using public engagement events 59 and social media 50 will play a pivotal role in expanding public knowledge. Training in public engagement is essential for all involved in the development and clinical administration of these therapies.
New and innovative ways of making connections between stakeholders are essential. Recently, the American Society of Gene and Cell Therapy debuted their patient education program to educate and inform patients, families, and the public about genetic diseases, therapies, and updates on clinical trials. 76 More of these initiatives must be developed in the coming years to further encourage education. Emphasis needs to be placed on finding ways to communicate, particularly with women, individuals in rural areas, older individuals, those with strong religious tendencies, and those with less education, to promote gene therapy literacy competency. This will subsequently assist these groups to participate in fact-based discussions on the topic, and ensure that correct information is given to those with varying levels of understanding.
Each gene therapy application must be considered on its merits
Gene therapies cannot be placed under broad “blanket” regulations. It has become clear that each application will need to be assessed on its own merits and ratio of risk-to-reward. 30,65 Policies and regulations generated should also be based on individual circumstances (risk, degree of disease severity, and medical vs. enhancement), as therapies that exhibit lower risk or are for severe diseases would have higher reward, are likely to be more acceptable, and have an easier road to clinical implementation. Each application will also need to establish the level of risk that would be acceptable for patients undergoing specific gene therapy treatments in situations where acceptability is conditional (e.g., method of delivery, access to alternatives, and assessment of efficacy). 65 While acceptability has notably improved for certain applications, others still require significant ethical and legal consideration before translation toward the clinic. Currently, germ line modification is banned worldwide, and is largely not ethically accepted. In our opinion, subsequent human germ line editing should continue to be banned until an ethical and regulatory framework has been established and agreed upon following extensive and broad-ranging consultations with the public, scientists, clinicians, stakeholders, and policy decision-makers.
Footnotes
Acknowledgments
The authors also acknowledge Nikki May who assisted with the original search design, Chloe Craig who assisted with the article quality assessment, and A/Prof. David Parsons for his valuable topic insight and article feedback.
Author Disclosure
No competing financial interests exist.
Funding Information
The study was supported by the Australian Cystic Fibrosis Research Trust. M.D. was supported by a Robinson Research Institute Career Development Fellowship.
Summary of the themes and their association with acceptability of gene therapy
| Theme | Subtheme | Acceptability | References |
|---|---|---|---|
| Demographics | Greater knowledge/education, n = 24 | Positive, n = 15 | 18,29,31,35,40,47,49,51,54,55,60,62 –65 |
| Neutral, n = 7 | 33,39,43,48,52,53,66 | ||
| Negative, n = 2 | 42,67 | ||
| Gender (women), n = 18 | Positive, n = 1 | 62 | |
| Neutral, n = 3 | 30,48,66 | ||
| Negative, n = 14 | 18,34,39,42,45,47,49,53 –55,57,63 –65 | ||
| Religion, n = 10 | Positive, n = 0 | ||
| Neutral, n = 2 | 48,53 | ||
| Negative, n = 8 | 18,39,46,47,51,55,60,64 | ||
| Age (young), n = 9 | Positive, n = 4 | 47,55,63,64 | |
| Neutral, n = 4 | 42,48,57,66 | ||
| Negative, n = 1 | 61 | ||
| Disease status, n = 2 | Positive, n = 0 | ||
| Neutral, n = 2 | 38,63 | ||
| Negative, n = 0 | |||
| Treatment specifics | Medical over nonmedical, n = 21 | Positive, n = 20 | 30,31,34,35,38 –40,43,50,51,53 –55,57,58,60,62,64 –66 |
| Neutral, n = 0 | |||
| Negative, n = 1 | 56 | ||
| Increased disease severity, n = 20 | Positive, n = 18 | 29,31,34,35,37,39,40,43,48,50,51,53 –55,58,62,65,67 | |
| Neutral, n = 0 | |||
| Negative, n = 2 | 41,56 | ||
| Gene therapy over alternative treatments, n = 4 | Positive, n = 2 | 32,36 | |
| Neutral, n = 0 | |||
| Negative, n = 2 | 39,54 | ||
| Somatic over germ line transgenesis, n = 15 | Positive, n = 11 | 34,35,38,40,45,49,56,58,62,64,65 | |
| Neutral, n = 4 | 30,31,55,60 | ||
| Negative, n = 0 | |||
| Increased invasiveness of delivery, n = 2 | Positive, n = 0 | ||
| Neutral, n = 0 | |||
| Negative, n = 2 | 32,61 | ||
| Risks of gene therapy | Too risky (risk outweighs benefit), n = 22 | Positive, n = 9 | 29,31,44,47,49,54,61,63,65 |
| Mixed (balance of risk/benefit), n = 5 | 33,50,51,59,62 | ||
| Negative, n = 8 | 18,19,32,41,43,53,57,67 | ||
| Potential ethical or moral issues | Effect of ethical and moral issues, n = 24 | Positive, n = 2 | 40,59 |
| Mixed, n = 4 | 45,46,49,65 | ||
| Neutral, n = 0 | |||
| Negative, n = 18 | 29,31,32,34,36,38,43,45 –47,49 –51,53,56,62,64,65 | ||
| Trust, fears, or concerns | Trust (lack of), fears, or concerns, n = 21 | Positive, n = 0 | |
| Neutral, n = 0 | |||
| Negative, n = 21 | 18,29,31,32,35 –37,41,42,44,46,47,50,51,56,57,61 –63,65,67 | ||
| Changes over time | Increase in time, n = 2 | Positive, n = 2 | 35,43 |
| Neutral, n = 0 | |||
| Negative, n = 0 |