
Abstract
Hemophilia arthropathy (HA) represents the majority of morbidity in severe hemophilia patients, especially in resource-limited countries. Adeno-associated virus (AAV)-mediated gene therapy is showing promise for managing hemophilia. However, patients with neutralizing antibodies (NAbs) against AAV, and inhibitors to clotting factors, are excluded from such therapy. This study explored the feasibility of AAV-mediated local gene therapy for HA. Factor VIII knockout (FVIII−/−) mice, with or without a FVIII inhibitor, were subjected to hemarthrosis induction and treated with either intravenous (IV) or intraarticular (IA) recombinant human factor VIII (rhFVIII). To investigate whether rhFVIII carried the risk to develop a FVIII inhibitor, FVIII−/− mice were treated with three doses of IV or IA rhFVIII and inhibitor development was measured. In patients with established HA requiring synovial fluid aspiration, plasma, and synovial fluid were collected and measured for anti-AAV capsid IgG (serotypes 1–9 and 843) and NAbs for AAV843. IA rhFVIII provided better protection from synovitis compared with IV rhFVIII, with or without the FVIII inhibitor. While IV rhFVIII led to all FVIII−/− mice developing an FVIII inhibitor (n = 31, median 4.9 Bethesda units [BU]/mL), only 50% of the mice developed a FVIII inhibitor by IA administration, and at a lower titer (median 0.55 BU/mL). In hemophilia patients, total anti-AAV IgG was lowest for AAV4 and AAV5, both in plasma and synovial fluid. Anti-AAV IgGs in synovial fluid for most samples were lower or similar to the plasma levels. These results show that direct IA rhFVIII administration yields better protection against bleeding-induced joint damage, even in the presence of an inhibitor antibody. IA rhFVIII delivery carried a lower risk of FVIII inhibitor formation compared with IV FVIII. The anti-AAV antibody level in synovial fluid was similar or lower than the plasma level, supporting the feasibility of local gene therapy for managing HA.
Introduction
Hemophilia is a genetic disorder due to the lack of functional clotting factors (i.e., factor VIII [FVIII] for hemophilia A and factor IX (FIX) for hemophilia B). Hemophilia arthropathy (HA) develops after repeated bleeding into the joints and represents the majority of morbidity in severe hemophilia patients. In recent decades, the management of hemophilia has progressed dramatically. Nonetheless, the management of HA and associated bone damage is still a major concern, especially in undeveloped countries. 1,2 Even under current prophylactic regimens, some patients may still develop joint disease. 3,4
HA shares similar histopathological features with invasive rheumatology arthritis 5 ; for example, synovial hyperplasia and neoangiogenesis. Intraarticular (IA) injections have been used routinely in the management of osteoarthritis (OA) and rheumatoid arthritis (RA), with potential benefits of increased bioavailability of therapeutic agents at the affected site, fewer potential side effects, and lower overall cost. 6 Gene delivery to joints by IA administration has been well documented in the management of RA and OA from preclinical studies to several ongoing clinical trials (reviewed 7 ). For example, gene therapy for cartilage preservation in OA has used both viral gene therapy and a nonviral platform. 8
In a previous study in FIX knockout (FIX−/−) mice, 9 we found that direct injection of clotting factor IX within the joint space protected against the development of synovitis. Furthermore, our study established that expression of FIX following adeno-associated virus (AAV) gene therapy in the joint may protect from hemophilic bleeding-induced joint pathology.
Hemophilia A is the most frequent and severe life-long bleeding disorder. It is caused by an inherited deficiency of FVIII, 10 accounting for 80% of hemophilia. Finding a potentially novel approach for protection against bleeding-induced joint disease in hemophilia A is clinically significant. In this report, we first investigated whether IA delivery of recombinant human (rh)FVIII could protect from bleeding-induced joint damage. Second, because there is more inhibitor antibody formation in hemophilia A patients compared with hemophilia B, we studied whether repeated IA FVIII carried the risk of developing anti-FVIII inhibitor antibodies.
Great success has been achieved by AAV-mediated gene therapy for both hemophilia A 11,12 and B 13 –15 patients in multiple ongoing clinical trials. Nevertheless, this therapy is currently restricted to patients who are negative for FVIII or FIX inhibitors, and negative for preexisting anti-AAV capsid-neutralizing antibodies (NAbs). To assess the feasibility of future local gene therapy by IA administration to protect against bleeding-associated joint disease in hemophilia patients, we compared anti-AAV IgG levels in synovial fluid and plasma from patients with HA. Our results showed that: (1) IA rhFVIII administration provided protection against bleeding-induced joint damage, even in the presence of an inhibitor antibody; (2) IA rhFVIII delivery had a lower risk of inhibitor formation in comparison to intravenous (IV) administration; and (3) anti-AAV IgG in synovial fluid was lower or similar to their circulating counterparts in plasma for most samples.
Materials and Methods
Animal care and study
FVIII knockout (FVIII−/−) mice with targeted destruction of exon 16 of the FVIIII gene were generously donated by Dr. H.H. Kazazian, Jr. (University of Pennsylvania, Philadelphia, PA) 16 and bred in-house. The animal protocols were approved by the UNC-Chapel Hill Institutional Animal Care and Use Committee. Hemarthrosis induction was performed as described previously. 9 Under continuous isoflurane inhalation, blood samples were collected from the retroorbital plexus into 1:9 parts 3.2% sodium citrate and stored at −80°C. Knee joints were collected by sectioning the femur and tibia 1 cm from the joint. The joints were fixed and decalcified using routine histological procedures.
IA and IV rhFVIII administration
Hemarthrosis was induced in wild-type and FVIII−/− mice. Within 15 min, FVIII−/− mice received IV rhFVIII at 100, 25, or 5 IU/kg. For IA administration, FVIII−/− mice received rhFVIII in a volume of 5 μL through a 30.5-gauge needle inserted into the left hind limb knee joint. The injection, per se, caused massive hemarthrosis in hemophilia mice. 17 –20 Two weeks after injury, treated knee joints were collected for histological examination (≥5 animals in each treatment group).
Histological grading
Hemophilic synovitis in injured and uninjured joints was graded according to a validated system. 21 Total synovitis scores from each joint were averaged. Images were captured with a DMX-1200 color camera using Act-1 software (Nikon, Tokyo, Japan).
FVIII activity, anti-hFVIII inhibitor assay, and anti-hFVIII IgG subclass measurement
Human FVIII activity was measured based on the one-stage FVIII activity assay (aPTT). rhFVIII (Advate®; Baxter, Deerfield, IL), diluted with pooled FVIII-deficient mouse plasma, was used to prepare the standard curve. The anti-human FVIII inhibitory antibody titer was measured by the Bethesda assay as described previously 22,23 using a Start 4 Coagulation Analyzer (Diagnostica Stago, Asnières, France).
For FVIII recovery (Table 1) from synovial fluid, due to the technical issues of using an aPTT assay, FVIII Enzyme-Linked Immunosorbent Assay (ELISA) Kits were used (Affinity Biologicals, Ancaster, Ontario, Canada). Anti-hFVIII IgG1 and IgG2a in synovial fluid were measured by ELISA, as previously described. 24 Synovial fluid/lavage was collected as previously described 9 by washing out the synovial fluid twice with 25 μL normal saline.
Factor VIII recovery in circulation and synovial lavage after intraarticular and intravenous administration of recombinant human factor VIII
For “FVIII recovery in circulation,” FVIII−/− mice were given 100 IU/kg rhFVIII by IV or IA injection (n = 7–8/time point/group). Citrated plasma was collected at 1, 4, 12, 24, and 48 h, FVIII activity was measured by FVIII-based aPTT clotting assay. For “FVIII recovery in synovial lavage,” a different pilot of FVIII−/− mice were given 100 IU/kg rhFVIII by IV or IA injection (N = 4–5/time point/group). Synovial lavage was collected and the samples are detected through hFVIII-specific ELISA, reported as %. Results are reported as percentages ± SD.
ELISA, enzyme-linked immunosorbent assay; IA, intraarticular; IV, intravenous by tail vein; rhFVIII, recombinant human factor VIII; SD, standard deviation; UD, undetectable.
Patient study
Paired synovial fluid and plasma samples were collected from 12 hemophilia patients with established HA who required synovial fluid aspiration before synovectomy. The study was performed in the Clinical Medical College, Yangzhou University, China. Approval was obtained from the Ethics Review Board.
AAV vectors
We utilized most of the available AAV serotypes (1, 2, 2.5, 3, 4, 5, 6, 7, 8, and 9) plus AAV843, a novel AAV2 variant from our laboratory that was developed by DNA shuffling with high liver tropism. 25 All vectors expressing the green fluorescent protein were driven by the cytomegalovirus promoter and manufactured at the Virus Vector Core Facility at the University of North Carolina (Chapel Hill, NC). AAV843 was prepared in-house. All vectors were produced using a triple transfection protocol by the transient transfection of HEK293 cells, and were purified from clarified cell lysates by ion exchange chromatography as described by Grieger et al. 26 Titers were determined by the quantitative polymerase chain reaction.
Anti-AAV IgG ELISA
Plasma samples were assayed by a modified binding ELISA 27,28 to determine the levels of total IgG against each AAV serotype. Briefly, 96-well plates were coated with 1 × 1010 particles/mL of AAV1–AAV9 capsids in carbonate coating buffer (antigen-positive [ag+]), or carbonate coating buffer only (antigen-negative [ag−]), for each sample. Following incubation overnight at 4°C, the plates were washed with phosphate-buffered saline (PBS) containing 0.1% Tween-20 (PBS-T; pH 7.4) and blocked for 1 h with blocking buffer, PBS-T, and 5% dry milk. Twofold serial dilutions, starting from 1:20 of plasma samples in blocking buffer, were added to the plates and incubated at room temperature for 1 h. The plates were washed with PBS-T and then incubated with horseradish peroxidase-conjugated anti-human IgG (Sigma-Aldrich, St Louis, MO) for 1 h at room temperature. After washing with PBS-T, the plates were developed with 3,3′,5,5′-tetramethylbenzidine (Sigma-Aldrich) at room temperature for 5 min. The reaction was stopped by adding 1 M sulfuric acid. The absorbance was read at 450 nm on a microplate reader. Total anti-AAV-IgG levels are expressed as an ELISA titer based on the following calculation: (OD450-ag+ − OD450-ag−)/OD450-ag−. Values ≥2 were considered antibody positive.
NAb assay against AAV843
To correlate anti-AAV IgG and NAb levels, a NAb assay using the hepatocyte-derived Huh-7 cell line was performed on AAV843 in vitro according to a published method. 29 Briefly, Huh7 cells were seeded in a 48-well plate at 1 × 105 cells/well, then cultured with 1 × 108 particles of AAV843/luciferase that were preincubated with a serial dilution of samples for 2 h at 4°C. Twofold dilutions, starting from 1:1, were used to determine the actual NAb titer. Luciferase activity in the cell lysate was measured with a Wallac-1420 Victor 2 automated plate reader (PerkinElmer, Waltham, MA) 48 h post-AAV transduction. NAb titers were defined as the highest dilution of the samples that reduced luciferase activity by 50% in comparison to that in cells transduced with AAV843/luciferase vectors preincubated with PBS.
Statistical analyses
Quantitative data are presented as mean ± standard deviation. The two-tailed unpaired Student's t-test was performed to compare two groups. The chi-square test was used for comparing survival percentages. p-Values of less than 0.05 were considered statistically significant.
Results
IA delivery of rhFVIII provided better protection from bleeding-induced synovitis
We first extended our previous finding of IA FIX in FIX−/− mice into FVIII−/− mice. rhFVIII was given to FVIII−/− mice from 5 to 100 IU/kg, either by IA or IV injection. As shown in Fig. 1, IA rhFVIII afforded better protection against blood-induced synovitis in comparison to IV administration. The protection achieved by 25 IU/kg IA was superior to that in mice treated with 100 IU/kg IV rhFVIII (synovitis scores 0.7 ± 0.2 vs. 2.5 ± 1.7, respectively). The protection achieved by 100 IU/kg IA (synovitis score of 0.25 ± 0.31) was similar to that in wild-type mice subjected to hemarthrosis induction (synovitis score of 0.27 ± 0.24). In addition, IA rhFVIII delivery did not increase circulating FVIII activity; FVIII activity around or less than 1% from 4 to 48 h was identified. We also investigated the kinetics of FVIII concentration within the joint space after IA and IV delivery. While low levels of FVIII can only be detected at 1 and 4 h after IV injection, strikingly higher-than-normal plasma levels were detected up to 48 h after IA delivery (Table 1).

IA delivery of clotting FVIII contributes to protection from synovitis in comparison to systemic administration of FVIII.
IA rhFVIII provided protection from bleeding-induced synovitis in the presence of a preexisting FVIII inhibitor
Clinically, patients with a FVIII inhibitor suffer from more serious bleeding following trauma. After successful induction of an anti-FVIII inhibitor in FVIII−/− mice (Fig. 2A), mice were randomly divided into three groups (FVIII inhibitor titers are represented by the averages and median values as shown in Fig. 2B). Hemarthrosis was induced in the presence of IV rhFVIII (100 IU/kg) or an IA injection of 25 IU/kg. In the presence of the FVIII inhibitor, survival following needle injury was 46% in mice treated with IV rhFVIII. However, 100% of mice treated with IA rhFVIII survived the needle puncture (Table 2). For joint protection, in the presence of the FVIII inhibitor, a single induction of hemarthrosis led to a synovitis score of 6.8 ± 0.9 two weeks posthemarthrosis induction. As expected, IV FVIII treatment did not provide protection in surviving mice in the presence of the FVIII inhibitor (score of 6.3 ± 1.0). Interestingly, 25 IU/kg IA rhFVIII provided significant protection with the mean synovitis score 1.7 ± 0.7 (Fig. 2B).
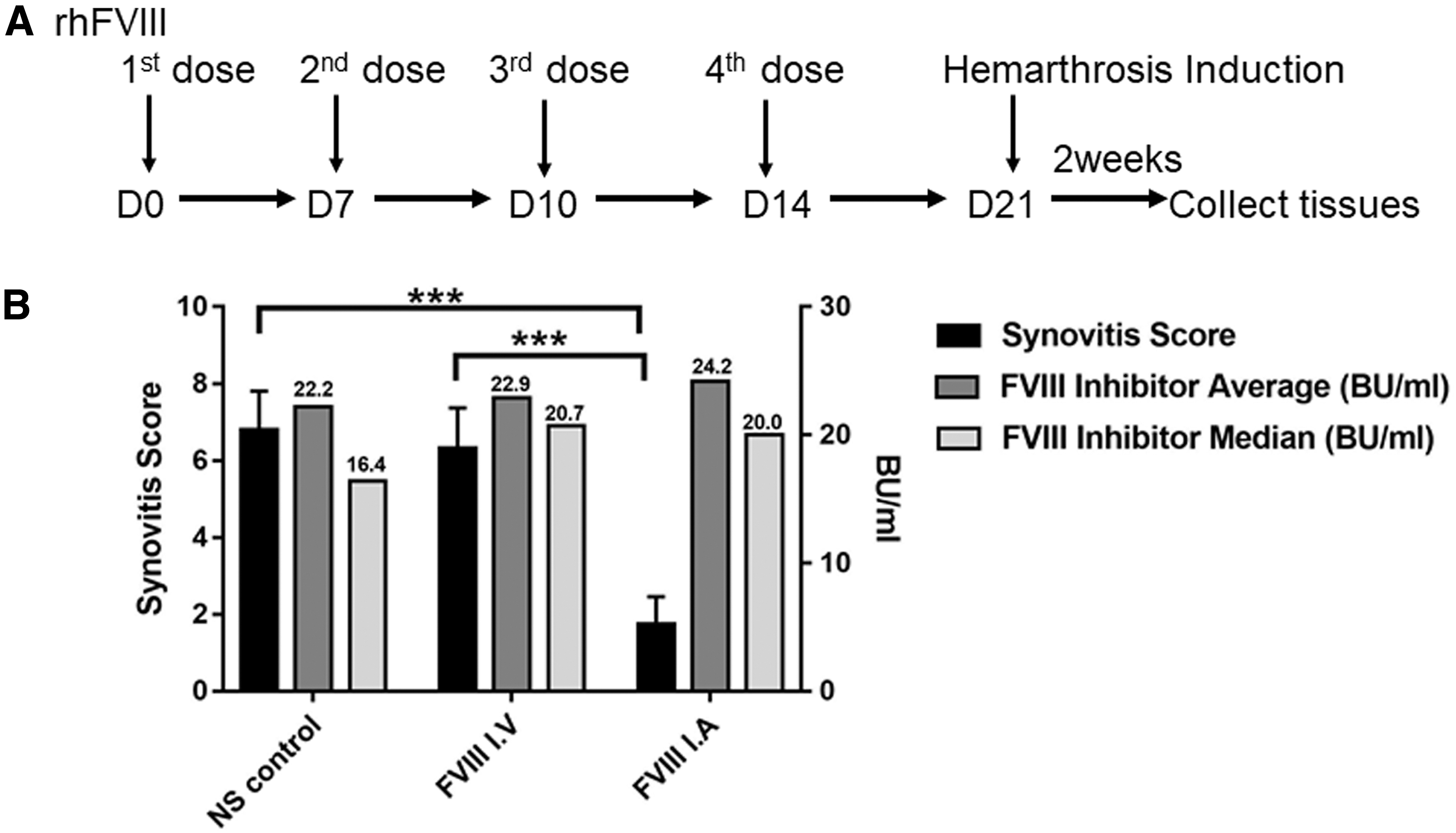
IA delivery of clotting FVIII contributes to protection from synovitis in the presence of an anti-FVIII antibody.
Survival after hemarthrosis induction in the presence of a factor VIII inhibitor
To generate the FVIII inhibitor, FVIII−/− mice received 100 IU/kg of rhFVIII at days 0, 7, 10, and 14 (Fig. 2A). At day 21, hemarthrosis was induced and the survival of mice was monitored for 2 weeks. The chi-square test was used to calculate significant differences in the survival percentages.
IA rhFVIII did not increase the risk of FVIII inhibitor development
Hemophilia A mice are susceptible to inhibitor formation after exposure to rhFVIII. 30 Next, to see if the delivery of rhFVIII carried an increased risk to develop an anti-FVIII inhibitor, FVIII−/− mice were treated IA or IV for 3 weeks with 100 IU/kg/week rhFVIII (Fig. 3A). Four weeks after the first IV or IA dose, FVIII inhibitor formation was monitored (Fig. 3B). All mice treated with IV rhFVIII developed an anti-FVIII inhibitor (mean 8.06 Bethesda units [BU]/mL, x 2 = 18.0, p < 0.01 vs. control), which was consistent with a previous report. 31 Interestingly, only 50% of mice developed the anti-FVIII inhibitor by IA delivery, and at a very low titer (mean 0.6 BU/mL, median 0.5 BU/mL). In this study, 0.4 BU/mL was used as the cutoff value to report a positive inhibitor.
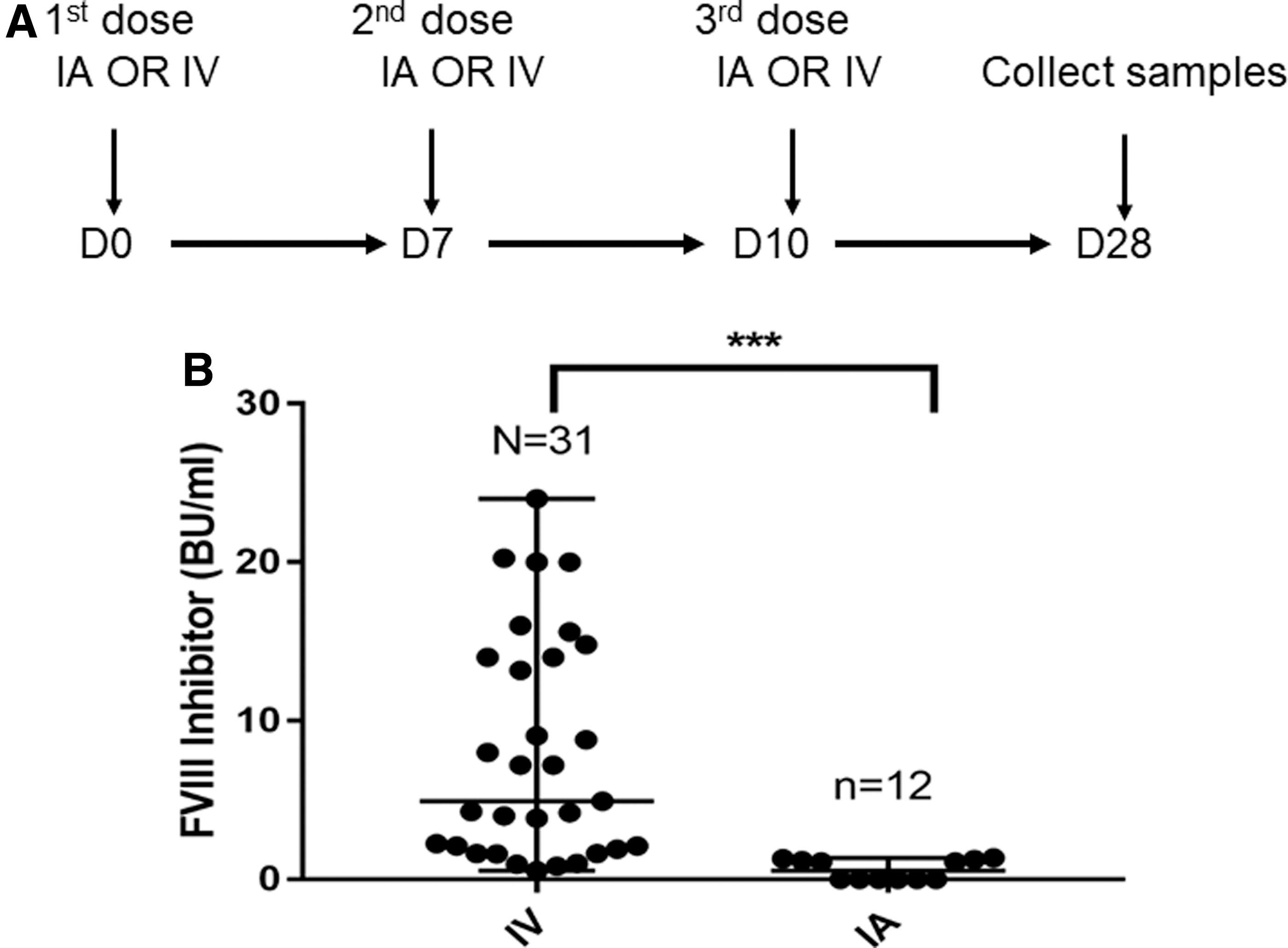
Comparison of anti-clotting FVIII inhibitor formation after IA or IV administration of rhFVIII.
Minimal/no IgG subclass in synovial fluid in mice with high circulating antibody
To investigate whether FVIII inhibitor and anti-FVIII immunoglobulin correlate in circulation with that in synovial fluid, in a separate group of FVIII−/− mice with FVIII inhibitor development after IV hFVIII treatment, both plasma and synovial fluid were collected. As high titer inhibitor antibodies with a range of 61 to higher than 275 BU/mL in the circulation (Table 3), anti-FVIII IgG was predominately IgG1, with low levels of IgG2a occasionally detected. The level of IgG1 (range from 21 to 406 μg/mL) showed a good correlation to the titer of anti-FVIII detected by Bethesda assay. The pattern of IgG subclass antibody responses associated with inhibitor antibody formation in the circulation in this report is consistent with Th2 or mixed Th1/Th2 responses, as reported in our laboratory. 24 In contrast, in synovial lavage, FVIII inhibitor was undetectable by Bethesda assay. Besides the low/no inhibitor in synovial fluid per se, technical issues also affected this result because lavage collection requires washing out the joint space. This led to a diluted synovial fluid. Nevertheless, the level of IgGs in synovial fluid was very low, with IgG1 ranging from undetectable to the highest value of 1.1 μg/mL and no IgG2a detected.
Factor VIII inhibitor and anti-factor VIII IgG subclasses in circulation and synovial fluid
FVIII−/− mice (Fig. 3) were given other two doses of IV 100 IU/kg rhFVIII. Blood and synovial lavage were collected 8 weeks since the first rhFVIII dosing. Anti-FVIII inhibitor, in BU/mL, was measured by Bethesda assay. Anti-hFVIII IgG1, IgG2a (μg/mL), from synovial fluid were measured by ELISA.
BU, Bethesda units.
Overall, the in vivo findings from hemophilia A mice indicated that direct IA rhFVIII provided protection against bleeding-induced joint damage, even in the presence of an inhibitor antibody. IA rhFVIII delivery carried a lower chance for FVIII inhibitor formation compared with IV delivery. Thus, further studies examining local FVIII expression for managing HA are warranted.
Prevalence of anti-AAV capsid antibodies in matched plasma and synovial fluid samples in hemophilia patients
Preexisting NAbs are a barrier for AAV-mediated targeted gene therapy. To investigate whether synovial fluid contained anti-AAV capsid antibodies, and how the level compared with the circulating value, matched samples of plasma and synovial fluid were collected from 12 patients with established HA. A binding ELISA was used to determine the levels of total IgG against each AAV serotype. As displayed in Tables 4 and 5, there were two tendencies, although there were no significant differences. Specifically, anti-AAV total IgG levels were lowest for AAV4 and AAV5, both in plasma and synovial fluid, with all tested samples at the lowest dilution of 1:20. Anti-AAV1 and anti-AAV2 were also generally low, with only a few samples higher than 1:20. Furthermore, anti-AAV IgG in synovial fluid for most of the samples was lower or similar to their circulating counterparts in plasma.
Anti-adeno-associated virus-neutralizing antibody in the plasma and synovial fluid in hemophilia patients
Samples with higher IgG against each AAV serotype.
AAV, adeno-associated virus; NAb, neutralizing antibody; SF, synovial fluid.
Summary of anti-adeno-associated virus-neutralizing antibody in the plasma and synovial fluid in hemophilia patients
Anti-IgGs against each AAV serotype (AAV1, AAV2, AAV2.5, AAV3, AAV4, AAV5, AAV6, AAV7, AAV8, AAV9, and AAV843) were measured by a modified binding ELISA method. To correlate anti-AAV IgG and Nab levels, a Nab assay was performed on AAV843.
We noticed that some samples (1, 2, and 7 in Table 4 far left column) contained relatively higher IgG against each AAV serotype. When the OD575 (an index for hemoglobin after hemolysis) in synovial fluid was measured, the higher OD values indicated that hemarthrosis events occurred in patients, resulting in IgG deposition in the joint space.
The NAb assay, using a hepatocyte-derived cell line (Huh-7), was employed for patient screening to compare the anti-IgG-binding ELISA and NAb results side by side. For this purpose, AAV843 was used. As shown in Table 4 (far right columns), a positive correlation between these two assays existed. Given the convenience of handling large samples with the binding ELISA, whether it would be a suitable screening assay before the NAb assay warrants further investigation, as recently reported. 32
Discussion
In this study, we found that, in a hemophilia A mouse model, IA rhFVIII administration provided protection against bleeding-induced joint damage, even in the presence of an inhibitor antibody. Furthermore, IA rhFVIII delivery resulted in a lower risk of inhibitor formation in comparison to IV administration. In hemophilia patients, we assessed almost all available AAV serotypes (AAV1–AAV9) and documented that anti-AAV total IgG levels were lowest for AAV4 and AAV5, both in plasma and synovial fluid, and the titers in synovial fluid were similar or lower than those in plasma. To our knowledge, this is the first report to compare anti-AAV IgGs in synovial fluid to circulating levels in hemophilia patients. In fact, there are no studies reporting anti-AAV IgG for most of the available AAV serotypes.
Consistent with our previous finding that delivering FIX within the joint space protected against the development of synovitis, we now demonstrated that IA rhFVIII administration provided better protection against bleeding-induced joint damage, even in the presence of an inhibitor antibody.
As AAV-mediated gene therapy for hemophilia is progressing into reality as a cure, some safety concerns and risks still remain, for example, inhibitors to FVIII/FIX from introduction of the transgene and transgene loss from cellular immune response to vector capsid. 33 Indeed, the development of NAbs, or inhibitors, against exogenously administered clotting factors is the most significant therapeutic complication of hemophilia A, affecting 30–40% of previously untreated patients given FVIII. 34 It is interesting to see IA rhFVIII administration result in a lower risk of FVIII inhibitor development. There are two possible explanations for this outcome: (1) low leakage, if any, of rhFVIII into the circulation after IA delivery may be insufficient to evoke the immune system toward FVIII inhibitor formation; and (2) local IA administration of rhFVIII may result in the rapid initiation of the coagulation pathway and minimize its propagation, which is involved in the pathogenicity of RA. 35 Likewise, these assumptions may also apply to mice with an anticlotting inhibitor. High doses of rhFVIII may override the inhibitor in the joint space. 36 Indeed, mice with high circulating FVIII inhibitor showed no FVIII inhibitor by Bethesda assay, despite the technical limitation to be taken into account. When anti-FVIII IgG subclasses were measured in synovial fluid, minimal to no IgG subclass content in the synovial fluid existed, although the possibility due to technical issues should not be excluded. We do not know yet whether this phenomenon is from poor circulation into the joint space due to the blood/joint barrier 37,38 or whether the joint space is an immunosuppressed site. In either scenario, the feasibility of local gene therapy by expressing clotting factors in the joint for the management of hemophilia joint disease has the hope of escaping recognition by the systemic immune system and warrants further investigation.
Vector-mediated gene therapy has been used for managing RA and OA. 39,40 In hemophilia, local expression of FIX by AAV in the hemophilia B mouse model 9 and FVIII by transduced mesenchymal stromal cells in the hemophilia A mouse model, 41 nonhuman primates, 42 and rabbits, 43 shows that IA injections are a promising therapeutic modality for treating HA. 44
Among the viral vectors tested, due to the wide range of tropism to multiple organs and the profiles of safety, efficacy, and persistence, AAV-mediated gene transfer has been used in the majority of ongoing clinical studies for patients with hemophilia. 11,13,45 –48 Thus, AAV is one of the most attractive vectors for gene therapy. However, preexisting NAbs are barriers for AAV-mediated gene therapy to transduce host cells, and the prevalence of NAbs against the vector imposes a major challenge for AAV gene therapy. The prevalence of NAbs against AAV has been well studied and documented in the gene therapy field, including reports from newborns, children, adolescents, 49 and a large population survey by international collaborators. 50 However, only a few reports 32,51,52 consider the hemophilia population specifically.
The prevalence of anti-AAV antibodies in synovial fluid of hemophilia patients has not been reported previously. Synovial fluid is produced as an ultrafiltrate of blood plasma, in which the volume and content may change in response to physiological events such as trauma, inflammation, and bacterial, fungal, or viral penetrance. 53 Differences of particular components in synovial fluid in comparison to circulating levels have been reported; for example, higher levels of glypican-354 and malondialdehyde 55 in synovial fluid in OA patients, and higher concentrations of proinflammatory cytokines in synovial fluid in RA patients. 56 These were attributed to the pathogenicity of the corresponding diseases.
Regarding NAbs against AAV in RA patients, similar to the current report, the prevalence of an NAb titer against AAV2, AAV5, AAV6, and AAV8 in the plasma, and matched synovial fluid, have been studied. The findings suggested that the titer in synovial fluid was lower than in plasma samples, indicating a difference in distribution of NAbs to AAV depending on the body fluid compartment.
57
In another study, 21 patients with joint diseases (19 samples side by side) were studied for the neutralizing activity of synovial fluid and plasma on AAV gene transfer to chondrocytes. The results showed that most synovial fluids displayed lower (up to 33-fold) neutralizing activity.
58
Our finding, in which anti-AAV IgG in hemophiliac synovial fluid in most patients displayed similar or lower titers compared with the circulating level, is partially consistent with those findings. This suggests the feasibility and potential translational significance of employing AAV-mediated local gene therapy for managing HA. It should be noted that the synovial fluid collected in this report was from patients with preexisting HA, with an inflamed environment after multiple hemarthrosis breakthroughs, as we found that some samples displayed higher IgG against almost all AAV serotypes. This might complicate antibody production under normal conditions. Thus, these patients may be more willing to undergo local gene therapy for the management of deteriorating disease. Nevertheless, anti-AAV4 and AAV5 IgG remained the lowest titers in the synovial fluid in human patients. Given that the efficacy and safety of AAV5 for arthritis has been investigated in mouse,
59,60
rat,
61
horse,
62
monkey,
63
and proposed clinical trials (
In summary, direct supplementation of FVIII by IA delivery in the joint space provided protection against bleeding-induced joint damage, even in the presence of inhibitor antibodies. IA rhFVIII delivery was associated with a lower risk of inhibitor formation, even in joints with preexisting damage. Furthermore, in hemophilia patients, this is the first report that the AAV NAb titer in synovial fluid is similar or lower than that in plasma, which suggests the feasibility of local expression of FVIII by gene therapy for the management of HA.
Footnotes
Acknowledgments
The authors thank Editage (
Author Disclosure
P.E.M., during the conduct of the animal studies, received research support through the University of North Carolina from Asklepios BioPharmaceutical and Novo Nordisk. He has received research support in the past from Baxter Healthcare, Novo Nordisk, Pfizer, and Prolor. He holds patents licensed to Asklepios, for which he receives royalties. He has received payment for consultation, services, and speaking for Asklepios, Chatham LLC, Baxter Healthcare, and Pfizer and has additionally consulted for Bayer, Novo Nordisk, and Biogen. The other authors declare no conflict of interest relevant to the study.
Funding Information
The work was supported, in part, by a grant from the Novo Nordisk Hemophilia Research Fund China, an unrestricted grant from Novo Nordisk, Fundamental Research Funds for the Central Universities, and a grant from the National Natural Science Foundation of China (#81970171). Junjiang Sun received a research grant from Asklepios BioPharmaceutical during the preparation of the article.