
Abstract
For more than 10 years, gene therapy for neurological diseases has experienced intensive research growth and more recently therapeutic interventions for multiple indications. Beneficial results in several phase 1/2 clinical studies, together with improved vector technology have advanced gene therapy for the central nervous system (CNS) in a new era of development. Although most initial strategies have focused on orphan genetic diseases, such as lysosomal storage diseases, more complex and widespread conditions like Alzheimer's disease, Parkinson's disease, epilepsy, or chronic pain are increasingly targeted for gene therapy. Increasing numbers of applications and patients to be treated will require improvement and simplification of gene therapy protocols to make them accessible to the largest number of affected people. Although vectors and manufacturing are a major field of academic research and industrial development, there is a growing need to improve, standardize, and simplify delivery methods. Delivery is the major issue for CNS therapies in general, and particularly for gene therapy. The blood–brain barrier restricts the passage of vectors; strategies to bypass this obstacle are a central focus of research. In this study, we present the different ways that can be used to deliver gene therapy products to the CNS. We focus on results obtained in large animals that have allowed the transfer of protocols to human patients and have resulted in the generation of clinical data. We discuss the different routes of administration, their advantages, and their limitations. We describe techniques, equipment, and protocols and how they should be selected for safe delivery and improved efficiency for the next generation of gene therapy trials for CNS diseases.
Introduction
The central nervous system (CNS) is protected by a unique microvasculature, the blood–brain barrier (BBB), composed of endothelial cells connected by tight junctions and adherent processes. The BBB controls brain homeostasis and ion and molecule movements thus protecting the CNS against potential intruders. The restrictive nature of the BBB provides an obstacle for drug delivery to the CNS, and major efforts have been made to generate methods to modulate or bypass the BBB for delivery of therapeutics. Contrarily, some pathologies of the CNS including stroke, multiple sclerosis, brain traumas and neurodegenerative disorders, alter the BBB, causing it to become more permeable, allowing the entry of molecules that can induce inflammatory responses and lead to neuronal damage. 1,2
Gene therapy has been applied to several CNS diseases, including neurodegenerative 3 and neurodevelopmental disorders, 4,5 and also for diverse conditions such as epilepsy, 6 glioblastoma, 7 and pain. 8 Increasingly, gene therapy products can be tailored to counter the pathophysiological mechanisms of particular disease mechanism, including the use of gene replacement, 9 –13 gene silencing, 14 transplicing, 15 modulation of cellular pathways to improve phenotype, 16 –19 or expression of suicide gene. 20
Gene therapy products can be delivered by various routes of administration, using either ex vivo or in vivo strategies. Ex vivo gene therapy involves autologous transplantation of hematopoietic stem cells corrected by genetic modification of lentivirus (hematopoietic stem cell-gene therapy [HSC-GT]) outside the body and subsequent transplantation of the cells back into the patient. Efficacy for HSC-GT has been shown in clinical trials for leukodystrophies (adrenoleukodystrophy [ALD], metachromatic leukodystrophy [MLD]). 21,22 Therapeutic action involves either production of the therapeutic protein by donor-derived cells that can migrate into the CNS (permanent source of the missing enzyme), and/or modulation of the immune environment (replacement of microglial cells and/or perivascular macrophages). In vivo gene therapy requires direct introduction of the vector (carrying the therapeutic gene) into the patient (Fig. 1). Intravenous (IV) administration is a common route of administration for in vivo gene therapy but for CNS diseases the limited capacity of gene delivery systems to cross the BBB remains a significant obstacle. Strategies such as disruption of the BBB integrity (by osmotic or biochemical means) or improvement of viral vector capsids continue to be developed to enhance peripheral administration. Direct delivery into the parenchyma of the brain or the cerebrospinal fluid (CSF) bypasses the BBB and permits more targeted gene delivery. After intrathecal (IT) or intracerebroventricular (ICV) administration, the therapeutic vector enters the CSF and is delivered throughout the CNS (at least to tissue adjacent to CSF spaces). After intraparenchymal administration, the therapeutic vector enters the brain parenchyma and is delivered locally into brain cells. The diffusion of the therapeutic product is limited around the injection site; however, secretion uptake may improve diffusion, notably the case for most lysosomal storage disease enzymes.

The vector of choice for in vivo CNS delivery is the adeno-associated viral (AAV) vector. Recombinant AAVs have been widely used for CNS gene therapy, demonstrating safety, stable, and long-term expression and some degree of neuronal tropism relevant for many therapeutic applications. A large body of preclinical results have been obtained, particularly in large animals like dogs, cats, and nonhuman primates (NHPs) that have demonstrated feasibility for clinical use. 23
Wild-type AAVs are nonenveloped parvovirus, which are characterized by an icosahedral capsid and a 4.7 kb single-stranded DNA genome. To complete a replication cycle, AAVs require coinfection by a helper virus like adenovirus or herpes virus. AAVs infect humans and other species including the NHP. 24 Natural infection with AAV is not known to lead to disease, although there is controversy concerning hepatocellular carcinoma. 25,26 The minimal sequence needed to generate recombinant AAVs is restricted to the 145 bp within the inverted terminal repeats (ITRs) flanking the transgene. 27 The overall capacity of AAV to package an ITR-flanked genome productively is the approximate size of the wild-type AAV genome (i.e., 4.7 kb).
Overall AAV vectors have been used and have proven their safety and low immunogenicity tolerance in >200 human studies.
28
Efficiency of an AAV administration is determined mainly by the capsid that directs the tropism of the virion, but can be impacted by the route of administration.
29
It is also well established that the specificity of transgene expression is dependent on both the capsid and the regulatory elements present in the vector.
30
There are a large number of AAV serotypes based on capsid structure.
31
AAV2, the first AAV serotype to be used as a replication-defective vector, has been the most extensively characterized. Other AAV serotypes developed later as vectors use a cross-packaging system, in which genomes flanked by AAV2 ITRs are packaged in other AAV capsids. These serotypes have a wide variety of tissue and cell tropism.
32
For gene transfer to the CNS the most frequently used capsids have been AAV1,
33
AAV2,
34
–36
AAV5,
37
AAV9,
12
and AAVrh.10.
9
AAV9 was shown to naturally cross the BBB but limited expression of therapeutic genes in the CNS after a single IV injection of vector.
38,39
Of importance, the first clinical report of gene-replacement therapy for spinal muscular atrophy (SMA) type I has demonstrated the safety and efficacy of this approach.
12
However, the efficacy of brain transduction efficacy may vary with the patient age at treatment. There are ongoing efforts to engineer capsids with improved capacity to cross the BBB. AAV variants
40,41
such as
Lentiviral vectors (LV) are members of the Retroviridae family, and based either on human immunodeficiency virus (HIV), nonprimate primates (simian immunodeficiency virus), or others such as equine infectious anemia virus (EIAV). 44 The viral genome contains two long terminal repeats (LTR), with elements required for gene expression, reverse transcription, and integration into host chromosome. 45 Different pseudo types of LV with different envelopes allowing for different viral tropism have been developed. The most frequently used is the vesicular stomatitis virus glycoprotein (VSV-G), which has a broad tropism in vitro and neuronal and glial tropism in vivo. 46,47 Lentiviruses are able to penetrate the intact nuclear membrane through nuclear pores, do not require cell division, and can efficiently infect quiescent cells. 48,49 This ability to transduce dividing and nondividing cells, long-term stable expression through transgene integration into the chromosomes of host cells, and their large cloning capacity make LVs desirable vectors for gene therapy. 50 They also have a cloning capacity of 9.7 kb.
LVs are particularly useful for ex vivo gene therapy applications. Hematopoietic stem cells (HSCs) can be stably transduced using LVs; allowing for stable, indefinitely persisting expression within the host cell, despite repeated cell division. This characteristic has been widely applied to CNS lysosomal storage diseases or ALD. 51,52 Random integration in the genome of host cells is associated with a potential genotoxicity risk, as previously observed with retroviruses. 53,54 However, long-term follow-up of gene therapy trials has not identified adverse events associated with insertional mutagenesis. 55 –57 In vivo use of lentivectors for CNS applications has been more limited. Because of their capacity to transduce neurons, they have been tested for the treatment of Alzheimer's disease (AD) and Parkinson's disease (PD). 58 –60 For this review, we focused more on AAV because they have been more widely used in CNS targeting for large animals and human clinical trials.
Evaluation of Administration Routes in Preclinical Studies
Translation to clinical application after proof-of-concept in mouse models of the disease most often requires efficacy and tolerance studies in large animals.
Many species have been used 61 for preclinical development. Affinity for the different types of brain cells in large animal species remains a major issue. The choice of the large animal models to be used is mainly based on the use of a large animal model of the disease when available 62 –65 otherwise on anatomical aspects to mimic the best situation to be reproduced for future clinical trials.
When the gene therapy product is administered by injection in the blood stream or the CSF, any suitable species of large animal can be used. However, when delivery is based on direct intraparenchymal (IP) injection into the brain for characterizing biodistribution, toxicity, diffusion, and affinity with different types of brain cells, pigs, sheep, and NHPs are preferred species for modeling trajectories and efficient targeting. In all cases it must be emphasized that the use of large animals is strictly limited for ethical reasons and should be performed in good laboratory practice (GLP) or GLP-like conditions to be usable for regulatory documents.
Intraparenchymal delivery
The principle studies of IP gene delivery in large animals are given in Table 1. Direct IP injection—either direct perfusion or convection enhanced delivery (CED)—allows targeted delivery in CNS regions while bypassing the BBB. However, IP injections remain more complex to perform than ICV or IT techniques for several reasons. 66 The choice of the target region is always a challenging balance between efficacy and safety. Therefore, the specific anatomy and pathophysiology of the disease should be considered when choosing target sites. Targeting the white matter in multiple sites may enhance vector spreading. 11 In particular, AAV vectors are readily transported along axons that facilitate the distribution of the therapeutic gene. 67 The spreading and directionality of AAV transport are serotype dependent. 68 AAV2, which has been widely used in IP gene delivery, resulted in anterograde transport 68 of vector particles from basal ganglia to cortex in NHP. 69,70 In contrast, AAV6 is axonally transported exclusively in a retrograde direction, 68 whereas AAV9 shows a bidirectional transport and is dose dependent. 71
Intraparenchymal delivery in large animal models
AAV, Adeno-associated viral; AD, Alzheimer's disease; CNS, central nervous system; ICV, intracerebroventricular; LV, lentiviral vector; MLD, metachromatic leukodystrophy; NHP, nonhuman primate; PBS, phosphate-buffered saline; PD, Parkinson's disease.
Recent studies suggest that AAV5 and AAVrh10 have more global transduction with widespread distribution in the brain 11,72,73 and spinal cord. LVs are able to deliver the therapeutic gene in a restricted area. 74,75
Intracerebrospinal fluid delivery
As an alternative to intraparenchymal delivery and to target larger brain or spinal cord volumes, especially in neurodegenerative diseases involving widespread regions, intra-CSF delivery is an option.
For this purpose, three major routes can be used: ICV delivery into the ventricles, the cisterna magna as widely used in large animal models (Table 1), or by IT delivery into the CSF surrounding the spinal cord (Table 2).
Intracerebroventricular administration in large animal models
CM, cisterna magna; CSF, cerebrospinal fluid; DRG, dorsal root ganglia; IC, intracisternal; MRI, magnetic resonance imaging; mRNA, messenger RNA; shRNA, short hairpin RNA; SMN, survival motoneuron protein; VGC, vector genome copy.
LVs have been used in one approach in adult sheep, but this reported attempt resulted in very limited transduction close to the needle track with up to 2.5 mm rostrocaudal transduction. 76 AAVs lead to greater transduction especially in adults. ICV delivery in young animals differ, providing extensive transduction of motor neurons in some cases. Using scAAV9 in 5-day-old pigs 77 and in 10- to 11-day-old dogs, Katz et al. reported a TPP1 activity increase in CSF a few days after transduction, but then loss of the transgene owing to immune response against the transgene product. 78 AAV9 and AAVrh10 have been predominantly injected with doses ranging from 1012 vg to 5.1013 vg in dogs, NHP, and cat 67,79 –87 mainly in the cisterna magna with either GFP or therapeutic genes (Table 2). Diffuse transgene expression was obtained in the cortex and cerebellum (Table 2). In most studies, efficacy of spinal cord targeting was not analyzed; however, available studies report highly variable results with large motor neuron transduction. 88
As an alternative to ICV delivery or depending on the pathology to improve spinal cord targeting, delivery in the CSF can be achieved through IT injection. Studies have been performed in dogs, 85,89,90 NHP, 13,84,91 pigs, 83,92 and marmosets 93 mainly using AAV9 or AAVrh10 vector in neonates (5 days old) or in adult animals (Table 3). Two major techniques are routinely used for IT delivery, either a single delivery without the use of a catheter, generally performed in the L4/L5 space, or with prior insertion of a catheter to allow single or multiple deliveries. 83,94 IT delivery leads to efficient motor neurons transduction ranging from 10–30% 83 to 80% 13 depending on the study (Table 3), but sparse transduction in the brain (Table 3). Two studies have evaluated placing the animal in the Trendelenburg position with the feet elevated above the level of the head to improve the upward diffusion of the vector. Variable results were reported, one showing no improvement 95 and the other one a slight increase, with up to 55% targeting of cervical motor neurons 13 (Table 3).
Intrathecal administration in large animal models
IV, intravenous.
Even if ICV delivery is designed to target basal ganglia (Fig. 1d), intracisternal delivery to target the cortex (Fig. 1c) and IT delivery for the spinal cord (Fig. 1b), the direct relationship between the site of injection and the efficient delivery to the target has never been proven, and appear to be different between NHP and human in relation to the volume of the respective brains and the distance between CSF pathways and the CNS targets.
In between intraparenchymal and intra-CSF delivery, for intraspinal targets, spinal subpial delivery has been proposed in mice, rats, and pigs. 96,97 Despite the short distances for spinal diseases, the primary issues remain the need for an open microneurosurgical approach after laminectomy (or a laminotomy) and the risk of neurological deficits secondary to spinal cord subpial bleeding.
Intravenous delivery
As an alternative to more invasive injections, IV delivery has recently become an option to target the CNS, especially with the SMA trial. 12 AAV9 and AAVrh10 are once again the major serotypes injected dosing from 1012 vg/kg up to 1014 vg/kg. In neonates (2–7 days old) studies have demonstrated up to 39% transduced motor neurons in cats 77 but other studies were unable to detect the transgene 88 (Table 4). In adults, it differs with mild to no neuronal transduction 81,90 either in spinal cord and brain (Table 4). Transduction was in any case much lower compared with ICV 84 or IT delivery and glial cells were predominantly transduced, 86,92 without clear explanation. In addition, IV delivery led to a significant transduction of peripheral organs (Table 4).
Intravenous administration in large animal models
MN, motoneurons.
Routes of Administration in Clinical Studies
Although IV delivery is readily transferred from animal models to human trial conditions, CSF or brain delivery techniques must be carefully adapted for human conditions (brain anatomy and volumes). ICV, cisternal and IT methods can however all be used in human subjects. Very little intraventricular vector diffusion occurs after cisternal or IT injection; most of the product remains in the spinal compartment or reaches the pericerebral space. Because of the size of the brain and the distance between the ventricles and the cortex, it is impossible to achieve consequent and homogenous diffusion by any CSF route.
Intraparenchymal injection is possible in the human brain, in deep nuclei, or in the white matter (but may need multiple simultaneous injections to obtain sufficient diffusion), but there is no reliable technique for delivering to the spinal cord parenchyma.
The doses of vector delivered depend on the route of administration. Although intraparenchymal delivery requires small amounts of vector ranging from 109 to 2.5.1012 total vg in NHP and human, doses from 1012 to 5.1013 vg are required for ICV or IT delivery. IV delivery dramatically increases the number of particles required, from 5.1012 to 5.1014 vg (1012 to 1014 vg/kg) in NHP and close to 1015 vg in patients in the SMA trial (2.1014/kg) (Tables 1–6).
Clinical trials with Intra parenchymal administration
EIAV, equine infectious anemia virus; WM, white matter.
Local administration of low doses of vector limits biodistribution and the risk of immunogenicity or toxicity owing to AAV capsid or expression of the transgene. The high doses required for intra-CSF and IV administration raise issues of immunogenicity, manufacturability, and final cost.
Translating gene therapy proof of concept in animal models to clinical application in patients requires adapting delivery protocols. Translation may be simple for intra-CSF or IV delivery, based on the weight of the animal or the volume of the brain tissue or of the CSF. Modeling the delivery into the brain parenchyma is more critical for designing a clinical protocol. This should take into consideration the volume of the target region determined by imaging, the sites and the number of injections, the degree of anatomical precision required, the volumes to be injected, and the flow (constant or CED). Translating these parameters from large animal brain to human brain requires specific anatomical adaptations (needle track in particular) and evaluation of feasibility, safety, and efficiency in terms of biodistribution in animal models under conditions as close as possible to the human clinical procedure.
There is no limit for age, and theoretically, it is possible to treat even newborns by all routes of delivery. It is possible to use frameless stereotactic delivery using magnetic or optic neuronavigation. In addition, robotic systems are now available even in the youngest subjects. The youngest child treated by our team with intracerebral delivery (16 targets supra and infratentorial) was 9 months old. 9
Intracerebrospinal fluid delivery
To overcome the inability of the gene therapy vectors to cross the BBB, direct injection within the CNS compartment has been attempted. 98 All trials using these routes of administration are given in Table 5. Three main modalities can be discussed.
Clinical trials with intra cerebrospinal fluid or intravenous administration
SMA, spinal muscular atrophy.
Intrathecal lumbar administration with two potential modalities
Direct unique injection by a lumbar tap or through an intraspinal catheter connected to a subcutaneous reservoir. The use of a single injection by lumbar tapping is a nonsurgical procedure. It could be performed, in a medical environment, with local anesthesia. In difficult cases, the use of fluoroscopy or ultrasonography 99 can facilitate the procedure (or to guide a catheter insertion). The main inconvenience of this technique is the risk of CSF leak in the extradural space at the moment of needle removal and 2 days after the procedure. Consequently, it is impossible to precisely control the quantity of vector administered within the intradural space. The use of atraumatic G22 needle (Sprotte) can minimize this risk. 99
To avoid this major inconvenience, an alternative is to install a subcutaneous reservoir connected to an intraspinal catheter. 99 This procedure must be performed in the operation room, under general anesthesia. Injection must be performed 1 or 2 weeks after the initial surgery and the removal of the system at least 1 week after. This technique guarantees control of the injected volume, but needs two general anesthesia, and increases the risk of infection. The main incertitudes of this technique are determining the exact distribution of the product between the different compartments; intraspinal CSF, intraventricular, and intracranial subarachnoid spaces (Fig. 1). The main disadvantage of the ITL access results from the natural flow of CSF from the intraventricular choroid plexus to the subarachnoid space around the spinal cord and finally to the pericerebral spaces for resorption through the venous system. Reaching the brain target through the CSF stream requires a large dose volume. Other associated strategies can be used to improve the efficacy such as a buffer flush or a Trendelenburg position. Complications owing to the device and its implantation also have to be considered. Meningitis can be a severe infectious complication that needs removal of the system and adapted antibiotics treatment. Other mechanical complication can be encountered such as migration, rupture, or disconnection, kinked or obstructed catheter. A CSF leak around the catheter to the subcutaneous space can lead to an artificial meningocele that can impair the ability to infuse the treatment. To overcome this problem, two other modes of administration have been proposed.
Intracisternal administration 100,101
In most cases, it is possible to inject within the cisterna magna at the level of the craniovertebral junction. Even if it is possible to do it while the patient is awake, general anesthesia will be preferred, especially in the pediatric population. The risk of leakage through this route is very low and in most cases the reservoir is useless.
Intraventricular administration
A third route to the CSF space is to inject directly within the cerebral ventricles. In most cases, it will be carried out in the frontal horn by direct puncture under stereotactic guidance or more frequently now under frameless neuronavigation. In adults, it is easily performed under local anesthesia and light sedation, in the pediatric population general anesthesia is preferable. Installation of an intraventricular catheter connected to a reservoir may be preferred; however, for a single injection, direct injection is safe and efficient. It is also better for controlling the volume of injection and its distribution. However, because of the risk of parenchymal bleeding, most authors prefer the cisternal approach.
Intraparenchymal delivery
Few human trials using the intracerebral route are reported (Table 6), both in adults (Huntington, Parkinson, and Alzheimer diseases) and children (SMA, Canavan, Batten, mucopolysaccharidosis, and MLD). The vast majority of the trials have used AAV vectors (from 107 to 1013 vg) with injections in the deep gray nuclei or in the white matter (only for metabolic diseases in children). Most published trials are phase 1/2 and one is phase 3. Several studies obtained promising results even if partial or preliminary. Of importance, few severe adverse events have been reported.
Technical Aspects: State of the Art
Regarding delivery technique, we focus here on intracerebral delivery, indeed, other routes of delivery have been largely described previously and have not been researched as intensively.
Devices for intraparenchymal delivery of therapeutics agents
Intraparenchymal drug delivery systems offer a practical method for bypassing the BBB to deliver gene therapy. Direct access to parenchyma allows delivery at doses and concentrations that would otherwise correspond to very high levels and volumes systemically. However, this method still has constraints and limitations. For >10 years, considerable research has focused on developing methods to enhance drug delivery, 102 through dedicated intraparenchymal devices.
Principles
Intraparenchymal delivery has two principle challenges: minimize backflow along the injection device and promote optimal drug distribution, 103 often in a spherical tissue volume. The distribution volume depends on infusion flow rate, infusion volume, and number of injection sites and the type of vector that is injected. 104 The occurrence of backflow depends on several variables including cannula radius, infuse flow rate, and tip location. 105 Indeed, many parameters influence the safety and efficiency of infusion: infusion flow rate, cannula size, infusion volume, and drug molecular size/charge. 106 Variations in flow rate impact the location of infusate distribution. Lower infusion rates (<1 μL/min) are associated with distribution localized primarily to the target tissue (they are used for focal injection in specific areas, mainly in gray matter nuclei), whereas higher infusion rates result in increased distribution into the surrounding parenchyma (“overflow”). 103,106 Several techniques have been proposed to increase infusion rates (up to 10 μL/min); among them the use of CED 107 appears to provide the best compromise for extensive diffusion with minimal local damage. They can be used in combination with multiple injections (up to 16) 9 when the whole brain must be treated (lysosomal diseases) (Fig. 2). 11 Increases in infusion rates raise the local pressure around the infusion site and also increases the extent of backflow. Cannula size seems to have no effect on distribution; however, larger cannulas cause more tissue damages and therefore produce decreased resistance pathways along the brain parenchyma–catheter interface that are associated with increased rates of backflow. 106
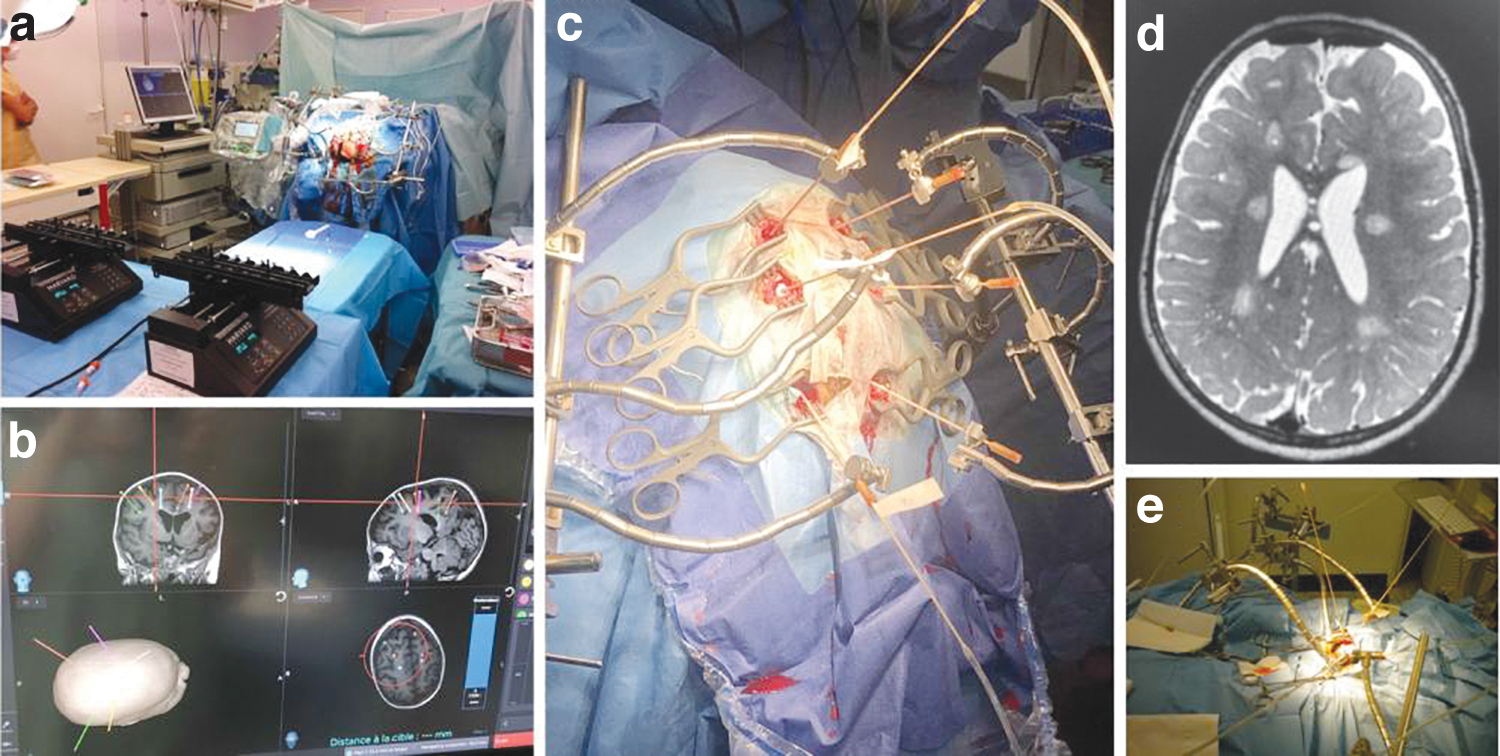
Intracerebral injection in NHP and humans.
Catheters subtypes
Three kind of delivery devices can be distinguished: catheters derived from another use (especially intraventricular devices), “homemade” designed catheters 9,11,102,108 from teams experimenting with preclinical intracerebral drug delivery or for early clinical studies, 9 and more recently commercialized catheter for specific intraparenchymal use (often developed from the homemade devices, and for intracerebral chemotherapy). Principal available devices are described in Table 7.
Devices for intracerebral gene therapy delivery
Ventricular catheters (2–3 mm outer diameter) that have been implanted in clinical trials to treat glioma have failed to distribute effectively and have been linked to poor distributions. 109,110 Microcatheters (<1 mm outer diameter) seem more reliable, and all FDA-approved catheters for CED belong to this category.
Design
Recent catheters have been designed to reach the goals of parenchyma delivery: minimize invasiveness through a minimal diameter tubing (Casanova), optimize infusion parameters to maximize distribution volume, and a reflux inhibiting feature required to halt backflow along the catheter entry track (Fig. 2). 109 All these characteristics are summarized in Table 7. Means to minimize backflow are the following: polymer-impregnated tips, 102,111 stepped-design cannula, 105,109,110 and recessed-design cannula 109,112 (Bristol). Means to enhance delivery are as follows: multiporous cannula, multiport catheter, mobile-tip catheter, and balloon-type cannula. A “valve tip” has been proposed to prevent blockage by occluding the inner bore of the cannula with a stylet during insertion. 103 Another new advance is a multisite delivery catheter with one single tube 113 (cleveland multiport cetheter) that allows multiple targeting points and more homogenous delivery in a three-dimensional array.
Pumps and syringes
To enable injection of small volumes at precise low speeds, specific pumps and syringes must be used. For pumps, most are manufactured for research use (Harvard Apparatus, Holliston, MA), and special authorizations must be obtained for clinical use.
Injection systems: combining precision delivery and limited procedure time.
Classical stereotactic techniques are well adapted for injection in a unique site of brain parenchyma—however, new techniques allowing multiple brain injections of the gene therapy for many indications are needed. Specific three-dimensional magnetic resonnance sequences allow precise targeting in white matter or in deep gray matter nuclei (striatum, thalamus, caudate nucleus, and so on). Preplanning using neuronavigation software (Medtronic® or Brainlab®) facilitates the choice of trajectories, modeling delivery and rehearsing the surgical procedure. Optic or magnetic neuronavigation system with or without robotic tools (Rosa®, Renishaw®, Medtronic, Brainlab) (Fig. 2) allows frameless insertion of multiple cannulas, supra or infratentorially according to the preplanning. Altogether these systems allow the delivery of therapeutic product reproducibly with high precision (∼1 mm). Intraoperative real-time magnetic resonnance imaging (MRI) has also been proposed as an additive tool to verify the position of the cannula and to check the diffusion of the product with simultaneous gadolinium injection, 66,114 although with the risk of long-term toxicity.
Risks Assessment
Linked to the delivery procedure
Risks owing to anesthesia are mainly correlated to the disease itself and related comorbidities. All injections or catheter placement can result in a CNS injury or hemorrhagic complications. Lumbar puncture is at very low risk of complication if carried out at the low lumbar level without spinal cord anomalies such as low tethered cord. Epidural hematoma can occur, especially with repeated punctures. Spinal epidural hematoma can remain asymptomatic but sometimes cause radicular pain and even rare motor impairment or sphincter dysfunction in case of cauda equina syndrome. A motor impairment requires surgical evacuation. Lumbar puncture can cause subarachnoid bleeding leading to radiculitis, pain, and headache. In case of spinal deformity, fluoroscopy or ultrasonography may help to guide the puncture.
Intrathecal catheter placement needs the use of a guide wire to conduct the catheter to the thoracic level or higher and can result in a spinal cord injury and cause motor or sensitive (transient in the vast majority of the cases) dysfunction. The risk of a hemorrhagic complication in the epidural or intradural space is higher in relation to the larger size of the needle.
Intracranial hypotension symptoms can occur secondary to a lumbar puncture and cause severe orthostatic headaches that can be managed with supine position, painkillers, and if needed, blood transfusion.
Intracisternal puncture requires an adequate cisternal space (confirmed by MRI), a motionless situation and an experienced operator. The size of the cisterna magna and the shape of the skull, a Chiari anomaly, or a foramen magnum stenosis increase the risk of neurological complication (Bulbomedullary junction injury responsible for cardiorespiratory arrest).
Intraventricular access is performed through a right frontal trajectory. Bleeding can occur along the trajectory at each level: subcutaneous hematoma or epidural hematoma is rare. Subdural hematoma can occur by direct bleeding or an intracranial hypotension secondary to a CSF loss; intraparenchymal hematoma can be asymptomatic but may, if extended, lead to motor or cognitive impairment. Intraventricular bleeding may be responsible for headaches and sometimes secondary hydrocephalus.
Linked to the treatment
Gene therapy using viral vectors is mainly hampered by immunogenicity 115 –119 particularly with AAV. Indeed, many people have already been infected by wild-type AAV once in their life, inducing anti-capsid neutralizing antibodies (NAb) spread among various serotypes. 120 –123 Moreover, cross-reactive immunologic material (CRIM) status is also important to predict clinical response. CRIM-negative patients with null mutations or out-of-frame stop codons are completely unable to produce protein (that has to be supplied/involved in their disease) and are therefore more predisposed to develop an anti-transgene response. 124,125 Such host immune responses, particularly happening when IV and intramuscular injections are performed, significantly impair delivery of the therapeutic protein and be possibly deleterious for patients. 126 –128 Delivery of AAV vectors directly into the brain induce low or absent anticapsid or anti-transgene NAb titers in serum. 114,129 –132 Thus, it must be considered for patient inclusion criteria and study design in clinical trials. Conventional strategies to prevent immunogenicity include corticosteroids or immunosuppressive drugs. Corticosteroids (e.g., methylprednisolone and prednisone) and immunosuppressive drugs (e.g., sirolimus, tacrolimus, rituximab, bortezomib, mycophenolate, and cyclosporine) are administered postinjection and eventually in pretreatment in several clinical trials, 12,133,134 although their effects are controversial. 135,136 Other approaches are emerging such as plasmapheresis, 135,136 editing AAV capsids to eradicate epitopes that induce NAb generation, 137 using tolerogenic nanoparticles, 138,139 and the incorporation in the transgene of microRNAs (miR) target sequences integrated in the expression cassette that specifically repress translation in antigen-presenting cells 140,141 or oligonucleotide sequences that inhibit Toll-like receptor 9 (TLR9) activation (in development by George Church's Laboratory, Harvard Medical School, patent WO2017214378A1).
Future Development and Perspectives
New AAV serotypes with broad CNS transduction after IV delivery
Over the past decade, significant efforts have been expended in updating the natural repertoire of viral vectors and engineering new serotypes. 142 Using the Cre recombination-based AAV-targeted evolution (CREATE) technique, new AAV variants have been isolated, some able to homogenously transduce the CNS, especially neurons and astrocytes, after IV injection in mice, 42,143 and potentially in NHP, although clear evidence of efficacy remain to be demonstrated. Improved CNS transduction is linked to Ly6, which is not expressed in all mouse lines and not in NHP. 144,145 Indeed, a major challenge is to identify capsids that will be able to efficiently pass the BBB and in mice, NHPs, and human subjects. In addition, the selected capsids should be compatible for large-scale production.
BBB opening as a solution to enhance CNS targeting
Temporary disruption of the BBB might help delivery in the brain parenchyma. Osmotic disruption of the BBB with intra-arterial injection of mannitol has been widely studied and allows for delivery of a variety of drugs and agents into the CNS, including viral vectors. 146 However, this technique induces a diffuse opening of the BBB, precluding targeted delivery of drugs, and is potentially associated with significant neurological side effects.
Ultrasound (US)-induced transitory disruption of the BBB is another technique that has gained increasing interest since Hynynen et al. demonstrated that the IV injection of preformed gas bubbles before low-intensity pulsed US sonications allowed for a reduction of the acoustic pressure necessary to safely open the BBB in rabbits. 147 The interaction between US and injected microbubbles is essential for opening the BBB, and mechanisms of BBB disruption may include transcytosis, cell fenestrations, and opening of tight junctions. 148 US-induced BBB disruption can be monitored with MRI, as a contrast enhancement in T1-weighted sequences after gadolinium injection 147 and is limited to the US beam. 149
The safety of the technique has been assessed through preclinical studies. With optimized parameters, histological side effects are limited to red blood cell extravasation and petechial bleeding 150 after both single or multiple US sessions. 151 BBB disruption may induce a transitory sterile inflammatory response. 152 Recent studies have confirmed that the technique was clinically well tolerated in NHPs. 153
This technique was used to deliver an AAV1/2 viral vector in a targeted manner to the striatum of rats. Transduction observed was mainly restricted to neurons and stable for >1 year. 154 Two main approaches have been developed to bypass the skull interface that induces attenuation and distortion of the US beam. In one case, InSightec (Haifa, Israel) developed a 512-element phased-array transducer, the ExAblate® 4000 system, that allows a transcranial and noninvasive opening of the BBB. 155 On-going clinical trials are currently evaluating the safety of the ExAblate system for drug delivery after BBB disruption (NCT02343991 and NCT02253212). In another case, CarThera SAS (Paris, France) designed an implantable device, the SonoCloud® device, which can be plugged into the skull and activated through a transdermal needle. 149 Interim results of the first clinical trial (SONOCLOUD, NCT02253212) evaluating the safety of this system in adult patients treated for recurrent glioblastoma with systemic carboplatin have shown no dose-limiting toxicities and no treatment-related serious adverse events. 156 A phase I trial (SONOKID) assessing the safety of repeated BBB disruptions by the SonoCloud device in association with IV chemotherapy in recurrent supratentorial malignant primitive tumors in the pediatric population was launched in 2020. 157 More recent studies have been reported with percutaneous US but with no additional value. 158
Encapsulated cells and optogenetics
Encapsulated cell technology (ECT) eventually combined with optogenetics allows the delivery of treatment in a continuous or in a controlled/discontinuous ways, respectively.
ECT is a concept based on the confinement of the grafted cells within a permeable device.
ECT has already been shown to be well tolerated in large animals such as dogs for the treatment of intervertebral disc degeneration
159
and in pigs
160
and NHPs
161
for AD. Moreover, ECT has already been translated to clinical studies where the safety, feasibility, and tolerability of procedure has been shown, for example, the delivery of neurotrophic factor in disorders of eye
162
–164
(
The optogenetic approach uses optical methods to modulate the cellular expression of molecules, which are activated by irradiation with light energy by genetic engineering to control/regulate cellular function or intracellular signal transduction. 171 One of the challenges of optogenetics is its translatability to the clinic. Many improvements in optogenetic technologies in NHPs have been performed to exert precise control of specific cells or brain regions at the millisecond timescale and to reliably transduce cells and readout the optically induced neural modulation. 172,173 A new optogenetic approach has been described by Ruiz et al., 2013 in which the native dura is replaced with optically transparent artificial dura allowing visual monitoring of the expression of the optogenetic agent over time. 174
The first optogenetic study of NHP was performed in 2009175 and followed by numerous studies performed to study the link between brain function and behavior using optogenetic stimulation. 176,177 None of the optogenetic studies allowing the delivery of treatment was performed in NPH. However, many applications of optogenetics in CNS diseases (stroke, epilepsy, multiple sclerosis, AD, and PD) were described by Ordaz et al.. One of the major obstacles to widely use optogenetic tools in patients remains the delivery to the brain. For this reason, it is essential to reduce brain tissue damage inflicted by probe penetrations and light-induced heating for optogenetic procedures. Once these problems are overcome, optogenetics can be an advantageous tool to treat neurological diseases providing an alternative treatment with less side effects than current therapies. 178 The first patient dosed with optogenetics was treated for retinitis pigmentosa in a clinical trial conducted by RetroSense Therapeutic in 2016. More recently, a phase I/II clinical trial of optogenetics for vision restoration is registered (NCT02556736, sponsor Allergan; NCT03326336, sponsor GenSight), but no results have been published to date.
HSC gene therapy to treat CNS diseases
Hematopoietic stem cell transplantation (HSCT) is the best example of stem-cell therapy and is currently an established treatment for several neurologically devastating inherited metabolic diseases, including ALD and lysosomal storage disorders (LSDs). 21,22 In LSDs, donor-derived microglia cells of myeloid origin are thought to be the source of enzyme after HSCT, cross-correcting the metabolic defect in affected host cells. 179 In addition, engrafted donor-derived cells may potentially help in reducing accumulated toxic substrates in the brain. Of importance, there is evidence that stem cells are not only replacing dying cells, but are also regulating inflammation and immune responses and have proneurogenic effects. 180
Numerous studies support the notion of using stem cells as a treatment for inherited diseases like LSDs, 179 HD, and also for complex diseases like AD, PD, and amyotrophic lateral sclerosis. 181,182 Further preclinical and clinical studies are needed to ensure the safety and efficacy of these treatment options. 182
Conclusion
The recent beneficial results demonstrated in phase I–II studies in human patients together with improved vector technology have placed gene therapy for CNS diseases in a new development paradigm. These approaches are no longer restricted to rare genetic diseases, but are being applied to common disease indications and pathways significantly expanding the scope of gene therapy for CNS indications. This expansion requires simplifying delivery protocols and anticipating the increasing need of vector production, particularly for IV targeting. Treating an increasing number of patients requires standardized delivery protocols suitable for adaptation in multiple centers around the world. Furthermore, manufacturability is a central component in expanding the GT field, not only the production of high quality and high quantity of vectors to meet future clinical demand, but also the cost and our capacity to make new gene therapy products accessible to all patients.
Footnotes
Author Disclosure
No competing financial interests exist.
Funding Information
No special fundings was received for this review.