
Abstract
Breast cancer is a heterogeneous disease, which is the consequence of several genetic and environmental factors. Also, it is one of the most common causes of cancer death and second leading cancer among women all around the world. Therefore, it is necessary to develop novel therapeutic approaches useful for the successful treatment of breast cancer. As conventional treatments had limited success, alternative approaches for the treatment of breast cancer have been applied in recent years. Hence, the molecular basis of breast cancer has provided the opportunity of using genetic materials for therapeutic uses. In this regard, gene therapy as one of the potentially efficient and beneficial treatments among various techniques became a popular treatment for different cancers, especially breast cancer. Accordingly, there are plenty of targets available for gene therapy of breast cancer. Gene therapy strategies have the potential to correct molecular defects that contributed to the cancer progression. These techniques should selectively target tumor cells without affecting normal cells. Moreover, data of clinical trials in gene therapy for breast cancer indicated that this approach has little toxicity compared to other therapeutic approaches. In this study, different aspects of breast neoplasm, gene therapy techniques, challenges, and recent developments will be mentioned.
Introduction
Breast cancer is a malignant tumor resulting from uncontrolled proliferation of abnormal cells related to some kind of genetic mutation, which is placed in the mammary glands and commonly begins in the mammary ducts or breast lobules. 1 –4 On the other hand, it is one of the most frequent cancers among women throughout the world and the second cause of death following lung cancer. 1 –3 Records show nearly two million new cases and 626,700 deaths in 2018; it solely accounts for 25% of all cancer cases and 15% of all cancer deaths between the female populations. Also, it has shown that in developed countries, almost half of the women are affected, and there were around 40% of death cases in that area. However, Asia and Africa have the least amount of breast cancer cases.
Different subgroups of breast cancer make it more difficult to treat. However, novel treatment approaches and early detection increase the chance of recovery in patients with breast cancer. Moreover, breast cancer has diverse etiology and pathology. 5 Subsequently, it can be classified into three types, including molecular classification, morphological classification, and tumor grade. Tumor grade is recognized as Nottingham combined histologic grade, which is based on the semiquantitative assessment of morphological characteristics associated with tumor differentiation from normal cells.
Breast cancer has subgroups in morphology that show its invasiveness and place of origin. 3,6 Molecular subtypes can be classified based on the hormone receptor status, progesterone receptor (PR), and estrogen receptor (ER), and based on gene expression profiling, including Luminal A, Luminal B, amplification of the human epidermal growth factor receptor 2 (HER2), and the basal-like mostly Triple-Negative breast cancer (TNBC). Moreover, these can be detected better than the other types with ER antagonist tamoxifen and aromatase inhibitors. 1,3,6 Luminal B is ER positive, but PR negative, and they can be either positive or negative for HER2. 1,3,5,6 HER2-positive tumors show an overexpression of the HER2 oncogene and are able to control and treat with the anti-HER2 monoclonal antibody trastuzumab and combined with conventional chemotherapy, in which the survival rate will be raised 30%. 1,3,5,7 Furthermore, TNBC does not react to hormone and HER2 receptors. Consequently, these types only treat in standard ways. Unfortunately, the trend of this type cannot be predicted. 3 ER-positive breast cancer constitutes 70% of Western women, while Arab women show a greater part in ER-negative breast cancer, with a high prevalence of TNBC (20% in the United Arab Emirates [UAE] to 39% in Saudi women), except for Lebanese women (9.3%), with rates comparable to that of European women (9%). Besides, In comparison with the other parts of the world, HER2 overexpression is much more common in the Arab region (39.5% in Lebanon).
Also, breast cancer is classified as invasive and noninvasive. 8 Invasive breast cancer attacks breast tissues and after growing, penetrates the skin and pectoral muscles. Its malignant cells can move to the lymphatic circulation and transfer to the armpits and organs, such as bones, brain, and lungs. This process is named metastasis. 4,8,9 Noninvasive carcinoma is a primary tumor and its extension is not transferred to the basal membrane that isolates the ducts and lobules of the breast from adjacent tissues. 8
There are several risk factors for developing breast cancer, including, reproductive, menstrual history, hormonal, age, benign breast conditions, alcohol, radiation, obesity, and lack of physical activity. 6,8,10
The most frequently mutated genes are breast cancer gene 1 (BRCA1) and breast cancer gene 2 (BRCA2), although additional genes related to hereditary breast cancer are emerging. 6,8 Novel studies in the technology of genomics in cancer resulted in parallel testing of multiple genes. 8,11 Subsequently, at present, next-generation panels are performing the simultaneous analysis of breast cancer susceptibility genes, from high penetrant genes (such as tumor protein p53 [TP53], BRCA1, and BRCA2) to intermediate penetrant genes (like checkpoint kinase 2 [CHEK2], partner and localizer of BRCA2 [PALB2], and Ataxia-Telangiectasia Mutated [ATM]) 6,8 (Fig. 1). However, some of them can raise the probability of other cancers, ovarian, pancreatic, and colorectal cancer to name, but a few. 6,8
Possible gene mutations associated with breast cancer development. Some examples of high-penetrant genes, including BRCA1, BRCA2, and TP53, and also intermediate penetrant genes, including CHEK2, PALB2, and ATM. 6,8 ATM, Ataxia-Telangiectasia Mutated; BRCA1, breast cancer gene 1; BRCA2, breast cancer gene 2; CHEK2, checkpoint kinase 2; PALB2, partner and localizer of BRCA2; TP53, tumor protein p53.
As mentioned before, early detection plays an important role to choose the best way to treat and the most common way for diagnosis of breast cancer, including breast screening done by a doctor to check for lumps in the armpits and breasts, breast ultrasound, mammography, magnetic resonance imaging, and breast tissue biopsy. 4,5,9,12 After confirmation of the existence of breast carcinoma, further tests and methods are done to classify the stage of cancer, such as computed tomography scan, positron emission tomography scan, and blood test. In comparison to all the tests, the golden standard for early breast cancer diagnosis is mammography, which has been fraught with sensitivity issues. However, some techniques, including clinical and self-breast cancer screening, have significant biases and usually could cause a false positive result, 4,5 while molecular biology techniques such as immunohistochemistry have played a significant role in meeting the needs of breast cancer diagnostics. 5,9 Also, studies indicated that gene therapy as a novel approach has broad potential to treat different cancers, including breast cancer. Herein, gene therapy as a new approach to treat breast cancer, and also its challenges, techniques, and advances, has been discussed.
A Snapshot of Breast Cancer
Breast cancer is a malignant tumor that begins within cells in the breast. 1,2,6,8,13 Also, it is one of the most frequent oncologic causes of cancer-related deaths among women, which is currently affecting more than one in ten women worldwide. 1,6,8 The chance of being diagnosed with breast cancer generally is related to getting older among women. 6 This disease is diagnosed in the women population at most. 1,6,8 However, even men can be affected by breast cancer. 6 Moreover, breast cancer is frequent in even developed or wealthy countries. 8 Fortunately, the mortality rate of breast cancer has declined in the last few years because of the enhanced emphasis on early diagnosis and also development of more effective therapeutic approaches. 6,8
Recent studies revealed that new cases of breast cancer are nearly the same for black and white women. 6 Although the mortality rate is different in all parts of the world, black women are more probable to be diagnosed with breast cancer at a younger age than white women. However, breast cancer incidence is lower among black women than white women. Even though the incidence of breast cancer is somewhat low among black women, the mortality rate of breast cancer is significantly higher in this ethnic group. It may concern that Asian/Pacific Islander women have the lowest incidence and death rates among all the cases around the world. Possible variations in biological features between black and white women have the potential to affect breast cancer screening and treatment outcomes among the two ethnic groups. 6
Various subtypes of breast cancer have been recognized: the ER+ and HER2/neu-positive subtype, the ER+ and HER2/neu-negative subtype, and the basal-like breast cancer, also known as TNBC tumors, which are high-grade tumors and the most aggressive subtype. 1,6 Studies have now confirmed that pregnancy and higher parity increase the risk of basal-like breast cancer, but reduce the risk of ER+/PR+ breast cancer. On the other hand, breastfeeding eliminates the increased risk of TNBC. 6
Genetic basis of breast cancer
Carcinogenesis is a complex process described by genetic and epigenetic changes, which eventually formed cancer by affecting main cellular pathways. These alterations in breast cancer are divided into two groups, including loss of heterozygosity (LOH) of tumor-suppressor genes and chromosomal alterations. 14 LOH is a common somatic alteration, which contributes to breast cancer development, and is a kind of genetic mutation in which one normal copy of a gene or genes is lost. In this process, one allele in a patient's tumor is lost when there is a heterozygous state in normal cellular DNA marker. 15 This process is very important if it happens at the locus of a tumor-suppressor gene (TSG) and afterward, inactivating mutation occurs in the second allele. Therefore, LOH is responsible for losses or inactivation of TSG. In breast cancer, LOH has been defined in different chromosomes such as 1, 3, 4, 5, 6, 7, 8, 9, 10, 11, 13, 16, 17, 18, 22, and X. 16,17
TSGs are a group of genes whose loss of function leads to increase in malignancy. These genes negatively affect growth and metastatic potential of cancer cells such as adhesion and protease activity regulation. 18 Moreover, there are some other mechanisms, except mutation, which can interfere expression or function of TSGs, including increase in the rate of proteasomal degradation, gene promoter methylation, and abnormalities in other proteins, which associate with gene product. 18,19 In the past decade, some of the important breast cancer-associated genes were discovered. In 1990, BRCA1 gene on chromosomes 17q21, and in 1995, BRCA2 gene on chromosome 13q12–13 were identified. The probability of developing breast cancer due to BRCA1 mutations is approximately 57–65% and in BRCA2 mutations, it is 45–49% over a lifetime. 20 Although BRCA1 and BRCA2 mutations are not very common in sporadic breast cancers, they are responsible for about 80–90% of all inherited breast cancers. 21 Loss of DNA repair function in BRCA1 and BRCA2 proteins resulted in tumor development because these two proteins play a crucial role in DNA double-strand breaks repair. In most of the sporadic cancers, expression of BRCA1 has reduced. There are some mechanisms that control the BRCA1 expression and inactivation like promoter methylation or protein ubiquitination. 22,23
The number of identified TSGs is expanding quickly. The first TSG gene discovered was retinoblastoma gene (Rb). Loss or mutation of Rb has been seen in over 30% of breast cancer patients and it has related to a higher progression. 24 The first identified TSG linked to hereditary breast cancer was p53 gene. P53 is the most studied TSG and the most common mutated gene in different cancers. P53 gene is a nuclear DNA-binding phosphoprotein that plays a significant role in cell cycle regulation, inhibition of angiogenesis, repairing damaged DNA, inhibition of abnormal cell proliferation, and apoptosis (programmed cell death) to elimination of malignant cells. 25 P53 gene mutation can happen in up to 50% of all cancers and over 20–30% in sporadic breast cancer. This gene has been classified as level II prognostic biomarker in breast cancer, and its mutation increases the risk of relapse. 26 Consequently, p53 and Rb play a crucial role in cell proliferation in breast cancer and regulate by oncogenes and other TSGs.
It is considered that the second leading type of cytogenetic alteration in breast carcinoma is gene amplification, which refers to the extrachromosomal, self-replicating elements. Therefore, the number of copies of gene and its function is increased. 14 In breast cancer, the most frequently amplified and functional genes are HER2 and the nuclear transcription factor c-MYC. 27 The location of HER2 gene is on chromosome 17q, which encodes receptor tyrosine protein kinase. HER2 can regulate uncontrolled cell growth and its amplification has been seen in 15–30% of breast carcinoma. A broad survey of DNA sequence data indicated that there is no mutation in the HER-2(neu) coding region, which proves that increasing the dosage of the wild-type gene plays an important role in tumorigenesis. 28 Moreover, c-MYC oncogene, which is located on chromosome 8q24, encodes a nuclear phosphoprotein that is a transcriptional regulator and plays a pivotal role in cellular differentiation, apoptosis, and proliferation. 29 In 15–25% of breast cancer tumors, c-MYC overexpressed, and is related to the poorer prognosis or more aggressive clinical characteristics. 30
Breast cancer risk factors
The initial factors of breast cancer remain unknown, but a woman's probabilities of developing breast cancer are associated with a broad range of risk factors, including woman's age, genetic and epigenetic factors, personal health history, family history, and diet. Environmental factors and lifestyle are also known to be accountable for a large portion of cancer incidence throughout the world. 6,8,31 Herein, environmental, genetics, and epigenetics risk factors of breast cancer have been discussed.
Breast cancer is the most frequent cancer that involves majority of women around the world. In 2018, there were over two million new cases of breast cancer and it is predicted that 627,000 women died from breast cancer all around the world. About 75% of women were postmenopausal and have breast cancer, and of course, the risk will increase when they reach the age of menopause. 32,33 The data of new cases that are reported by cancer registries indicated over 10-fold variation in the rates of breast cancer incidence across populations all around the world. Breast cancer has increased over the past two decades. It has been reported that patients younger than 65 years can be overcome from breast cancer for 5 years. 32,34 The risk factors for breast cancer are due to the mixture of factors. Main factors are being a woman and getting older. Herein, some of the important environmental risk factors have been discussed.
Getting older
U.S. data have shown that women at their menopause age, which is a mean of 45 years old or older, carried a 2.5-fold risk. Hormone replacement therapy can be used and the effect can be seen for 5 years, after 5 years the therapy will be stopped but the efficacy will disappear after a while. 32 Advancing age, menopausal hormone therapy, positive family history of breast cancer, and nulliparity were positively related to breast cancer. Later age at menarche, around 16 years or older, or menopause at almost 55 years or older was less strongly related to breast cancer than was supposed. Moreover, there were weak positive relationships between taller height and heavier weight, and only extreme obesity (body mass index 35 kg/m2 or more) was statistically remarkable and associated with breast cancer. 35
Family history
Family history is one of the most broadly identified breast cancer risk factors. The family history of breast cancer is a heterogeneous risk factor, which relies on the diagnosed age, number of family members affected, and the number of unaffected women in the pedigree. 6,8,31 For instance, a woman's breast cancer risk will raise if she has a first-degree relative diagnosed with breast cancer at a young age or if she has several relatives with breast cancer. 6,8 Mostly, 5–10% of breast cancer is thought to be hereditary. 8,31
In 2009, one study indicated more than 9,000 women with breast cancer (13.7%) having a first-degree relative (mother, sister, or daughter) with a breast cancer history. More than 5000 women (7.3%) gave birth for the first time over age 30. One-third of the patients informed surgical menopause, nearly one half applied oral contraceptives, and two-thirds used menopausal hormone therapy. 35
Radiation therapy
Few studies of radiation therapy of breast cancer in women illustrated distress, severity, and occurrence of multiple symptoms. Five symptoms that indicated the highest incident rates were worrying, lack of energy, trouble sleeping, sweats, pain, and feeling drowsy. Moreover, women younger than 30 years with radiation therapy to the breasts or chest are at higher risk of getting breast cancer than others. 36
Age and sex risk factors
The median age a woman is diagnosed with breast cancer is 61 years. Approximately 1% of men will face breast cancer over their lifetime, while one in eight women will be diagnosed with breast cancer during her life. 6,8
Reproductive history
Reproductive factors have an important impact on the risk of breast cancer. Early age of first full-term birth is extremely protective against late-onset breast cancers, although the risk of early-onset breast cancer raises in each pregnancy, including the first one. Mothers with their first full-term birth at younger than 20 years indicated a 50% decreased risk of breast cancer as opposed to nulliparous women. However, those who delayed their first birth until the age of 35 had a 22% developed risk. 37,38
Life habits
Unhealthy diet and lack of physical exercise can result in weight gain, which plays a crucial role in breast cancer growth and survival rate. 8 Many studies have demonstrated that physically active women have a lower risk of breast cancer compared to inactive women. This decreased risk of breast cancer has been observed in both premenopausal and postmenopausal women. 6,8 Besides, postmenopausal women who promote physical activity can result in a lower risk of breast cancer compared to women who do not exercise after menopause. 6 However, the percentage of reduced risk obtained throughout physical exercise differs between 20% and 80%, with the highest risk reduction observed between those who are most active. 8
Also, diet is a significant factor in health differences in breast cancer and other chronic diseases. Diet can enhance or reduce the risk of cancer. 6,8 The American Cancer Society suggests a diet constituted of more fibers, including whole grains, fruits, and vegetables. 6 Nutritional factors containing vitamin D, meat, fiber, and dietary fat have been studied as both increasing and inhibiting breast cancer development and survival. 6,8
Genetic risk factors
In human breast cancer, one of the main genetic abnormalities is genetic deletions. LOH in breast cancer has been reported at different chromosomal locations, including 1p, 1q, 2p, 3p, 6q, 7q, 8q, 9q, 11p, 11q, 13q, 15q, 16q, 17p, 17q, 18p, 18q, and 22q. 8 The LOH in some chromosomal locations has been proved to include a known six TSG involved in breast cancer, such as p53 at chromosome 17q13, BRCA1 at 17q21, and BRCA2 at 13q12–13. 8,31 The BRCA1 and BRCA2 gene mutations constitute most autosomal dominant inherited breast cancer. 6,31 On the other side, they are human genes that generate tumor-suppressor proteins. 6 These proteins are involved in repairing damaged DNA. Accordingly, they play a critical role in warranting the genetic material stability of the cell. When either of these two genes is changed, muted, or does not function perfectly, DNA damage will not repair, precisely. Consequently, cells will generate further genetic alterations that may cause cancer development.
Collectively, mutations of BRCA1 and BRCA2 genes are considered to constitute between 5% and 10% of all cases of breast cancer and about 20–25% of hereditary breast cancer. 6,8 Also, at most, 55–65% of women who inherit a deleterious mutation in BRCA1 and nearly 45% of women who inherit a deleterious mutation in BRCA2 will manifest breast cancer symptoms at the age of 70. 6,31 Breast cancer in women with a deleterious mutation in BRCA1 gene is also more probable to be TNBC, which has a milder prognosis than other breast cancers. 6,8 Also, BRCA2 mutation is a risk factor for breast cancer in men. 6 Although harmful mutations in BRCA1 and BRCA2 are responsible for breast cancer in ∼50% of families with numerous breast cancer cases, several mutations in other genes have been related to higher risks of breast cancer. 6,8 Rare mutations include BRCA1 interacting protein C-terminal helicase 1 (BRIP1), epithelial cadherin (CDH1), ATM, CHEK2, protein transport protein Sec23B (SEC23B), and PALB2 to name but a few. 5,6,8 Most of the mutations in these genes are associated with smaller increases in breast cancer risk than mutations observed in BRCA1 and BRCA2. 6,8
Epigenetic risk factors
Decreasing the expression of TSGs can increase the susceptibility to breast cancer. However, family history and mutational inactivation of TSG comprise only a small percentage of breast tumors. 39 Epigenetics is related to nonmutational effects, which can alter gene expression. Some studies indicated that endocrine disruptors, which are seen in foods and drinking water, can disrupt epigenetically hormonal regulation and raise breast cancer risk. 39,40 On the other hand, epigenetic biomarkers including DNA methylation, can raise cancer risk by altering gene expression. Epigenetic biomarkers play a critical role in preventing and also recognizing modifiable pathways for targeting interventions and decreasing cancer incidence. DNA methylation markers can improve cancer outcomes along the prevention continuum. 41
Approaches to Gene Therapy
A brief overview of gene therapy
In the historical phase, the history of the ethical debate on human gene therapy is examined. Therefore, the threshold of the Nirenberg was appealed in 1967. The open dispute centered around two initial controversial cases, including those of Rogers and Cline. The in-depth discussion has lasted from 1980 to present, but now adaptation for somatic cell gene therapy, especially a public policy, is emerging. 42 In the human gene therapy debate, many years passed before a moral line was well defined between research relevant to treatment using somatic cell alterations and all other research alternatives involving germline cells, yet which did not morally condemn the possibility of altering germline cells to treat and prevent the transmission of genetic disorders. Two concerns, including somatic cell gene therapy and germline gene therapy, had to be identified and separated for purposes of debate and public policy considerations. 43 However, in the early stages, somatic cell gene therapy and germline gene therapy frequently merged.
Gene therapy has become the research focus for many medical subjects around the world and it has a lot of potential, but it cannot genetically reach the goal unless gene delivery issues are resolved. 44 During 15 years, almost 70% of clinics studied cancer gene therapy, the main goal being successful in vivo transfer of genetic materials. The aim of the delivery system differs based on the application. 45,46 For instance, a prolonged and sustained expression is required for treating diseases associated with one gene dysfunction such as hypercholesterolemia, while a short period of gene expression is enough for most cancer gene therapy approaches. 44 One of the beneficial reasons for gene therapy, especially about cancer topic due to its great development, is nontoxic carriers that deliver genetic materials into targeted tissues.
Gene therapy became one of the most focused topics in laboratories in medicine, pharmacy, biochemistry, and chemical engineering all around the world to its two different group vehicles: biological and nonbiological. Both groups have their advantages and eliminations.
44,47
Biological vehicles, which are viral vectors, are biological systems that transfer genomic materials to host cells. Both DNA and RNA viruses can be used in this way.
44
The viruses, which are used, are modified in laboratories to eliminate their pathogenicity.
48
The limitations of viral vectors in the status of safety, especially immunogenicity, and the capacity of transgenic materials encourage researchers to emphasize the second group, nonviral vectors. Nonviral vectors are naturally cationic and consist of cationic polymers, in particular cationic liposomes, poly
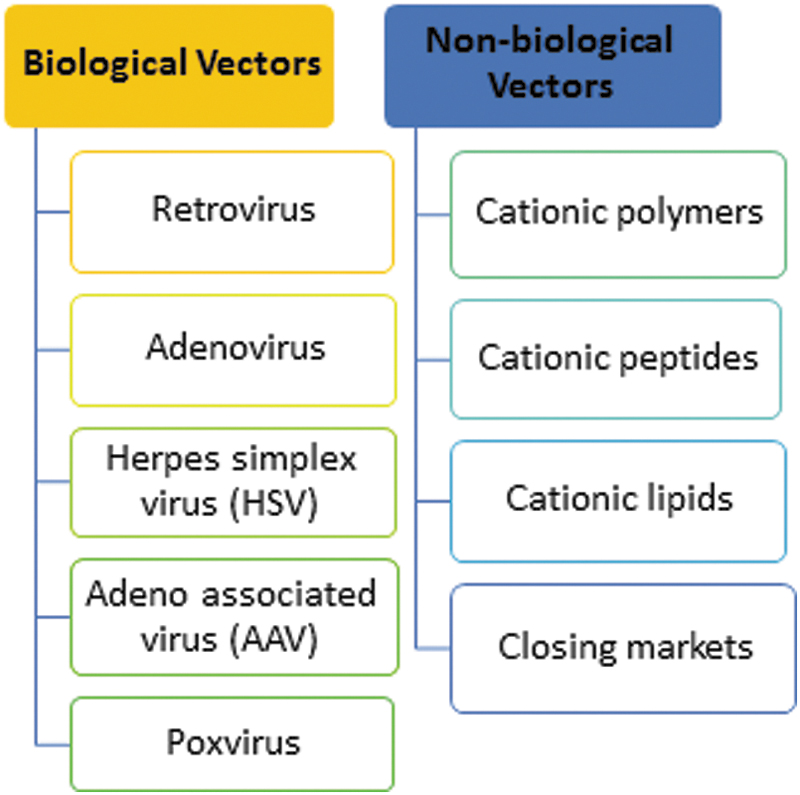
Members of the biological and nonbiological vectors used in cancer gene therapy. Biological vectors, including retrovirus, adenovirus, HSV, AAV, and poxvirus. Nonbiological vectors, including cationic polymers, cationic peptides, cationic lipids, and closing markets. 44,48,50 AAV, adeno-associated virus; HSV, herpes simplex virus.
Four problems with human gene therapy
42,43
: Applying ethics of human experimentation to somatic cell and germline gene therapy. Applying ethical commitment to future generations to stop transmission of genetic disease. Applying genetic knowledge to inhibit or treat genetic diseases and use “enhancement genetic engineering”. Holding the potential to direct the applications of human genetic information to ethically acceptable outcomes in modern societies and still keep scientific and academic freedom.
Two well-known cases of active conflict regarding experimentation and human gene therapy ethics 42,50 :
The first experiment applied an indirect approach, especially injection of a virus, which was considered to stimulate genetic expression. The first case preceded the needed previous group review of research.
The second was a genuine genetic experiment, which is intended to transfer copies of ribosomal DNAs (rDNAs) containing normal genes. It was after the practice was well established.
The most important moral distinction is between uses of genetic knowledge that may relieve patients' suffering, morbidity, and mortality, and those potential uses that would alter characteristics having little or nothing to do with disease. However, cancer is a complex difficulty to deal with it. Various changes on the genetic level of these cells, oncogenes, and TSGs have a great effect on the development of cancer cells. 11,51 These two gene groups counterbalance one another. As TSGs cause apoptosis, oncogenes increase cell proliferation. Accordingly, apoptotic genes and anti-oncogenes can be efficiently applied to treat cancer. 51
On the other hand, gene therapy and chemotherapy can be combined through suicide gene therapy approach. This approach is based on the conversion of a nontoxic prodrug into its active cytotoxic metabolite in the cancer cells. 52 This conversion is interceded by a non-mammalian enzyme, which in the neoplastic cells is overexpressed due to a successful transfection with their genes. Furthermore, cancer is immunogenic. Hence, increasing the immune response against cancer cells can be obtained through genes encoding for cytokines such as interleukin-12 (IL-12) gene, which broadly applied in gene therapy for cancer. Despite the therapeutic approach, the development of efficient and safe gene delivery systems stays the central challenge for gene therapy, including its principal use of cancer gene therapy. 52,53 Moreover, the recent progression in personalized medicine offers great opportunities for researches in gene therapy. 54
Gene therapy for breast cancer
Surgery is the main treatment for early stages of breast cancer. However, there are other treatments such as radiation therapy, chemotherapy, and hormonal therapy. 55 These kinds of treatments are not suitable always, systemic therapies for metastatic disease are not curative, and these treatments are always with clinical risk. 44,55 In a recent study, risk in clinical part in women with breast cancer with an average 21-gene recurrence score of 11–25 who were assigned to endocrine therapy, chemotherapy, or the combination was prognostic. The rate of distant recurrence in endocrine therapy of women 50 years of age or younger at 9 years was <5% and with a low recurrence score of 4.7% ± 1.0%. In this age group, the estimated distant recurrence at 9 years passed 10% among women with high clinical risk and an intermediate recurrence score who only took endocrine therapy (12.3% ± 2.4%) and among those with a high recurrence score who took chemoendocrine therapy (15.2% ± 3.3%). 56 As a result, gene therapy might prove a beneficial substitute for these conventional treatment modalities.
Developments in molecular technologies have broadened a new horizon in finding novel targets in gene therapy. For instance, the emerging of short interfering RNA (siRNA) gives the opportunity to quickly distinguish whether these overexpressed genes are potential candidates for gene therapy. 44,55 In the following sections, various strategies for gene therapy in breast cancer have been discussed.
Genetic compensation
Gene replacement strategies
One of the important techniques in gene therapy for breast cancer is TSG replacement. Lack of one or more TSG genes can result in cancer growth. Therefore, TSGs can suppress or apoptosis tumor cell 14 (Fig. 3). Indeed, the most attractive genes with the potential to arrest cell cycle when presented to breast cancer cells are gatekeeper genes. Some of these gene are BRCA1, BRCA2, p53, Rb, 57,58 p16, 59,60 p27, 61 p21, 62 Testin, 63 Maspin, 64 and melanoma differentiation-associated gene-7 (mda7). 65
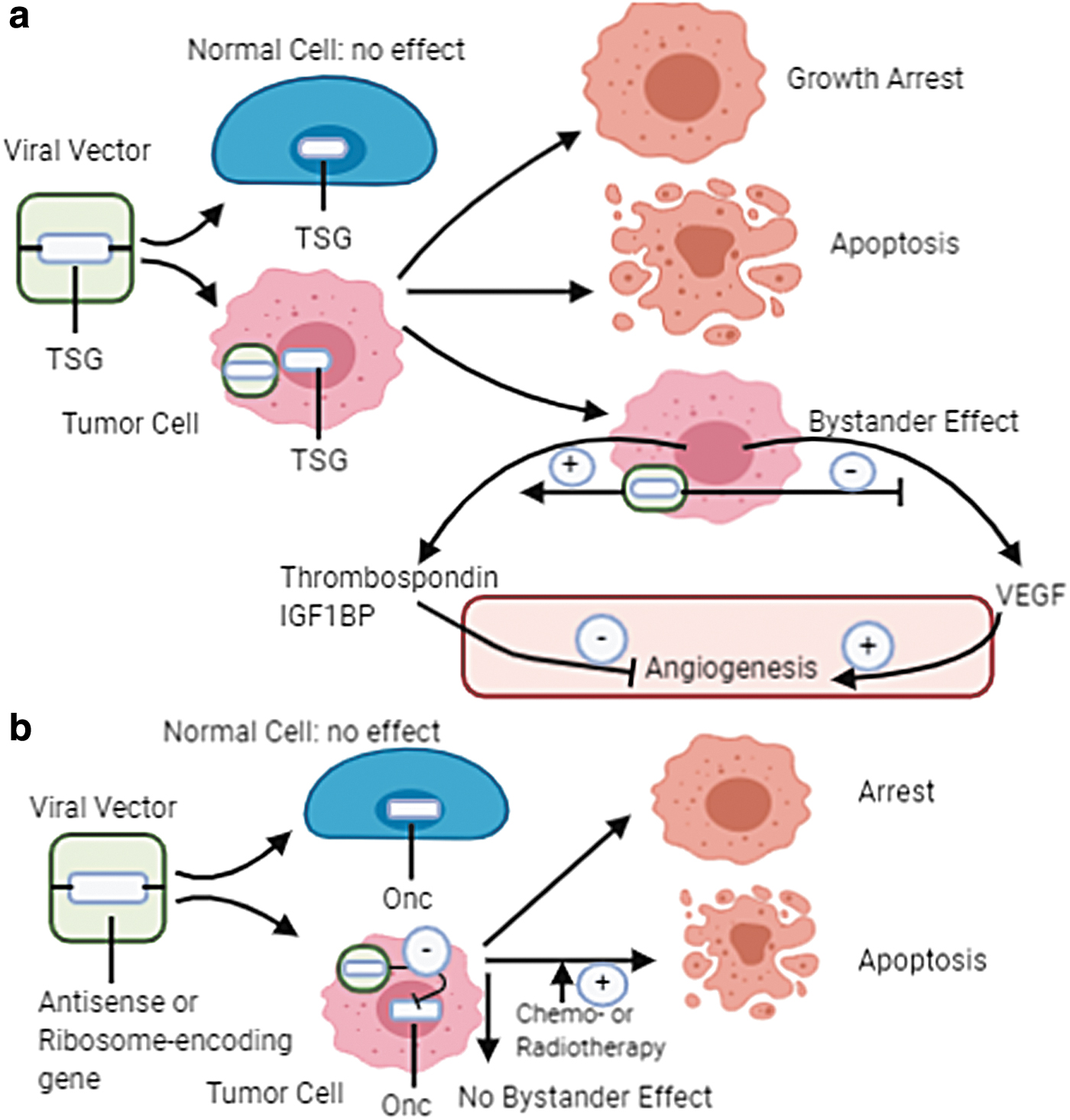
Cancer gene therapy with the delivery of TSGs or inhibition of oncogene expression.
75
Most clinical trials indicated TSG replacement strategy such as p53 replacement. 62,66 This strategy involves the introduction of expressing wild-type p53 into breast cancer cells, which create the normal balance of cell growth and cell death of breast cancer cells. One of the aspects of p53 insertion is the bystander effect. 66 It means that a small percentage of cancer cells is being transduced in vivo in which p53-transduced cells are killed along with the surrounding nontransduced cells. 67 The suggested mechanisms include secretion of solvable proapoptotic proteins, immune upregulation, and antiangiogenesis. A bystander effect is extremely beneficial for successful gene therapy approaches. 68
In 1994, Zhang et al. described delivered p53 into lung cancer by an adenoviral vector for the first time. Accordingly, an in vivo study of p53 gene transfer xenograft models of breast cancer in mouse demonstrated notable suppression of tumor proliferation. 69 The other candidate TSG for replacement strategy in breast cancer is Rb gene. 58 Studies indicated the reduction in tumorigenicity of breast cancer model in nude mice by restoration of Rb expression technique. Moreover, replication-incompetent adenoviral vector can express N-terminal truncated Rb protein, which has increased the suppression of breast cancer. There are registered clinical trials for breast cancer using TSG gene replacement therapy involving p53, Rb, and mda7 genes. 14
Antisense strategy
In this strategy, antisense molecules can precisely inhibit the pathogenic gene expression. The techniques of antisense oligodeoxynucleotides, which are short single-stranded DNA (ssDNA) molecules, are altering gene expression by suppressing the transfer of genetic information into protein 70,71 (Fig. 3). The gold standard of antisense technology involves replacing one oxygen atom of the phosphodiester linkage with sulfur. Indeed, nuclease resistance and oligomer stability are enhanced by this backbone modification. Antisense oligodeoxynucleotides can suppress messenger RNA (mRNA) processing by various mechanisms, including RNase-mediated mRNA cleavage, translation arrest, and inhibition of transcription or splicing. 71,72 Concerning antisense inhibition of oncogene activity, studies indicated the inhibition of lymphoma proliferation by proposing naked antisense DNA to c-MYC. 14
There are other genes associated with breast cancer that are successfully targeted by antisense oligonucleotides such as ribosomal protein P2, αV integrin, erythroblastic oncogene B homolog 2 (c-erbB-2), methylenetetrahydrofolate reductase (MTHFR), protein kinase C-alpha (PKC-α), p21, B-cell lymphoma 2 (Bcl-2), cellular oncogene fos (c-fos), telomerase, telomerase reverse transcriptase, plasma membrane calcium ATPase, and type I insulin-like growth factor receptor (IGF-IR). 14,73 Clinical development demonstrated introducing an antisense oligonucleotide to precisely suppress PKC-α. While its single-agent activity is moderate in breast cancer, its possible function can be in concordance with conventional chemotherapy. 71
RNA interference therapy
Another useful strategy for gene therapy is RNA interference (RNAi) technology, which is a potential intracellular mechanism with the ability to post-transcriptional gene silencing (PTGS) by highly specific technique started by double-stranded RNAs (dsRNAs) homologous to the gene. 74 siRNA and short hairpin RNA (shRNA) can be applied for this strategy for temporary or long-term abrogation of the expression of target gene in breast cancer. 14 Accordingly, some studies indicated specific downregulation of c- by RNAi, which suppresses the development of breast cancer MCF-7 cells in vitro and in vivo. 75
Another technique in breast cancer for ablation of oncogenes is ribozymes. These RNA molecules can work as enzymes also in the whole lack of proteins. Also, they can catalyze the cleavage of RNA substrates and covalent bond formation in RNA strands at particular sites. 14,76 Ribozymes first were applied to treat human immunodeficiency virus (HIV) disease. 77 Hammered ribozyme is one of the best-characterized ribozymes with small catalytic RNA motif, which can generate trans-acting ribozymes directed as opposed to specific RNA sequences. Furthermore, gene-tailored ribozymes presented to cells to knock down the expression of some particular genes. 14 Accordingly, researches indicated that in a mouse model, adenovirus-mediated ribozyme can target HER-2/neu and inhibit the in vivo breast cancer cell proliferation. 78 Moreover, survivin, which also named baculoviral inhibitor of apoptosis repeat-containing 5 (BIRC5), is one of the cancer therapeutic targets and a suppressor of apoptosis protein family, which can control cell proliferation. This protein may be expressed in many human cancers selectively without expressing in normal adult tissues. In this regard, ribozyme-mediated cleavage can inhibit the antiapoptotic activity of survivin in MCF-7 cells. 79 This strategy is important for cancer gene therapy. 75
One of the challenges in this strategy is the possibility of affecting mRNAs in normal cells in which these genes are required for growth factor-dependent signal transduction and a cell cycle in normal cells. 14 To prevail this difficulty, an allosteric trans-maxizyme, a dimer of minimized ribozymes (minizymes), has been created to target two different oncogenes, heparan sulfotransferase (hst-1) and cyclin D1, which are overexpressed in breast cancer cells. 80
Growth receptor strategies
The aim of this strategy is to disrupt normal cellular localization of growth receptors by using the protooncogene erbB-2, which has been investigated in breast carcinoma widely. 14 Accordingly, transfer of a gene that encodes an anti-erbB-2 intracellular single-chain antibody (sFv) can lead to the downregulation of cell surface erbB-2 levels and induce apoptosis in erbB-2 overexpressing breast cancer cells. 14,81,82 Also, adenovirus early region 1A (E1a or E1A) has been discovered to repress HER-2(neu) expression in either rodent or human breast cancer cells during transcriptional suppression of HER-2(neu) promoter. The adenovirus type 5 E1A gene can encode a phosphonuclear protein (transcriptional factor), which is the first viral gene product expressed in host cells after the adenoviral infection. 82,83 This factor, for its part, can stimulate viral gene transcription and reprograms the host's cellular gene expression to permit profitable distribution of adenovirus in host cells. 14 The E1A gene, which is delivered through a cationic liposome, can suppress tumor proliferation and increase the disease-free survival of tumor-bearing mice in an orthotopic model of breast cancer. 14,84
Suicide gene therapy
Suicide gene therapy is a therapeutic technique that was suggested in the late 1980s. 85 This strategy is divided into two approaches, including toxin-based cancer gene therapy and gene-directed enzyme prodrug therapy (GDEPT) or gene prodrug activation therapy or virus-directed enzyme prodrug therapy. 85,86 Toxin gene therapy includes the transfection of genes that express toxic molecules and enzyme-activating prodrug therapy represents the transfection of genes with the ability to express enzymes that can selectively stimulate specific prodrugs. 86 GDEPT is a useful strategy due to improving the efficacy and safety of conventional chemotherapies of cancer. This technique is classified into two-step gene therapy approach for cancer therapy. 87 In the first step, the gene for a nonendogenous enzyme is transferred to the breast cancer cells, and in the second step, a nontoxic prodrug is administered and converted into an active cytotoxic form by expression of the foreign enzyme into the tumor. Consequently, activated prodrugs are able to kill transfected breast cancer cells. 52,88 The enzymes suggested for GDEPT in breast cancer can be assigned into two classes. The first class contains foreign enzymes with the nonmammalian origins, such as carboxypeptidase G2 (CPG2), bacterial cytosine deaminase (CD), and viral thymidine kinase (TK). 89 The second class involves enzymes of human origins, such as cytochrome P450 isoforms. In this approach, the two most suitable examples are CD and TK, which convert 5-fluorocytosine and ganciclovir (GCV), respectively, into their toxic drug forms. GDEPT-mediated toxicity would not be restricted only to cells that have been transduced because of the bystander effect in GDEPT, which can be described as the cytotoxic effect on nontransduced cancer cells after the administration of prodrug. 88 –90 As a result, only a part of tumor mass is genetically altered to express an activating enzyme. 90
There are some experimental studies from murine and human tumor models, which propose mechanisms that show bystander effect, including transduction of endothelial cells within the tumor, induction of antitumoral immunity, and transfer of phosphorylated GCV among tumor cells through gap junctions. 91 Different experimental tumor models have proved that combination of gene therapy with suicide genes and cytokines is a beneficial strategy. 14 Moreover, by applying protein translational control, tumor specificity of molecular chemotherapy can be increased. Indeed, an effective program for increasing the specificity of gene therapy for cancer in vivo is translational targeting of suicide gene expression in the cells of breast cancer in vitro. Various reports show the effectiveness of the GDEPT system can be improved by double transfer of suicide genes. 90 Accordingly, cancer cell transfection with two distinct suicide genes enables the activation of two different kinds of prodrugs. 14,52
Proapoptotic gene therapy approach
In different cancer cells, including breast cancer, impairing apoptosis signaling is a usual event and plays a pivotal role in the initiation and progression of tumor. 11 The resistance of tumor cells to apoptosis is very harmful due to two consequences: first, increase the spontaneous tumor proliferation, and second, give them resistance to host defense mechanisms, in addition to several kinds of therapy. 92 The identification of genes that play the main role in apoptosis induction proposes another approach for breast cancer gene therapy. In this strategy, genes that induce apoptotic cell death and also transmit further death signals to surrounding tumor cells are delivered and indeed they make a bystander effect. 14
There are different proapoptotic approaches in breast cancer, including functional replacement of TSGs, suicide gene therapy, BCL-2 family proteins, ligand systems and pathways, and death receptor. 14,93 BCL-2 is the first oncogene identified by repressing apoptosis. The BCL-2 family genes have appeared as main apoptosis regulators. In this regard, overexpression of antiapoptotic BCL-2 family members, in particular, Bcl-XL and BCL-2, represents as critical factors in breast carcinoma. 93 Furthermore, death receptors or ligand systems can control apoptosis in breast cancer cells. Tumor necrosis factor-alpha (TNFα), tumor necrosis factor-related apoptosis-inducing ligands (TRAIL), and fas ligand (FasL) are examples of these receptors. 94,95 When the human TRAIL gene was introduced into breast cancer cells and the subcutaneous xenografts of human breast cancer in nude mice by applying an adenoviral vector, it resulted in the prompt generation and expression of TRAIL protein and finally the breast cancer cell death. 14,94,96
Heat shock proteins can promote tumorigenesis by suppressing apoptosis. 97 Researches indicated that the significant stress-inducible heat shock protein 70 (Hsp70), also identified as Hsp70i or Hsp72, is thought to be an antiapoptotic protein , which is relevant to cancer. Furthermore, Hsp70 is an antiapoptotic chaperone protein that can extremely express in human breast cancers and also cancer cell lines. 98,99 Accordingly, the only repression of its synthesis by adenoviral transfer or classical transfection of antisense Hsp70 complementary DNA (cDNA) can result in the extensive human breast cancer cell death, while it does not influence the survival of nontumorigenic breast epithelial cells or fibroblasts (WI-38). 14,98
Antiangiogenic gene therapy approach
Tumor growth and proliferation are angiogenesis (new blood vessel formation)-dependent processes. Hence, repression of angiogenesis is an efficient strategy for the diagnosis and treatment of breast carcinoma. Quantification of microvessel density in tumor specimens is associated with metastasis or tumor regression in several malignancies, in particular, lung and breast cancer. 100
In breast cancer, liposomes can complex to plasmids to encode angiostatin and endostatin ,which can repress breast carcinoma in nude mice. Indeed, antiangiogenic therapy could not control breast cancer proliferation only in humans. 101 Accordingly, it has been proposed that when antiangiogenic therapy is combined with other approaches, both gene transfer-based and conventional are more useful and get better results. 100 In theory, both hormonal and chemotherapeutic approaches could accomplish antiangiogenic therapy, as their antitumor activity is mediated by various mechanisms. 101
One study showed that the relationship of angiostatin with tamoxifen in a breast cancer transgenic mouse model could provide more favorable outcomes than either approach applied alone. 102 Moreover, it has been demonstrated the possible effectiveness of intramuscular delivery of the endostatin gene to the brain for metastatic breast cancer treatment has been demonstrated. 103 It has proved that the administration of recombinant proteins that repress angiogenesis may result in tumor recurrence in mouse models. Therefore, it is necessary to repeat the administration of recombinant proteins to attain a desired therapeutic effect. Indeed, these inhibitors (angiostatin and endostatin) are safe. 101 Due to these considerations and also because the manufacturing and purifying of recombinant proteins in considerable quantities for clinical application are complicated, gene therapy proposes a reasonable strategy as patients could directly generate the inhibitors in their cells. 14
Genetic immunotherapy
The immune system response could be used for the particular elimination of cancer cells. 104 If the immune system becomes susceptible to control breast cancer cells, the prosperity of breast cancer treatment is dependent on innovative approaches in cancer immunotherapy. 105 Immunotherapy based on its capability to engage the host immune system against cancer can be classified into active and passive. The passive strategy represents the administration of preformed components of the immune system, including antitumor cytokines, tumoricidal effector cells to patients, and tumor antibodies to straight eliminate the tumor cell. The active strategy attempts to activate the immune response in patients to produce an antitumor immunity by applying immunostimulatory cytokines and tumor vaccines. 104
There are some causes concerning the desirable development of genetic immunotherapy approaches such as the ability of gene therapy to achieve immunotherapeutic modalities in a more efficient and less toxic way. 14 Also, it is necessary to administrate genes encoding therapeutic proteins, which allow for more natural sustained protein levels in vivo and decrease difficulties with cytokines that are toxic at high levels, but offer short circulating half-lives. 105
Gene delivery systems
Advances in genetic alteration of cancer cells resulted in the development of more effective therapeutic approaches with fewer side effects. Accordingly, the development of effective gene delivery systems should be considered. Gene delivery techniques classified as viral vectors and nonviral vectors. 106,107 Viral vectors are more commonly used compared to nonviral vectors because viral vectors have higher transfection efficacy than nonviral vectors. As the purpose of cancer gene therapy is to transduce as many cancer cells as possible with the therapeutic genes, transfection efficiency is one of the principal concerns in this context. 44,108,109
Viral vectors
Viruses are extremely useful at transducing cells by their genetic material. Therefore, they present great delivery systems for gene therapy. 44 Recombinant viruses should genetically engineer to carry target genes and need a packaging cell line for particle production. Indeed, their viral feature should be paired with the disease targets. 107
The most frequent viral vector applied for gene therapy in several diseases, including cancer, are retroviruses. These viral vectors derived from the Moloney murine leukemia virus. By the development of pseudotyped retroviruses, there are some challenges for using these vectors, for instance, viral titers and the effectiveness of gene transfer can be overcome. 106 Retrovirus carriers are produced by putting therapeutic ones in a place of vital viral genes. Retroviruses are small RNA viruses with average DNA, which merge with genome and produce viral proteins that are removed when changing into a carrier. 110
The second most frequent vectors applied in clinical gene therapy are adenoviruses. Although these vectors are beneficial, they make immunological and inflammatory responses that may provide repeated administrations impossible. One of the solutions to overcome this problem is using adenoviral vectors of different serotypes. 106,109 Some advances have been made on adenoviral vectors. Accordingly, third-generation vectors, called gutless or gutted adenovirus, have been introduced, which lack all viral genes. These vectors are dependent on helper viruses for proper functioning. Several efforts have been done to combine the advantages of both retroviruses and adenoviruses through a chimeric virus. Also, a less commonly used vector, the adeno-associated virus (AAV), incorporates at a locus on human chromosome 19, which does not code for any critical gene. 111 Moreover, herpes simplex virus-based vectors are also being used in various gene therapy strategies. 106
Nonviral vectors
There are two nonviral delivery techniques for transferring genetic materials, including physical techniques similar to injection or gene gun, and chemical techniques. Some physical techniques of gene transfer have been evaluated for gene therapy of breast carcinoma at clinical trials. 107,112
Nonviral vectors are cationic in nature and cooperate with the negative part in DNA by electrostatic interactions. 110 Nonviral vectors are less commonly applied, although they have some pivotal advantages compared to viral vectors. Lipofection, liposome-mediated gene transfer, is the third most common vector system in gene therapy clinical trials. Moreover, the transfer of naked DNA by physical techniques is another strategy for nonviral gene therapy. 45,113 While viral vectors have several disadvantages over nonviral vectors, viral vectors have more transfection efficacy, which makes them preferable. Some of the general advantages and disadvantages of these two vectors are shown in Fig. 4. 106 Also, characterization and specific pros and cons of viral vectors and nonviral vectors can be seen in Tables 1 and 2.

Some of the important general advantages and disadvantages of delivery vectors. 108
Characteristics and comparison of viral vectors commonly used in breast cancer gene therapy
AAV, adeno-associated virus; AV, adenovirus; dsDNA, double-stranded DNA; HSV, herpes simplex virus; RV, retrovirus; ssDNA, single-stranded DNA; ssRNA, single-stranded RNA.
Characteristics and comparison of nonviral vectors commonly used in breast cancer gene therapy
BMCs, bacterial minicells.
Present Status and Future Perspectives
Gene therapy includes the substitution of a defective gene with a normal and usable copy of that gene and also in comparison with chemotherapy is a useful strategy in cancer treatment. Accordingly, several innovative gene therapy approaches are being developed to rebuild safer and more effective vectors or transgenes. 114 At present, gene expression can be targeted in a particular way in tissue and organ by applying cutting-edge delivery technologies. Through these progressions, gene therapy has become responsive to conventional cancer therapy with the ability to promote this strategy in favor of first-line therapy for neoplastic diseases. 107 Currently, gene therapy procedures have a wide range of advanced applications. At first, gene therapy techniques centered on rare diseases intervened by deleterious monogenetic disorders. However, with progress in this area of research, several progressive and chronic diseases, in particular heart failure, neurodegeneration, metabolic disorders, and cancer, were also assessed by applying novel gene therapy strategies. 115
At present, various forthcoming techniques are being developed for targeting cancer applying gene therapy 114 :
Increasing tumor sensitivity to conventional radiotherapy and drugs or expressing a gene to trigger apoptosis,
Embedding a wild-type TSG to offset for its deregulation or absence,
Applying antisense (RNA/DNA) strategy for inhibiting the expression of an oncogene,
Increasing the tumor immunogenicity to incite immune cell identification.
There is a great future for cancer treatment according to gene therapy researches. This knowledge is improving at the molecular level and is a new strategy to stop cells that are growing. However, there are some obstacles for this condition, which should be overcome. The main subject in cancer gene therapy is mostly about technologies from a direct intervention on tumor cells to make the immune system respond to the tumor. 44 Accordingly, this strategy needs knowledge regarding the pathways of intracellular signaling. It is important to know the relationship between cancer cells and the immune system in immunotherapy. There are plenty of targets accessible for breast cancer gene therapy. 107 Some of the most current breakthroughs in nonviral strategies to target gene therapy of breast carcinoma are involving transcriptional control and expanding recombinant, multifunctional bio-inspired systems. Moreover, DNA vaccines for the treatment of breast carcinoma are in development. 107,112
Challenges in Gene Therapy
Although there is notable progress preclinically in cancer gene therapy such as improved targeting and expression in a particular way in tumor, various challenges still limit progress, such as biosafety, low-efficiency delivery, and nonspecial expression. 44 Successful gene therapy in cancer for perfect transgene expression to suppress a tumor-associated gene and delivery of a tumor-therapeutic gene to infected tissue at adequate doses are some of the main challenges in this field. 114
Gene therapy can be successful when vectors or vehicles can act in a targeted manner and delivers a certain gene to target cells without minimal issues. Viruses are useful for their great effect in transducing cells, although the safety concerns in respect of the application of viruses in humans make the non-viral delivery system an effective substitute. These nonviral vectors are suitable for its ease of large-scale generation and use, and loss of distinct immune response. 116 On the other hand, the advancement of viral gene therapy techniques has been restricted for patients with breast cancer. Moreover, viruses should be targeted by presenting evidence in vivo and in patients clinically, and when the virus introduces to its intended position, its rate of infectivity should be sufficiently high to make a notable therapeutic outcome in the absence of immunogenicity. 107
Consequently, to alter the gene therapy of cancer into an effective approach, which is tackle metastatic disease, two central challenges should be addressed. First, the vector or virus requires to meet the tumor efficiently. Second, it requires to evade neutralization by the immune system. 107,108 Furthermore, there are some challenges in which tumor-associated antigens targeted for a DNA vaccine for breast carcinoma. Enhanced focusing on personalized medicine and the biopsy screening resulted in creating a patient or tumor special DNA vaccine that presents various antigens. In addition, with the transferring of fusion coding sequences of DNA for rather than one antigen and adjuvants similar to granulocyte-macrophage colony-stimulating factor (GM-CSF), the chances of incurring a therapeutic immune response will be increased. 107 These challenges are significantly important for the successful development of this field and provided opportunities for cutting-edge translational research. 117 Accordingly, to reach the latest potential of gene therapy approaches such as long-term therapeutic advantage or best possible treatment, it is important to be fully aware of these impediments and develop approaches to circumvent these obstacles. 44,107
Conclusion and Closing Remarks
There are several gene therapy approaches that have been developed for breast cancer treatment. Gene therapy is an essential issue and plays a crucial role in the future of cancer. The great and specific formulation in gene delivery should preserve the nucleic acid substances, precisely target the tumor site, and escape the endosomal degradation. Either viral or nonviral vectors can be improved for moving therapeutic genes that can kill tumor cells. These two kinds of delivery vectors have some demerits and limitations. Still, no delivery system can be used in all sorts of gene therapy with no side effects, although scientists have explored some delivery systems that can be useful for gene delivery to particular tissues or cells. A lot of changes happened to delivery and novel carrier systems to develop a great view of good transfection. 110,118
Accordingly, one of the significant obstacles for genetic-based therapy is the production of proper delivery vectors that need to be endorsed and achieve regulatory approval. Although there has been an improvement in applying nucleic acids in the form of drugs, there are still problems across the vectors applied to deliver in these treatments. Immunological issues across viral delivery vectors, less efficient delivery by nonviral approaches, and the production of recombinant vectors should all be tackled. 107
Moreover, recent advances in personalized medicine suggest exceptional prospects for researches in the field of gene therapy. 54 In this regard, researchers are improving and applying diagnostic tests concerning genetics to better prognosticate patients' reactions to targeted therapy. 54,119 On the other hand, developing bioinformatics tools can increase our awareness and insight into the genomics of breast cancer and open up new horizons for the investigation of novel strategies. 11 It is expected that continuing the production of significant preclinical data and developments of delivery vectors will result in improvements in clinical testing of gene therapies for patients with breast carcinoma. This science will grow soon because of the possible revolution in therapeutic outcomes.
Footnotes
Acknowledgments
The authors would like to thank Dr. Mohsen Khorshidi for his kind support.
Author Disclosure
No competing financial interests exist.
Funding Information
No funding was received for this work.