
Abstract
China, the first country worldwide to approve a gene therapy in 2003, almost lost the advantage for a head start in cell and gene therapy (CGT) development due to a lack of clear and strict regulatory frameworks. The rapid advancements of CGTs' development worldwide as well as their therapeutic potential have triggered the government to conduct a spate of regulatory reforms to promote normative development of CGTs in China. Encouraged by policy support, the remarkable progress for CGTs in China has been observed over the past few years, thereby catapulting China back into the forefront of CGTs worldwide. This article aims to provide an overview of regulatory reforms, the current development landscape of CGTs, as well as key contributors and challenges for CGT development in China.
Introduction
Cell and gene therapies (CGTs) are designed ideally to halt a disease in its tracks or reverse its progress, which transform the traditional paradigm of disease treatments and may provide breakthrough opportunities for some severe diseases. 1 China, as one of the forerunners in advancing the development of innovative technologies, began research on CGTs at an early stage, conducting the world's first clinical trial for gene therapy in 1991 and approved the world's first gene therapy (Gendicine) in 2003. 2 However, due to loose and ambiguous regulation of CGTs, the development of CGTs was once in chaos in China, with unapproved CGTs being widely used for disease prevention and treatment in private clinics or even large hospitals. 3
In 2016, the event of “Wei Zexi” alarmed the whole nation; a college student died from receiving unapproved DC-CIK cell therapy for synovial sarcoma. 4 This tragedy resulted in an immediate government “shutdown” of almost all research of CGTs in China, which severely impeded research and development of CGTs. 5 The application of unproven CGTs in patients has also perpetuated a global health problem leading to multiple patient injuries and deaths, threatening legitimate research efforts, and undermining regulatory authority to safeguard public health. 6 All stakeholders on national and international levels must collaborate to efficiently address this complicated and multifactorial problem. 7
The rapid advancements of CGTs worldwide coupled with their therapeutic potential in fulfilling unmet clinical needs of patients in China have prompted the Chinese government to establish effective regulatory frameworks for CGTs. Over the past few years, a series of technical guidelines related to CGTs have been released by the Chinese government to provide incentives and encourage investments in the field. 8 Most recently, thanks to the government support, substantial progress in the field of CGTs have been achieved in China. Currently, China is ranked second in terms of the number of patent applications and registered clinical trials for CGTs worldwide, following the United States. 9 On June 23, 2021, the first chimeric antigen receptor T (CAR-T) cell therapy, Yescarta, was approved in China for the treatment of relapsed or refractory large B cell lymphoma after two or more lines of systemic therapy in adult patients, which is a remarkable milestone for cell therapy in China. 10
In this article, we aim to (1) provide an overview in the evolution of regulatory reforms related to CGTs in China, (2) present the current development states of CGTs for publications, patents, clinical trials, and products in China, (3) discuss key contributors for the growth of CGTs' development in China, and (4) explore what challenges remain for CGTs, and what efforts await to achieve its future success in China.
Regulatory Reforms for CGTS in China
Over the past three decades (1990–2020), over 30 national regulatory guidelines or standards for CGTs have been released by Chinese regulatory authorities (Supplementary Table S1). The regulatory reforms in China can be roughly divided into three periods: initial period, rectification period, and standardization and acceleration period. The milestones for the regulatory reforms and major events for CGTs in China are highlighted in Fig. 1.
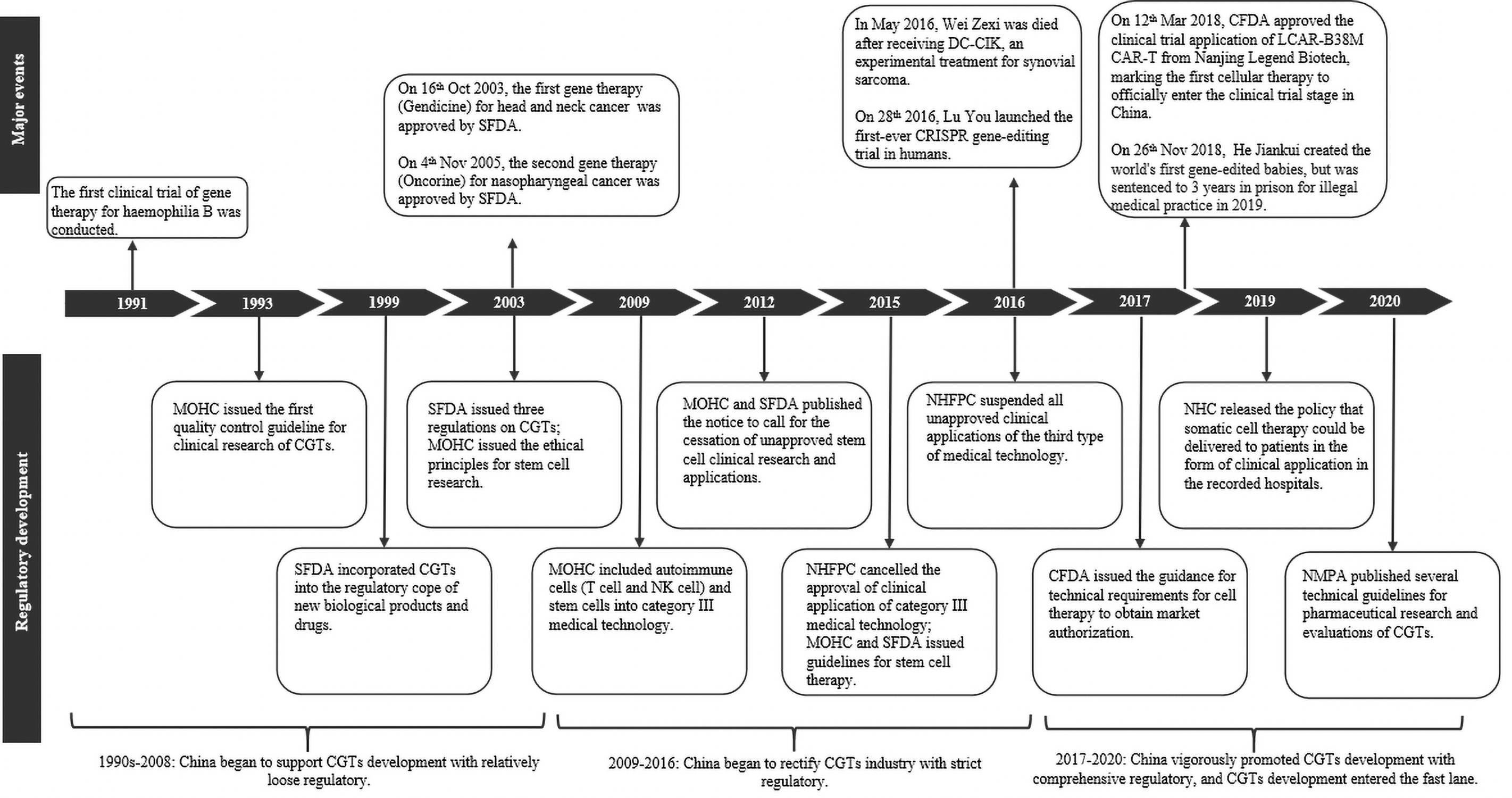
The major events and three regulatory development periods related to CGT in China from 1991 to 2020, including the key milestone events, important events affecting the regulatory reforms, three regulatory development periods and key regulatory guidelines and issues in each period. CFDA, China Food and Drug Administration; CGTs, cell and gene therapies; MOHC, Ministry of Health of the People's Republic of China; SFDA, State Food and Drug Administration; NHC, National Health Commission; NHFPC, National Health and Family Planning Commission of the People's Republic of China; NMPA, National Medical Products Administration.
Initial Period with Loose Regulation (1990s–2008)
In 1993, CGTs were first incorporated into the regulatory system in China, with the release of the first quality control guideline for clinical research of CGTs by the Ministry of Health of the People's Republic of China (MOHC). 11 In 1999, the State Food and Drug Administration (SFDA) stated that CGTs were supervised as new biological products. 12 In 2003, SFDA drafted the guidelines for human cell research, which included requirements for manufacturing, nonclinical research, and clinical trial of cell therapy. 13 SFDA also issued the guidelines for human gene therapy research, which stipulated requirements for clinical trial application and quality control. 14 That same year, MOHC and the Ministry of Science jointly issued ethical principles for research of human embryonic stem cells, and MOHC published the technical guideline for human-assisted reproductive technology, which prohibited the gene therapy for the purpose of reproduction. 15,16
During this period, Chinese authorities began to explore how to regulate CGTs' development. The regulatory environment was relatively loose.
Rectification Period with Strict Regulation (2009–2016)
In 2009, MOHC announced autoimmune cells (T cell and NK cell) and stem cells were included on the list of category III medical technology. Medical institutions with approvals from MOHC were allowed to conduct clinical applications of products on this list in routine clinical practice. 17 However, due to the relatively loose regulatory system, many cell therapies without approvals were illegally applied in some medical institutions, thereby creating chaos in the CGT industry. As a result, in 2011, MOHC and SFDA jointly published a notice for the cessation of unapproved stem cell clinical research and applications, and the self-examination and self-correction for cell therapy for 1 year were performed in China. 18
In 2015, National Health and Family Planning Commission of the People's Republic of China (NHFPC) cancelled the approval of clinical application of category III medical technology. 19 Subsequently, NHFPC and China Food and Drug Administration (CFDA), previously known as SFDA, jointly issued the guidelines for clinical research of stem cell therapy, which stipulated that medical institutions needed to be recorded in both the NHFPC and CFDA before initiating stem cell clinical research. 20 In 2016, due to the death of Wei Zexi, NHFPC stopped all the clinical applications of unapproved immune cell therapy, which resulted in the stagnation of immune cell therapy development in China. 5 That same year, the NHFPC issued measures for the ethical review of biomedical research involving humans, which required the responsibilities of Medical Ethics Committees and further specified the basic scope and operation procedure of informed consent. 21
During this period, China took actions to rectify the CGT industry by tightening its regulatory policies. However, from an overarching perspective, the regulation of CGTs in China was far from standardized and clarified.
Standardization and Acceleration Period with Comprehensive Regulation (2017 to Present)
After experiencing several setbacks, China attempted to establish a stricter and comprehensive regulatory system for CGTs. In 2017, CFDA released the technical guidance on the research of cell therapy, in which the requirements for manufacturing, quality control, nonclinical trial, and clinical trial were specified. Additionally, this guideline stressed that the market authorization of CGTs should be regulated as biological products. 22
In 2018, a Chinese scientist called He Jiankui, announced that his team had used the CRISPR gene-editing system to edit DNA in human embryos to make them less susceptible to human immunodeficiency viruses. This scandal received widespread criticism from some of the world's top scientists. 23 Subsequently, the Chinese court sentenced him to 3 years in prison for illegal medical practice. 23 Affected by this event, China decided to impose stricter regulation for human gene editing and began to step up legislation in this area. In 2019, the National Health Commission (NHC) submitted a new draft of civil code, which required that scientific and medical studies pertaining to human genes or embryos must follow the relevant regulations and cannot harm people's health, breach moral or ethical standards, or violate public interests. 24 The civil code was adopted on May 28, 2020 and took effect on January 1, 2021, which first brought medical and scientific research related to human genes or embryos under civil legislation. 25
Around the same time, China also published several guidelines to standardize and promote the development of CGTs. In 2018, CFDA published key requirements of clinical trial applications for cell therapy to encourage the development of innovative drugs for diseases with unmet needs. 26 In 2019, the NHC also issued the guideline to permit that somatic cell therapy with safety and effective data could be delivered to patients in the form of clinical application in the recorded medical institutions. 27 In 2020, the National Medical Products Administration (NMPA), previously known as CFDA, published five technical guidelines (in consultation, currently) for CGTs in sequences. Two guidelines for clinical trials of immune cell therapy and stem cell-based therapy were released in July and August, whereas three guidelines for pharmaceutical research and evaluation of immune cell therapy, gene therapy, and gene transduction and modification system were released in September. 28 –32
To accelerate the access to drugs in urgent clinical needs, State Administration for Market Regulation established four expedited programs for marketing authorization of drugs in the latest version of the “Drug Administration Law,” including breakthrough therapy designation, priority review and approval, conditional approval, and special examination and approval (Supplementary Table S2). 33 The program of priority review and approval was first proposed in 2015 and updated in 2020; by the end of February 2021, five CAR-T cell therapies have been granted priority review designations (Table 1). 10 The program of breakthrough therapy designation was first proposed in 2020, and the LCAR-B38M, a CAR-T product from Legend Biotech Corporation, was the first product to be granted a breakthrough therapy designation by CDE in China. By the end of February 2021, five CAR-T products were granted breakthrough therapy designations (Table 1). 10 No CGTs have been granted conditional approval so far.
Cell and gene therapies with priority review and breakthrough therapy designations in China as of February 28, 2021
In this period, China has made a lot of efforts to promote CGT development with more regulatory guidelines released to provide clarifications on the requirements for research and clinical trial for CGTs.
Current Development Landscapes of CGTS in China
Publications and patent applications for CGTs
According to the analysis from Chinese Academy of Sciences, China generated 24,199 publications and 4,850 patent applications related to CGTs between 1988 and 2017, which ranked second after United States with 36,901 publications and 14,573 patent applications. 9
In China, the number of publications for CGTs began to increase rapidly between 2003 and 2007 (about 4,500), more than four times compared with that in the period of 1998–2002. 9 The number of publications reached its peak between 2008 and 2012 (about 9,100) and a slight decrease was observed between 2013 and 2017 (about 8,900). 9 Over the period of 1988–2017, two organizations from China were among the top 10 organizations generating the largest publications worldwide: Shanghai JiaoTong university ranking seventh with 795 publications and Huazhong University of Science and Technology ranking eighth with 757 publications. 9 The top 10 organizations with most publications in CGTs in China were all from universities and public research institutes. 34
The patent application trend for CGTs in China was similar to that of publications, with a rapid increase during 2003–2007 (about 300) compared with that during 1998–2002 (about 100). 9 However, unlike that of publications, the number of patent applications still increased dramatically in the period of 2013–2017 (about 3,000), three times higher than that in the period of 2008–2012 (about 1,000). 9 During the period of 1988–2017, one organization from China was listed on the top 10 organizations with most patent applications over the world: Chinese Academy of Sciences ranking seventh with 280 patents. 9 Among the top 10 organizations in China, Guangzhou SALIAI Stem Cell Technology, who ranked third with 131 patents, was an enterprise, and the other organizations were all universities and public research institutes. 34
Clinical trials for CGTs
Currently, the United States and China are leading the race in CGT development with 3,907 and 1,041 clinical trials registered on
China, however, has the leading position in clinical trials for CAR-T therapies, according to the registry on
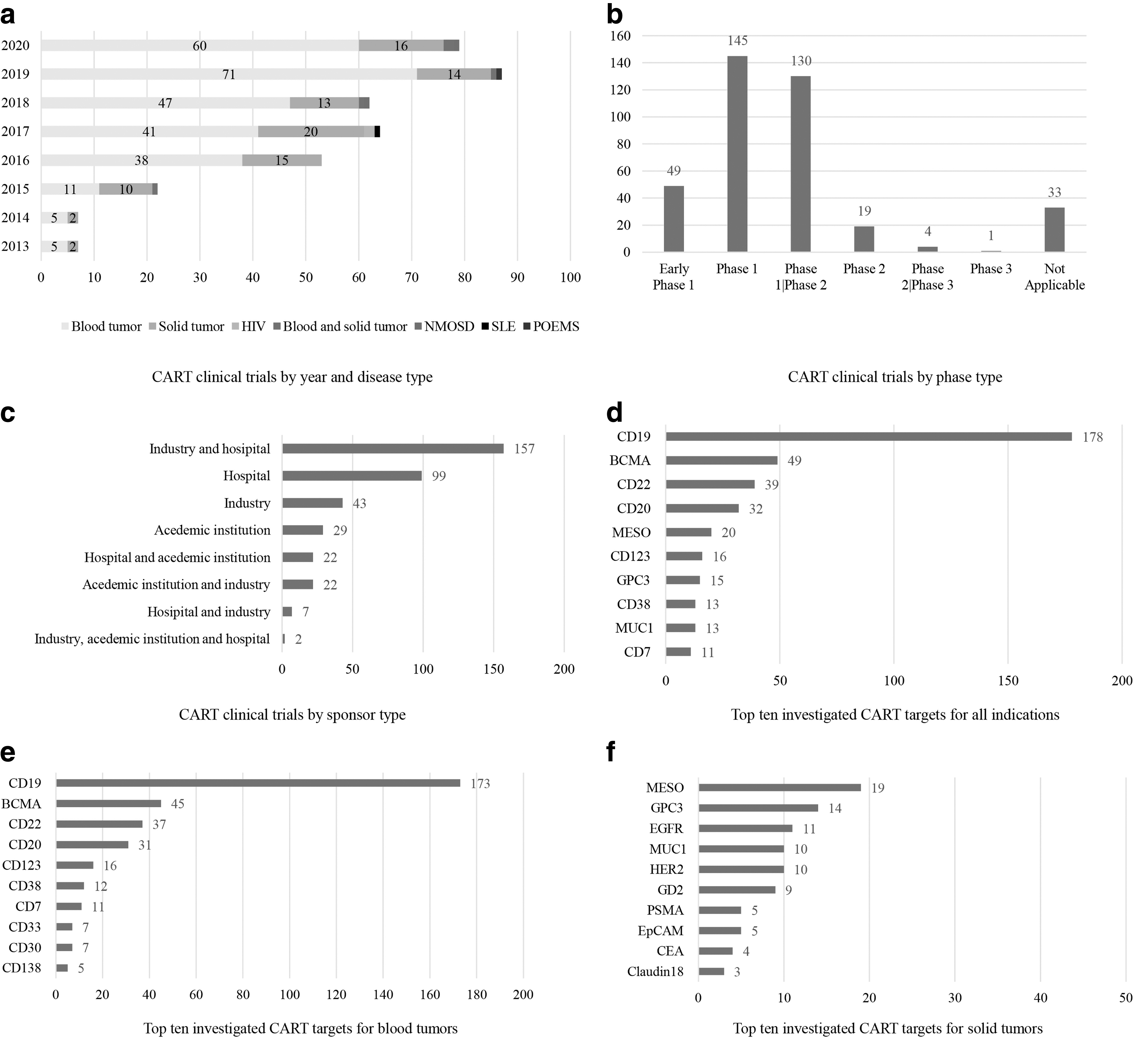
The analysis of registered CART clinical trials on
Most clinical trials (n = 324, 85.0%) were still in the early phases (Phase 1 and Phase 1/2) (Fig. 2b). Only five clinical trials (1.3%) were in the late phases (Phase 2/3 and Phase 3). Among them, three trials investigated the CD19-targeted CAR-T for the treatments of acute lymphoblastic leukemia and B cell lymphoma, one trial investigated the CD123 and CLL1-targeted CAR-T for the treatment of acute myeloid leukemia, and one trial investigated the BCMA-targeted CAR-T for the treatment of multiple myeloma. The clinical trials were mostly sponsored by collaboration between industry and hospital (n = 157, 41.2%), followed by hospital (n = 99, 26.0%) and industry (n = 43, 11.3%) (Fig. 2c).
A total of 69 targets were investigated (Supplementary Table S3), either as single target or a combination of multiple targets. The top five most studied targets for all indications were CD19 (n = 178), BCMA (n = 49), CD22 (n = 39), CD20 (n = 32), and MESO (n = 20) (Fig. 2d). The top five most targets for blood tumors were CD19 (n = 173), BCMA (n = 45), CD22 (n = 37), CD20 (n = 31) and CD123 (n = 16), and the top five most targets for solid tumors were MESO (n = 19), GPC3 (n = 14), EGFR (n = 11), MUC1 (n = 10), and HER2 (n = 10) (Fig. 2e–f).
Investigational new drug applications for CGTs
On March 12, 2018, CFDA approved the first investigational new drug (IND) application of a CAR-T therapy from Nanjing Legend Biotech, which marked that the first CGT was officially licensed for clinical trial initiation in China. 10 This is significant because clinical trials of CGTs not authorized by CFDA will not be accepted for application of market authorization in China.
By the end of 2020, a total of 78 IND applications of CGTs from 53 companies were identified from CDE website. 10 The year 2018 had the most IND applications (n = 38), followed by 2020 (n = 25), 2019 (n = 11), and 2017 (n = 4). Among the 78 IND applications, 12 were approved after the review of CDE, 36 were granted implied approval without receiving rejection or question from CDE within 60 days of their submitted applications, and 30 are still under review. Among 48 IND applications receiving approval or implied approval, 31 were for CAR-T therapies targeting CD19 (n = 22), BCMA (n = 5), CD20 (n = 1), CD30 (n = 1), CLDN18.2 (n = 1), and GPC3 (n = 1). The remaining CGTs with IND approvals included 10 stem cell therapies, 2 gene therapies, and 5 other therapies.
On January 19, 2021, CDE approved the IND application for ET-01, an investigational CRISPR/Cas 9 gene-editing therapy for patients with transfusion-dependent β-thalassemia, which marked the first gene-editing therapy IND application approval in China. 10
Key Contributors to Rapid Development of CGTs
In general, there are three key contributors for the rapid development of CGTs in China: (1) policy and funding support from national and regional governments, (2) investment support from venture capitalists, and (3) multilateral cooperation between biotech companies.
Policy and funding support from national and regional governments
Accompanied with a strict oversight system to standardize the regulation of CGTs, the Chinese government also issued a series of policies to promote the development of CGTs over the past few years. In 2017, the National Development and Reform Commission (NDRC) issued the “13th Five-Year Biological Industry Development Plan,” which stressed that the development of stem cell and CAR-T industry should be one of main focuses in the next 5 years. 39 In 2019, NDRC released the “Catalog for Guiding Industry Restructuring (2019 version),” which classified the varying industries into three categories (encouraged, restricted, and eliminated categories) for directing domestic and foreign investment and guiding government agencies to manage local investment projects. 40 In this document, CGTs were designated as “encouraged” category.
To respond to the national call, various regional governments successively issued policies to accelerate the development of CGTs. For example, the regional governments of Hebei, Shenzhen, and Shanghai have already released the related policies to encourage medical institutions to carry out the stem cell researches in the pilot-free trade zone. 41
At the same time, the Chinese government also increased investments in the CGT industry. According to statistics, stem cell research has been one of the key projects supported by the central government for 3 consecutive years: $69.6 million for 25 projects in 2016; $136.2 million for 43 projects in 2017; and $84.1 million for 30 projects in 2018. 42 In 2019, the Ministry of Science and Technology issued the guideline indicating that the government planned to allocate another $58.0 million to support additional 12 stem cell research projects. 42
This support from the government stimulated great progress with several “first” projects being implemented or in the development. For example, the first Chinese National Gene Bank was officially opened on September 22, 2016 after a 5-year development funded by the Chinese government. 43 It is the world's largest gene bank so far, which aims to promote public welfare, life science research, and industry innovation by supporting the CGTs' development. On August 17, 2018, China Gene Group and Luohu Hospital announced to build China's first specialized hospital for CGTs. 44 On July 31, 2020, the construction of Cell and Gene Therapy Innovation Center was initiated in Beijing and is expected to be put into use by May 2021, which aims to provide the professional services of R&D and clinical trials for biotech companies. 45 On September 28, 2020, the first Chinese cell therapy sharing industry support platform was initialized in Jinan and is expected to be put in use in 2023, which will be the first industrial support system integrating shared laboratories, shared contract development and manufacturing organizations (CDMOs), and shared clinical centers for cell therapy in China. 46 These reflect the Chinese government's interests and incentive toward the field of CGTs by investing extensively in building scientific and technological innovation infrastructure.
Investment raised from venture capital
Promoted by policy encouragement and huge market potential, more and more investments targeted to the Chinese CGT market have been made in recent years. By the end of 2020, about 105 venture-raising events for cell therapy occurred in China with a total amount of $2.5 billion (Supplementary Fig. S1a). 47,48 The amount of venture financing soared to $380.0 million in 2018 with a 706.8% increase compared with 2017 (Supplementary Fig. S1a). This may have been promoted by several technical guidelines and encouraging policies for cell therapy issued in 2017 and 2018, along with the approval of two CAR-T cell therapies (Kymriah and Yescarta) in 2017 by Food and Drug Administration (FDA) in the United States. Among the 105 venture-financing events, 16 of them (15%) were in the angel round, 35 of them (33%) were in the A round, 20 of them (19%) were in the B round, 8 of them (8%) were in the C round or above, and 3 of them (3%) were in the initial public offering (IPO) round (Supplementary Fig. S1b). 47,48
In the face of COVID-19, there were still 41 venture-raising events for CGTs with a total amount of $2.4 billion in China in 2020. 48 The top 10 venture-financing events with largest raised funds for cell therapy in 2020 are summarized in Supplementary Table S4. Nanjing Legend Biotech with raising $423.84 million in US IPO, was the biggest winner in 2020, which also emerged as one of the largest public raises in biotech history.
Partnerships with multinational companies
The multilateral cooperation between biotech companies also accelerated the development of CGTs in China. The multinational companies usually build up collaborations with domestic biotech companies in the form of licensing and joint venture partnerships or establish international clinical research centers to accelerate the layout of Chinese CGT market.
Several pharmaceutical giants or pioneering CGT developers have established partnerships with Chinese biotech companies in the past 5 years (Table 2). 49 Some examples include (1) Juno Therapeutics and its joint venture with WuXi AppTec, named JW Therapeutics, in the development of novel cell-based cancer immunotherapies in 2016; (2) Kite Pharma's joint venture with Shanghai Fosun, named Fosun Kite, for the development of CAR-T in 2017; (3) Nanjing Legend's collaboration with Janssen in granting a world license for the development of LCAR-B38M in 2017; (4) Cellular Biomedicine and its strategic licensing agreement with Novartis to manufacture Kymriah in 2018; and (5) MilliporeSigma establishing a strategic alliance with GenScript focusing on the manufacturing of CGTs in 2019. CAR-T cell therapy for cancer was one of the major focuses in their partnership agreements between Chinese and foreign companies (Table 2). The three companies with approved CAR-T cell therapies, Novartis, Kite (a Gilead Company), and Juno (a Bristol-Myers Squibb Company), all have established alliances in China for the manufacturing and commercialization of their products.
Partnerships between Chinese and foreign cell and gene therapy companies from 2014 to 2021
CAR-T, chimeric antigen receptor T; CGTs, Cell and gene therapies.
The interests of foreign companies in investing CGTs in Chinese companies are foreseeable because of the large market potential, local resources, and research capabilities.
Challenges and Suggestions for CGTS in China
Due to the nature of CGTs, many countries face several challenges in common for the development of CGTs such as great heterogeneity and variation in manufacturing and limited availability of nonclinical data. Besides the common challenges, the clinical development of CGTs in China also faces several specific challenges.
Regulation framework
Even though China has released a series of regulations, the current regulatory framework still cannot meet the rapid development of CGTs in China. Currently, unlike the United States and Europe, CGTs in China follow a “dual-track” regulatory scheme; companies could achieve market authorization from NMPA with proved safety and effectiveness evidence from clinical trials and medical institutions could conduct clinical research within regulatory of NHC. However, the regulatory jurisdictions between NMPA and NHC deserve more clarity, especially for clinical research for somatic cells. Nevertheless, China still has not established comprehensive ethical supervision for CGTs even though many efforts have been made. Some Ethics Committees lack the necessary practical experience and theoretical knowledge, making it difficult to keep their independence. 50 To enhance systematic trainings for Ethics Committees is suggested to instruct and supervise in research protocol and informed consent.
Manufacturing and supply chain
Unlike conventional therapies, the development, manufacturing, and transport of CGTs require consideration and care, including temperature controls and tracking and verifying the chain of custody, which could significantly influence the translational success of these products. 51
In China, the virus vectors usually come from a laboratory's small-scale packaging, which cannot ensure the quality level of carrier uniformity, titer, purity, and infection efficiency of vital vectors. 52 The cells used for clinical research are usually developed in the laboratories of hospitals and research institutions and few of them could meet the requirements of Good Clinical Practice (GCP). 52 Some companies usually work with CDMOs to accelerate the clinical and commercial programs of CGTs. However, the majority of CDMOs for CGTs are located in Europe and North America. 53 In China, the development of CDMOs is in the infancy stage, which lacks the full-lifecycle services from R&D, production to forensic listing. More effects are encouraged from public and private sectors to establish standardized manufacturing, supply chain infrastructure, and professional CDMOs in China.
With the first approval of CAR-T, China needs to address how to develop a standardized and robust good manufacturing practice-compliant manufacturing process for CAR-Treg cells to increase success rate and decrease the costs of CAR-T therapies. Further improvements on optimization of CAR constructs, delivery techniques (viral or nonviral systems), potency testing, and manufacturing automation platforms are suggested. 54
Long-term clinical efficacy and safety evidence
So far, most cell therapies are in the preclinical and early phases of clinical development and long-term clinical evidence is relatively limited, which requires some time to achieve clinical validation. The published Chinese clinical data for CGTs are usually obtained from single center, nonrandomized clinical trials with limited enrolled patients, which increase the uncertainty of trials' outcomes. 55 CAR-T therapies are usually criticized for their severe and occasionally lethal toxicities such as cytokine release and neurological toxicity. 56 A major safety concern for gene therapy is their potential to stimulate immune reactions, which usually requires the usage of immunosuppression. 51 Some gene therapies rely on the use of modified infectious virus, which also increases the risks of life-threatening viral infection. 51
Chinese regulators are suggested to establish dialogue with companies at the early stages of clinical development to address the issues regarding clinical trial designs, risk management plan development, and pharmacovigilance activities, including postauthorization efficacy or safety studies. 57
Pricing and reimbursement
Compared with conventional drugs, CGTs usually require relatively high prices considering the high costs associated with manufacturing, the small market size (especially for orphan products), and life-long clinical benefits through a potential one-time cure. In the case of Yescarta, the first CAR-T therapy in China, the one-time treatment cost is $373,000 in the United States, which equals 35.6 times per capita GDP in China ($10,484 in 2020). 35,58 How to price and reimburse CGTs to ensure patient accessibility is a big challenge for payers in China.
With the increasing approved number of CGTs, Europe and the United States have provided valuable exemplars of innovative payment models to address the concerns of high treatment cost, upfront payment burden, and uncertainty in clinical outcomes for CGTs. For example, in the case of Yescarta, England and France use coverage with evidence development schemes to reimburse it where the future price and reimbursement reassessment will be based on a combination of both longer-term follow-up from the ongoing trials, and real-world data; Italy and Spain have introduced an outcomes-based staged payment scheme, whereby payments (adjusted for a confidential discount on the list price) will be made in instalments linked to individual patient outcomes. 59
Payers in China are suggested to learn from the valuable experience in other countries to explore the reimbursement plan suitable for China's national conditions. Companies could try to find different funding options such as charity organizations, commercial insurance agencies, and patient assistance programs to decrease affordability gaps.
Conclusion
China lost the advantage of being one of the frontrunners in CGTs and is now engaged to catch up with other leading countries. After a long period of unregulated field, CGTs are entering a much more policy-regulated environment in China. While there is more to be done, the necessary legal environment is there and continues to improve. Important investments have been initiated to establish a public infrastructure to stimulate and support the emergence of a performing CGT industry in China. This is translated through fast growth of scientific production and patent filings. Public and private funding are growing fast, showing the high expectations from investors and central/regional governments. The large domestic market as well as the research capability and infrastructure have encouraged foreign companies to enter partnerships with Chinese companies for research, manufacturing, and commercialization.
The future development of CGTs in China will rely more on the multilateral cooperation between governments, companies, and research institutions at the national and regional levels than just private company initiatives. Chinese regulatory authorities are suggested to issue more targeted practical guidelines for the development, production, and application of CGTs to form a comprehensive framework. Research institutions should increase the quality and innovation levels of publications and patents to promote the clinical application and transform of their research. Domestic companies should pay more attention to the trends of market, deeply integrate therapies and new-generation medical innovation technologies, and explore the diversification of products. They also need to explore more possibility to forge strategic alliances with developers of CGTs in other countries, which China will benefit from more extensive exchanges of knowledge and technologies to strengthen their own capability, in addition, to promote the exportation of domestic technologies and CGT products to other countries. The example of Nanjing legend, which successfully completed the IPO, has clearly showed how innovation will attract foreign players, and how it will in turn stimulate the future investments.
Footnotes
Acknowledgments
The authors acknowledge Tarek El-Maghrabi for providing medical writing supports.
Author Disclosure
No competing financial interests exist.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Figure S1
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.