
Abstract
We report the safety (primary endpoint) and efficacy (secondary endpoint) of a novel intracerebral gene therapy at 5.5 years of follow-up in children with Sanfilippo B. An uncontrolled, phase 1/2 clinical trial was performed in four patients aged 20, 26, 30, and 53 months. Treatment consisted of 16 intracerebral and cerebellar deposits of a recombinant adeno-associated viral vector encoding human α-N-acetylglucosaminidase (rAAV2/5-hNAGLU) plus immunosuppression. An intermediate report at 30 months was previously published. Thirty treatment-emergent adverse events were reported between 30 and 66 months after surgery, including three classified as severe with no serious drug reactions. At 5.5 years, NAGLU activity was persistently detected in the lumbar cerebrospinal fluid (18% of unaffected control level). Circulating T cells reacting against NAGLU peptides were present, indicating a lack of acquired tolerance. Patients 2, 3, and 4 showed progressive brain atrophy and neurocognitive evolution that did not differ from untreated Sanfilippo A/B children. Patient 1, enrolled at 20 months of age, had a milder disease with normal brain imaging and a significantly better cognitive outcome than the three other patients and untreated patients, although not equivalent to normal children. After 5.5 years, the primary endpoint of this study was achieved with a good safety profile of the proposed treatment. We have also observed sustained enzyme production in the brain and absence of immunological tolerance. Cognitive benefit was not confirmed in the three oldest patients. Milder disease in the youngest patient supports further investigations of adeno-associated vector-mediated intracerebral gene therapy in Sanfilippo B.
Introduction
Sanfilippo B or mucopolysaccharidosis type IIIB (MPS IIIB) is a severe neurodegenerative condition where the lysosomal α-N-acetylglucosaminidase (NAGLU) catalytic activity is impaired by mutations in NAGLU. Usually, in these children, neurological development is normal until 2 years and thereafter neurological impairment occurs progressively. Therapeutic trials in affected children aim at delivering the lacking enzymatic activity especially in the brain. Intravenous infusion of recombinant NAGLU was not successful (NCT02324049). Currently ongoing investigations focus on intracerebroventricular infusion of a chimeric enzyme (NCT02324049) or peripheral infusion of gene therapy vectors having some capacity to cross the blood–brain barrier (NCT03315182).
According to preclinical studies that we previously performed in MPS IIIB mice 1 and MPS IIIB dogs, 2 we were allowed by the regulatory authorities to enroll four children in a uncontrolled, phase 1/2 clinical trial of intracerebral gene therapy combined with immunosuppression. The treatment protocol consisted of 16 surgical deposits of an adeno-associated vector encoding NAGLU (rAAV2/5-hNAGLU) in the subcortical white matter and cerebellum. An intermediate report at 30 months concluded that the treatment was well tolerated, including normal brain imaging 3 months after surgery. 3 NAGLU produced by genetically modified cells was detectable in the cerebrospinal fluid (CSF). Circulating CD4 and CD8 lymphocytes responding to NAGLU peptides and producing tumor necrosis factor α (TNFα) were detected, suggesting differentiation into effector lymphocytes, although a combined immunosuppressive regimen prevented overt immune reaction. 4 Neurocognitive progression seemed to have improved, especially in the youngest patient who was <2 years old at enrollment. We report here the final result of this study after a 66-month follow-up (5.5 years), which confirms the previously shown excellent safety profile of the treatment and the observed partial efficacy in the youngest patient.
Patients and Methods
Primary endpoints, study design, and patients
Primary endpoints of this uncontrolled, phase 1/2 clinical trial were the occurrence, intensity, and causality of treatment-emergent adverse events (TEAEs). Secondary endpoints were the definitions of exploratory tests that could become evaluation criteria for further efficacy studies.
Study design, inclusion/exclusion criteria, and neurosurgical procedures were previously described. 3 Four children aged 20 (patient 1), 26 (patient 2), 30 (patient 3), and 53 (patient 4) months were enrolled between September 17, 2013, and April 7, 2014. Main characteristics at diagnosis and inclusion were previously reported (shown again here as Supplementary Table S1).
Treatment consisted of 16 intraparenchymal deposits (12 within the brain and 4 within the cerebellum) of rAAV2/5, plus immunosuppressive therapy. The vector used was produced by uniQure in the Sf9 cell line and is similar to the one used by Ellinwood et al. 5 Immunosuppression was started 14 days before surgery (0.2 mg/Kg tacrolimus and 1,200 mg/m2 mycophenolate mofetil per day, orally). Mycophenolate mofetil was maintained for 6 weeks after surgery, and tacrolimus was progressively reduced and was the only treatment maintained during whole study. Safety, tolerance, neurocognitive progression, brain growth as evaluated by brain magnetic resonance imaging (MRI), NAGLU enzymatic activity in CSF, circulating T cells responding to NAGLU, and anti-AAV5 antibody were measured serially before and after surgery, as previously described. 3,4
Tacrolimus dosage was adjusted during the extension phase to obtain trough blood concentrations of 4–6 ng/mL. All adverse events were recorded by monthly contacts with families. Local practitioners in contact with investigators evaluated clinical aspects, routine hematology, and biochemistry every 6 months. Evaluations performed every 18 months (48 and 66 months after surgery) at the investigation center also included neurocognitive testing; brain MRI; cardiac ultrasonography; electrocardiogram; abdominal echography; tacrolimus dosage; varicella zoster virus, Epstein Barr Virus, and cytomegalovirus viral serology; and immunomonitoring (immunophenotyping, circulating T cells responding to NAGLU, and cytokine assessments 4 ). Neutralizing anti-AAV5 antibodies were absent at 30 months and not further measured. Protein and glucose concentrations, cell counts, and NAGLU catalytic activity levels were determined in CSF samples collected at 48 and 66 months. High heparan sulfate concentrations were detected in lumbar CSF throughout the initial follow-up and were not measured thereafter.
Neuropsychiatric/cognitive assessments
The four enrolled children were subjected to the same series of neuropsychological tests at baseline and every year over the 5.5-year follow-up period. They included the Brunet–Lezine revised test, equivalent, but not identical, to the Bayley test; the Wechsler Preschool and Primary Scale of Intelligence III (WPPSI-III); the Vineland Adaptive Behavior Scale (Vineland-I test); and the PEP-3 test (Psychoeducational Profile, 3rd edition). The same trained neuropsychologist performed all tests during the study. Considering the cognitive performance of patient 1, the Brunet–Lezine revised test (designed for children up to 30 months of age) and the WPPSI-III test were used together at 30 months, and the WPPSI-III test was used alone at 48 and 60 months. Trajectories of neurocognitive development and developmental quotients (DQs, ratio of developmental age to chronological age × 100) were recorded. Data were subsequently compared with reported measures in 19 and 8 untreated severe MPS IIIA and MPS IIIB cases, respectively. 6,7 All comparison values were analyzed together to calculate the regression coefficient (DQ MPS IIIA + MPS IIIB, R 2 = 0.94193) and to draw the reference regression curve for untreated patients (red, expon. DQ MPS IIIA + MPS IIIB). Regression coefficients were also calculated for DQ values of treated patients (DQ of patients 1, 2, 3, and 4; n = 4 values for each patient; R2 coefficients are indicated in Fig. 2). Each patient DQ value was compared with the mean of all control values measured in the same 1-year window using one-sample t-tests.
Standard protocol approvals, registrations, and patient consent
The study was approved by the Agence Nationale de Sécurité du Médicament et des Produits de Santé and the ethics committee of Comité de Protection des Personnes Île-de-France II and was endorsed by two parent associations, Association Française contre les Myopathies and Vaincre les Maladies Lysosomales. All parents have provided written informed consent. An international independent data monitoring committee assessed safety data. The trial was registered with EudraCT, number 2012-000856-33; International Standards for Clinical Trial Registries, number ISRCTN19853672; and Clinical trial.gov, number NCT03300453.
Results
Clinical examination findings showed mild progression over the 5.5-year follow-up period. The four enrolled children developed moderate valvular dysfunction detected on the systematic heart ultrasonographies performed at the age of 51 months (patient 1), 26 months (patient 2, at inclusion), 43 months (patient 3), and 104 months (patient 4) in the absence of clinical symptoms. Liver size increased moderately in the four patients (mean increase = 3.2 ± 0.9 cm) between the 30th month and the end of follow-up. Splenomegaly was detected at clinical examination of patient 4 at inclusion and by ultrasonography in patient 1 at 87 months of age and patient 3 at 43 months of age. Kidney measures remained stable in the four patients. A total number of 30 TEAEs were reported between the 30th and 66th month of follow-up, compared with 117 during the initial period of the study (Table 1). Three adverse events were classified as severe due to a short hospitalization: one moderate gastroenteritis event needing an hospitalization in patient 3 and another severe in patient 2 (tacrolimus was transiently stopped for 1 week due to its high blood level during these events); patient 4 underwent an operation for nasal polyps, which was considered as a severe adverse event. None of these three events were considered to be related to study treatment. No suspected unexpected serious adverse drug reactions were reported. The other 27 TEAEs observed between 30 months and the end of the study were of the same type as those observed in the initial period of the study (Table 1).
Comparison of nonsevere treatment-emergent adverse events recorded initially and from 30 to 66 months after surgery
As published (1).
Twenty-five adverse events were classified as grade 1 and two as grade 2.
Anemia, increased EBV DNA.
Bronchitis (n = 3), cough (n = 1), fever (n = 2), conjunctivitis (n = 1), sleeping disorders (n = 1), and atopic dermatitis (n = 1).
ALAT, alanine transaminase; EBV, Epstein Barr virus.
NAGLU catalytic activity levels measured in patient's CSF at 48 and 66 months were equivalent to levels at the initial period of the study (values at 66 months were 13.7 ± 0.9 nmol/H/mL, 10 ± 0.6 nmol/H/mL, 8.3 ± 1 nmol/H/mL, and 9.6 ± 0.5 nmol/H/mL for patients 1, 2, 3, and 4, respectively) and remained higher than those at baseline for each patient. These values correspond to an average of between 14% and 24% of levels detected in unaffected children (57 ± 12 nmol/H/mL, n = 4). They were equivalent in the four enrolled patients (Supplementary Table S2 and reference 3 ).
Circulating CD4 and CD8 T lymphocytes undergoing proliferation and/or TNFα production when exposed to NAGLU or NAGLU-derived peptides were detected in the four patients at 48 and 66 months. 3,4 This result indicates the long-term persistent circulation of memory and effector CD4 and CD8 T lymphocytes previously primed to react against NAGLU and testifies to the lack of induced tolerance.
General and neurological assessments of patient 1 showed improvements in everyday activities, school participation, and behavior. She is presently able to follow the first grade of elementary school at the age of 6 and half years, although with need for individual help. Patients 2 and 3 are in a special needs school with behavioral disturbances for patient 3, while patient 4, at the age of 10 years, has marked cognitive deficit and behavioral disturbances, while still ambulatory. Figure 1 represents the trajectories of cognitive development by age of the four children during the 66 months of follow-up, as measured by three different neuropsychological tests with consistent results for each patient. Patient 1 persistently acquired skills over the 66 months of follow-up, although not at the same rate as normal children. Patients 2, 3, and 4 did not acquire new skills and their performance declined with time. Figure 2 shows regression analysis of DQs measured by the Brunet–Lezine/WPPSI and the Vineland tests, compared with reported values in untreated severe MPS IIIA and MPS IIIB children. 6 –9 Results indicate significantly higher performance of patient 1 at each time point compared with the natural history of the disease. In contrast, the disease course in patients 2, 3, and 4 was similar to the reference population.

Trajectories of neurocognitive development by age during follow-up. Cognitive growth trajectory of developmental age in the four children is compared with that in unaffected children and with the mean expected trajectory of rapidly progressing MPS IIIA patients. Arrows indicate time of treatment. MPS, mucopolysaccharidosis.

Analysis of developmental quotients. Cognitive scores measured yearly in the four patients using the Brunet–Lezine test
In accordance with observations made at earlier stages, MRIs performed at 48 and 66 months did not show any image of possible scar or residual inflammatory reaction attributable to surgery. Brain imaging was normal in patient 1 without brain atrophy, whereas brain atrophy was present in patients 2, 3, and 4, as indicated by increased ventricle and pericerebral space sizes assessed by semiautomated measurement of the total CSF volume and CSF in the ventricles using Carestream Vue PACS, version 12.1.6.0117, on 3D-T2 images (Fig. 3).
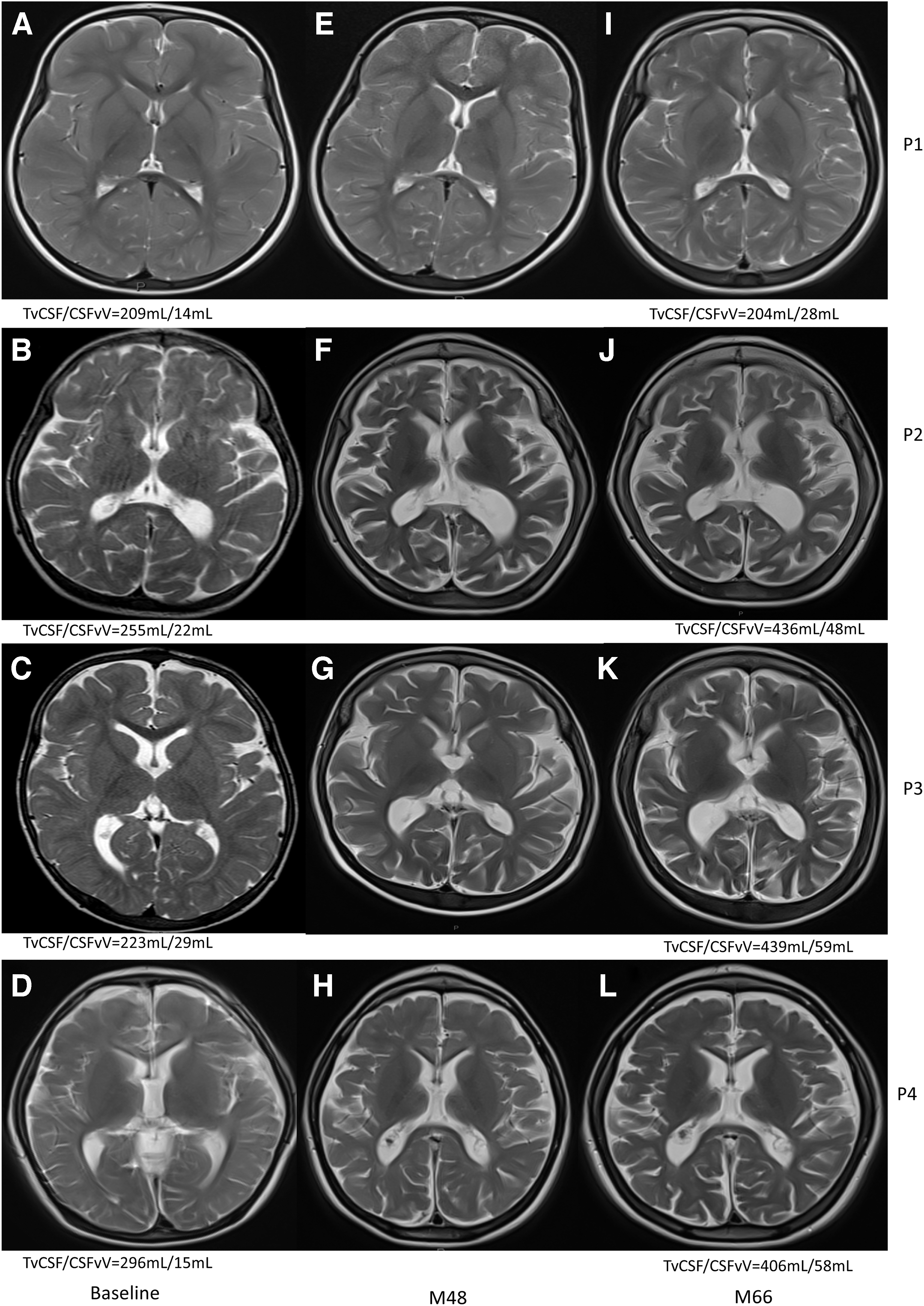
Axial T2-weighted brain MRI scans of the four patients at inclusion
Discussion
In this uncontrolled, phase 1/2 clinical trial, we have shown that intracerebral gene therapy using adeno-associated vector encoding NAGLU combined with immunosuppression has a very good safety profile after long-term follow-up in the four included children. Sustained enzyme production in the brain and absence of immunological tolerance were observed. Milder disease was noticed in the youngest patient, while cognitive benefit was not confirmed in the three oldest patients.
Study endpoints
Surgical vector delivery into the brain parenchyma, including in the cerebellum, AAV5-mediated transgenesis of brain cells, and enzyme expression in brain tissue were not associated with adverse events, indicating excellent long-term safety of the gene therapy procedure. In accordance with our previous preclinical observations in deficient dogs, 5,10 the evidence for circulating anti-NAGLU-responsive CD4 and CD8 T cells producing TNFα, and absence of immune tolerance induction after 66 months, confirms that immunosuppression was mandatory to prevent overt immune reaction in the brains of all treated patients. However, three severe adverse events occurring in two patients were associated with increased titration of tacrolimus and possibly related to immunosuppression. They were fully reversed after transient interruption of the immunosuppressant. Taken together, these results indicate that the treatment protocol is safe and therefore acceptable for larger studies.
NAGLU activity in lumbar CSF samples is a relevant marker of the efficiency of AAV5-mediated intracerebral gene transfer. Stable levels equivalent to roughly 20% of unaffected children over the 66-month follow-up period indicate long-term gene expression and NAGLU production. However, it is likely that NAGLU activity is not evenly distributed within treated patient's brain tissue, as suggested by preclinical studies in dogs showing concentration gradients centered on vector deposition sites. 5,10 Preclinical studies in dogs also showed persistent pathology in meninges and choroid plexus associated with high glycoaminoglycans concentration in the CSF, which contrasted with detectable NAGLU activity in this fluid. We therefore assume that normal CSF composition and flow were not normally restored in treated children and that pathology persisted in meninges. Preclinical studies in treated dogs also showed persistent pathology in endothelial cells, possibly causing partial obstruction of the brain microcapillary lumen. It is therefore possible that altered brain blood perfusion dynamic persisted in treated patients.
It is accepted that trials involving invasive intervention in MPS III patients can be conducted without a formal comparator group due to rarity and severity of the disease provided that a detailed description of the natural history is available and can be used to measure outcomes 11 and cognitive development.
We used brain imaging as an indicator of the progression of brain pathology and neurodegeneration. Brain atrophy is commonly observed in MPS IIIB children after the age of 40–50 months, although difficult to quantify. 12 Patient 4 had mild brain atrophy at inclusion (53 months). Evidence of brain atrophy appeared between 56 (30 months after surgery) and 74 months of age (48 months after surgery) in patient 2 and between 42 and 60 months of age (12 and 30 months after surgery) in patient 3, indicating that treatment did not stop the disease process in the brain. Conversely, patient 1 had normal brain imaging with no sign of atrophy on the last MRI performed at the age of 86 months (66 months after surgery).
Our appreciation of the neurocognitive progress greatly benefited from the detailed description of cognitive performance in young untreated MPS IIIA and MPS IIIB patients. 6,7 We used a similar protocol. The evolution of cognitive skills in patients 2, 3, and 4 was within the range of published data for untreated MPS III patients, indicating that treatment had little or no impact on cognitive performance. In contrast, performance of patient 1 was significantly better and also better than that published for untreated MPS III patients. They were nevertheless not equivalent to a normal child, leading to progressive lowering of DQ. Combined with MRI data, this result indicated milder disease progression in patient 1.
Why did enzyme delivery in the brain fail to modify the natural course of the disease in patients 2, 3, and 4?
There is strong evidence for remarkable improvement of clinical outcomes in patients with different types of MPS receiving enzyme replacement therapy. However, whatever the disease type and main target tissue, treatment efficacy is always optimal when initiated very early in life. 13 The age limit for efficient intervention to prevent lysosomal storage lesions in the brains of MPS III patients is currently unknown. In our preclinical studies in MPS I and MPS IIIB dogs, 5,10 clearance of storage lesions in the brain was almost total when treatment was performed immediately after weaning and almost inexistent in animals treated at 8 months of age. In humans, treatment performed beyond 24 months of life, as in patients 2, 3, and 4 (at 26, 30, and 53 months, respectively), may be too late to prevent or reduce disease-induced brain damage. Delivery of the therapeutic enzyme early in the course of the disease is likely mandatory to prevent and/or clean brain storage lesions and to improve the natural course of the disease.
However, one might expect that delivery of a therapeutic enzyme would at least stop the disease process once delivered, preventing further deterioration. This was not the case in patients 2, 3, and 4, whose cognitive skills declined after 60 months of age. Therapeutic enzyme levels in patient's brain tissue might have been too low for efficient cleaning and/or prevention of lysosomal storage lesions, at least at certain brain locations, although preclinical observations in affected dogs do not support this hypothesis. 5,10 Other hypotheses include persistent pathology in meninges and microvessel walls, as well as the lack of correction of blood and/or CSF-brain perfusion defects. In addition, we cannot exclude that persistent pathology outside the brain contributed to disease progression in the brain through other mechanisms, including alterations of microbiota. 14 –16 A combination of these factors may have triggered a neurodegenerative process that further evolved autonomously, leading to deterioration independently of the presence of NAGLU activity in brain tissues. This hypothesis further emphasizes the importance of very early treatment. Another possibility would be that intraparenchymal delivery of the vector alone would not be sufficient to saturate the target nerve cells, and a combination of other possible deliveries (e.g., intravenous) may help to obtain/access all cells and organs that may intervene in the disease evolution.
Was the milder disease observed in patient 1 a consequence of the treatment?
It is tempting to consider that the disease process would have been more severe in patient 1 without earlier treatment inducing a partially restored NAGLU activity early in life. The main argument supporting this view is the presence in this patient of the same two mutations in the NAGLU gene (c.214-237dup and W540X) that were associated with the severe disease course in her brother. Cognitive acquisition in patient 1, although better than in the reference untreated population, was slower than in nonaffected children, leading to progressive lowering of her DQ with age. However, she was still able to acquire new skills at 7.2 years and had not started to deteriorate at the end of the study follow-up.
An alternative hypothesis to account for a milder form of the disease in patient 1 is the possibility that her genetic background carries modifier genes, not present in her brother, which may alleviate the severity of the disease. 17 –19 This hypothesis cannot be excluded at this stage.
A different immune response inducing better tolerance may also be another explanation as we have previously observed a low level of and less differentiated circulating NAGLU-specific CD4+ and CD8+ T cells without proinflammatory cytokines in the CSF in patient 1. 4 This could be related to an age-dependent level of differentiation of NAGLU-specific T lymphocytes.
A definitive conclusion will therefore have to wait for longer follow-up of patient 1 and, more importantly, for the setting up of additional trials specifically designed for efficacy assessment in very young children.
Conclusions
After completion of 5.5 years, the follow-up of the four patients enrolled in this study demonstrates that the trial protocol was well suited to reach endpoints, demonstrating good safety compatible with future larger studies and indicating exploratory markers for efficacy assessment. The study also provides indications to increase the chance of success: treatment performed early in life, likely before 2 years of age and even better soon after birth, and delivery of the therapeutic enzyme not only into the brain but also into peripheral organs, including meninges, choroid plexus, and brain microvasculature.
Footnotes
Authors' Contributions
M.T., J.-M.H., M.Z., J.A., K.D., M.-L.G., and B.P.-B. conceptualized and designed the study, drafted the initial article, and reviewed and revised the article. D.Z., G.P., B.H., and S.D.B. coordinated and supervised data collection and critically reviewed the article for important intellectual content. All authors approved the final article as submitted and agree to be accountable for all aspects of the work.
Acknowledgments
The authors thank the four families and the nurses for granting permission for and helping them in treating the enrolled patients.
Author Disclosure
M.T. and S.D.B. have received consulting fees from uniQure during the early phase of the study. M.Z. is a participant in a concomitant MPS IIIA trial sponsored by Lysogene®. K.D., J.A., B.H., M.-L.G., B.P-B., D.Z., G.P., and J.-M.H. have nothing to disclose. No honorarium was given to anyone to produce the article.
Funding Information
This study was supported by uniQure, Association Française contre les Myopathies, Institut Pasteur, and Vaincre les Maladies Lysosomales. The study was sponsored by Institut Pasteur during the first 30 months and by uniQure during the following 36 months. The sponsors had no involvement in collection of data, interpretation of data, and writing of the report.
Supplementary Material
Supplementary Table S1
Supplementary Table S2
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.