
Abstract
Based on recent success in using modified RNA in clinical applications, we tested the safety, feasibility, and efficacy of direct delivery of citrate-saline-formulated mRNA into an hibernating ischemic heart muscle using an electromechanical mapping and injection catheter system (NOGA/Myostar) in a porcine chronic myocardial ischemia model. Chronic ischemia was induced in domestic pigs (n = 24) using a bottleneck stent placed in the left anterior descending coronary artery. Low (1 mg) and high (7.5 mg) doses of citrate-saline-formulated vascular endothelial growth factor (VEGF)-A165 mRNA were administered in the study. LacZ mRNA and citrate-saline buffer were used as controls. Ten intramyocardial injections (200 μL each) of the mRNAs or citrate-saline buffer were given endovascularly into the hibernating ischemic myocardium using the NOGA catheter. Positron emission tomography 15O-radiowater imaging was performed 7 days after the induction of ischemia and 28 days after the mRNA delivery to measure quantitative myocardial blood perfusion. Coronary angiography, left ventricular function measurements, and clinical chemistry were obtained at each time point. Thirty-five days after the mRNA transfers, pigs were sacrificed, and infarct size and general histology were analyzed. LacZ mRNA pigs were sacrificed 24 h after the transduction. Citrate-saline-formulated mRNA delivery into the ischemic myocardium with endovascular injection catheter did not lead to meaningful transduction with the translation of VEGF-A165, nor therapeutic effects in the heart. VEGF-A165 mRNA showed no statistically significant improvements in left ventricular ejection fraction (LVEF), cardiac output, myocardial perfusion, infarct size, collateral growth, or capillary area in the study groups. However, there was a trend in the high-dose group toward an improved LVEF and cardiac output at rest. No significant adverse effects were observed. In conclusion, the NOGA/Myostar injection catheter system is ineffective in delivering citrate-saline-formulated mRNAs into the heart muscle with the doses and methods used in a porcine chronic myocardial ischemia model.
Introduction
Coronary artery disease (CAD) is still a major clinical problem worldwide. 1 In addition to pharmacological therapy, CAD is treated with coronary angioplasty, stenting, and bypass surgery. Unfortunately, many elderly and comorbid patients are not eligible for these operations. 2,3 Thus, there is an urgent need to develop new, minimally invasive therapies for CAD. Proangiogenic gene therapy could offer an alternative treatment strategy for these patients. 4 –6 In the light of recent successful applications of mRNA in the clinics, 7 –11 mRNA-based products could be used for proangiogenic gene therapy in severe CAD patients.
Vascular endothelial growth factors (VEGFs) induce efficient angiogenesis and arteriogenesis, and are potential candidates for proangiogenic therapies. 4,5,12 In previous preclinical and clinical studies, the most commonly used vectors to transduce the myocardium have been plasmids and adenoviruses with a short-expression profile and adeno-associated viruses, which can cause a long-term gene expression. 4 Modified mRNA is a nonviral alternative for cardiac gene therapy hypothesized to induce an adequate VEGF-A production profile that would last long enough to induce functional angiogenesis but not overexpressing VEGF-A to induce potentially leaky vessels. It differs from native mRNA in having a longer half-life in the cytoplasm than the native mRNA. 13 Previously, direct intramyocardial injections of VEGF-A165 mRNA have been shown to reduce mortality and improve myocardial function by inducing angiogenesis and reducing infarct scar size in mice. No adverse effects, such as apoptosis or innate immune response, were detected. 14 In a chronic porcine infarction model, epicardial injections of VEGF-A165 mRNA improved systolic cardiac function and myocardial relaxation, induced angiogenesis, and decreased myocardial fibrosis. Also, this study showed safety and minimal immunogenicity of mRNA therapy. 15
In the current study, we evaluated the safety and efficacy of percutaneous catheter-mediated VEGF-A165 mRNA gene transfer in the porcine chronic ischemia model precisely in the same way as it would be conducted in the clinical catheterization laboratory for human CAD patients using the NOGA/Myostar system. It was found that VEGF-A165 mRNA showed no statistically significant improvements in cardiac functions and myocardial pathology, although there was a numerical trend in the high-dose group toward an improved left ventricular ejection fraction (LVEF) and cardiac output at rest. No adverse effects were observed. However, since LacZ mRNA did not show any detectable gene expression 24 h after the transduction, indicative that VEGF-A165 mRNA neither resulted in transduction nor VEGF-A production, we conclude that NOGA/Myostar catheter delivery of mRNA with the current procedure and formulation tested is not the best option for CAD patients.
Materials and Methods
Overview
VEGF-A165 mRNA gene transfers were evaluated in a porcine chronic ischemia model, 16 and the study included VEGF-A165 mRNA concentration of 3.75 mg/mL in a citrate-saline buffer as the high-dose group (7.5 mg n = 7), 0.5 mg/mL in a citrate-saline buffer as the low-dose group (1 mg n = 7), and the citrate-saline group as a control (n = 8). In addition, LacZ mRNA (2 mg) was administered as an additional control, and animals (n = 2) were sacrificed 24 h after the transduction to measure transgene expression. All experiments were done using female domestic pigs (25 kg). Pigs were chosen randomly to study groups after the ischemia operations, and all groups remained blinded for the investigators until all animal experiments, laboratory work, and analyses were completed (Fig. 1). mRNAs were manufactured as previously described. 9,15,17
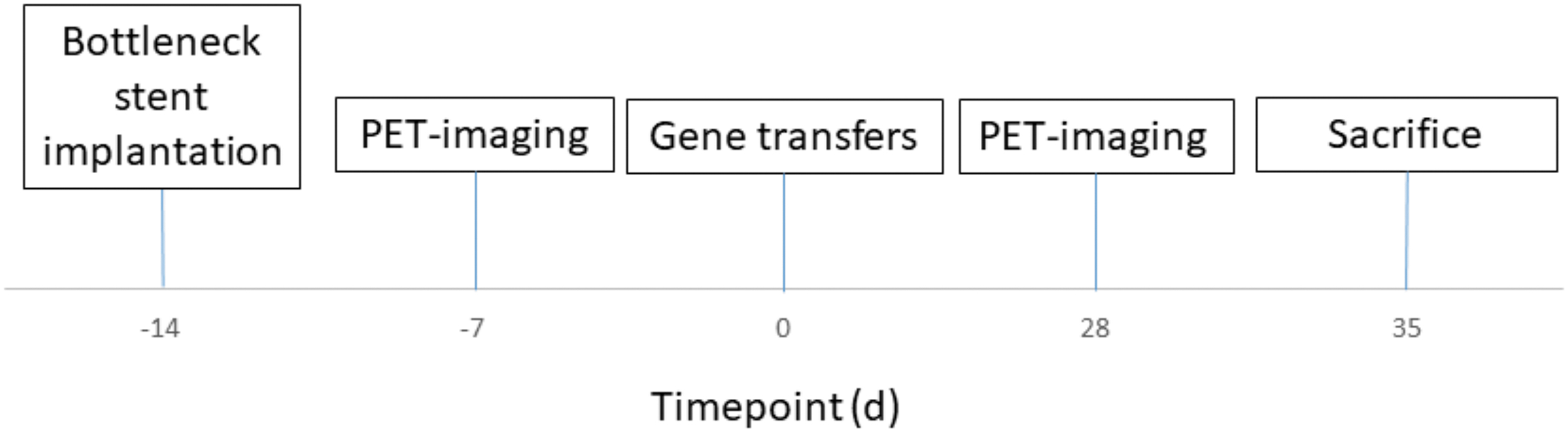
Time points. Color images are available online.
Animal experiments
Pigs received daily 200 mg of amiodarone (Cordarone®; Sanofi-Aventis, Helsinki, Finland) and 2.5 mg of bisoprolol (Bisoprolol ratiopharm; Ratiopharm GmbH, Ulm, Germany) to prevent fatal ventricular arrhythmias. The medication started 1 week before the ischemia operation and was continued daily until the end of follow-up. Before the procedures, pigs were sedated with an intramuscular injection of 1.5 mL atropine (1 mg/mL; Leiras, Helsinki, Finland) and 6 mL of azaperone (Stresnil® 40 mg/mL; Janssen Pharmaceutica N.V., Beerse, Belgium). After the initial sedation, animals were put under general propofol (Propofol-Lipuro 20 mg/mL; B. Braun, Melsungen, Germany) and fentanyl (Fentanyl™ 50 μg/mL; Janssen-Cilag, Espoo, Finland) anesthesia with doses of 15 mg/kg/h and 10 μg/kg/h, respectively. After a 5-week follow-up, animals were sacrificed with an overdose of potassium chloride and propofol. All animal experiments were approved by the Animal Experiment Board in Finland.
Ischemia
One day before the ischemia operation, the animals received loading doses of clopidogrel (300 mg, Clopidogrel Mylan; Mylan S.A.S., Saint Priest, France) and acetylsalicylic acid (300 mg, ASA-Ratiopharm; Ratiopharm, Espoo, Finland) to prevent acute in-stent thrombosis after the stent placement. At the beginning of the ischemia operation, animals received 100 mg of lidocaine i.v. (Lidocain 10 mg/mL; Orion Pharma, Espoo, Finland) and 2.5 mL of MgSO4 intravenously (i.v.). (Addex-magnesiumsulfate 246 mg/mL; Fresenius Kabi, Uppsala, Sweden) to prevent ventricular arrhythmias and 30 mg of enoxaparin i.v. (Klexane®; Sanofi-Aventis). To induce chronic myocardial ischemia, a bottleneck stent was placed in the proximal part of the left anterior descending artery (LAD) as previously described.
16
Briefly, the bottleneck stent consists of a bare-metal stent (Coroflex® Blue,
mRNA transfer
mRNA transfers were done 14 days after the ischemia operation when chronic ischemia was stabilized and acute endogenous responses were attenuated. For the gene transfers, the MyoStar® intramyocardial injection catheter system (Biosense Webster, a Johnson & Johnson company, Diamond Bar, CA) was introduced to the left ventricle via an 8 F femoral sheath. Under fluoroscopic guidance and using the NOGA mapping system, an electroanatomic map of the left ventricle was acquired. Using this map as a guide, 10 injections (200 μL each) were injected into the left ventricle of the myocardium to the hypokinetic but still viable areas. 18,19 This area corresponds to the viable but hibernating myocardium, with the greatest likelihood to respond to the therapy. For viability, a unipolar voltage over 5 mV was used as a criterion. For hypokinesia, a local linear shortening as low as available was selected, typically at least below 12% but preferably below 6%. The injection needle length was set to 3–4 mm. The injections were kept at 30 s, and the injection needle was held inside the myocardium for 5 s after the injection before pulling the needle out. No priming with the drug product was performed.
Ejection fraction and cardiac output
LVEF was measured using the angiogram workstation ventricle analysis program (Innova 3100IQ; GE Healthcare) from the cine radiograms of the left ventricle filled with contrast medium. Animals were imaged at baseline, before mRNA transfers, and 35 days after the transfer. LVEF, stroke volume, end-diastolic volume, and end-systolic volume were estimated using Simpson's method. Cardiac output (CO) was calculated using the stroke volume from the left ventricular cine radiograms and heart rate. Parameters were measured both at rest and stress. Pharmacological stress was induced using i.v. dobutamine (Dobumin Hameln 12.5 mg/mL; Hameln Pharma Plus Gmbh, Hameln, Germany) infusion starting at 10 μg/kg/min and increasing the dose if needed until the heart rate of 160 bpm was reached.
Rentrop scoring
The Rentrop classification of the filling of the LAD with contrast medium was used for the analysis of collaterals from the right coronary artery (RCA) and left coronary artery (LCA), the latter consisting of bridging antegrade collaterals from the LAD and collaterals from the left circumflex artery. In the Rentrop classification, 0 corresponds to no filling of any collateral arteries, 1 corresponds to the filling of the side-branches of the LAD, 2 corresponds to the partial filling of the LAD main vessel, and 3 corresponds to the complete filling of the LAD main vessel. The final Rentrop score is the sum of the values for both RCA and LCA. 20
Positron emission tomography imaging
The animals were imaged at baseline, 1 week after the ischemia operation, and at the end time point 4 weeks after the gene transfer using a positron emission tomography (PET) scanner for regional myocardial perfusion with 15 O-radiowater. 21,22 The treatment area where the injections were given was identified by comparing the NOGA maps from the gene transfer operations with the PET perfusion maps. 18 Remote areas where no injections were given were used as control. Global perfusion is the average perfusion of the left ventricle.
PET studies were performed using an ECAT EXACT HR+ scanner (Siemens-CTI, Knoxville, TN). Myocardial perfusion was evaluated by PET 15 O-radiolabeled water (805 ± 87 MBq) both at rest and during pharmacologic stress. The pharmacologic stress was induced with i.v. adenosine at the rate of 200 μg/kg/min (Adenosin Life Medical, Life Medical Sweden AB, Stocksund, Sweden) combined with phenylephrine 5 μg/kg/min (Fenylefrin Abcur, Abcur AB, Helsingborg, Sweden) administered i.v. starting 2 min before imaging and continuing throughout the stress study to induce myocardial hyperemia. The phenylephrine was used to limit systemic hypotension due to the high adenosine dose, as the clinically used adenosine dose of 140 μg/kg/min is not high enough to induce maximal hyperemia in pigs. The acquisition frames were as follows: 14 × 5, 3 × 10, 3 × 20, and 4 × 30 s (total duration 4 min 40 s).
The acquired PET data were reconstructed in a two-dimensional (2D) mode with an iterative reconstruction algorithm ordered subset expectation maximization (OSEM) using 6 iterations and 16 subsets. The transaxial field of view (35 cm) was reconstructed in a 128 × 128 matrix, yielding a pixel size of 2.57 × 2.57 mm. The measurements were corrected for scatter, random counts, and dead time. The device produces 63 axial planes with a slice thickness of 2.43 mm. Regional myocardial perfusion (in mL/g/min) was measured using Carimas 2 software (Turku PET Centre, Turku, Finland).
Infarct size
To assess the amount of infarcted myocardium 35 days after the mRNA transfers, the heart was cut to five 10-mm-thick short-axis slices and stained with tetrazolium chloride as previously described.
16
The infarct size was calculated using ImageJ software (
Immunohistochemistry and capillary analyses
Tissue samples were collected from the gene transfer area and control area, lung, liver, spleen, kidney, and ovarian. The samples were fixed with 4% paraformaldehyde for 24 h at room temperature, incubated at 15% sucrose for 24 h, and then embedded in paraffin. Immunohistochemistry staining for vascular endothelium was detected with biotinylated lectin (Biotinylated Griffonia, Bandeiraea, Simplicifolia Lectin I; Vector Laboratories, Burlingame, CA) and visualized with 3,3′-diaminobenzidine (DAB). The average microvascular area (%), capillary count, and capillary area (μm2) were evaluated from the expected injection sites, that is, the maximal transduction area, and also infarct border zone and control area. Five microscopic images were taken per area from each animal using AnalySIS software (Olympus Soft Imaging Solutions, Münster, Germany). The border zone images were taken so that half of the image contained fibrotic tissue and half contained viable myocytes. The maximal transduction area was identified based on the injection sites in the NOGA maps. LacZ mRNA-transduced animals were sacrificed 24 h following the gene transfer, and samples were collected for histological analysis. Samples were processed as described above. The β-gal-positive nuclei were detected using an α-β-galactosidase primary antibody (Promega, Z378B) and visualized using a biotinylated α-mouse secondary antibody (Vectastain, BA-2000), HRP-conjugated ABC system (Vectastain, PK-6100), and DAB (Invitrogen, 002020). All images were taken from areas with the visually largest capillaries in the given tissue section and analyzed blindly without knowledge of the treatment group.
Statistics
Results are expressed separately for each individual animal in dot plots, a line indicating the average value for the group. Statistical significance was evaluated by an ordinary one-way analysis of variance (ANOVA), or a two-way ANOVA when appropriate, followed by Dunnett's post hoc test. The control group was used as a reference group in comparisons of the group differences. The p-value of <0.05 was considered statistically significant. Computations were performed with Prism 6 for MAC OS X, Version 6.0c (GraphPad Software, Inc., La Jolla, CA).
Results
Perfusion
No differences in absolute or relative perfusion or perfusion change over time from baseline to the last time point were observed in the treatment area at rest (Fig. 2A–C). At stress, there were no perfusion changes in the control or high-dose groups (Fig. 3A–C). However, the perfusion in the low-dose group decreased by 25% ± 35% during the follow-up, but the decrease was not statistically significant (p = 0.29).

Absolute myocardial perfusion, absolute perfusion change, and relative perfusion change at rest in different areas.
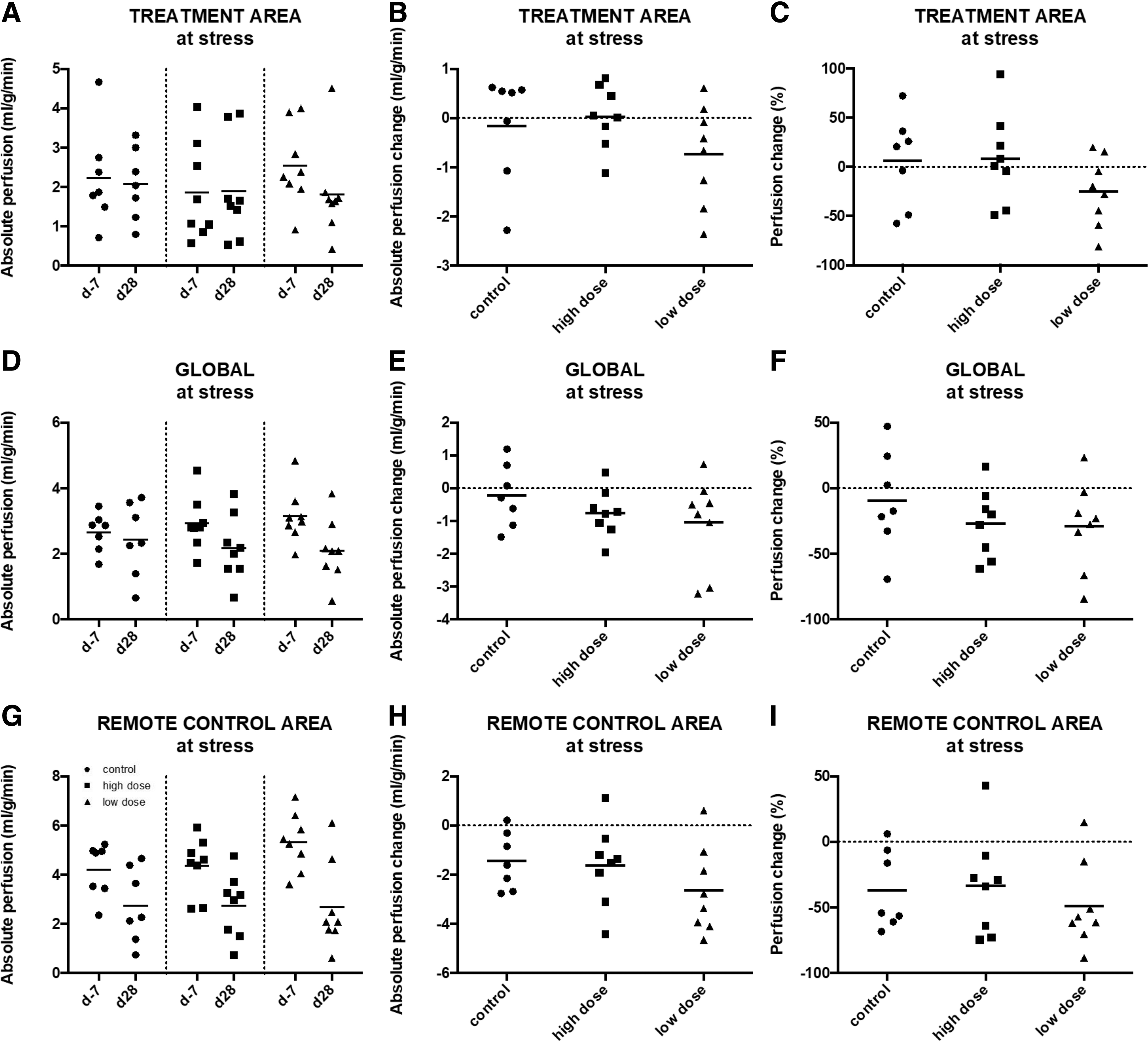
Absolute myocardial perfusion, absolute perfusion change, and relative perfusion change at adenosine-induced stress in different areas. There were no perfusion changes in the control or high-dose group in the treatment area
From baseline to the last time point, the global perfusion decreased significantly in the high-dose group (Fig. 2D–F). The absolute perfusion changed −0.26 ± 0.19 mL/g/min (p = 0.01) and the relative perfusion changed −24% ± 19% (p = 0.01) (Fig. 2F) during rest. Also, there was a trend toward lower perfusion in the low-dose group during rest, both absolutely −0.11 ± 0.17 mL/g/min (p = 0.10) and relatively −9.6% ± 16.5% (p = 0.10). However, these changes did not reach statistical significance. The control group was the only group where the perfusion at rest was increased during the follow-up time, 0.13 ± 0.30 mL/g/min absolutely and 18% ± 40% relatively. At stress (Fig. 3D–F), the perfusion was decreased in all groups without significant differences, −9.6% ± 38% for the control group, −27% ± 26% for the high-dose group, and −29% ± 34% for the low-dose group.
In the remote area at rest (Fig. 2G–I), the perfusion was decreased in the high-dose group by 24% ± 23% and in the low-dose group by 14% ± 9.1%, while only a minor change was seen in the control group (−2.9% ± 28%). None of these changes reached statistical significance. At stress (Fig. 3G–I), perfusion in the remote area was decreased almost equally in all groups, −37% ± 30% for the control group, −34% ± 39% for the high-dose group, and −49% ± 33% for the low-dose group. Changes did not reach statistical significance.
In all groups and time points, the absolute perfusion at rest averaged 1 mL/g/min in all areas, at stress 2–3 mL/g/min in the treatment area and globally. However, in the remote area at stress in all groups, the perfusion was 4–5 mL/g/min at baseline and decreased to 2–3 mL/g/min after 5 weeks. The representative polar maps from the radiowater-PET perfusion measurements are shown in Fig. 4.
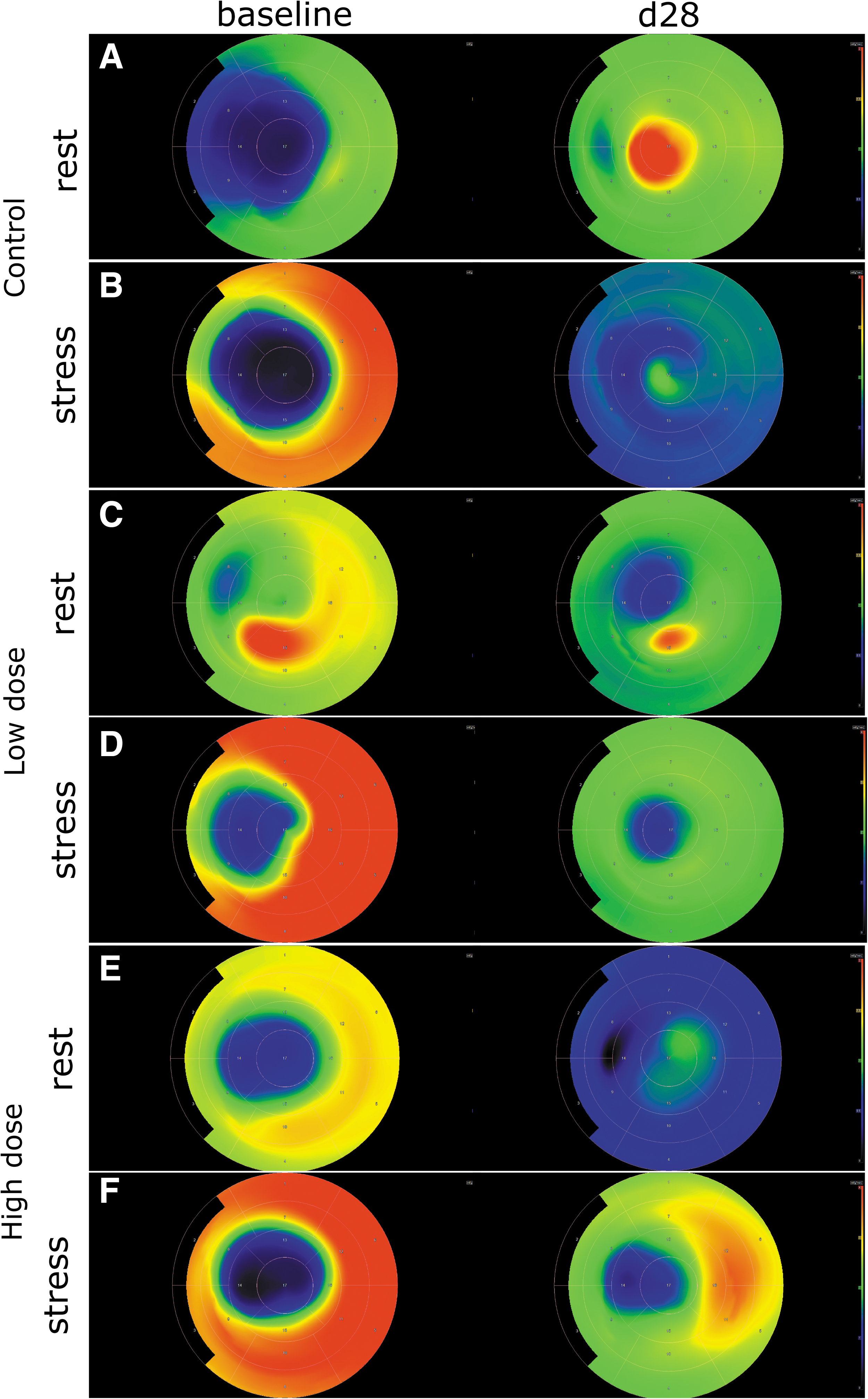
The representative polar maps from the radiowater-PET perfusion measurements for the control
Left ventricular function
After the ischemia operation, the average LVEF at rest (Fig. 5A, B) was 43% ± 6.2% in the high-dose group, 47% ± 7.4% in the low-dose group, and 51% ± 8.1% in the control group. During the follow-up, the LVEF increased to 48% ± 10.7% in both the high-dose and low-dose groups, while it decreased to 50% ± 8.5% in the control group. However, the increase of LVEF was not statistically significant in the high-dose group or the low-dose group (p = 0.38 and p = 0.84, respectively). At stress (Fig. 5C, D), the average LVEF was 60% ± 10.7% in the high-dose group and 65% ± 6.2% in both the low-dose and the control groups after ischemia. One month after the treatment, the LVEF decreased in all groups, to 59% ± 8.5% in the high-dose group, to 62% ± 10% in the low-dose group, and 60% ± 9.9% in the control group. These decreases were not statistically significant.

LVEF at different time points and LVEF change from time dosing and 5 weeks later during rest and stress. After the ischemia operation, the average LVEF at rest
Similarly, after the ischemia operation, the average CO at rest (Fig. 6A, B) was 2.5 ± 0.8 L/min in the high-dose group, 2.9 ± 0.8 L/min in the low-dose group, and 3.4 ± 0.9 L/min in the control group. CO increased to 4.3 ± 1.9 L/min in the high-dose group, 3.4 ± 1.0 L/min in the low-dose group, and 4.1 ± 1.7 L/min in the control group 1 month after the treatment. However, increases were not statistically significant. After ischemia, the average CO was 6.0 ± 1.5 L/min in both the high-dose and low-dose groups and 7.0 ± 1.7 L/min in the control group at stress (Fig. 6C, D). One month after treatment average, CO was 8.2 ± 2.7 L/min in the high-dose group and 7.9 ± 2.3 in the low-dose and control groups. There were no statistical differences between the groups or changes between before and after the treatment within each group.
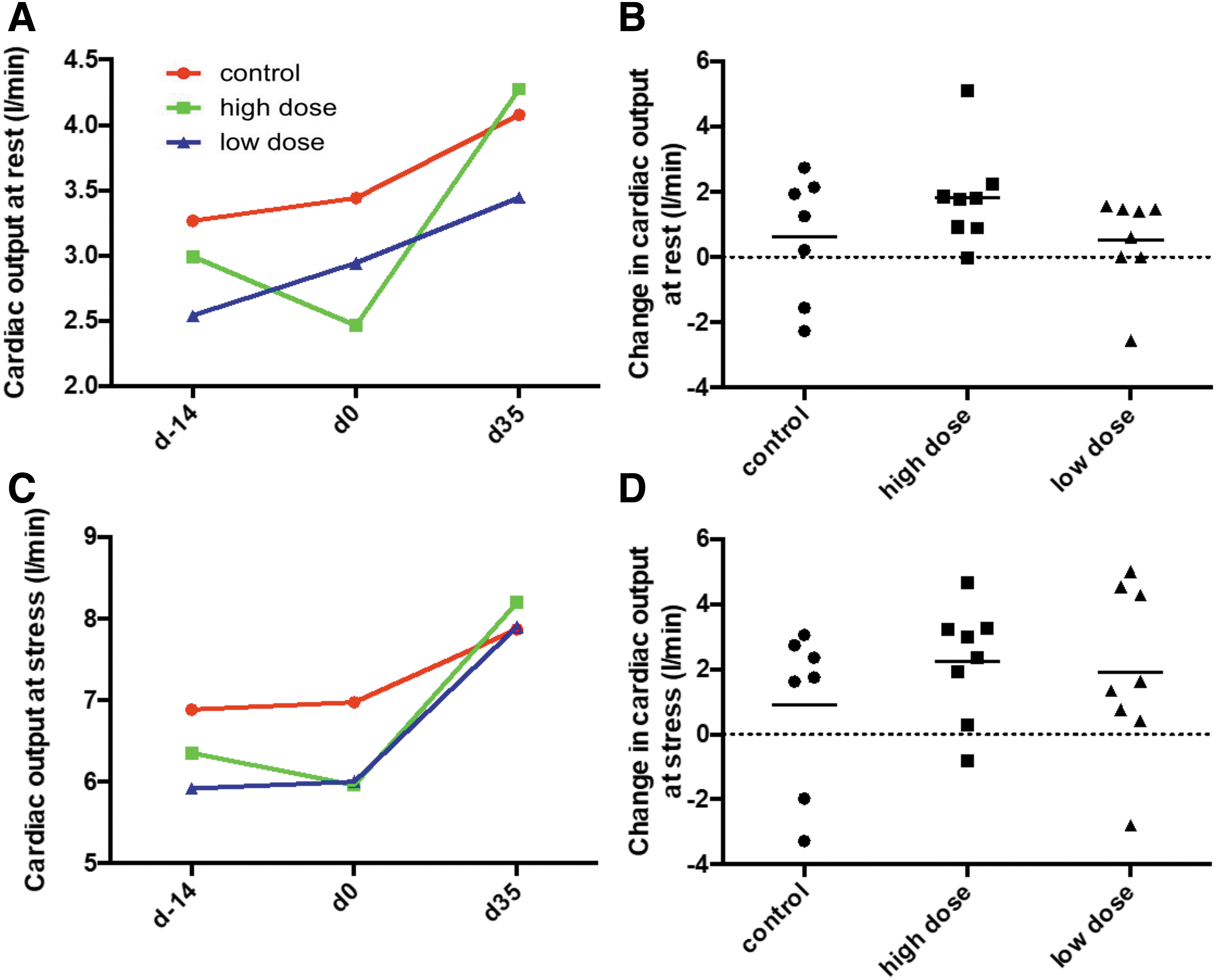
Cardiac output at different time points. After the ischemia operation, CO at rest
Collateral growth
The collateralization changes measured by Rentrop scoring were as follows: in the high-dose group from 3.3 ± 0.8 to 3.7 ± 0.5 and in the control group from 3.2 ± 0.8 to 3.3 ± 0.5, while staying at 3.3 ± 0.9 in the low-dose group over the 1-month follow-up. However, the changes were not statistically significant.
Infarct size
The total infarct size (Fig. 7) 5 weeks following the treatment was 32.6% ± 7.3% in the high-dose group, 31.5% ± 7.3% in the low-dose group, and 25.2% ± 7.1% in the control group. Examined separately, the transmural infarct size was 16.1% ± 6.0% in the control group, 18.4% ± 8.8% in the high-dose group, and 14.1% ± 9.5% in the low-dose group, while the proportion of the subendocardial infarction was 9.1% ± 6.5% in the control group, 14.2% ± 4.0% in the high-dose group and 17.3% ± 9.7% in the low-dose group. The infarct sizes between the groups were not statistically significant.
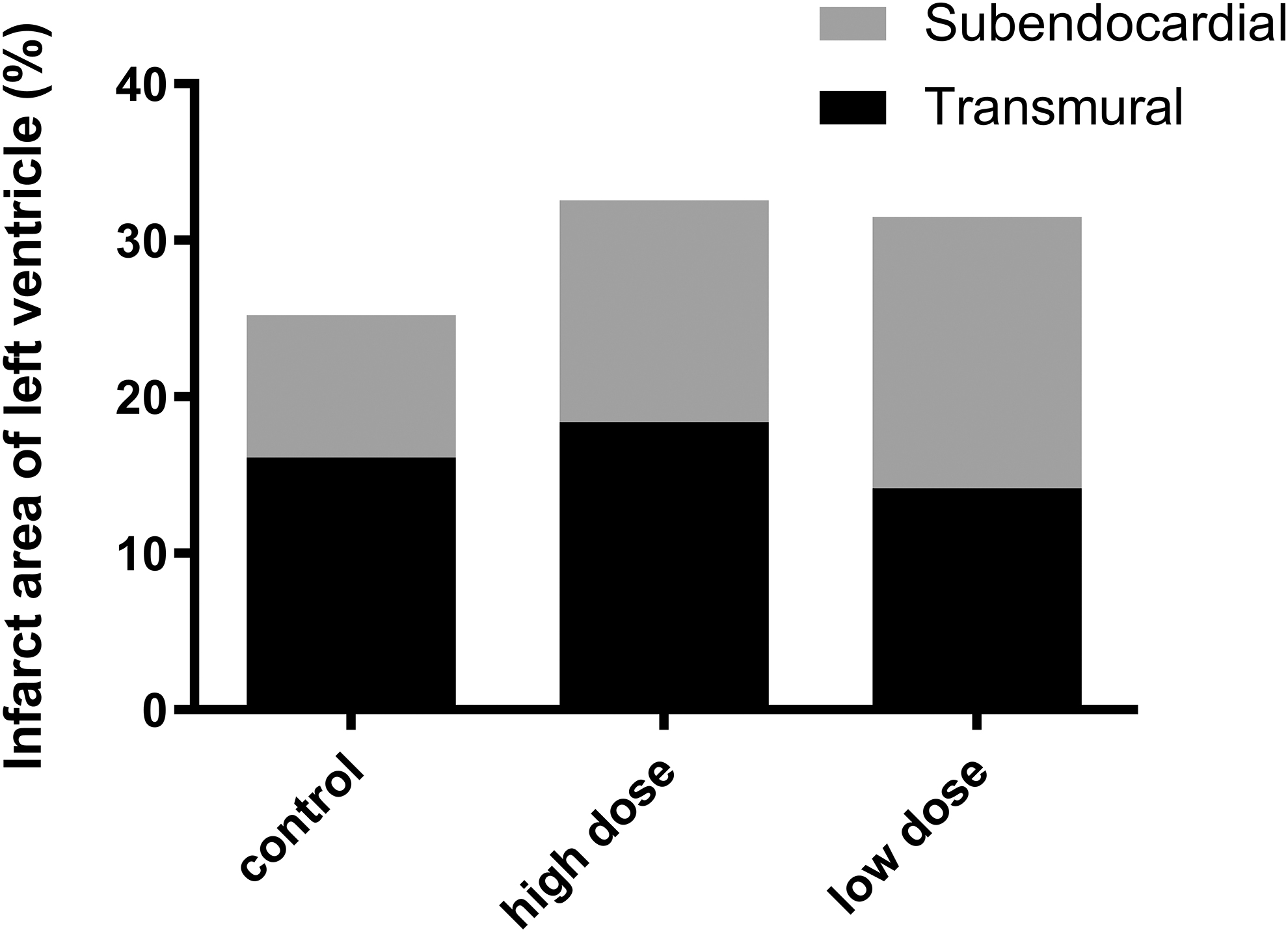
Infarct size at the sacrifice. The total infarct size was 32.6% ± 7.3% in the high-dose group, 31.5% ± 7.3% in the low-dose group, and 25.2% ± 7.1% in the control group. Transmural infarct size was 16.1% ± 6.0% in the control group, 18.4% ± 8.8% in the high-dose group, and 14.1% ± 9.5% in the low-dose group, while the proportion of the subendocardial infarction was 9.1% ± 6.5% in the control group, 14.2% ± 4.0% in the high-dose group, and 17.3% ± 9.7% in the low-dose group. The infarct sizes between the groups were not statistically significant.
Capillary area
The average capillary numbers (Fig. 8A) per section area in the control, high-dose, and low-dose groups were 77 ± 20, 73 ± 9, and 66 ± 16 in the border zone, 216 ± 47, 222 ± 57, and 222 ± 39 in the control area, and 205 ± 36, 215 ± 40, and 196 ± 55 in the maximal transduction area, respectively. These changes did not reach statistical significance.

Capillary count, capillary area, and total microvascular area in the different regions of the left ventricle at the sacrifice. The average capillary numbers
The capillary areas (Figs. 8B) in μm2 per section area for the control, high-dose, and low-dose groups in the border zone were 62 ± 19, 60 ± 10, and 65 ± 15. In the control area, the respective capillary areas were 48 ± 12, 41 ± 15, and 38 ± 5, and in the maximal transduction area, they were 48 ± 12, 46 ± 11, and 45 ± 7. These changes were not statistically significant.
The total microvascular area (Fig. 8C) as a portion of the total area for the section (%) in the control, high-dose, and low-dose groups was 0.89 ± 0.32, 0.87 ± 0.21, and 0.82 ± 0.24 in the border zone, 2.0 ± 0.20, 1.8 ± 0.74, and 1.7 ± 0.34 in the control area, and 1.9 ± 0.53, 1.9 ± 0.43, and 1.7 ± 0.36 in the maximal transduction area, respectively. These changes were not statistically significant. Representative images of lectin-stained sections are shown in Fig. 9.

Representative images of lectin-immunostained myocardial sections from the injection sites, that is, the maximal transduction area, border zone, and control area for the control, low-dose, and high-dose groups. No significant difference in capillary numbers or capillary areas was seen between the groups (Magnification 20 × , scale bar 100 μm). Color images are available online.
Transduction pattern and efficiency
To study the NOGA/Myostar-mediated intramyocardial transduction pattern and efficiency, LacZ mRNA coding for the beta-galactosidase enzyme was used. Animals were sacrificed 24 h following the transduction, and samples were collected for histological analysis. No clear transduction area or pattern could be visualized using beta-galactosidase immunostaining. Only a few positive cells could be identified, making the quantification of the transduced cells unreliable (Fig. 10).
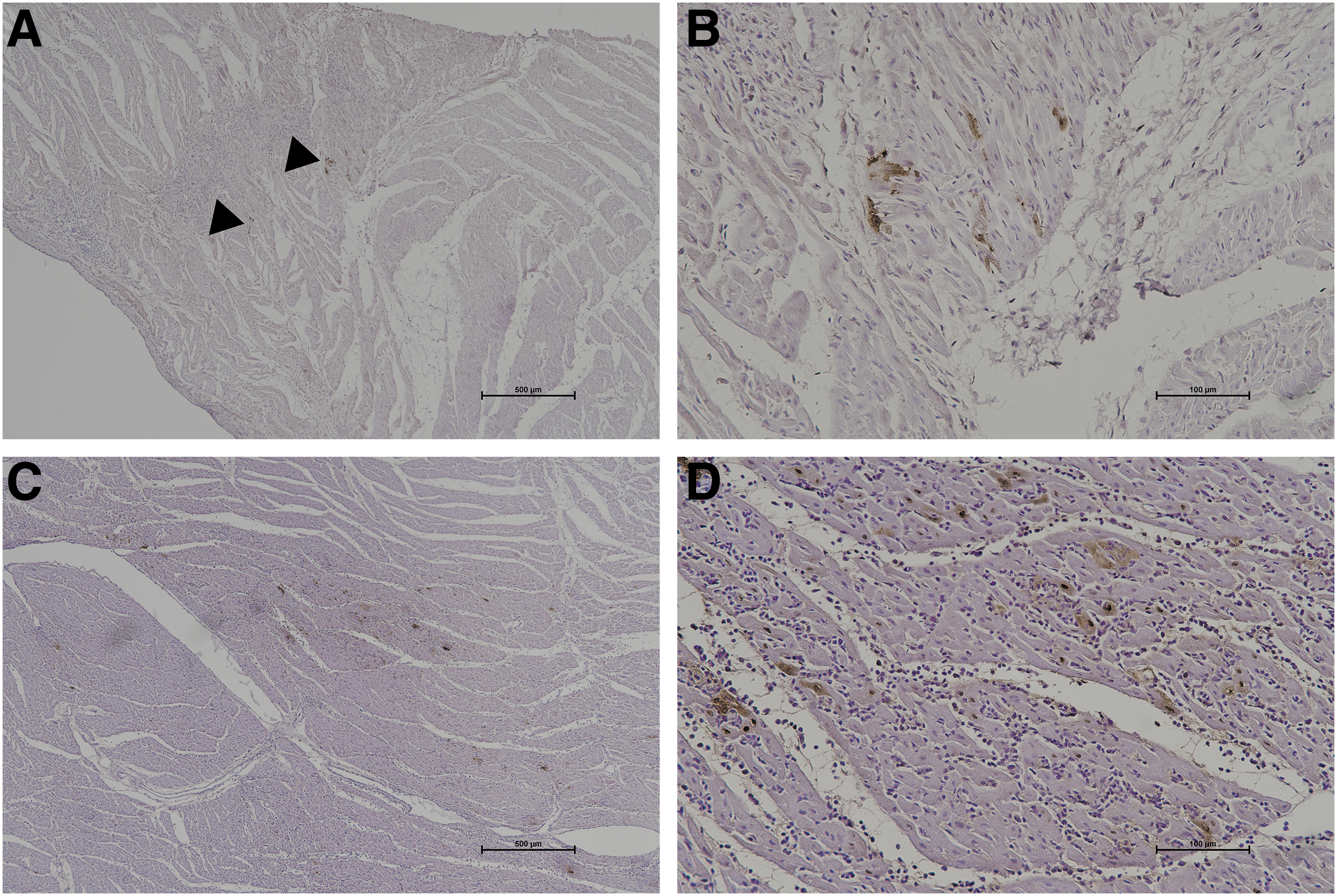
B-galactosidase enzyme stained using beta-galactosidase immunostaining from myocardial sections. Only a few positive cells could be identified
Conclusion
VEGF-A165 mRNA showed no statistically significant improvements in cardiac function, blood flow, or histological parameters. On the contrary, no adverse effects were observed, and no pathological findings were detected in the lungs, liver, spleen, kidneys, or ovaries. There was a numerical trend in the high-dose group toward an improved LVEF and CO at rest. However, the baseline LVEF and CO in these animals in the high-dose group were noticeably lower than in the control group, and regression to mean might at least partially explain the observed trend. In global myocardial perfusion at rest, there was a statistically significant decrease in the high-dose group compared with the control group. While the reduced perfusion was unexpected, it did not impact either LVEF or CO during rest or stress and is not considered clinically meaningful.
In conclusion, endocardial NOGA/Myostar injections with our current process do not seem to represent a viable way to deliver citrate-saline-formulated mRNA to the ischemic myocardium compared with, for example, direct epicardial injections. More effort is needed to optimize the mRNA delivery into the heart muscle to achieve better transduction efficiency utilizing a catheter approach. 23,24
Discussion
Our results differ from earlier findings where exactly the same VEGF-A165 mRNA formula used here improved cardiac parameters, induced angiogenesis, and decreased myocardial fibrosis in minipigs after 2 months of follow-up. 15 In that study, 20 epicardial injections (100 μL each) to infarct and peri-infarct areas were administered 7 days after the induction of ischemia with permanent LAD ligation. The study included two VEGF-A165 mRNA doses, low dose (1 mg, n = 8) and high dose (10 mg, n = 8). Both groups showed similar positive results. 15 Similar positive results have been obtained from mice. 14 In both the previous studies using direct epicardial injections, sufficient transduction efficiency was achieved and cardiac benefits thereof. Also, it was evident from a randomized, double-blinded, placebo-controlled study that direct intradermal injections of VEGF-A165 mRNA in men with type 2 diabetes were well tolerated and led to a dose-dependent increase in local protein production, suggesting local transduction efficiency. This was associated with enhanced basal skin blood flow 4 h and 7 days after the treatment. 9 At the moment, a randomized, double-blinded, placebo-controlled phase 2a clinical trial (EPICCURE) is ongoing. This trial tests the safety, tolerability, and efficacy of epicardial injections of VEGF-A165 mRNA in patients undergoing coronary artery bypass grafting (CABG) with stable CAD and moderately decreased LVEF. mRNA transfers in EPICCURE will be done during the CABG. 25
In addition to differences between delivery methods, differences in ischemia models and animal species can partially explain differing results compared with previous large-animal studies. Permanent LAD ligation used in the previous large-animal study is highly invasive and results in more acute coronary artery occlusion compared with the current ischemia model, where the bottleneck stent in LAD leads to reversible myocardial ischemia, and the later occlusion of the stent causes chronic myocardial ischemia and collateral artery growth. Also, the previous large-animal study was performed with 5-month-old female, sexually mature minipigs weighing ∼20 kg, meaning that no significant growth in pig size was observed during the follow-up. In our study, domestic pigs gained ∼22 kg in all groups in 35 days of follow-up leading to significant musculoskeletal growth.
Positive results with the same VEGF-A165 mRNA formula were seen even with 1 mg doses when delivered epicardially, whereas, in our experimental settings, no such positive results were obtained even with 7.5 mg doses. The main difference between the studies is the delivery method suggesting that epicardial injections are a more potent way to deliver mRNAs to CAD patients, for example, during CABG operation.
One possible reason for the lack of transduction efficiency can be attributed to the transfection of naked mRNA using citrate-saline formulations. It has been shown that naked nGFP mRNA, delivered in sucrose-citrate buffer or saline, resulted in low transfection levels in cardiomyocytes in vitro, whereas the use of positively charged transfection reagents yielded a high transfection level in vitro but increased apoptosis in the injection area in vivo. Despite the poor transduction efficiency in vitro, significant protein translation without apoptosis was seen in the heart in vivo when the naked mRNA was delivered with sucrose-citrate buffer or saline, supporting naked mRNA delivery as the optimal approach in vivo. Also, this study used direct injections into the myocardium in open-chest surgery. 23 One possibility would be to use lipid-based carriers to deliver mRNA, but previous studies report that mRNA can be expressed in the myocardium without the need for lipid carriers. 15,23
Previously, VEGF-A165 has led to mixed results in CAD gene therapy clinical trials using adenovirus 26 or plasmid vectors. 26 –36 In a few studies, an improvement in myocardial perfusion, 26 –28,33 decreased angina frequency and nitroglycerine consumption, 27,29 and improved quality of life 33 –36 were seen. However, some trials ended up being negative. 30 –32 Four of the studies used the NOGA/Myostar-injection system as a delivery method, 30 –32,35 but all plasmid-based trials were negative. 30 –32
Possible reasons for the lack of effects in the current study include a lack of statistical power as the study had only a limited number of animals. Potential contamination of the citrate-saline-formulated mRNA with blood during the NOGA/Myostar mapped endocardial injections might have led to the degradation of the mRNA, limiting transduction efficiency as well as the potential beneficial effects of the treatment. The limited transduction efficiency was evident in the experiments with LacZ mRNA where no effective gene transfer was observed as only a few beta-galactosidase-positive cells could be identified in the heart sections near the injection channels. Thus, reduced or even lack of mRNA transduction and functional protein production could explain the negative results on efficacy in this experimental setting.
Footnotes
Acknowledgments
We thank the animal caretakers Heikki Karhunen, Minna Törrönen, and Riikka Venäläinen for their assistance with the animal experiments.
Author Disclosure
L.-M.G. and R.F.-D. are employers of Astra-Zeneca.
Funding Information
This study was supported by Astra-Zeneca.