
Abstract
α1-antitrypsin (AAT) deficiency is a common autosomal recessive hereditary disorder, with a high risk for the development of early-onset panacinar emphysema. AAT, produced primarily in the liver, functions to protect the lung from neutrophil protease; with AAT deficiency, unimpeded neutrophil proteases destroy the lung parenchyma. AAT is susceptible to oxidative damage resulting in an inability to inhibit its target proteases, neutrophil elastase, and cathepsin G. The major sites of oxidative modification on the AAT molecule are methionine residues 351 and 358. We have previously demonstrated that an engineered variant of AAT that resists oxidation by modifying both protein surface methionines (M351V and M358L) provides antiprotease protection, despite oxidative stress. In mice, intravenous delivery of the modified AAT(AVL) variant by AAV serotype 8, AAV8hAAT(AVL), primarily to the liver resulted in long-term expression of an AAT that resists oxidative inactivation. In this study, we evaluated the safety of intravenous administration of AAV8hAAT(AVL) in a dose-escalating, blinded, placebo-controlled toxicology study in wild-type mice. The study assessed organ histology and clinical pathology findings of mice, intravenously administered AAV8hAAT(AVL) at three doses (5.0 × 1011, 5.0 × 1012, and 5.0 × 1013 genome copies [gc]/kg), compared to control mice injected intravenously with phosphate-buffered saline. As previously demonstrated, administration of AAV8hAAT(AVL) resulted in dose-dependent expression of high, potentially therapeutic, levels of serum human AAT protein that persist for at least 6 months. Antibodies against the AAV8 capsid were elicited as expected, but there was no antibody detected against the AAT(AVL) protein generated by the AAV8hAAT(AVL) vector. There was no morbidity or mortality observed in the study. The data demonstrate that intravenous administration of AAV8hAAT(AVL) is safe with no significant adverse effect attributed to AAV8hAAT(AVL) vector at any dose. This study demonstrates that AAV8hAAT(AVL) has a safety profile consistent with the requirements for proceeding to a clinical study.
INTRODUCTION
α1
AAT deficiency is associated with considerable morbidity, and an approximate reduction of 15 to 20 years in lifespan. 1,3,8,17,18 The disorder affects 70–90,000 individuals in the United States, and accounts for ∼2% of the cases of emphysema. 1 –5 The current therapy for AAT deficiency is weekly, biweekly, or monthly intravenous administration of human AAT purified from pooled plasma. 7,19 –23
While highly effective as an antiprotease, AAT is susceptible to oxidative damage, which results in an inability to inhibit proteases such as neutrophil elastase and cathepsin G. 24 –31 With oxidant stress, two surface active site methionine residues at positions 351 and 358 are modified to methionine sulfoxide. 28,31 –36 Smokers, ex-smokers, and nonsmokers are exposed to oxidants in the lower respiratory tract. Oxidative inactivation of AAT is common in smokers and the antiprotease activity of the lung epithelial lining fluid (ELF) of smokers' is markedly lower compared with nonsmokers. 26,29,37 The sources of the oxidants in smoker's lungs include the endogenous oxidants of cigarette smoke as well as those produced by activated macrophages, which are abundant in the lower respiratory tract of cigarette smokers and ex-smokers. 29,37,38 Nonsmokers are exposed to inhaled oxidants from the environment. 24,26,39
We have developed AAV8hAAT(AVL), an adeno-associated virus serotype 8 (AAV8)-based gene therapy for AAT deficiency coding for an engineered variant of AAT (Met351 to Val, Met358 to Leu). 31,40 –47 AAV8hAAT(AVL) is based on the normal AAT (M1 Ala213) variant, the normal variant form which the common Z mutation variant is evolved. 48,49 In a prior study, we demonstrated that 6 months after intravenous administration of AAV8hAAT(AVL) at doses of 4 × 1012 and 1.6 × 1013 genome copies [gc]/kg to male wild-type mice, the treatment mediated persistent high levels (0.7 and 1.8 mg/mL, respectively) of human AAT in serum and 14–42 μg/mg total protein in lung ELF, providing antiprotease protection to the lower respiratory tract, despite oxidant stress. 47
In support of translating AAV8hAAT(AVL) gene therapy to treat individuals with AAT deficiency, we designed this study to assess the safety of this vector and route of administration in 240 mice. The data demonstrate that intravenous administration of AAV8hAAT(AVL) results in persistent high levels of human AAT protein in the serum, and is safe and well tolerated in mice as required for translation of this therapy to humans,
METHODS
Study design
The blinded, placebo-controlled study compared the safety of intravenous administration of AAV8hAAT(AVL) (Supplementary Fig. S1) to mice with general assessment, hematologic and histological outcomes (Table 1) and was carried out at the Belfer Gene Therapy Core Facility (BGTCF). Age-matched C57Bl/6N mice (120 male and 120 female; from Taconic Farms) were randomly assigned by sex to four treatment cohorts (n = 30M/30F per treatment cohort): three cohorts of AAV8hAAT(AVL) [5 × 1011, 5 × 1012, and 5 × 1013 gc/kg, which is equivalent to 1.25 × 10, 10 1.25 × 1011, and 1.25 × 1012 gc total doses for a standard 25 g mouse] and one control cohort administered vehicle (phosphate-buffered saline [PBS]). Each cohort was further divided into three groups by scheduled endpoint (n = 10M/10F per cohort per time point) for sacrifice at 1 week, 1month, and 6 months after vector or vehicle administration (Table 1).
AAV8hAAT(AVL) toxicology study design in C57Bl/6 mice
AAV8hAAT(AVL) vector administered intravenously on day 0 of the study to 8-week-old C57Bl/6 mice. There are 3 dose groups—low dose (5 × 1011 gc/kg), middle dose (5 × 1012 gc/kg), and high dose (5 × 1013 gc/kg; (n = 10F/10M per dose per time point). All mice are randomly assigned to cohort groups, to avoid potential study bias, with staggered dosing of animals across all groups. Cages are numbered without treatment qualifiers. Nontechnician will keep the treatment key. Personnel who are injecting the vector are blinded to treatment and dosage.
PBS-administered animals will serve as controls and be sacrificed at the same time points as the vector-dosed animals (n = 10F/10M per time point).
10F/10M from each dose group and the PBS group are evaluated per time point. Of these 5 female and 5 male mice at each dose (or PBS) and time point, blood is sampled for hematologic and chemistry assays and organs are fixed with 10% neutral-buffered formalin for histology. The serum from the other 5 female and 5 male is used for anti-AAV antibodies, anti-hAAT(AVL) antibodies, and hAAT(AVL) protein levels.
Mice are observed daily by animal care staff for morbidity and mortality.
Body weight is obtained on the day of dosing, daily the first week after dosing and weekly thereafter, and on the day of scheduled euthanasia (terminal body weight).
Complete blood count—total red blood cell count, hemoglobin concentration, hematocrit, mean corpuscular volume, mean corpuscular hemoglobin, mean corpuscular hemoglobin concentration, reticulocyte count and percentage, platelet count, and relative and absolute counts of white blood cells, neutrophils, lymphocytes, monocytes, eosinophils, and basophils.
Serum chemistry parameters—ALP, alanine aminotransferase, aspartate aminotransferase, creatine kinase, gamma-glutamyl transpeptidase, albumin, total proteins, globulins, albumin/globulin ratio, total bilirubin, blood urea nitrogen, creatinine, cholesterol, triglycerides, glucose, calcium, phosphorus, chloride, potassium, sodium, and sodium/potassium ratio.
Samples of blood, liver, lung, diaphragm, kidneys, heart, brain, spleen, pancreas, bone marrow, skeletal muscle (quadriceps), and gonads will be reserved for future assessment using AAV8hAAT(AVL) genome distribution by TaqMan qPCR if required.
Total and neutralizing anti-AAV8 antibody are analyzed using ELISA and transduction inhibition-based assays with a luciferase reporter vector, respectively. Humoral immunity to the AAT protein was determined using an ELISA.
Histopathology was evaluated in brain, heart, lung with main stem bronchi and caudal trachea, liver (sections of the right lobe, left lobe, and right portion of the median lobe), kidneys (pair), lymph node (tracheobronchial), diaphragm, sternum with bone marrow, pancreas, spleen, skeletal muscle—longitudinal and cross-sections (quadriceps femoris from each hind leg), gonads, chest cavity organs, and gross lesions. A comprehensive gross pathology and histopathology will be performed for unscheduled deaths to determine the potential cause of death.
AAT, α1-antitrypsin; ALP, alkaline phosphatase; ELISA, enzyme-linked immunosorbent assay; PBS, phosphate-buffered saline.
Vector was administered at 8 weeks of age (±3 days). Before vector administration, the mice were weighed (week 1), ear-tagged, and further randomized within sex into four subgroups based on treatment and then based on sacrifice time points of 1 week, 1 month, and 6 months. Group randomization was performed by nontechnician staff with treatment qualifiers assigned (cohort A, B, C, and D) instead of dose or treatment group to avoid potential study bias, and dosing of animals was staggered across all groups. Cages were numbered without treatment qualifiers. Treatment key was kept confidential, and personnel who were administering the vector or observing mice for health assessments were blinded to treatment and dosage during the study.
To allow statistical assessment of outcomes, a total of n = 10 mice/gender were used for each cohort and each sacrifice time point. To assess acute toxicity as well as that mediated by innate immune system, 7-day (1 week) time point was assessed. To assess toxicity, as well as that mediated by an acquired immune response, 28-day (1 month) time point was used. Long-term toxicity was determined from 180-day (6 month) time point. Assessment time points were ±1 day for 1 week post-treatment cohorts and ±2–3 days for 1- and 6-month cohorts.
At 8 weeks of age (±3 days), on day 0 of the study, mice were injected intravenously with a volume of 100 μL into a lateral tail vein, for a single vector or vehicle administration. Animals were excluded from the study if their weight was outside the range of 18–30 g before injection, or if any of the fluid from the intravenous injection leaked subcutaneously or externally during administration. To account for these exclusions, 20 additional mice (50% males and 50% females) were ordered and available at the time of injection for each time point group. Mice received daily health checks by technical personnel and a weekly health report, and were weighed weekly until the time of sacrifice. Detailed in-life observations were recorded.
At each scheduled time of sacrifice (1 week, 1 month, and 6 months), blood was collected by cardiocentesis and 10 mice (5 males and 5 females) were analyzed by the Laboratory of Comparative Pathology (LCP) for complete blood count, serum chemistry, postmortem macroscopic examination, organ weights, and histopathology. The serum from the remaining 10 mice (5 males and 5 females) was analyzed by the technical staff at the BGTCF for determination of serum AAT levels, total and neutralizing anti-AAV8 antibody levels, and anti-human AAT(AVL) antibodies.
Detailed methods regarding the design and manufacture of the vector AAV8hAAT(AVL), vector administration in mice, in life health assessments, necropsy, and all assay methods are provided in Supplemental Data.
Statistics
For the weight of the whole body and each organ, the group mean, standard deviation, and standard error were calculated for each sex in each group at each time point. Each group mean was compared to the corresponding control group mean (same sex, at same time point, in PBS group), and the percentage change from the control group mean was calculated. A repeated measures of analysis of variance (RM-ANOVA) was performed on each dose cohort versus PBS-treated controls, with time as the repeated co-factor, testing for genders separately and combined. Analysis was done between each group versus PBS independently for the 1-week, 1-month, and 6-month time points, with difference of the group means considered statistically significant if p < 0.05.
For each hematology and serum chemistry parameter, the group mean, standard deviation, and standard error were calculated for each sex in each group at each time point. Each group mean was compared to the corresponding control group mean (same sex, at same time point, in PBS-treated group), and a percentage change (% difference = [(xtreated−xcontrol) × 100/xcontrol] from the control group mean was calculated. A two-tailed unpaired t-test was performed on the same pairs of groups and the difference of the group means was considered statistically significant if p < 0.01. Values were compared to historical normal ranges for mouse blood, which were strain specific when available. 50 The results of this analysis were provided to the pathologist for interpretation. All statistical analyses were performed with GraphPad Prism v9.3.0 (GraphPad Software, San Diego, CA).
RESULTS
AAT levels in serum
Evaluations of the serum of the 7-day (1 week), 28-day (1 month), and 182-day (6 month) cohort demonstrated dose-dependent increases in expressed hAAT in treated mice, with 32% to 80% of peak levels observed as early as 7 days postadministration. High dose-dependent levels of human AAT were observed in both male and female mice (Fig. 1A, B). As documented in many studies by us and others, AAV vectors administered intravenously are associated with higher levels in male compared to female mice, a gender-related phenomenon that is mouse specific. 47,51 –57 Nearly 4.4 mg/mL (85 μM) of hAAT was detected in the high dose male cohorts, which is far greater than the therapeutic requirements for successful treatment. These results are comparable to the AAV8hAAT(AVL) serum levels observed in our prior publication 47
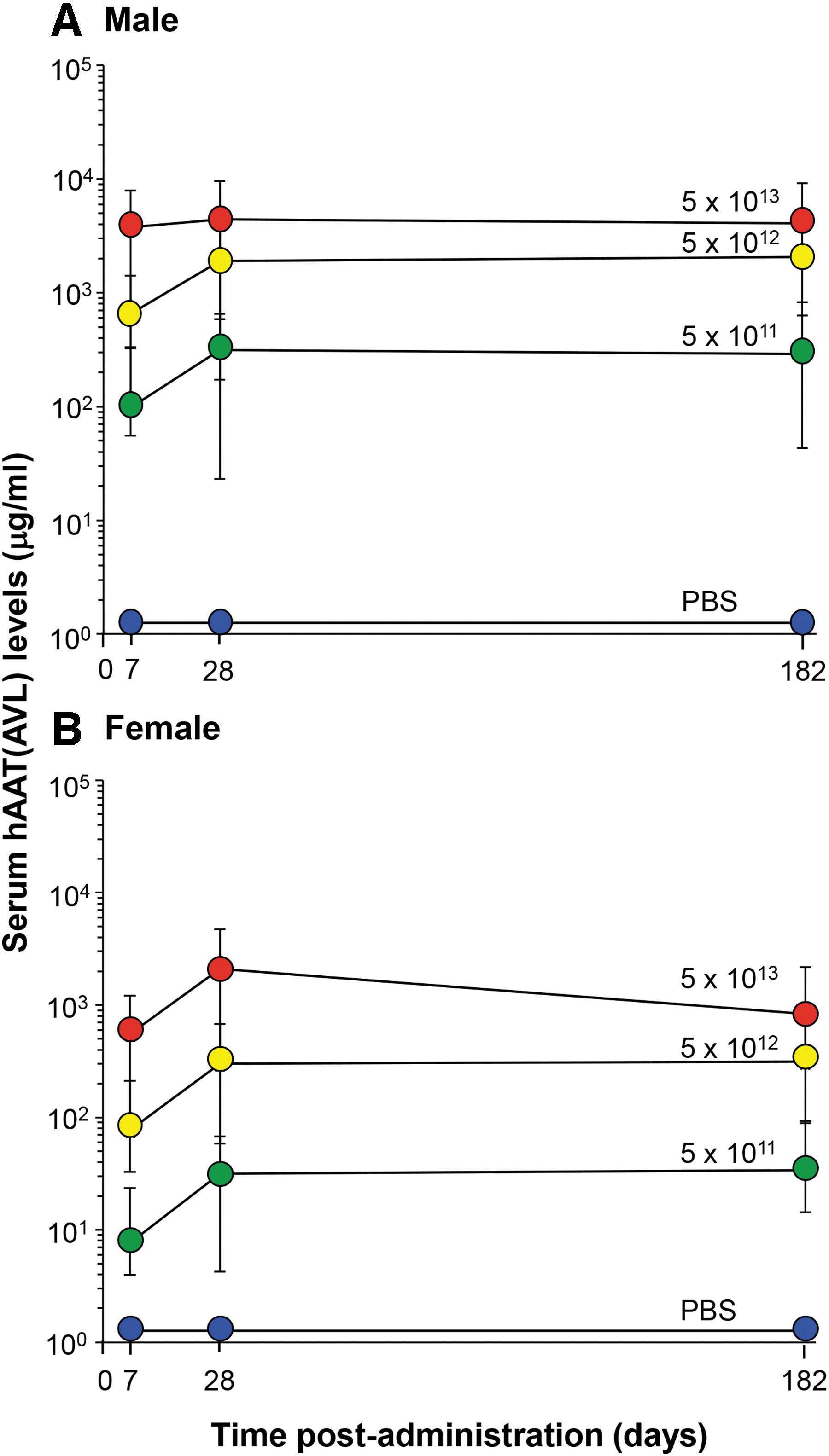
Effect of intravenous administration of AAV8hAAT(AVL) on serum levels of hAAT(AVL) as a function of dose and time. AAV or PBS control-treated wild-type C57Bl/6N mice (n = 5/dose/gender/time point) were assessed for serum human AAT(AVL) levels by human-specific ELISA. At indicated end point times of 1 week, 1 month, and 6 months, mice were bled for assessment of serum hAAT(AVL) levels. Shown are serum hAAT(AVL) levels for PBS and the 3 AAV8hAAT(AVL) doses (5.0 × 1011, 5.0 × 1012, and 5.0 × 1013 gc/kg). Levels are expressed as the geometric mean ± SEM for each dose cohort (gender data plotted separately). Results of hAAT(AVL) levels detected for each dose group are shown, color coded by treatment (blue, PBS; green, AAV8hAAT(AVL), 5.0 × 1011 gc/kg; yellow, AAV8hAAT(AVL), 5.0 × 1012 gc/kg; red, AAV8hAAT(AVL), 5.0 × 1013 gc/kg).
General safety and clinical observations
No mouse was found to exhibit severe adverse reactions to the study drug AAV8hAAT(AVL) at any dose or PBS postvector administration in the acute or long-term study cohorts. No morbidity requiring early sacrifice or mortality was observed during the study.
Mice in the study were assessed for respiratory function, alertness, general behavior, reflex responsiveness, and general health. The study drug, AAV8hAAT(AVL), was well tolerated in the mice at each dose level, with no emergency requiring analgesics or supplemental food care. Body weights were obtained 1 week before injection, on the day of dosing, daily the first week after dosing and weekly thereafter for length of each cohort's planned sacrifice time point.
Mice (both males and females) did not lose weight over the course of the study (Fig. 2A, B). RM-ANOVA analysis of the weight gain in treated cohorts and time points showed no significance difference when compared to PBS for all the low dose males and females at 5 × 1011 gc/kg dose (p > 0.8), except for males at 6 months (p < 0.0001). For the mid-dose, 5 × 1012 gc/kg dose, significant differences with PBS control were observed only for males at 1 week (p < 0.007) and 6 months (p < 0.004). For the high (5 × 1013 gc/kg) dose cohort, significant differences were observed for all cohorts versus PBS controls (p < 0.002), except females at 6 months (p > 0.6).
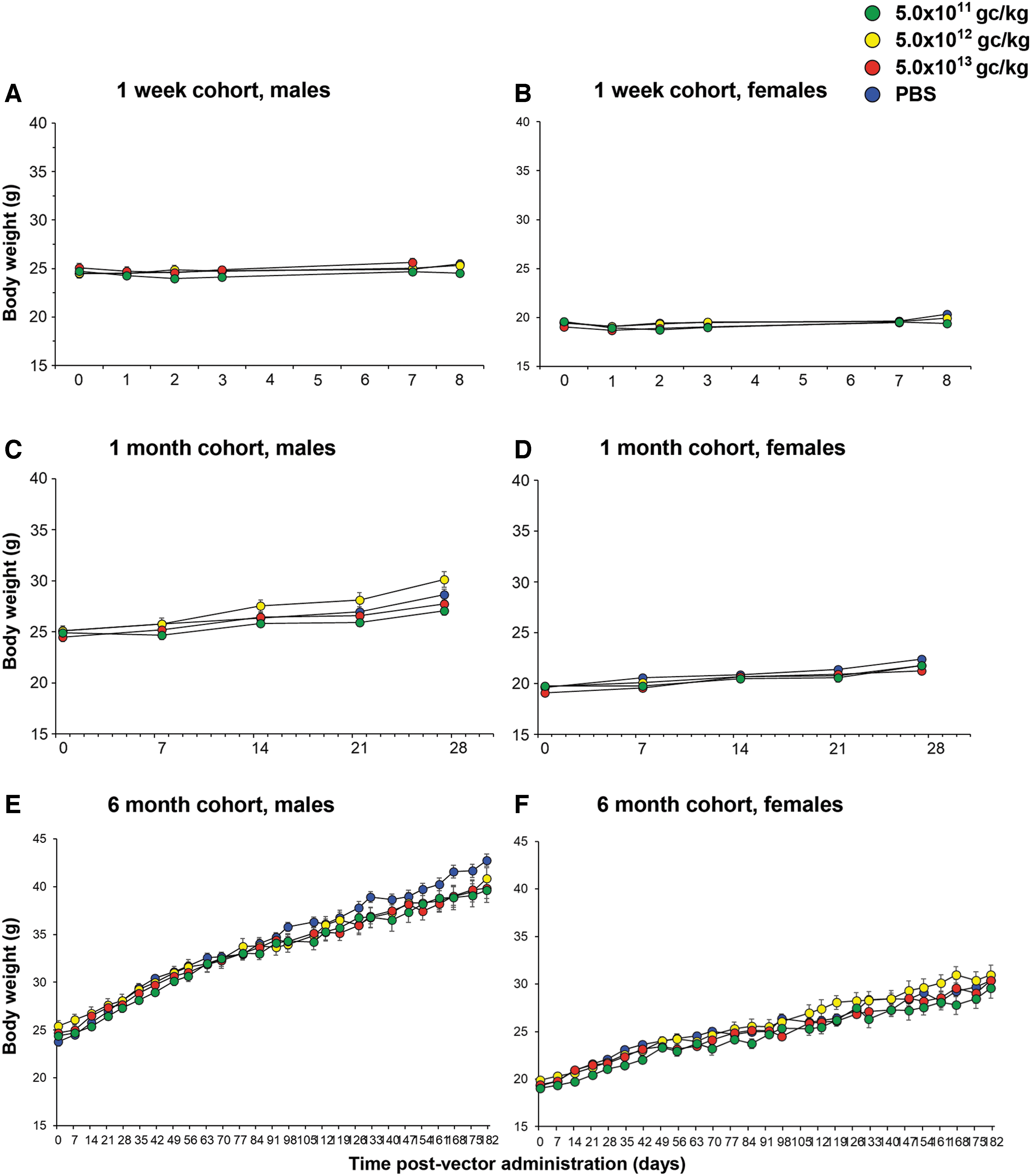
Body weights of treated wild-type C57Bl/6 mice postadministration. As a measure of efficacy and health status, all mice were weighed at regular intervals postvector or PBS treatment until they were sacrificed at predetermined endpoints for each cohort (Table 1). Mean weights (g) ± SEM are shown for time of assessment (in days) postvector administration, from arrival to sacrifice.
Gross pathology and organ weights
Comparisons of male and female organ weights showed the expected increase in weight as the mice aged, but no significant difference compared to PBS controls (Supplementary Fig. S2). A summary of all dose group differences between treated and control mice for all parameters is presented in Table 2.
Summary of group differences observed between treated and control animals
An adverse effect was determined if there was a difference observed between the controls and treatment groups and whether the effect was adverse based on pathologist review of clinical significance. Blood and serum parameters were compared to normal ranges, and if the increased or decreased value still fell within the normal range, the change was not deemed to be adverse.
Different, but within normal range, except for sporadic animals in one gender and at one time point and lacked gross or microscopic pathology correlates
Different, but within normal range
Different, but within normal range, except for sporadic animals in the low- and the high dose groups (not the mid-dose), but lacked gross or microscopic pathology correlates
na, not applicable
Hematology
Individual animal hematology results from scheduled sacrifice were compiled (Supplementary Fig. S3). Normal daily fluctuations in hematological parameters were observed and expected. Some parameters, such as reticulocytes, white blood cell counts, and neutrophils/lymphocyte (absolute and % of total cell counts), did present with individual mice, with values outside the reference ranges obtained from the matching PBS controls (Supplementary Fig. S3). Results for red blood count, hemoglobin, and hematocrit showed decreased means (3–6%) in the high dose, 5 × 1013 gc/kg, cohort in both males (1 and 6 month) and females (1 and 6 month) compared to the PBS controls (Table 2). While means of the group values differed between the high dose and the PBS controls, these values remained within the normal range of expected values for male and female C57Bl/6N mice.
Lymphocyte cell counts were reduced (40–41%) in the high dose, 5 × 1013 gc/kg, cohort in both males (6 month) and females (6 month) compared to the PBS controls (Table 2). While different, these values remained within the normal range. Differences in these parameters were deemed to be “possibly attributed” to the test article by the reviewing pathologist, but not an adverse effect of the drug (Table 2), as they remained within the normal range. Because of a very low platelet count in one animal (female) in the 1-week, high dose cohort (5 × 1013 gc/kg), the blood smear from this animal was reviewed and revealed numerous platelet clumps. The low platelet count was interpreted to be an artifact caused by platelet clumping that occurred at the time of blood sampling.
Serum chemistry
Individual animal serum chemistry results from scheduled sacrifice were compiled and are presented in Supplementary Fig. S4. Normal daily fluctuations in serum chemistry parameters were observed and expected. Some parameters, such as blood urea nitrogen, alkaline phosphatase (ALP), aspartate aminotransferase, and creatine kinase, did present with individual mice, with values outside the reference ranges obtained from the matching PBS controls (Supplementary Fig. S4).
Serum cholesterol results did show decreased values (14–30%) in the high dose, 5 × 1013 gc/kg, cohort in both males (1 week, 1 month, and 6 month) and females (1 week and 1 month) compared to the PBS controls (Table 2), but while different, these values remained within the normal range. This parameter was deemed to be “possibly attributed” to the test article by the reviewing pathologist, but not an adverse effect of the drug (Table 2) as the values, while lower, remained within the normal range.
Serum AAV8 neutralizing and total antibody titers
As a measure of systemic immune response to the AAV8hAAT(AVL) vector, we assessed the serum for anti-AAV8 vector antibodies. As expected, all the treated mice developed anti-AAV8 total and neutralizing antibody titers (Fig. 3). Highest levels were observed in the 6-month cohorts, with the high dose (5 × 1013 gc/kg) developing the highest titers, which were significant compared to the PBS controls. Control PBS-treated mice did not have any anti-AAV8 titer.

Serum anti-AAV8 total and neutralizing antibody titers in mice after intravenous administration of AAV8hAAT(AVL). Assessment of total anti-AAV8 and neutralizing anti-AAV8 antibody titers in treated mice for humoral response evoked by IV administration of AAV8hAAT(AVL). The total antibody titer is expressed as the reciprocal of the serum dilution, while the neutralizing antibody titer is expressed as the reciprocal of serum dilution at which 50% inhibition of AAV8Luc was observed.
Serum anti-hAAT(AVL) antibody titers
Despite the presence of the human AAT with the AVL variant in the treatment vector, none of the doses tested generated levels of serum anti-hAAT(AVL) antibodies, consistent with the safety of the AAV8hAAT(AVL) therapy (Fig. 4).
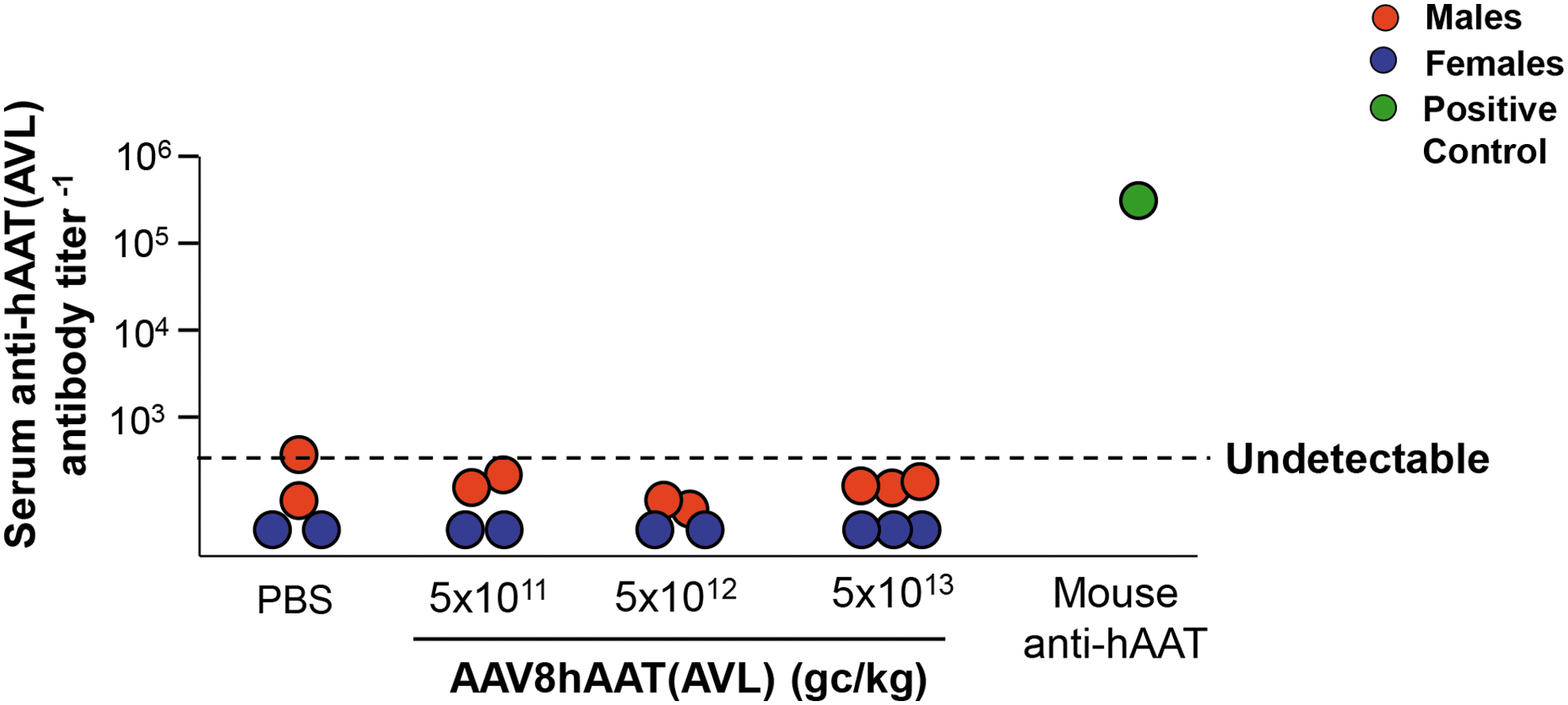
Assessment of serum antibody titers against human AAT(AVL) protein. Serum samples from the 6-month cohorts were assessed for the presence of antibodies against the expressed AVL variant of AAT evoked by IV administration of AAV8hAAT(AVL). No anti-AAT(AVL) antibody was detected. The antibody titer is expressed as the reciprocal of the serum dilution. Shown are serum anti-hAAT(AVL) antibody levels for n = 2 mice per cohort [except, n = 3 for high dose, male = red circles, female = blue circles] for PBS and the 3 AAV8hAAT(AVL) doses (5.0 × 1011, 5.0 × 1012, and 5.0 × 1013 gc/kg). The antibody titer is expressed as the reciprocal of the serum dilution. All mice were treated at 8 weeks of age ±3 days. Black dashed line represents the PBS control titers as the undetectable baseline of the assays. Positive control for plate was mouse anti-hAAT monoclonal antibody (green circle). Color images are available online.
Immune responses
There was no observable innate immune response associated with the treatment as measured by infiltrates of leukocytic cells in all organs evaluated. Furthermore, aside from some sporadic changes, no immune-mediated liver damage was observed by liver enzyme biomarkers ALP, alanine transaminase, aspartate transaminase, and gamma-glutamyltransferase activity (Supplementary Data—Pathology Report).
Histopathology
Results of macroscopic and histopathologic examination at scheduled sacrifice for individual animals were compiled by the reviewing pathologists (Supplementary Data—Pathology Report). Lesions that were observed in at least two animals in the study were noted and recorded for the incidence (number of mice/cohort) and severity of the lesion. Pathology review of the spleens revealed significant follicular lymphoid hyperplasia in all dose cohorts, males and females, in the acute 1-week mice (2 to 5/5) and in the higher doses (5 × 1012 and 5 × 1013 gc/kg), males and females, in the 1-month mice (5/5) compared to the PBS controls, which showed no hyperplasia (Table 2). This hyperplasia was deemed to be “attributed” to the test article by the reviewing pathologist, but not an adverse effect of the drug (Table 2). Assessment of the dorsal root ganglia showed no abnormality.
DISCUSSION
AAT deficiency is an autosomal recessive hereditary disorder associated with premature emphysema exacerbated by cigarette smoking. AAT is a powerful antiprotease secreted by the liver that primarily functions to protect the alveolar structures. 1,2,7,8,12 –15 The life span of affected individuals with AAT deficiency is decreased by 15–20 years. 1,3,17,18,58 Current therapy consists of a lifetime of weekly intravenous infusions of AAT purified from pooled human plasma. This is costly, is burdensome for the patient, poses a risk of infection or an immune response to the infused product, and is subject to oxidation inactivation. 47,59 –61
A one-time treatment by intravenous administration of an adeno-associated virus gene transfer vector coding for AAT is an experimental approach to provide a sustained supply of AAT to the lung. 62 If effective and safe, this would provide a more convenient, safe single treatment. AAT in the lung is subject to inactivation by oxidation, an effect mediated by cigarette smoking, inhaled environmental pollutants, and oxidants generated by activated inflammatory cells. 63,64 We have developed an engineered variant of AAT that resists oxidation, with antiprotease function to protect against the development of emphysema. 47
We have previously demonstrated that an AAV serotype 8 vector expressing a cDNA encoding an oxidation-resistant human AAT when delivered intravenously results in a physiological level of oxidation-resistant AAT in the serum and lung of treated mice. 47 Based on this proof-of-concept data in which AAT function persists in the context of oxidants such as that from smoking, we have carried out a pivotal safety and toxicology study in mice as a next step in the clinical development of AAV8hAAT(AVL).
Safety of AAV8hAAT(AVL)
The goal of this toxicology study was to provide data supporting clinical translation of AAV8hAAT(AVL) by demonstrating its safety as a prerequisite for initiating a Phase 1 trial to assess the safety and preliminary measure of efficacy of the AAV8hAAT(AVL) vector administered to AAT-deficient individuals.
Intravenous administration of AAV8hAAT(AVL) led to dose-dependent high levels of AAT that persisted out to 6 months postadministration, the longest time point studied. While these high levels were observed in both male and female mice, there was a gender-related difference with higher levels per dose administered seen in male versus female mice, a phenomenon that is specific to mice and has been observed previously. 47,51 –56,65
With regard to the safety of the AAV8hAAT(AVL) treatment, we compared anatomical and clinical pathology findings between treated mice, injected intravenously with AAV8hAAT(AVL), at three doses (5.0 × 1011, 5.0 × 1012, and 5.0 × 1013 gc/kg) and control mice injected intravenously with PBS. The vector was well tolerated in all animals at all three doses over the course of the 6-month study with no clinically relevant systemic toxicity observed. No vector-related morbidity or mortality was observed in any mice in the study and all animals continued with normal growth rates after dosing.
There was no adverse outcome associated with the vector as measured by hematology, serum chemistry panel, and gross and microscopic pathology. As expected, all the treated mice developed anti-AAV8 total and neutralizing antibody titers. Differences in hematology and serum chemistry parameters were typical of normal biological variations or were sporadic and seen in one gender or at one time point and lacked gross or microscopic pathology correlates.
While some findings were “attributed,” or “possibly attributed,” to administration of the AAV8hAAT(AVL), they were not interpreted as adverse effects as they did not result in clinical signs or weight loss, were not pathologically significant to the health of the animals, and mostly were within the normal range. No pathologic change was observed in dorsal root ganglia. Because the findings labeled “attributed” or “possibly attributed” did not correlate with any untoward clinical outcome, they do not flag safety concerns, but they do provide guidance as to parameters that should be monitored at regular intervals during the clinical study and provide insight into the design and timing of assessments in the clinical study.
It is important to note that AAT deficiency in the ZZ genotype individuals can result in liver disease. Since we intend to target the liver with this gene therapy, the clinical trial will exclude individuals with the evidence of significant liver disease and all participants will be carefully monitored for liver function.
In summary, AAV8hAAT(AVL) was well tolerated in all animals at three different doses and at three different time points when delivered intravenously with no systemic toxicity, or vector-related morbidity or mortality. This study demonstrates that AAV8hAAT(AVL) has a safety profile consistent with the requirements for a clinical study and mediates persistent expression of the hAAT at the doses assessed.
Footnotes
ACKNOWLEDGMENTS
We thank J. Mezey for advice regarding statistical analysis and N. Mohamed for editorial support. These studies were supported, in part, by NIH R42 HL140670.
AUTHORs' CONTRIBUTIONS
J.B.R.—study design, data analysis, and involved with drafting of the article; B.P.D.—study design, conducting of study-related assays, and data analysis; A.G.—carrying out animal study, in-life assessments, necropsies, conducting of study-related assays, and data analysis; N.G.—conducting of study-related assays and data analysis; V.K.—carrying out animal study, in-life assessments, and necropsies; A.C.—carrying out animal study, in-life assessments, and necropsies; M.Y.-B.—carrying out animal study, in-life assessments, necropsies, and data analysis; C.M.-Z.—carrying out animal study, in-life assessments, and necropsies; S.M.K.—data analysis and involved with drafting of the article; S.M.—study pathologist; R.G.C.—study design, study oversight, and involved with drafting of the article; D.S.—study design, study oversight, data analysis, and involved with drafting of the article.
AUTHOR DISCLOSURE
D.S., S.M.K., and R.G.C. hold equity in and are consultants to LEXEO.
Funding Information
These studies were supported, in part, by NIH R42 HL140670, an STTR grant to LEXEO Therapeutics.
Supplementary Material
Supplementary Data
Supplementary Figure S1
Supplementary Figure S2
Supplementary Figure S3
Supplementary Figure S4
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.