
Abstract
With efficient transduction across most cell types and larger packaging capacity, Adenovirus 5 (Ad5) makes an attractive choice as a viral vector. However, a reported past mortality and known immunogenicity cast doubt on the safety of its use. An online database search was performed for all clinical trials administering intratumoral injection of gene therapy packaged in Ad5, being conducted in the United States, and using the Common Terminology Criteria for Adverse Events (CTCAE). Studies with unclear adverse events (AE) were excluded. The primary outcome collected was grade ≥3 (AE). Analyses were performed using Fisher's exact test. Thirty-nine prospective clinical trials across a variety of cancers were identified: 14 studies of therapeutic Ad5 alone, 12 with chemotherapy, 16 with radiation, and 11 with surgery. There were 3 mortalities out of 756 patients (0.4%), which were most likely unrelated to Ad5: 1 due to hypoxic encephalopathy, 1 due to splenic vein thrombus, and 1 due to disease progression. In trials that reported total AE (grades 1–5), there were 284 (10.3%) grade ≥3 AE out of 2,745 total AE in 477 patients. The overall life-threatening (grade 4) AE rate was 1.4% (34/2,425 AE in 428 patients). Overall, the most frequent grade ≥3 AE were lymphopenia (20.6% in 14 trials, 209 patients), dyspnea (8.7% in 11 trials, 208 patients), and neutropenia (8.6% in 12 trials, 174 patients). The most frequent grade 4 AE were neutropenia (4.6%), lymphopenia (3.3%), and leukopenia (3.1% in 13 trials, 192 patients). Our analyses demonstrated relative overall safety of Ad5 and warrant re-evaluation for the use of Ad5 as a delivery vector for gene therapy products.
INTRODUCTION
Gene therapy is an exciting field, holding the promise of delivering treatment options for a wide variety of diseases at their most proximate cause. As cancer is generally the consequence of changes made at the genetic and/or epigenetic level, this mode of treatment provides a unique opportunity for therapeutic intervention.
Gene therapy has been studied as an adjunct to the current standard of care for several decades. 1,2 One important component of gene therapy drug development is choosing the optimal delivery mechanism to allow for efficient uptake. Viruses are often used as delivery vectors, taking advantage of their natural function to enter cells and deliver genetic materials. 1 While there are several viral vectors commonly used such as adeno-associated virus, lentivirus, and adenovirus (Ad), Ad is one of the most frequently utilized. Within Ad, there are many serotypes with serotype 5 (Ad5) being one of the most commonly employed. 3
Ad5 is well known as a common virus infecting humans with a tropism for epithelium (respiratory, ocular, and intestinal) and liver cells. 4 There are many factors that make Ad5 an attractive choice for vector delivery: good transduction efficiency in dividing and nondividing cells, large packaging capacity, and a low frequency of insertional mutagenesis. 5
In clinical trials, Ad5 is used to package oncologic gene therapies with a variety of mechanisms of action. These can generally be categorized into suicide genes, immunostimulatory, oncolytic, or tumor suppressor. Suicide genes encode an enzyme, which on administration of a prodrug induces cell death. Immunostimulatory delivers immunoregulatory genes to the tumor cells and stimulates a localized immune response. Oncolytic viruses are replication competent and cause lysis of tumor cells. Tumor suppressor drugs re-engage the mutated tumor suppressor pathway. 1
Despite these usages and their potential advantages, there have been several safety concerns about the use of Ad5. The vector is known to be immunogenic due to pathogen-associated molecular patterns (PAMPs) on multiple components of the virus (capsid, viral DNA, and specific intermediates). When recognized, these PAMPs could trigger the release of cytokines and chemokines, potentially cause a cytokine storm. 4 There are also concerns that, given the prevalence of prior exposures, neutralizing antibodies could prevent the virus from acting on its target. 6
In addition, there was a heightened safety concern due to one patient death, possibly from a cytokine storm, which slowed down the field of gene therapy, and more specifically, the use of Ad5. 1 Briefly, in 1999, a patient in a gene therapy trial for the treatment of ornithine transcarnamylase died after administration of an Ad5 packaged therapy. There were several factors which may have contributed to the death such as deviation from the protocol without IRB approval and patient selection criteria. A legitimate question raised was whether this death was related specifically to the gene therapy vector itself. The event raised the safety concerns of Ad5 vector and slowed down its use as a delivery vehicle in the development of gene therapy drugs. 1,2,7
As a way to combat some of these safety concerns, the newer generations of Ad5 have been engineered to have reduction in the cytotoxic response, removal of the genes responsible for replication, and increase in packaging capacity. 7 At this time, over 20% of all gene therapy oncologic clinical trials use Ad5 as the delivery vector 9 and two Ad5 packaged gene therapy drugs (Gendicine and Oncorine) have been approved for use in China.
While Ad5 is increasingly utilized due to its positive attributes as a vector, there continues to be concerns about expanding its use. 1,9 This review will concentrate on intratumoral delivery. Intratumoral injection provides a highly targeted administration method with the least systemic spread that is being used more frequently to directly deliver therapy. The advantage of this analytic approach is that local therapies (1) come with unique risks for adverse events (AE) and these need to be understood and characterized, (2) should theoretically have less AE compared to systemic administration, so if the rate of serious AE is high, then that would raise concern for other types of administration, and (3) are often given in combination with traditional systemic agents and the risks of these combinations are poorly understood.
Therefore, we aim to evaluate the safety of Ad5 by examining AE in published oncologic clinical trials that employ intratumor injection of Ad5 packaged drugs, and determine whether these safety concerns are justifiable or overstated.
MATERIALS AND METHODS
This review was conducted using PRISMA guidelines.
10
There was no inclusion of human trial samples and therefore did not require ethics committee approval. An online search of PubMed and
Studies were included if they used an Ad5 or chimeric Ad5 delivery vector for administration of an oncologic drug through an intratumoral route in a clinical trial occurring in the United States and reported AE. They were also included if the Ad5 delivery vector was given alone or in combination with standard of care cancer treatments. This allowed a comparison of Ad5 with or without the expected co-treatment and allowed analysis of the anticipated real-world delivery. Studies were excluded if AE were not reported, unclear, or not reported using the National Cancer Institute's (NCI) Common Terminology Criteria for Adverse Events (CTCAE).
The primary outcome was grade 5 (mortality) adverse events (AE). Secondary outcomes were grade ≥3 (serious), grade 3 (severe), and grade 4 (life threatening) AE. Additional extracted data included type of cancer, phase of clinical trial, mechanism of action, additional and/or concomitant therapies (chemotherapy, radiation, or surgery), number of doses, dose level, number of patients treated, total (grade 1–5) AE, number of patients with grade ≥3 AE, and number of AE categories reported. There was no comparison of the mechanism of action as the numbers were too small and the purpose of the article was to examine the safety of the delivery vector, not the package.
AE were reported by the NCI's CTCAE terms (sign, symptom, or disease), allowing multiple AE to be assigned to an individual patient (i.e., a patient presenting with syncope, hypotension, and laboratory abnormalities could account for several AE). To account for this reporting, the frequency of the serious (grade ≥3) AE is presented either as a proportion of the total (grade 1–5) AE reported in the trial (serious AE/total AE) or as a percent of patients (patients with serious AE/total number of patients), depending on the data provided in each individual trial. Total AE is used to refer to trials that presented the total number of AE recorded in the trial across all grades. 1 –5
Clinical trials presented their AE either with all serious (grade ≥3) AE as one grouped value or with each grade as separate and individual values. Grouped value trials refer to grade 3, 4, and 5 AE presented altogether without breakdown by grades and therefore an inability to differentiate the seriousness of each AE. Separated value trials refer to trials that presented individual AE (grade 3, 4, and 5) by grade level. Grouped value AE were compared across all trials, but analysis by individual grades (grade 3 vs. grade 4) was only able to be undertaken in trials that reported separated values of AE.
Trials reported their AE by one of three categories. AE were classified as unedited in the subanalysis, if the authors presented all AE without modification based on the presumed cause of the AE (i.e., author did not remove AE even if it was clearly related to disease progression or co-treatment). Drug-related trials were those that reported only the AE, which the investigator determined to be related to the experimental Ad5 drug, and excluded those caused by other aspects of co-treatment or primary disease. If trials reported AE that only occurred above a certain percent or certain number of patients, this was classified as most frequent reported AE.
Analysis of extracted data was conducted using Microsoft Excel and GraphPad QuickCalcs. Differences between two categorical groups were calculated using Fisher's exact test with differences considered significant at p < 0.05. Differences between continuous groups were calculated using means with t-test.
RESULTS
Included Studies
A search of PubMed and Clinicaltrials.gov, as well as manual retrieval from the references, identified a total of 385 publications. After removing duplicates and assessing eligibility, 39 clinical trials were identified and are included in this review. 11 –48 The PRISMA flow diagram of publication selection is shown in Fig. 1.
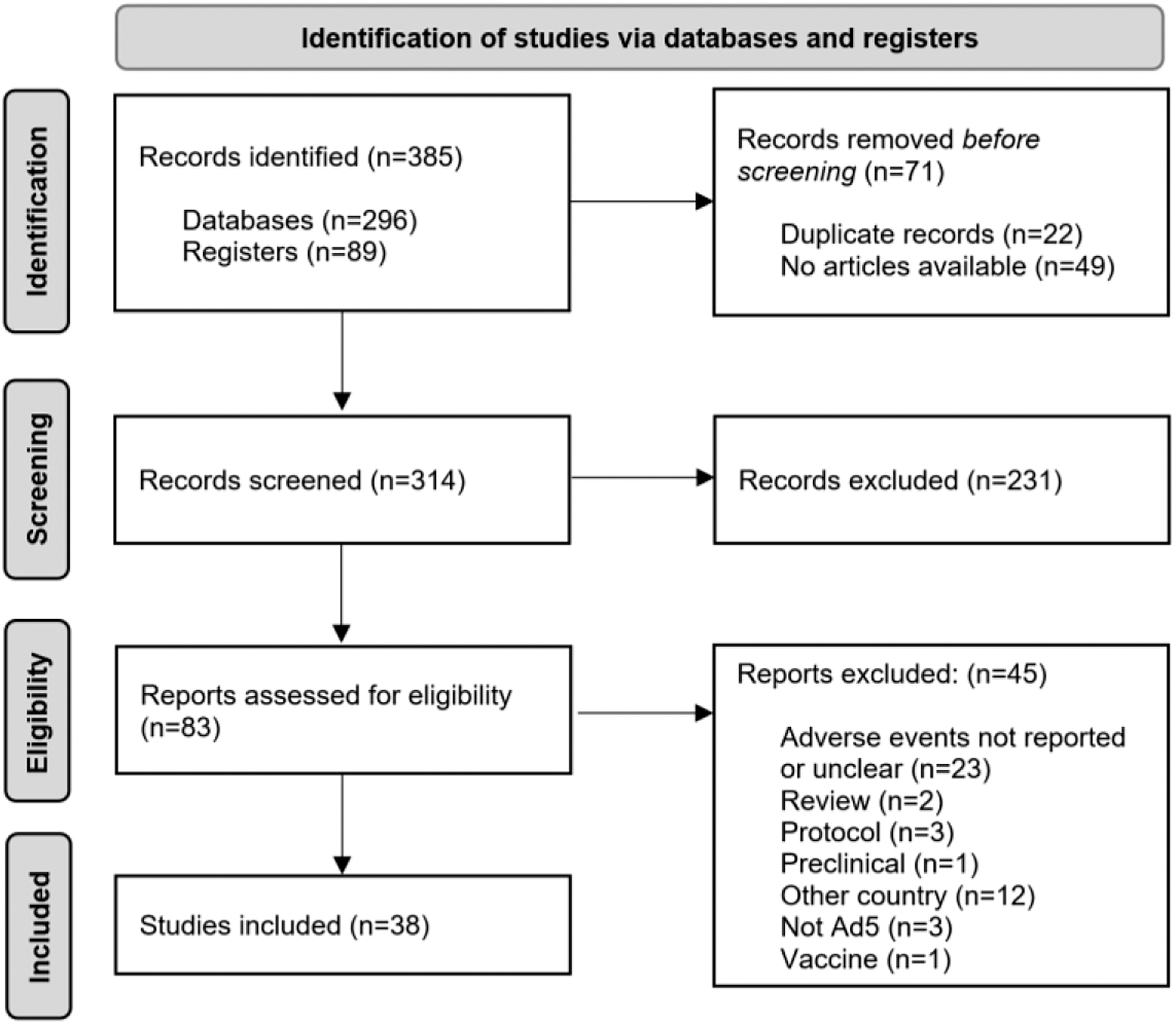
The PRISMA flow diagram of the identification and selection of relevant articles for this review.
Study Characteristics
There were 39 clinical trials (ct), comprising 756 patients (pts) treated with an intratumoral injection of an Ad5 or Ad5 chimera packaged experimental drug for cancer. As reported in Table 1, these trials encompass a variety of cancers: most commonly, prostate (9 trials), glioma or glioblastoma (6 trials), head and neck squamous cell cancer (HNSCC, 6 trials), and pancreas (4 trials). The majority of trials was phase I (25 trials) with 9 phase II trials. The Ad5 drug was given at varying dose levels, either in viral particles (vp, range 10e7–10e13) per injection or plaque-forming unit (pfu, range 10e6–10e12), but AE were not reported by dose level.
Trial characteristics and associated adverse events
Only trials that reported separate AE.
Trials with multiple co-treatments are counted individually.
Trials with multiple and single dosed arms are excluded.
One clinical trial reported breast and melanoma AE combined, reported, in this study, under breast.
Ad5, Adenovirus 5; AE, adverse events; HNSCC, head and neck squamous cell cancer; NSCLC, non-small cell lung cancer.
The trials included several mechanisms of action for the experimental Ad5-packaged drug with 17 (43.6%) trials using replication-competent adenovirus. There were 13 trials that investigated treatment with the experimental Ad5-packaged drug alone versus 12 trials that co-treated with chemotherapy, 16 with radiation, and 11 with surgery. If a clinical trial co-treated with multiple modalities, the sequence was chemotherapy followed by radiation and surgery. There were two trials that used different co-treatment modalities consisting of surgery versus chemoradiation, which were counted individually in the analysis.
CTCAE categories were used to report AE, but each trial varied in the number of categories that were reported (average 20.8, range 5–69). To limit site specific AE (i.e., mucositis) and ensure that the most frequent AE did occur over a broad range of trials, the most frequent AE were analyzed only if the category was reported in 10 or more trials.
Primary Outcome
Out of all 756 patients (Table 1), there were 3 (0.4%) grade 5 (mortalities) reported. All three deaths were in patients co-treated with both chemotherapy and radiation. In addition, all three patients received multiple doses of an immunomodulatory packaged Ad5 drug. Two deaths, one due to splenic artery thrombosis and one to progression of disease, were reported in a pancreatic cancer trial (Hecht 2012). The remaining mortality was due to hypoxic encephalopathy in an HNSCC trial (Seiwert 2013). There were five additional mortalities due to gastrointestinal hemorrhage, septic shock, disease progression, small bowel perforation in the pelvis from invasive carcinomatosis, and aspiration after an elective hernia repair, which were in drug-related trials and were not categorized as grade 5 AE by the investigators. 21,31,39,44
Secondary Outcomes
In total, there were 767 grade ≥3 AE among all the trials. Among separate value trials (n = 33), there were 468 serious grade 3 AE, and 86 life-threatening grade 4 AE. Among the 29 trials, which reported a total number of AE across all grades, the overall grade 4 and 5 rates were 1.4% and 0%.
Of trials that reported grade ≥3 AE (Table 2) by the number of patients, there were increased serious grade AE when comparing Ad5 co-treated with chemotherapy to Ad5 alone (36.1% vs. 16.0%, p = 0.03). Ad5 co-treated with radiation compared to Ad5 alone only had an increased rate of serious AE in the unedited trials (24.7% vs. 6.9%, p = 0.01). There was no difference seen across any trial that co-treated with surgery.
Serious (grade ≥3) adverse events compared by co-treatment and analyzed by number of patients and proportion of adverse events
Bold values indicate statistical significance.
Pt = patient; Grp = grouped (Grade ≥3); Sep = separated grades reported.
Compared to Ad5 alone.
Number of patients with serious AE (Grade ≥3) divided by the total number of patients in the trials.
In trials that reported total AE, Ad5 with chemotherapy had significantly more grade ≥3 (18.2% vs. 10.7%, p = 0.00), grade 3 (14.1% vs. 9.7%, p = 0.02), and grade 4 (4.1% vs. 1.1%, p = 0.00) AE when compared to Ad5 alone. Ad5 with radiation had significantly fewer grade ≥3 (7.4% vs. 10.7%, p = 0.01) and grade 3 (6.8% vs. 9.7%, p = 0.02) AE compared to Ad5 alone. There was no statistical difference when comparing Ad5 alone with the surgical co-treatment group.
Outcomes based on trial type
In trials that reported unedited AE, Ad5 co-treated with chemotherapy had significantly increased grade ≥3 (18.5% vs. 4%, p = 0.00), grade 3 (13.7% vs. 3.3%, p = 0.00), and grade 4 (4.8% vs. 0.7%, p = 0.00) AE when compared to Ad5 alone. Ad5 co-treated with radiation and Ad5 co-treated with surgery both had a statistically significant increase of grade 3 AE (radiation-6.7% vs. 3.3%, p = 0.04 and surgery 8.2% vs. 3.3%, p = 0.03).
In the trials that reported only drug-related AE, the only statistically significant difference was Ad5 co-treated with chemotherapy in grade 3 AE compared to Ad5 alone(8.6% vs. 4.7%, p = 0.01). There was no significant difference in the comparison of the other co-treatment arms.
Trials that reported only the most frequent AE, Ad5 co-treated with radiation had statistically significant fewer grade ≥3 (5.9% vs. 15.6%, p = 0.00) and grade 3 (5.9% vs. 15.1%, p = 0.00) AE than Ad5 alone. Ad5 co-treated with surgery also had significantly fewer grade ≥3 AE than Ad5 alone (7.5% vs. 15.6%, p = 0.00).
Results by grade of AE
Table 3 reports grade ≥3 AE with the highest frequency. Overall, lymphopenia was the most common serious (grade ≥3) AE (20.6%), followed by dyspnea (8.7%), neutropenia (8.6%), nausea (7.1%), hyponatremia (7.1%), transaminitis (6.8%), anemia (6.1%), headache (5.7%), and weakness (5.7%).
Most commonly reported adverse events (≥ 10 trials)
Bold values indicate statistical significance.
Chemo = chemotherapy; Rad = radiation.
Compared to Ad5 alone.
CTCAE, Common Terminology Criteria for Adverse Events.
The most frequent grade 3 AE were lymphopenia (17.2%), dyspnea (7.7%), and nausea (7.1%). Ad5 co-treated with chemotherapy was statistically increased in grade 3 leukopenia compared to Ad5 (11.1% vs. 0%). Ad5 co-treated with radiation was statistically increased in grade 3 lymphopenia (25.4% vs. 7% p = 0.02) and grade 3 hypernatremia (9.1% vs. 0% p = 0.05) compared to Ad5 alone. Ad5 co-treated with radiation was statistically decreased in grade 3 weakness compared to Ad5 alone (0% vs. 9.6% p = 0.00). Ad5 co-treated with surgery was statistically increased in grade 3 transaminitis compared to Ad5 alone (25% vs. 2.4% p = 0.00).
The most frequent grade 4 AE were neutropenia (4.6%), lymphopenia (3.3%), and leukopenia (3.1%). Ad5 co-treated with chemotherapy had statistically increased grade 4 neutropenia compared to Ad5 alone (19% vs. 0% p = 0.02). Ad5 co-treated with surgery was statistically increased in grade 4 anemia compared to Ad5 alone (8.3% vs. 0% p = 0.04). Common grade 4 AE reported in <10 trials were hyperbilirubinemia (4.4%), pneumonia (3.1%), and pulmonary emoblism (6.7%).
Multiple dosing and replication characteristic outcomes
Trials which dosed with either single or multiple injections (range 1–25 doses) and reported a total number of AE (grade 1–5) were compared to one another (Supplementary Table S1). The average number of doses in trials with multiple injections was calculated by using the minimum and maximum number of possible doses to determine a range (overall 4.4–6.2 doses). Overall, the multiple dosed trials had statistically significant more grade ≥3 (12.4% vs. 8.2%, p = 0.00) and grade 4 (2.2% vs. 0.3%, p = 0.00) AE when compared to single-dosed trials.
Trials that reported unedited AE had an average multiple dose range between 2.4 and 4.4. There was a statistically significant increase with multiple compared to single dosing in grade 4 AE (2.4% vs. 0.6%, p = 0.01). In drug-related trials, there was an average multiple dose range between 4 and 6.4. There was a statistically significant decrease with multiple compared to single dosing in grade 3 AE (5.6% vs. 13.3%, p = 0.02).
In trials reporting most frequent AE, the average dose range was between 7.8 and 8.7. With multiple compared to single dosing, there was a statistically significant increase in grade ≥3 (19.4% vs. 5.8%, p = 0.00), grade 3 (19.8% vs. 5.8%, p = 0.00), and grade 4 (2.5% vs. 0%, p = 0.00) AE.
AE were compared by replication-competent versus replication-incompetent Ad5 as replication-competent Ad5 continues to proliferate in the tumor cells and could be expected to cause more AE (Supplementary Table S2). The mechanism of action of replication-competent therapeutics was mainly oncolytic, except for 2 suicide drugs and 4 drugs, which were combinations of oncolytic with other mechanisms.
In trials reporting their total (grade 1–5) AE, there was a statistically significant increase of grade ≥3 AE (11.6% vs. 8.8%, p = 0.02) and grade 3 AE (10.7% vs. 7.6%, p = 0.01) in replication-competent Ad5 when compared to replication incompetent. In trials that reported only unedited AE, there was a statistically significant increase with replication competent in grade 4 (2.7% vs. 1.1%, p = 0.05) AE compared to replication incompetent. There was no other significant difference between replication-competent and replication-incompetent arms when comparing trials reporting drug-related or most frequent AE.
DISCUSSION
Gene therapy has the potential to revolutionize cancer treatment as we know it. To fulfill this promise, in addition to a sound experimental drug, an optimal delivery vector needs to be available. The use of adenovirus vectors will certainly expand the tool box for drug development. However, it is important that we critically evaluate all aspects of any innovation, especially its safety. A real safety concern about Ad5 as a viral vector was raised following the death of a young patient who was treated for an inherited enzyme deficiency.
Following this tragic event, there was reasonable cause for concern about the safety of Ad5 as a viral vector. 1 Multiple publications have investigated this specific incident and many questions were raised about the cause of the patient's death, including the possibility that the cytokine storm was a result of adenovirus exposure. The other possible causes were the administration of the clinical trial or drug. In brief, certain modifications to the protocol of that trail did not undergo IRB approval/review and there were unreported preclinical results, which made identifying Ad5 as the culprit of the death versus an uninvolved component challenging. 2,49
There are many advantages to Ad5 over other vectors: good transduction efficiency across a variety of cells, large packaging capacity, and low frequency of insertional mutagenesis. Withholding its use due to unfounded safety concerns could prevent real progress in cancer gene therapy. Likewise, overutilization without truly understanding the risks could be more detrimental to the field and to patients. To better quantify this risk, we investigated all available prospective clinical trial data with an emphasis on the most serious complications, specifically death and serious (grade ≥3) AE.
Ultimately, the risk for grade 5 mortality (0.4%) was extremely low, following experimental Ad5 treatments. In addition, all the reported mortalities were in unedited trials, which means disease progression or co-treatment-related AE were included. In fact, Ad5 seems unlikely to be the cause of any of these three mortalities (splenic artery thrombosis, progression of disease, and hypoxic encephalopathy). 26 Also, supporting Ad5 as the unlikely cause of mortality is the fact that none of these mortalities occurred in the adenovirus 5-alone group or in the trials reporting drug-related AE. There was also no death related to cytokine storm or overwhelming inflammatory response, which would have been the cause if it were Ad5.
In addition, all three mortalities were co-treated with 5-fluorouracil (5-FU) and radiation, which carry their own rates of morbidity and mortality. While chemotherapy has well-known AE, 5-FU has specific known AE of neutropenia, leukopenia, gastrointestinal toxicity, and hyperammonemic encephalopathy (<5.7%). 50,51 Radiation also causes adverse effects, such as nausea, vomiting, and weakness, as well as dependant effects of edema or fibrosis on targeted area. 52
There were five additional deaths reported in drug-related trials, which were not characterized as grade 5 AE by the principal investigators (PI) of the associated studies. It is reasonable to consider that these deaths were likely not caused by the Ad5 vector because all deaths were due to different underlying causes, such as an aspiration event after elective hernia procedure or disease progression, as well as the PI's judgment in not categorizing them as a grade 5 AE. 21,31,39,44 There was, however, one mortality due to septic shock which, without access to the medical records, could conceivably be a consequence of one of the therapies that the patient received. However, even if all five of these additional mortalities were included, the mortality rate would still be <1%.
The definition of our secondary outcomes was the rates of serious (grade ≥3), severe (grade 3), and life-threatening (grade 4) AE. These were examined across all studies, as well as by subgroup (unedited, drug related, and most frequent) to not inappropriately represent the AE and inadvertently skew our results. Comparing trials that reported the number of patients with serious AE was likely the most accurate method. Our analysis demonstrated that combinatory trials with chemotherapy or radiation had higher rates of serious AE.
However, this was not repeated when comparing the drug-related subgroup, likely indicating that the higher rate of AE was due to the co-treatment and not the experimental Ad5 drug or method of delivery. This would support our theory that Ad5 is a safe delivery vector. These trials also reported the number of patients with serious (grade ≥3) AE, but did not separate out individual grades, making it impossible to differentiate the severe versus life-threatening AE.
As only 13 trials reported AE by the number of patients, the proportion of serious to total AE allowed comparison across a larger group of trials. Across all trials, patients who underwent gene therapy through direct injection of an Ad5-packaged experimental drug alone reported low rates of serious (grade ≥3) AE (10.3%), which was significantly lower than when Ad5 was dosed in combination with chemotherapy (18.2%). In addition, the majority of AE were severe (grade 3) (9.7%), as opposed to life threatening (grade 4) (1.1%), and continued to be significantly lower than treatment with chemotherapy (14.1% and 4.1%, respectively). The trend of fewer grade 4 than grade 3 AE in drug-related and more AE in treatment with chemotherapy supports the safety of Ad5.
There was an unexpected finding of fewer grade 3 and grade ≤3 AE for Ad5 co-treated with radiation (9 trials, 138 pts) compared to Ad5 alone in all studies and the most frequent subgroup. Of the trials co-treated with radiation, 6 (67%) of these trials were in prostate cancer, which had a high rate (67%) of singly dosed regimens and were the only trials that recruited early stages of cancer, possibly leading to a healthier patient population. The opposite was seen in the unedited subset, possibly due to the fact that only 33% were trials in prostate cancer. There was no statistically significant difference in the drug-related subgroup, meaning that when looking at an experimental drug-related AE, there was no difference in AE in Ad5 alone and when co-treated with radiation and no difference in grade 4 AE across all subgroups.
The majority of the most frequently reported AE were laboratory abnormalities, such as lymphopenia, neutropenia, and hyponatremia or systemic symptoms, such as nausea, fever, and chills, all of which might be expected with the co-treatment. While one of the most frequent AE was dyspnea, the only grade 4 dyspnea occurred in lung cancer trials and could be attributed to disease progression, underlying co-morbidities, or the method of injection, but would require medical record review to be certain. However, the cause of the grade 3 dyspnea is more uncertain as it occurred in head and neck, prostate, and lung cancer trials.
The decision to examine only AE reported in 10 or more trials was to aid in limiting the number of cancer-specific AE; however, there were still several AE that appeared to be disease related, such as headache, which occurred in glioma and head and neck cancer trials. Another AE of interest was transaminitis as liver toxicity is a known effect of Ad553; however, the majority of cases were mild with only three grade 4 AE (2 in head and neck cancer trials and 1 in glioma). The only statistically significant transaminitis occurred in a single pancreatic trial, which co-treated with surgery, making it difficult to separate the disease and the treatment.
When comparing single versus multiple dosed trials, there was an increase in AE with multiple doses, except in drug-related AE. There was a significantly higher rate of grade 4 AE across all, except the drug-related subgroup. Interestingly, the drug-related subgroup had less overall grade ≤3 AE with a significant decrease in grade 3 AE. While an increase in AE with multiple doses and interventions would be expected, it is unclear why the drug-related subset had the opposite trend. One possibility is that the single dosed arm in the drug-related subgroup reported the fewest number of AE categories (12.7) compared to the other subgroups (28, 32, and 31 AE categories). In addition, there were only three trials with 26 patients in the drug-related AE single dose arm compared to 116 patients in the multiple-dose arm.
Ad5 can be engineered to be replication competent (i.e., oncolytic) or incompetent depending on the design of the experimental drug. When comparing these drugs, there appears to be an increase in AE with replication competent when comparing grade ≥3 and grade 3 AE across all studies, which is not repeated in subgroup analysis and is of unclear significance. There is also an increase of grade 4 AE in replication competent compared to replication incompetent in the unedited subgroup. The difference between these AE mainly comes from one study of metastatic sarcoma co-treated with chemotherapy.
In this one study, there were 9 (8.7%) grade 4 AE out of a total 104 AE in only 6 patients, compared to all the other studies that had a combined grade 4 AE rate of <2%. If this one study was excluded, the average grade 4 AE would drop to 1.3%, in line with the remainder of the trials. It is unclear why this one study has a higher rate of AE. More importantly, there does not seem to be any significant difference in AE when comparing drug-related studies, indicating that replication-competent Ad5 experimental drugs do not inherently indicate a higher risk.
In undertaking any comparison of multiple trials, the main difficulty is ensuring an equal comparison across studies. While the most accurate way would be to compare patients affected, only a small percent (34%) of trials provided these data. Therefore, the analysis mainly compared the proportion of serious AE across studies, which still provided a risk of AE, although not an absolute number.
In addition, while all trials used CTCAE to report their AE, varying number of categories were reported in each trial. While most articles specified the subtype of AE reported (unedited vs. drug-related vs. most frequent), those that did not specify were assumed to be unedited. However, the broad range of AE categories reported (5–69 categories) make it likely that even the unedited trials still reported AE with some amount of author discretion.
Another limitation is that most trials treated at multiple dose levels, but did not separate their AE by level, making it impossible to determine if the dose of Ad5 had an effect on the AE. Trials also did not specify their specific chemotherapy or radiation dosages or regimens, making this impossible to analyze. Additional studies reporting these data points will help to further study the safety profile of Ad5, as well as allow differentiation by invasiveness of procedure and stage of disease.
CONCLUSION
While there are still questions to be answered, the overall picture of this broad analysis supports the continued use of Ad5 as a safe delivery vector for oncologic gene therapy with relatively few AE, especially in terms of mortalities and life-threatening AE.
Footnotes
ACKNOWLEDGMENTS
The authors acknowledge Dr. Kelly Banas for gene therapy writing support.
AUTHORs' CONTRIBUTIONS
Y.S.: conceptualization (lead), formal analysis (lead), and writing original draft (lead). G.T.: writing original draft (supporting), and reviewing and editing original draft (lead). B.C.Y.: edited and reviewed (equal). E.K.: edited and reviewed (equal). N.P.: edited and reviewed (equal). S.W.: edited and reviewed (equal), and final approval of version to be published.
AUTHOR DISCLOSURE
No competing financial interests exist.
FUNDING INFORMATION
No funding was received for this article.
Supplementary Material
Supplementary Table S1
Supplementary Table S2
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.