
Abstract
Distant metastasis and primary tumor relapse are the two main hurdles to the success of surgical treatment for cancer patients. Circulating tumor cells (CTCs) and incomplete surgical resection are the primary cause of distant metastasis and local recurrence of tumors, respectively. Chimeric antigen receptor (CAR)-modified T cells target residual carcinomas and CTCs hold the potential to inhibit primary recurrence and reduce tumor metastasis, but the experimental evidence is lacking. Here, we developed a surgery-induced tumor metastasis model in immunocompetent mice to investigate the efficacy of CAR-T cells therapy in preventing metastasis and local recurrence. We observed that subcutaneous tumor resection has induced a large number of CTCs intravasated into circulation. EpCAM-specific CAR-T was effective in clearing CTCs following surgical removal of the tumor. This resulted in less pulmonary metastasis and longer survival in mice when compared to mice treated with surgery followed by Mock-T cells infusion. In addition, the local relapse was obviously inhibited at the surgical site followed by EpCAM-CAR-T cell treatment. This study demonstrated that CAR-T cell therapy can be an adjuvant treatment following surgery to prevent tumor metastasis and inhibit primary tumor relapse for cancer patients.
INTRODUCTION
Despite the emergence of cancer immunotherapy recently, solid tumors are still the leading cause of death. 1 –4 Surgical excision is the preferred therapy for early-stage tumor before metastasis. However, the incomplete tumor resection associated with positive surgical margins has increased the risk of relapse at the surgery site, which has a well-documented negative effect on clinical outcome, 5 especially for patients with advanced tumors. For those patients, local recurrence has a high prevalence and antirecurrence remains a challenge. Meanwhile, metastatic disease is another cause of reduced overall survival and adverse outcomes postsurgery. 6,7 Metastatic cancer has a high morbidity rate in patients and cause more than 90% of cancer-related deaths. 6,8 Since metastasis cannot be easily treated by second surgery, radiotherapy, or other regimens due to systemic disseminated cancer cells, 6,9 the prevention of metastatic disease also remains a challenge at present. 10 Thus, a feasible and efficient approach to clear residual tumor cells in the positive surgical margin and prevent metastasis is needed for patients postsurgery.
Growing evidence has been found that circulating tumor cells (CTCs) are a clinicopathological feature in early stage and a predictor for relapsed tumors and inferior clinical outcomes, 11 –16 which is the most predominant cause of tumor metastasis. 17 CTCs are a specific subset of tumor that sloughed from the primary tumor, circulated and survived in the circulatory or lymphatic systems, finally, infiltrated distant organs and developed multiple metastatic tumors. Stem-like phenotype helps CTCs retain metastasis-initiating capacity and maintains cellular plasticity, malignancy, and tumor-seeding potential. 18 As metastatic cancers represent the descendant of CTCs, elegant strategies targeting CTCs that prevent CTC formation and targeting CTCs survival would be effective in disrupting cancer metastasis. 19 –22 Hence, immunotherapy targeting CTCs might provide a feasible approach to interrupt metastasis formation.
The chimeric antigen receptor (CAR)-T cell therapy, which endows T cells with tumor-specific recognition and cytotoxicity, has achieved remarkable success in hematological malignancies. 23 –25 Many studies have replicated its success in treating solid tumors and obtained clinical benefits for patients with glioblastoma, 26 neuroblastoma, 27 or prostate cancer 28 and others. Therefore, CAR-T cell therapy is a promising immunotherapeutic paradigm for solid tumors.
Our recent preclinical data have confirmed the efficacy of EpCAM-specific CAR-T cells in treating epithelial tumors. 29,30 EpCAM is widely expressed on the basolateral membrane of epithelial tissue. 31 Overexpressed EpCAM in carcinoma is associated with tumor formation, growth, migration, metastasis, and epithelial-to-mesenchymal transition (EMT). 32,33 Meanwhile, most CTCs, originate from primary and metastatic tumors, have strong EpCAM expression. 17,34 Upregulated EpCAM expression in CTCs has been reported as a predictor for early distant metastasis and poor prognosis, leading to lower survival as well. 35 Inspired by the investigations above, we speculate that the use of EpCAM-specific CAR-T might be extended for use as adjuvant treatment to clear circulatory CTCs, prevent metastasis, and local recurrence following surgery.
To verify the assumption above, we developed a surgery-induced tumor metastasis model in mice and monitored CTCs by droplet digital PCR (ddPCR). We found that the formation of CTCs can be induced by subcutaneous tumor resection. Treating mice with surgery followed by EpCAM-specific CAR-T cell treatment, we demonstrated that CAR-T cells are effective in eliminating peripherally circulating CTCs, which resulted in pulmonary metastasis reduction. Meanwhile, due to the stable expression of EpCAM in primary carcinoma, there is a delayed primary tumor recurrence and growth after mice infusion of EpCAM-CAR-T cells. Our work has provided evidence that CAR-T cell therapy can be used as an adjuvant therapy to prevent metastasis and inhibit primary recurrence following surgical tumor removal.
MATERIALS AND METHODS
Cell lines and culture
The lentivirus packaging cell line HEK-293T was purchased from American Type Culture Collection (ATCC, Manassas, VA, USA). Murine cancer cell lines, including the colon cancer cell line CT-26 and the Lewis lung cancer cell line LL/2 were purchased from the Chinese Academy of Sciences. To obtain human EpCAM stable expression murine cancer cell lines, CT-26 and LL/2 cells were modified by human EpCAM gene and selected with 2.5 mg/mL puromycin for at least 48 h. HEK-293T and LL/2 cell lines were cultured in Dulbecco's modified Eagle's medium (Gibco, Waltham, MA, USA). CT-26 was maintained in RPMI-1640 medium (Gibco). All medium was supplemented with 10% (v/v) heat-inactivated fetal bovine serum (PAN, Aiden Bach, BY, USA), 100 U/mL penicillin, and 100 mg/mL streptomycin (Hyclone, Logan, UT, USA).
Murine T cells were obtained from lymph nodes of 8–10 weeks old C57BL/6 mice and cultured in RPMI 1640 medium supplemented with 10% (v/v) heat-inactivated fetal bovine serum, 100 U/mL penicillin, 100 mg/mL streptomycin, 2 mM L-glutamine (Gibco), 0.1 mM nonessential amino acids (Gibco), 1 mM sodium pyruvate (Gibco), 0.05 mM 2-mercaptoethanol (Gibco), and 100 U/mL mouse IL-2 (PeproTech, Rocky Hill, NJ, USA).
Animal
Six-to-eight weeks old C57BL/6 mice were purchased from the Beijing HFK Bioscience Co. Ltd. (Beijing, P.R. China). All animals were fed and bred under specific pathogen-free conditions in the Laboratory Animal Center of State Key Laboratory of Biotherapy. All animal experiments were performed according to the animal health care regulations of the Ethics Committee in State Key Laboratory of Biotherapy, Sichuan University.
EpCAM-CAR construction and lentivirus production
The human EpCAM-specific was screened by our research group. Signal peptide, hinge, and transmembrane domains were derived from murine CD8α. Mouse CD137 and CD3ζ are intracellular signaling activation domains. The EpCAM-CAR was synthesized by BGI and cloned into pCLK backbone. To prepare the lentivirus, EpCAM-CAR plasmid along with pSPAX2 and pMD2.G were cotransferred to HEK-293T cells with calcium phosphate at a 2:2:1 ratio. Forty-eight hours later, supernatant was collected and concentrated with ultracentrifuge, the lentivirus particles were enriched in the precipitate.
Flow cytometry
The expression of human EpCAM on the surface of tumor cells was detected by flow cytometry. Briefly, 5 × 105 tumor cells were obtained and washed twice with phosphate-buffered saline (PBS). Next, tumor cells were stained with 5 μL phycoerythrin (PE)-antihuman EpCAM antibody (Biolegend, San Diego, CA, USA) in a PBS buffer with 2% bovine serum albumin and incubated at 4°C for 30 min. For T cell analysis, 1 × 106 EpCAM-CAR-T cells or Mock-T cells were incubated with EpCAM-Fc protein (Novoprotein, Shanghai, SH, China), Pacific Blue antimouse CD3, PE-antimouse CD4, APC-antimouse CD8, PE-antimouse CD44, and APC antimouse CD62L (Biolegend) at 4°C for 30 min. Cells were then washed twice with PBS and stained with anti-Fc FITC (Jackson ImmunoResearch, West Grove, PA, USA) and incubated at 4°C for 30 min again. All samples were tested on a NovoCyte Flow Cytometer (ACEABIO, San Diego, CA, USA) and analyzed with NovoExpress 1.3.0 software (ACEABIO).
Production of EpCAM-CAR-T cells
To generate EpCAM-CAR-T cells, six-well plates were pretreated with 2 μg/mL antimouse CD3 and antimouse CD28 antibodies (BioLegend) at 4°C overnight. Murine T cells were separated from lymph nodes and cultured in the plates for 36 h to fully activate T cells. Next, activated T cells were transfected with EpCAM-CAR lentivirus under the condition of centrifugation at 2,500 rpm and 32°C for 1.5 h. Eight micrograms per milliliter polybrene was added to promote transfection. Eight hours later, T cells were transfected with EpCAM-CAR lentivirus as described above once more. After 48 h, EpCAM-CAR expression can be detected by flow cytometry.
Coculture assay and quantitative detection of cytokines
The cytotoxicity of EpCAM-CAR-T cells was detected by coculture assay. EpCAM-CAR-T cells or Mock-T cells were cocultured with 1 × 104 antigen-positive or negative cells in 96-well plates at indicated E:T ratio (10:1 and 5:1). Twenty-four hours later, the supernatant was collected. The secretion of mouse interferon-γ and tumor necrosis factor-α was quantified using an ELISA MAX™ Deluxe Set (Biolegend) according to the manufacturer's protocol.
Droplet digital PCR
Orbital blood of mice was collected at the indicated points, and the genomic DNA was extracted with Genomic DNA extraction kits (TIANGEN, Beijing, China). Next, DNA samples were mixed with PCR MIX (Naica, Boston, MA, USA), primers, TaqMan probe, and fluorescein and transferred to chip format. PCR reactions were performed according to manufacturer's protocol.
Forward primer for PCR: 5′-CTGTCATTTGCTCAAAGC-3′, Reverse primer for PCR: 5′-CTGCTTGGCCTTAAAGAG-3′, TaqMan probe for PCR: 5′-CAACTGCTATCACCA CAACCACAAT-3′.
Tumor model
For the tumor surgical resection model, C57BL/6 mice were subcutaneously inoculated with 3 × 105 LL/2-EpCAM cells. When the tumor volume reaches ∼500 mm3 (∼16 days later, defined as day 0), the primary tumors were excised with surgical operation. Afterward, all mice were randomly grouped into three groups, six mice per group. Next, three doses of 3 × 106 EpCAM-CAR-T cells or Mock-T cells were infused via the tail vein on days 1, 3, and 5. Pulmonary metastatic foci were counted when mice were sacrificed. Orbital blood was collected as designed to calculate circulatory CTCs levels by ddPCR. Local recurrence was tested by monitoring tumor volume at the surgery site.
Statistical analysis
Data analysis was performed with GraphPad Prism 5.0 software and presented as the mean ± standard deviation unless otherwise indicated. Mouse IFN-γ and TNF-α secretion and numbers of metastasis in the animal model were analyzed with Student's t-test. One-way analysis of variance (ANOVA) was used for the analysis of human EpCAM gene copies and tumor volume. Mouse survival was analyzed with Log-rank test. p < 0.05 was considerate statistically significant.
RESULTS
In vitro antitumor activity of EpCAM-specific CAR-T cells
In elevating the antitumor activity of the EpCAM-CAR-T cells, we engineered a CAR incorporated murine CD8α signal peptide, human EpCAM-targeted single chain variable fragment (scFv) with a murine CD8α hinge and transmembrane domain, and murine 4-1BB and CD3ζ signaling domains (Fig. 1A, B). Murine T cells, separated from lymph nodes, were engineered by the CAR-carrying lentivirus. As presented in Fig. 1C, EpCAM-CAR can be stably expressed on the surface of murine T cells after 48 h transduction. Approximately 36% of T cells were identified as EpCAM-CAR-positive T cells. After 7 days of culture in vitro, majority of cells in the system were CD3-positive cells (Fig. 1D). EpCAM-CAR-T cells have differentiated more CD4-positive subtype compared to Mock-T cells (empty lentivirus modified murine T cells without CAR gene). Meanwhile, EpCAM-CAR-T cells have maintained more naïve phenotype (CD44-CD62L+) and less effector subset (CD62L−) when compared to Mock-T cells indicated lower differentiated level of CAR-T cells (Fig. 1D).
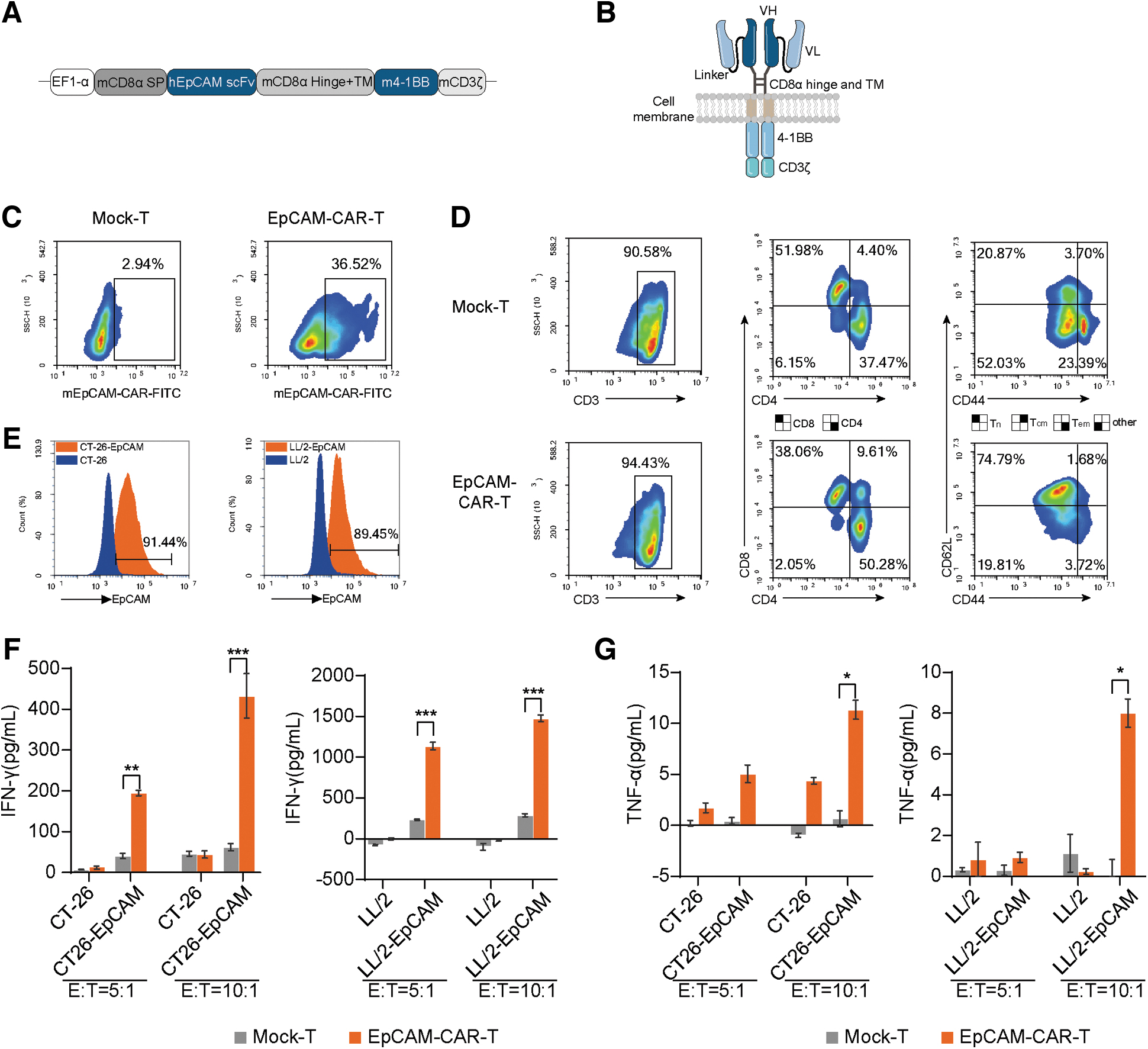
Characteristics of EpCAM-CAR-T cells.
To test tumor cytotoxicity of EpCAM-CAR-T cells, human EpCAM was stably overexpressed on the surface of CT-26 and LL/2 cells (Fig. 1E). EpCAM-CAR-T cells and Mock-T cells were, respectively, cocultured with a panel of human EpCAM-positive tumor cells or wild-type tumor cells at different effector to target ratio (E:T) for 24 h. We observed that there was increased cytotoxicity-related cytokines (IFN-γ and TNF-α) secretion after EpCAM-CAR-T cells cocultured with antigen-expressing tumor cells. In contrast, wild-type tumor cells, which were antigen-negative, cannot activate CAR-T cells or induce obvious cytokine secretion (Fig. 1F, G). The evidence demonstrated that EpCAM-CAR-T cells hold EpCAM-specific cytotoxicity for EpCAM-expressing tumor cells.
EpCAM-CAR-T cells reduce pulmonary metastasis after surgical tumor resection of mice
Many studies have elucidated the possible factors that result in tumor dissemination, such as surgical tumor resection. 7,36 In this study, we developed a model that subcutaneous tumors were surgically resected to model advanced metastatic disease. 3 × 105 EpCAM-expressing Lewis lung cancer (LL/2-EpCAM) cells were subcutaneously inoculated to C57BL/6 mice. Sixteen days later, mice were treated with surgery to remove primary tumor when the tumor volume reaches ∼500 mm3. Subsequently, three doses of 3 × 106 EpCAM-CAR-T cells or Mock-T cells were intravenously administered at days 1, 3, and 5 (Fig. 2A). As shown in Fig. 2B, multiple pulmonary metastasis emerged in mice treated with normal saline (NS) after surgery. Meanwhile, after surgical tumor resection, we counted lung metastatic foci and found that EpCAM-CAR-T cells effectively reduce pulmonary metastasis compared with mice treated with others (Fig. 2C). Similar results were further observed in lung pathological examination, mice treated with NS, and Mock-T cells have obviously increased numbers of pulmonary metastasis and higher tumor burden, which was significantly reduced in mice with administration of EpCAM-CAR-T cells (Fig. 2D). These findings demonstrated that EpCAM-CAR-T cells have shown anti-metastasis potential following surgery.
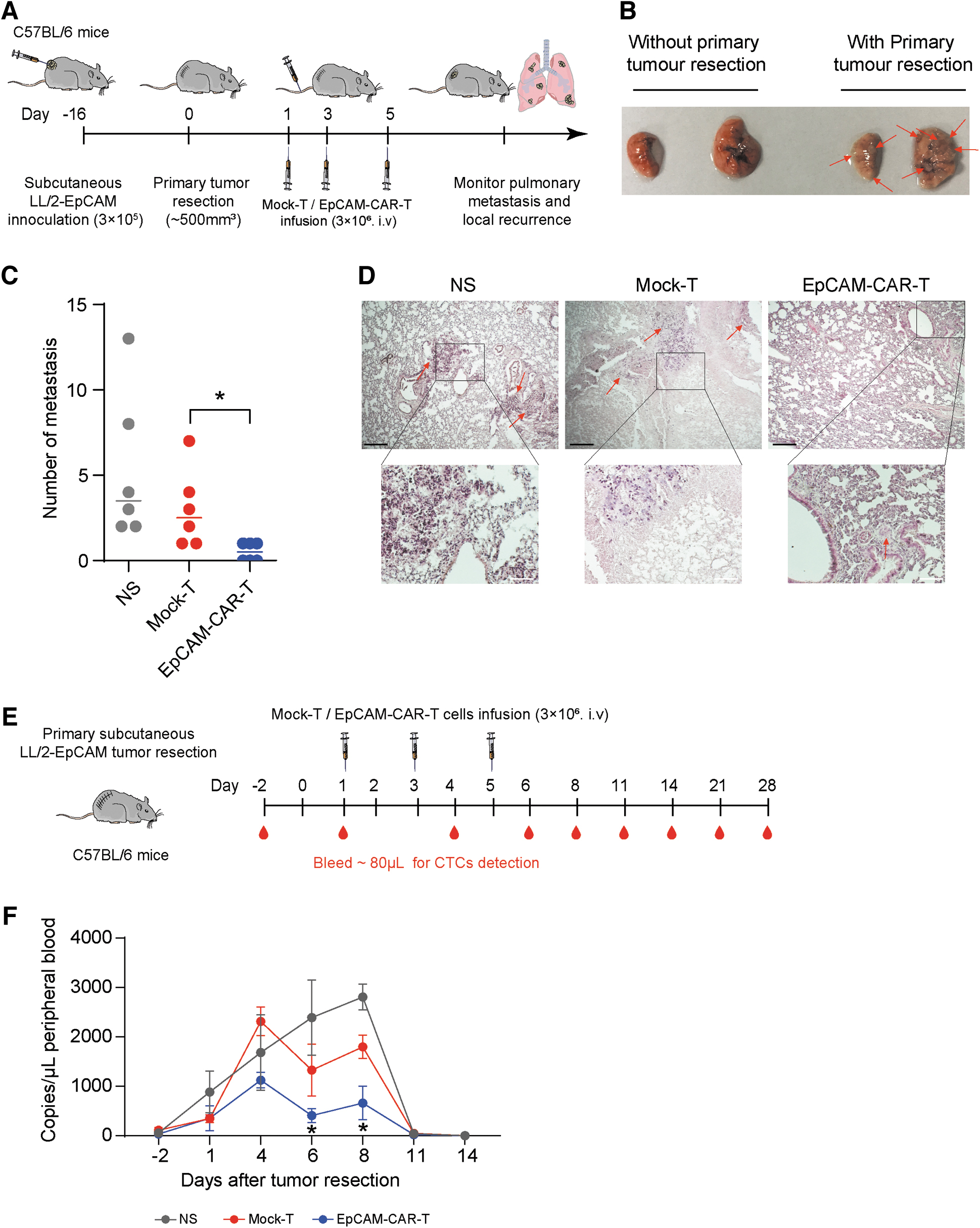
EpCAM-CAR-T cells reduced pulmonary metastasis when mice were treated with surgery following CAR-T cells infusion.
Meanwhile, to further explain the findings above, we monitored CTCs in mice peripheral blood by ddPCR. As EpCAM is a reliable surface molecule for CTCs, we collected mice orbital blood and identified CTCs with human EpCAM gene-specific ddPCR at indicated points (Fig. 2E). As shown in NS-treated mice, CTCs shed from primary tumor intravasated into bloodstream in a short time and reached the peak in vascular system after 8 days of surgical tumor resection. Finally, survived CTCs seed metastases at distant organs and decreased undetectable level after 11 days of circulation and survival in vascular system. In this process, Mock-T cells-treated mice have similar CTCs dynamics with NS-treated groups. However, mice received administration of adoptively transferred EpCAM-CAR-T cells has significantly decreased CTCs numbers in circulation after 4 days of surgical tumor resection, especially on days 6 and 8 (Fig. 2F). These findings provide evidence that CTCs have been captured and demolished by EpCAM-CAR-T cells. Furthermore, considering the results observed from pulmonary metastasis (Fig. 2C, D), there are reasons to prove that EpCAM-CAR-T cells could be used as an adjuvant therapy to target and clear circulatory CTCs and prevent the formation of metastases.
EpCAM-CAR-T cells inhibit primary tumor relapse
The unresected surgical margin remains a high risk for primary tumor relapse. 37 Since our previous researches demonstrate the curative activity of EpCAM-CAR-T cells for epithelial tumor, we speculated that the EpCAM-CAR-T might have effects on local tumor recurrence and regrowth after surgical resection. To further validate the assumption, we evaluated the primary relapse burden of the mice after surgery (Fig. 2A). We found that the majority of mice experienced primary recurrence after the initial surgical tumor resection (Fig. 3A). Rapidly progressive tumor regrowth was observed in NS- and Mock-T-treated mice after surgery, while mice that received EpCAM-CAR-T cell infusions showed delayed tumor recurrence and growth. Meanwhile, mice treated with EpCAM-CAR-T cells have obtained longer survival benefit compared to other groups (Fig. 3B). Therefore, these results demonstrated that intravenously delivered EpCAM-CAR-T cells showed antitumor efficacy at the surgical site.
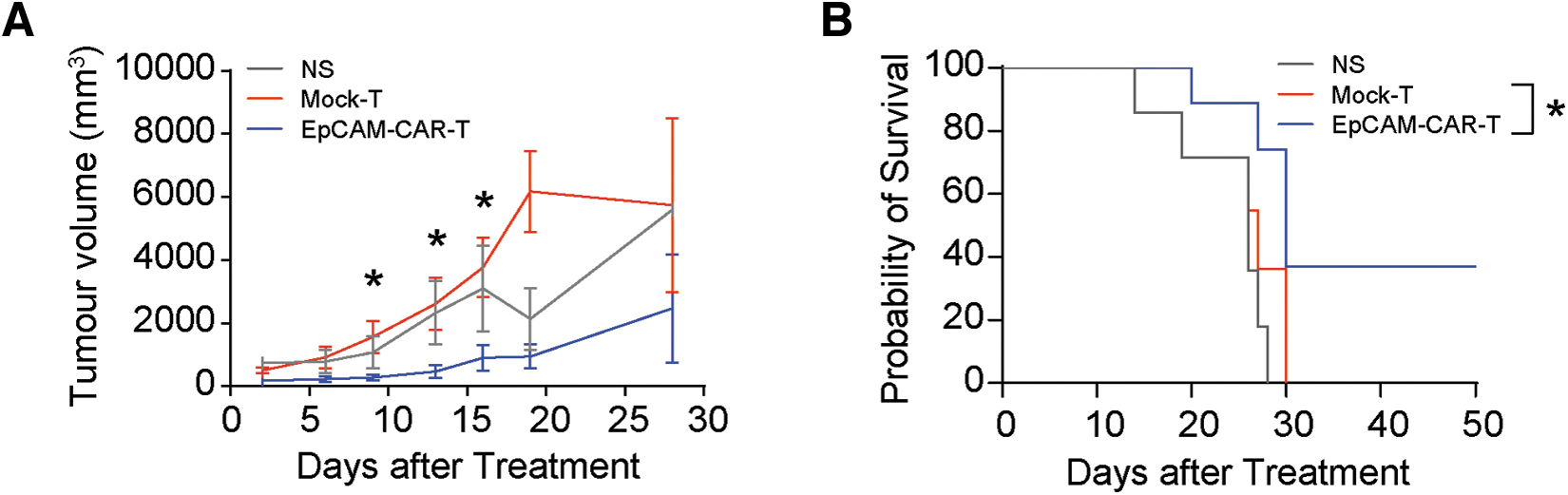
EpCAM-CAR-T cells inhibit local recurrence and prolong survival of mice.
DISCUSSION
As an integral part of treatment options for cancer, surgical resection has played a critical role in the treatment of lung cancer, 38 prostatic cancer, 39 and others solid tumors. However, unresectable surgical margins would increase the risk of local recurrence and result in poor prognosis, as well as reduce overall survival of patients. 37,40 For nonsmall cell lung cancer, 30–50% of patients experience relapse and metastasis, and die from the cancer in 5 years after surgical resection. 7 Thus, it is worth preventing tumor recurrence and metastasis through an adjuvant treatment after surgery.
A recent study reported that mesothelin-specific CAR-T cells can be used as an adjuvant therapy to clear residual tumor cells after incomplete surgery in preclinical models, and verified the antirelapse activity of CAR-T cell therapy. 41 Similar results were further confirmed in this study (Fig. 3), suggesting the use of CAR-T cells may be useful in inhibiting local recurrence during surgery. Of note, there are slight differences in the final antirelapse outcomes of treatment in this research compared with the previous study, 41 which may be triggered by different delivery pathways of T cells as the local delivery pathway is more efficient compared with systemic infusion in trafficking CAR-T cells into the tumor mass and achieving persistence and tumor eradication. 26,42 Of course, to further confirm the antirelapse benefit of locally administered CAR-T cells, more in vivo experiences are needed.
In this study, we observed successful elimination of CTCs by EpCAM-CAR-T cells (Fig. 2). As most carcinomas are derived from malignant transformation of epithelium, EpCAM is a universal surface marker of epithelial tissue. Hence, EpCAM is also a reliable surface marker for CTCs in the majority of epithelial cancer. 17 Despite the fact that many CTCs have low or negative EpCAM expression, they downregulate EpCAM expression in the process of EMT for many types of cancers. 43,44 EpCAM-positive CTCs are a substantial subset of all CTCs. 45 The clinical diagnostic and prognostic values of EpCAM-positive CTCs have been validated in numerous clinical researches, especially in prostate cancer and triple negative breast cancer. 46 For these tumor diseases, EpCAM could still be a substantial marker for capturing CTCs.
Meanwhile, since CTCs have dissociated in vascular system from primary site, CTCs-direct CAR-T cells could not be limited by microenvironments and physical barriers from tumor matrix. 47 The CAR-T cells can eliminate CTCs with high efficiency, which may decrease the success of distant metastasis postsurgical operation.
It is known that metastasis is a late event for cancer progression, but metastatic dissemination often occurs early during tumor formation, especially for breast cancer and pancreatic cancer. 48 –52 Previous study found that 80% of metastases in mice are originated from early dissemination cancer cells in breast cancer. 51 For patients, CTCs detection rates at Tis and T1 stage of breast cancer were 50% and 81.67%, 11 suggesting that CTCs may spread before visible tumor is present. Meanwhile, premalignant cells enter the bloodstream in the early stages of pancreatic carcinogenesis, and distant metastasis even occurred before tumor evolution in the primary site. 50 These accumulated results demonstrated that CTCs circulation is likely to be an earlier event in tumor formation.
In this study, although the EpCAM-CAR-T cells displayed anti-metastasis activity, very earlier CTCs dissemination and seeding may cause minimal residual metastasis (Fig. 2D). Thus, it is worth considering that CAR-T cell therapy should be administered in the early stages of tumor or combined with radiotherapy or other treatment regimens before early disease progression, and further used to prevent CTCs plantation and metastasis formation, which will be studied in our future research.
In summary, EpCAM-CAR-T cells can be used to treat epithelial carcinoma. It can be broadened for use as a surgical adjuvant treatment to prevent postoperative metastasis, which benefits from the efficient circulatory CTCs clearance efficacy of CAR-T cells. Meanwhile, CAR-T cell therapy is an alternative adjuvant therapy to inhibit local recurrence and postsurgical progression. Therefore, our research provided preclinical evidence about the application of CAR-T cell therapy in preventing metastasis and local recurrence.
Footnotes
ACKNOWLEDGMENTS
We thank the staff of animal platform of the State Key Laboratory of Biotherapy, Sichuan University for their advice on animal experiments.
AUTHORs' CONTRIBUTIONS
W.W. designed the whole investigation. D.L. and L.J. performed the experiments; Y.H., W.Z., J.L., S.T., X.G., Q.X., and J.Y. provided important suggestions and materials, and J.L., F.W., Y.Z., Y.Y., and F.Y. analyzed the experimental data. D.L., W.Z., and W.W. edited the manuscript.
AUTHOR DISCLOSURE
No competing financial interests exist.
FUNDING INFORMATION
This work was supported by National Key Research and Development Program of China (2020YFC0860200), National Natural Science Foundation of China (81972878 and 82172733) and Key Research and Development Program of Sichuan Province (2022ZDZX0024).