
Abstract
Little is known about patients' and families' lived experiences of participating in pediatric gene therapy (GT) clinical trials. Currently, pediatric GT research targets a broad range of indications––including rare and ultra-rare diseases––which vary in severity and in the availability of alternative therapies. Pediatric GT differs meaningfully from adult GT because the decision to participate involves a dyad of both the child and parent or caregiver/s. It is critical to understand patients' and caregivers' perceptions and experiences of social, emotional, physical, and logistical burdens or benefits of participating in such trials, and how they weigh and prioritize these factors when deciding whether to participate. We conducted a scoping review of the current literature in this subject area with objectives to (1) provide an overview of existing literature, (2) identify gaps and areas for further research, and (3) better understand the lived impact of pediatric GT research on patients and their parents/caregivers. Four themes emerged, including (1) weighing risks and benefits (2) timing of GT trial participation, (3) value of clear communication, and (4) potential impact on quality of life. Notably, our sample surfaced articles about how patients/parents/caregivers were thinking about GT—their understanding of its safety, efficacy, and risks—rather than accounts of their experiences, which was our initial intention. Nevertheless, our findings offer useful insights to improve the informed consent process and promote a more patient- and family-centered approach. Moreover, our findings can contribute to patient advocacy organizations' efforts to develop educational materials tailored to patients' and families' expressed informational needs and perspectives, and can inform more patient- and family-centered policies from GT clinical trial sponsors.
Introduction
Lived experience refers to the subjective and personal experiences of people who have a particular medical condition. In the context of clinical trial participation, the term refers to the unique perspectives, needs, preferences, and concerns of trial participants and their caregivers who have direct experience with the condition being studied. In the specific context of this review, lived experience encompasses how pediatric patients and their caregivers make decisions and think about gene therapy (GT) research, and how they make meaning of trial-related emotional, social, and ethical trade-offs that impact their lives and illness experience.
This encompasses a range of scenarios, including engaging in, considering, declining, and desiring GT research opportunities, among others. The objectives of this scoping review are to (1) provide an overview of existing literature in this area, (2) identify gaps and areas for further research, and (3) better understand the lived impact of pediatric GT clinical trial participation on patients and their caregivers (often their families). 1,2 It is critical for the field that stakeholders understand the full family experience of pediatric GT; this is the rationale behind this review.
GT research currently targets a broad range of rare diseases for which few or no treatment exists. More than 90% of rare diseases currently lack an U.S. Food and Drug Administration (FDA)-approved treatment. 3 Rare diseases are particularly devastating in pediatric populations; two out of three rare diseases appear before 2 years of age, causing 20% of infant mortality and 10% of pediatric hospitalizations, and 30% of rare disease patients die before the age of 5. 4 Candidate and approved GTs are often long-awaited and highly anticipated methods of treatment for individuals with such unmet needs.
To date, eight GTs have been approved by the FDA, with an estimation by the head of FDA's GT review division that, by 2025, the agency “will be approving 10 to 20 cell and gene therapy products a year based on an assessment of the current pipeline and the clinical success rates of these products.” 5,6 Presently, for many children with rare diseases, enrolling in a GT clinical trial might be their only opportunity to access what they might perceive to be a “curative” treatment.
When making a decision about whether to enroll a child in a GT clinical trial, caregivers must weigh factors such as the inability for most treatments to be repeated or re-dosed; uncertainty around the durability, efficacy, and safety of an experimental treatment; risk of a child's disease progressing if they wait for an approved treatment or more safety data; and efficacy of existing approved alternative treatments. 5 –7 While GTs offer novel opportunities, they also pose opportunity costs, along with possible risks of significant adverse events (SAEs). 8 The confluence of these factors within a high-stakes decision-making framework creates a unique ethical context for pediatric rare disease patients and their parents and caregivers. The progressive nature of many of these diseases also adds a time constraint to participation.
In addition to medical factors, trial participation involves inherent logistical hurdles such as traveling to a trial site (often located in urban academic medical centers), travel expenses, missing school (for child patients), taking leave from work and potential loss of income (for adult caregivers), and adjustments to disrupted living circumstances, including for siblings or extended family members of the trial participant. 9 Nevertheless, qualitative research on the lived experience of participating in a GT trial is surprisingly sparse. As Addison and Lassen note, the field lacks human stories of GT and critical perspectives in the development of evidence-based informed consent and decision-making support practices. 1
There are many factors that complicate the decision to pursue GT as a treatment. Most GTs are delivered through a viral vector, wherein the viral DNA is removed and replaced with the transgene containing the “correct” copy of the disease-causing gene. Because GT recipients develop innate and adaptive immune responses to the vector being used, GTs can currently only be delivered once—a factor that impacts the assessment of risks and benefits and increases the stakes of trial participation. In addition, the lack of efficacious treatment options for many rare diseases raises concerns that this paucity of treatment options may impact decision makers' assessments of possible risks and benefits of an innovative treatment.
Within the context of sparse alternative treatments for many rare diseases, there is often great urgency around trial enrollment and gaining access to an ongoing GT trial. Interviews with adult sickle cell disease (SCD) patients, for instance, found gaps in their understanding of the prolonged time interval between scientific discoveries and the commencement of trials and subsequent regulatory approvals; patients worried that the time frame of GT development might not match their own limited therapeutic window, especially as their conditions deteriorated. 10 Not only does this likely cause stress for families but it also underscores the need for greater transparency and improved informed consent practices that address a patient's and their family's experiences of living with a rare disease and how they navigate treatment uncertainty. 11,12
Bluebond-Langner et al. 13 (p.469) note that for families of children with life-limiting conditions, “the definition of what constitutes ‘normal’ is altered to accommodate the child's changing condition and family life,” and parents will hold their own views of their child's status and well-being, even if they diverge from those of the clinician.
Pediatric GT differs meaningfully from adult GT in that many pediatric participants are too young to provide informed consent, so parents/surrogates must make decisions on their behalf. For pediatric GT trials, the risks will differ depending on a potential participant's rare disease, age, disease progression, and myriad other factors that must be assessed by the decision maker. There is a fair amount of literature examining adult patients' perspectives on the benefits and burdens of GT.
These accounts in the adult patient population suggest that some GT recipients have had a positive, life-changing experience that improves their lives in ways that outweigh the burdens of living with their rare disease. 14 This view of GT as a “cure” reflects elements of therapeutic misconception, wherein people may conflate the intended goals of research (to produce generalizable knowledge) and treatment (to confer individual benefit). It is reasonable that the line between the two becomes more blurry for children with rare diseases for which the experimental intervention is the only candidate treatment, thus underscoring the need for transparency between researchers, clinicians, and trial participants and their caregivers about trial aims and the participant's prospect of benefit. 11,15,16
Given that the field of pediatric GT is relatively young, and the literature is still emerging in this area, we chose to conduct a scoping review. This methodology is specifically designed to assess content areas where evidence is not yet fully developed and enabled us to cast a wide net across heterogeneous research methodologies to identify gaps where more inquiry is needed. 2
RESEARCH DESIGN AND METHODS
Our study followed the guidelines from the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA ScR; PRISMA extension for scoping reviews). 2 We included English language-only empirical research articles published any time before July 2021. Studies of other genetic treatments such as cell therapy, antisense oligonucleotides, Clustered Regularly Interspaced Short Palindromic Repeats, and articles on germline editing were excluded. Normative or conceptual articles and studies in which only adult perspectives were represented or in which findings were aggregated and pediatric patients' and families' perspectives could not be assessed independently were also excluded. No disease/condition was excluded to allow for inferences across multiple disease areas.
For our search strategy, we followed a rigorous search process with robust assistance from a librarian at NYU Grossman School of Medicine (Appendix A1). Database searches conducted on PubMed, Embase, and CINAHL produced 778 articles. An additional 55 articles were identified for inclusion through manual searching. After removing duplicates, 590 articles met criteria for abstract review. Two members of our team (L.K. and C.H.) conducted abstract reviews, and 59 articles were selected for full text review. These 59 articles were divided into three groups and partnered pairs from our subgroup (L.K./A.B.H., C.H./M.V., and E.J./K.B.) conducted full text review for all articles in each group. L.K. served as final arbiter on all articles and resolved any discrepancy within each pair. The final sample consisted of 10 empirical research articles meeting inclusion criteria (Fig. 1).
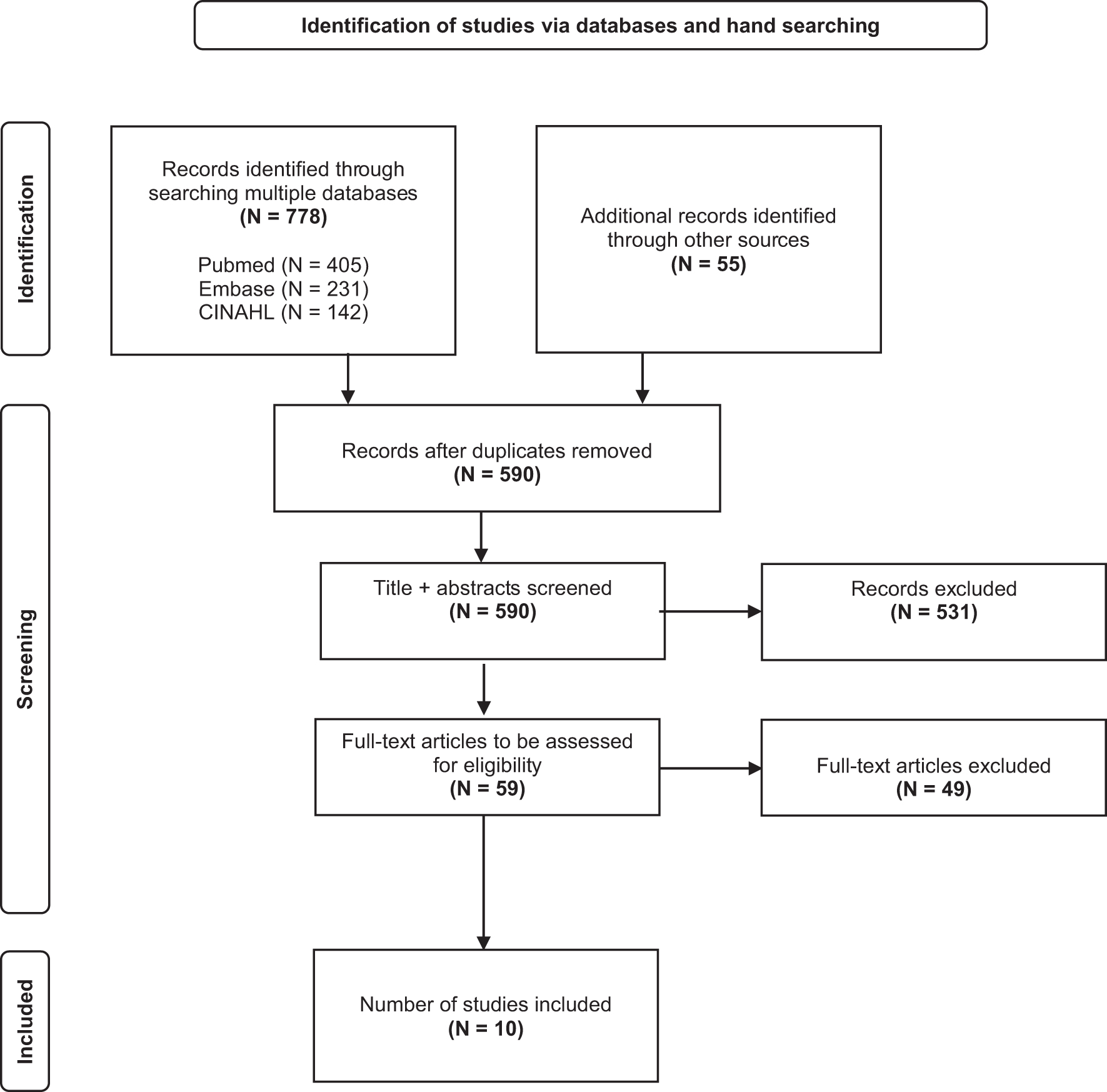
Flow diagram of database searches, screening, and identification of final sample set. From Tricco et al. 2
Data were charted using a standardized data extraction tool developed by the team with input from subgroup members to capture relevant domains within the sample. Before implementation, the data extraction tool was piloted by 6 team members using two sample studies. Two reviewer pairs (L.K./A.B.H. and C.H./J.D.B.) then completed full data extraction on the 10 studies in the final sample, with each pair extracting and charting data from 5 studies. Charted data were analyzed by L.K. and C.H. by synthesizing data across all 10 studies to identify key themes.
While the aim of this review was to assess literature on the lived experience of pediatric patients and their families who are participating in GT clinical trials, it is important to note that most articles in our sample addressed attitudes and perspectives toward GT rather than the actual, lived impact of the trial on their lives, further highlighting the gap in this area of research.
RESULTS
Ten articles met criteria for inclusion in the final sample. The sample included five mixed-methods studies, four qualitative studies, and one study that was qualitative/mixed methods. Three studies were conducted in the United States, two in Canada, one in Japan, one in United Kingdom, one in The Netherlands, one in Australia, and one did not specify. Seven studies used convenience sampling, one used snowball sampling, and two did not specify a sampling technique. Target conditions of GTs in our sample included Angelman syndrome (AS), type 1 diabetes, inherited retinal disease, Hemophilia A and B, and Duchenne Muscular Dystrophy (DMD). A variety of qualitative methodologies were employed across the studies, including focus groups, case studies, surveys, and interviews (Table 1).
Articles in final sample for full-text analysis
DMD, Duchenne muscular dystrophy; MAR, maximum acceptable risk.
Key themes are explained below. As mentioned, most articles in our sample set addressed attitudes and perspectives toward GT rather than the actual, lived impact of the trial on their lives, underscoring the need for more data collection in this area of research.
Weighing risks and benefits
Detailed portrayals of how families weigh the risks and benefits of GT for their child predominately appear in forums and media, that is, blogs, Facebook pages, online forums, webinars, and in-person group meetings, making it difficult to fully assess, within academic literature, those factors that matter most to families facing complex medical decisions. Furthermore, the prognosis and characteristics specific to a rare disease color the way families approach their assessments, making it difficult to claim anything universal about “the risks and benefits” of GT.
Even with this limitation, most studies in our final sample effectively examined some of the risk/benefit calculations that families make, in which they balance trial risks against their child's ability to cope with their chronic condition and expected symptom-free interval times. Contrary to concerns that parents may suffer from therapeutic misconception or unrealistic optimism, participants from our sample studies differentiated between hope and expectation. Parents considered the advantages of not enrolling in the clinical trial—including avoidance of trial risks or waiting for advanced therapeutic medicinal products (ATMPs) with a greater safety profile—against the continued clinical deterioration of their child. Many parents/caregivers were uncomfortable with enrolling their child in a first in-human clinical trial, but would consider a later stage trial with a pediatric safety and efficacy profile.
Some of the themes of risk/benefit calculation that Brooks and Bubela highlighted in their study of motivating theories in clinical trial enrollment for pediatric chronic conditions were (1) fear of adverse events; (2) desires to wait-and-see/hold out for better treatment options; and (3) fears about receiving a placebo. 17 Fear of adverse events as a part of the threat appraisal was a predominant consideration for parents who were deciding whether to enroll their child living with a manageable, chronic condition in a pediatric trial of an ATMP, an umbrella term that encompasses GT. 17
Paquin et al.'s study of Duchenne caregiver priorities found that many, but not all, participants reported a willingness to trade a 1% risk of treatment-related death for the anticipated benefits, even for a one-time administration with time-limited benefits. 18 This optimism could reflect or be shaped by the Duchenne advocacy community sampled in the research enterprise; DMD is in the top 25 diseases with the most orphan drug designations. 19 They have conducted their own research on patient preferences and risk profiles, potentially reducing concerns about risks. 20,21
Brooks and Bubela found that parents/caregivers considered whether to take on the risks for GT, or whether to wait-and-see until there was progress in safety and efficacy data. 17 On the other hand, Paquin et al. found their participants exhibit a “therapeutic optimism” reflected in the negative perceptions of many participants about loss of eligibility for future trials, especially among parents of younger children. 18 Certainly, calculating how long to “hold out” will differ depending on the severity of a disease. Notably, in Peay et al.'s study of Duchenne caregivers, the authors found that burdens of DMD (i.e., child's ability to cope with the condition and expected symptom-free interval time) may be associated with willingness to accept serious risks for a noncurative treatment. 22
Risk tolerance is not, however, an absolute. While more than half of the parents/caregivers in Peay et al.'s study tolerated a hypothetical 1% risk of death when balanced against DMD progression and limited treatment options, many parents expressed unwillingness to tolerate trials that were deemed “too risky.” 23 Some parents/caregivers were uninterested in trials designed with placebo arms, “because of wished for benefit in exchange for assumption of risk,” and still others preferred to defer risk of trial enrollment “until a highly valued function was about to be lost.” 23
In van Balen et al.'s study, authors examined factors that influenced hemophilia patients' and their parents' decision making about switching to a new treatment option. 24 Participants expressed concern about short- and long-term safety and believed the effects of GT were not sufficiently well understood, with some expressing a “wait-and-see” attitude for novel treatments writ large.
Some parents/caregivers also pointed to burdens of weighing risks and benefits in their role as a surrogate. In a study of parental perspectives on GT for children with hemophilia, Khair et al. recorded weights on risk/benefit calculation specific to decision making on behalf of one's child as they matured through adolescence. 25 Parents reflected that because GT fundamentally changes a person, with the responsibility of making a decision for a child, there is, “potential for future rebellion from the child due to the parent making the decision for them,” and that taking hemophilia away from a child when it could be a large defining part of them could pose additional risks that are unique to GT. 25
Timing of GT trial participation
Timing was a theme that arose repeatedly, both in terms of patients' current and expected disease trajectories and the development timeline of novel GTs for specific conditions. Many parents/caregivers noted how learning about and understanding the impact of GT trials take a significant time investment, and they called for thorough communication processes that would enable them to make informed decisions. While time is of the essence, for those living with rare diseases, there may be little to no time for actively learning about or participating in meetings on new medicine, given the significant time burdens in parents/caregivers' day-to-day lives of caring for children with rare diseases. 26 Certainly, time to learn about trials and urgency will vary depending on disease severity. However, when designing and communicating about GT clinical trials, it is important to keep such burdens in mind to ensure that additional stresses are minimized.
The amount of time necessary to prove that GT was successful also influenced the decision to enroll in a trial. For some hemophilia patients, Costea et al. found that participants “appeared content to wait for strong evidence to become available, before considering enrolling in a clinical trial of gene therapy.” 27 A majority of their respondents (65.4%) considered a time period range between 1 month and 1 year to be acceptable symptom-free time period to indicate GT “success.” 27 This response could, the authors presume, be related to the availability in Canada of safe and effective protein replacement therapies for hemophilia. However, it also indicates that emerging biotechnology can be viewed with caution.
Value of clear communication
In addition to needing time, parents/caregivers called for thorough communication processes, particularly around safety, which would enable them to make informed decisions. Brooks and Bubela documented a caregiver preference for talking to the lead clinical researcher before making an enrollment decision and receiving complete information about risks, benefits, and uncertainty to help them in the process. 17 While participants had a general understanding of GT, some lacked confidence about the accuracy of information they had acquired. For instance, Khair et al. conducted focus groups of hemophilia patients in which nearly all respondents (60/63) had heard of GT for the disease, and 53/60 said that they would consider it for their child. 25 Yet, the groups revealed a lack of consistency in how families learned about and received information about GT, reporting that, “awareness was high, but tended to be vague and fragmented. All participants felt their attitude toward gene therapy was conflicted.”25(p.123)
Some participants felt that being kept informed gave them hope and would ensure they were prepared for a future when GT was available; for them, such information was seen as valuable and reassuring, particularly in the early days after diagnosis or when struggling with treatment. Still, others reported making a conscious decision not to engage with GT as they felt it was too far in the future and thus not worth considering for their child. 25 Some were reluctant to consider GT, while it was still new, associated with uncertainty, and while current treatments were working well. 27
Even across different preferences for how information was delivered, by whom, and when, there was a consistent desire for information: Participants across one sample wanted communication about trials to be in plain, simple, and nonscientific language, and where possible, to include the child in the decision-making and assent processes. 25
Potential impact on quality of life
Overall, studies showed that parents/caregivers had a strong desire to preserve their child's current level of function and maximize their quality of life, even more than finding a “cure” or increasing potential lifespan. This, in turn, impacted their perceptions of safety and efficacy, as well as risk tolerance. For instance, finding a cure remains important to DMD patients, but it might not be their primary or immediate concern. 27 Peay et al. found that, “by a large margin, the highest utilities [for caregivers of children with DMD] …was a treatment that ‘stops progression of weakness' (0.877) and ‘slows progression of weakness' (0.800). These scores had almost twice the utility of the next-highest score, ‘5-year gain in expected life span.’” 22
While finding a “cure” may certainly be a goal for parents/caregivers, many participants from our sample expressed more specific desired outcomes. In a study of parents of children with AS, Adams et al. found that “almost all parents of children with AS (95%) and the comparison group (89%) agreed that treatments aiming to reduce symptoms associated with their child's syndrome were positive.” 28 Some parents were not interested in trials designed with placebo arms because of wished for benefit in exchange for assumption of risk. Others cited hope for symptom-free interval time as a motivating factor, but also felt that hope can be a double-edged sword. 28
In van Balen et al.'s study (2020), the authors examined factors that influenced hemophilia patients' and their parents' decision making about switching to a new treatment option. 24 They found that ease of use of medication (i.e., fewer injections, easier handling, and alternative administration) had an added value for new treatments. However, participants also expressed concern about short- and long-term safety and believed the effects of GT were not sufficiently well understood, with some expressing a “wait-and-see” attitude for novel treatments writ large. 24
Within the DMD community, patient preferences toward treatment, assessment of risks and benefits, attitudes, and experiences of treatment have been well-documented. One of these studies highlighted preference differences between subgroups at different stages of disease. 18 The study, which examined 27 adults with DMD and 247 caregivers of children with DMD, revealed that caregivers of ambulatory children cared significantly less about the chance for improved lung function when deciding to join a GT trial than either adults with Duchenne (p < 0.001) or caregivers whose child used a wheelchair (p < 0.001). 18
The survey study of parents of children with AS found that significantly more parents of children with AS (95%) compared to the mixed comparison group (56%) felt genetic treatment trials aiming to find a “cure” should be a priority within their child's syndromes, and that they would want to “cure” their child's syndrome if possible. 28 The AS group also had significantly higher confidence in their understanding of ways in which GT aims to treat their child's syndrome. Finally, not all necessarily wished to “cure” their child's syndrome (i.e., they may just wish to reduce the symptoms associated with it). 28
DISCUSSION/IMPLICATIONS
This scoping review aimed to assess the empirical research conducted to date about pediatric perspectives on and lived experiences of pediatric GT clinical trials. Overall, the articles reviewed predominately fell into perspectives on GT, expressing a range of attitudes toward GT that were largely dependent on a child's disease, its progression, and on the availability of alternative treatments. These findings suggest that existing empirical research focuses primarily on decision making about whether to enroll a child in a GT clinical trial rather than the actual experience of the GT trial, which is not so surprising, given the relatively small GT trial sizes to date.
As authors, we had hypothesized that there would be more mention of logistical hurdles and other socioeconomic burdens that we have repeatedly heard about from rare disease parents and patient advocates, but there was surprisingly little mention of these aspects of trial participation. It is reasonable to presume that worry over logistics might be mitigated by factors such as the organizing and funding sources of a rare disease and the number of GTs in the pipeline for a disease, as well as the occurrences and transparency of coverage over recent SAEs.
To be sure, decision making is a critical aspect of the lived experience of interest to the authors; weighing the risks and benefits of GT inevitably impacts the social, emotional, and logistical experience of families. Previous studies have highlighted the need for additional decision-making tools tailored specifically for GT trials. For example, one recent study suggested that decision tools used in the hemophilia GT space ought to include, in addition to safety, efficacy, and cost, “detailed information on the gene therapy process.” 29 Another study of informational needs of patients with SCD and their caregivers pointed to their disease community's relatively limited understanding of GT and called urgently for culturally appropriate, patient-centered education for GTs. 30 Both of these studies further demonstrate the need for and current gaps in information and education about GT.
When considering and addressing these gaps, stakeholders should make sure that any decision-making tool and education about GT are developed and disseminated as equitably as possible to ensure historically underserved populations have equal access to GT information and supports. Even though rare disease communities may learn about, perceive, and consider GT differently depending on relevant disease factors (such as disease progression, alternative treatments, and even phenotypic expression), having a clearer picture of what the lived experience entails will help them to make a better decision for their family. Data gathered from our sample can serve as a “primer” to inform other meaningful aspects of decision making that will inevitably impact patients' and families' lived experience of GT.
Part of the rationale behind gathering this information is that parents and caregivers of children with rare diseases often live in a permanent complex and stressful emotional state due to their child's illness. Previous research shows that this group reports feelings of isolation, frustration, and hopelessness. 31 –34 This may largely be attributed to the time and physical burdens of caregiving, which take away from prioritizing one's own health.
One study from Eurordis (The European Organisation for Rare Diseases) found that 30% of caregivers spend more than 6 h per day—meaning the majority of the active part of their day—helping their child patient. 35 In comparison, figures from the Organisation for Economic Co-operation and Development (OECD) also show that 50% of caregivers (for patients suffering from any type of disease or dependent conditions) provide less than 1.4 h a day. 33 Consequently, rare disease patient caregivers seem to be clearly above the OECD caregiver average.
The above will not surprise most rare disease caregivers who experience this first hand. Yet, it is important for GT trial stakeholders who are designing GT trials to understand the physical, emotional, and mental toll that parents/caregivers expend navigating their child's “diagnostic odyssey,” contemplating treatment options, enacting care plans, and organizing follow-up care. Some have even suggested that health care providers should screen parents for psychosocial impairment and, additionally, should provide interventions that consider holistic, as well as gender-specific differences in psychological health. 36 Kolemen et al. argue for the necessity of psychological support for parents in reducing their long-term stress. 37
Patient advocacy organizations can and do provide support for caregivers—the Courageous Parents Network is one example of a parent- and caregiver-oriented nonprofit that provides caregiver resources, including a multimodal resource called “Evaluating the Clinical Trial Option.” 38 The authors of this article commend thoughtful resources like these, as they aim to meet the goals of family-centered care. However, more work is needed in this area, especially as more GTs gain FDA approval. Specifically, it has come to our attention that more guidance and support are needed for each step of the clinical trial process, such as when a clinical trial is put on hold; this can be potentially devastating or may even feel like receiving a diagnosis all over again, especially if a clinical trial was one of few options. 39
To date, the published literature does not adequately address the lived experience of actually participating in a pediatric GT clinical trial for patients or for their families. Within the existing published research, there has been very little examination of factors that parents/caregivers and children weigh, beyond safety and efficacy, when considering participation in a trial. Furthermore, current studies of rare diseases burdens are often siloed between disciplines, creating obstacles for researchers to collect reliable and sufficient data in this area. 40 It is important to note that pediatric patients' own perspectives are almost entirely absent from the literature, making this an important area for future research efforts.
Additional areas for further research could include the capacity for and experience of travel to trial sites, time off or leave from work, lost earnings, provision, and cost of childcare for other children, disruption or reconfiguring of intrafamilial relationships, and other logistical or social-emotional considerations. These qualitative data are critical to informing future trial designs. For example, if caregivers tend to focus more on quality-of-life outcomes than additional years of life, these priorities should be centered in clinical outcomes measured in GT trials and incorporated into shared decision-making approaches to informed consent/assent for clinical trial participation. 41 Ultimately, further inquiry is needed to better understand the ways in which patients and their families are impacted by GT trials to develop more patient- and family-centered policies, trial designs, and decision-making support tools.
Limitations
Our study has a number of limitations. We only included English-language articles and it is possible that studies published in other language may have yielded different information. Given that some rare disease clinical trials may recruit from an international and potentially non-English cohort of families and patients, this is an important consideration, as related to the necessity for effective education and communication related to trials, risks, and expectations. In addition, heterogeneity in study design and types of data reported across the sample prevented us from conducting a meaningful critical appraisal of study quality.
Operationalizing the concept of “lived experience” presented a further challenge, as the construct is multi-faceted without clear consensus on the dimensions most relevant to our inquiry. This conceptual complexity is reflected in our search string (Appendix A1). Finally, we adhered to best practices for scoping reviews according to the PRISMA ScR Checklist to ensure trustworthiness of our study findings; however, each member of the research team brought their own perspective and experience to the study. To address this potential bias, the team held regular reflexive discussions to acknowledge and examine our own positionality in relation to the topic area.
CONCLUSION
The field of pediatric GT research continues to expand, and additional clinical trials will become available for a variety of conditions over the next decade and beyond. Given this anticipated growth, the field has an important and timely opportunity to better understand how patients and their parents/caregivers choose whether or not to consider GT, and their lived experience of participating in clinical trials. Pediatric patients' own perspectives are almost completely absent from the literature, marking an important area for future research efforts. Such insights from further research will inform more patient- and family-centered clinical trial design and can help to ensure that clinical trial design and implementation reflect patients' and families' values, their priorities, and their goals for care. This scoping review lays a foundation for future research in this space.
Footnotes
ACKNOWLEDGMENTS
We would like to thank all PGTME Lived Experiences Subgroup members for their invaluable contributions to this project. In particular, we would like to thank Alix Hall and Mathew Vo for help with reviewing articles, as well as for developing and testing the final data extraction sheet.
AUTHOR DISCLOSURE
K.B. is employed by and holds stock in Pfizer, Inc. E.J. is employed by and holds stock in Encoded Therapeutics. These materials reflect only the personal views of these authors and may not reflect the views of their employers. Alison Bateman-House and Cara Hunt receive salary support from Parent Project Muscular Dystrophy (PPMD). L.K., R.M., and J.D.-B. declare that they have no conflicts of interest to disclose.
FUNDING INFORMATION
The Lived Experiences subgroup of the Pediatric Gene Therapy and Medical Ethics Working Group (PGTME) at NYU Langone Health works to place the stories and perspectives of patients and their families at the center of discussion about gene therapy research.
Appendix A1. Database Searches
PubMed:
(“genetic therapy”[MeSH Terms] OR “genetic therapy”[All Fields] OR “gene therapy”[All Fields] OR “genetic therapies”[All Fields] OR “gene therapies”[All Fields]) AND (“decision making”[MeSH Terms] OR “decision making”[All Fields] OR “lived experience”[All Fields] OR “lived experiences”[All Fields] OR “patient experience”[All Fields] OR “patient experiences”[All Fields] OR “Patient Preference”[MeSH Terms] OR “Patient Preference”[All Fields] OR “patient satisfaction”[MeSH Terms] OR “patient satisfaction”[All Fields] OR “patient perspective”[All Fields] OR “patient perspectives”[All Fields] OR “qualitative research”[MeSH Terms] OR “qualitative research”[All Fields] OR “perception”[MeSH Terms] OR “perception”[All Fields] OR “perceptions”[All Fields] OR “opinion”[All Fields] OR “opinions”[All Fields] OR “awareness”[All Fields] OR “Attitude to Health”[MeSH Terms]) AND (“child”[MeSH Terms] OR “child, preschool”[MeSH Terms] OR “children”[All Fields] OR “infant”[All Fields] OR “non-adult”[All Fields] OR “parent”[All Fields] OR “parents”[All Fields] OR “parenting”[All Fields] OR “parental”[All Fields] OR “young adult”[All Fields] OR “adolescent”[MeSH Terms] OR “Parental Consent”[All Fields] OR “parenting”[MeSH Terms])
Embase (Ovid):
(decision making.mp. or exp decision making/or (lived experience or lived experiences or patient experience or patient experiences or Patient Preference or Patient Preferences or patient satisfaction or patient perspective or patient perspectives or qualitative research or perception or perception or perceptions or opinion or opinions or awareness or Attitude to Health).mp.) and (gene therapy.mp. or exp gene therapy/or genetic therapy.mp. or gene therapies.mp. or genetic therapies.mp.) and (young adult.mp. or exp young adult/or parenting.mp. or exp child parent relation/or parental consent.mp. or exp parental consent/or parental.mp. or parents.mp. or exp parent/or child.mp. or exp child/or exp preschool child/or exp infant/or infant.mp. or exp adolescent/or adolescent.mp.)
CINAHL (EBSCOhost):
(“genetic therapy” OR “gene therapy” OR “genetic therapies” OR “gene therapies”) AND (“decision making” OR “lived experience” OR “lived experiences” OR “patient experience” OR “patient experiences” OR “Patient Preference” OR “Patient Preference” OR “patient satisfaction” OR “patient perspective” OR “patient perspectives” OR “qualitative research” OR “perception”[All Fields] OR “perceptions” OR “opinion” OR “opinions” OR “awareness” OR “Attitude to Health”) AND (“child” OR “preschool” OR “children” OR “infant” OR “non-adult” OR “parent” OR “parents” OR “parental” OR “young adult” OR “adolescent” OR “Parental Consent” OR “parenting”)