
Abstract
Ex vivo machine perfusion (EVMP) is rapidly growing in utility during solid organ transplantation. This form of organ preservation is transforming how organs are allocated and expanding the definition of what is considered a suitable organ for transplantation in comparison with traditional static cold storage. All major organs (heart, lung, liver, kidney) have been influenced by this advanced method of organ preservation. This technology also serves as an unprecedented platform for effective administration of advanced therapeutics, including gene therapies, during organ transplantation to optimize and recondition organs ex vivo in an isolated manner. Applying gene therapy interventions through EVMP introduces different considerations and challenges that are unique from gene therapies designed for systemic administration. Considerations involving vector (choice, dose, toxicity), perfusate composition, and perfusion circuit components should be evaluated when developing a gene therapy to administer in this setting. This review explores these aspects and discusses clinical applications in transplantation where gene therapy interventions can be developed relevant to heart, lung, liver, and kidney donor grafts.
INTRODUCTION
Gene therapy has remarkably expanded in accessibility, safety, and efficiency over the last three decades allowing for its widespread application in medicine, and offers the promise that diseases can be cured rather than managed lifelong. 1,2 In parallel, there have been similar advancements in the field of organ transplantation with the clinical use of ex vivo machine perfusion (EVMP) for the preservation of donor organs. Application of this technology to transplantation has allowed for organs to be preserved in a near-physiologic state, which has been demonstrated to minimize the amount of injury that an organ sustains and even recondition it while it is in transit from the donor to the recipient. 3
Organ transplantation remains the most effective treatment for patients who develop end-stage organ failure.
4
However, there has been a significant donor shortage affecting the ability to perform transplantation for everyone in need. There are currently 103,615 patients on the waitlist to receive an organ transplant in the United States; however, only 42,889 transplants were performed in 2022. Notwithstanding, 2022 was the year with the most transplants ever performed in the United States, which in part can be attributed to the growing clinical use of EVMP (data accessed on October 31, 2023 from
Ex vivo machine perfusion
Static cold storage (SCS) has been the standard of care for organ preservation to this present day. 4 It consists of flushing the procured organ with preservation solution at 0–4°C, submersing the organ into a bag filled with preservation solution, and then storing the bag and contents on ice until transplantation. While the simplicity and cost-effectiveness of this preservation modality made it the preservation method of choice, this method is associated with ischemia–reperfusion injury (IRI) to the organ and tissue injury secondary to prolonged hypothermia.
As a result, organs are only able to be stored using SCS for a limited period before tissue damage begins to compromise transplantation outcomes. 4 –7 This preservation period becomes even shorter when an organ is procured from a donation after circulatory death (DCD) donor or from an extended criteria donor (ECD) versus a traditional donor from brain death (DBD). Before EVMP was available for clinical use, DBD organs were the only ones that could consistently be safely offered to patients because these organs tend to come from younger patients without chronic disease and fared best after preservation by SCS.
DCD describes the retrieval of organs after death confirmed using circulatory criteria rather than neurological ones where cardiopulmonary interventions are withdrawn for several minutes and the patient is monitored for complete cessation of cardiac activity. 8 Generally, ECDs are donors over the age of 60 or a donor over the age of 50 with vascular comorbidities. 9 Preservation of these marginal grafts by SCS is associated with a higher risk of developing post-transplantation complications. 10 EVMP has also ushered in the era of growing utilization of DCD and ECD organs, which would have otherwise been discarded. 10
EVMP functions by perfusing the donor organ with perfusate that provides oxygen and nutrients to support tissue metabolism while preventing metabolic waste from locally accumulating within the organ. 4,11 EVMP can be performed under different temperature conditions: hypothermic (1–18°C), subnormothermic (32°C), or normothermic (34–38°C). By maintaining the baseline degree of metabolic activity and minimizing the amount of ischemia time, EVMP extends the amount of time an organ can remain ex vivo before transplantation. 4,10 As a result, organs stored on EVMP are able to be offered to recipients residing farther away.
Beyond the direct effect that EVMP has on reconditioning donor organs, it can serve as a method for delivering genes and other types of therapeutics directly to the donor organ (Fig. 1). This gene delivery approach offers the advantages of being able to administer controlled vector dosing directly to the organ with no off-target vector delivery while minimizing side effects and toxicity typically associated with systemic viral vector administration. The clinical significance of this is the potential to be able to directly confer genetic protective or reconditioning traits to protect organs from IRI, and acute and chronic rejection among others (Fig. 2).
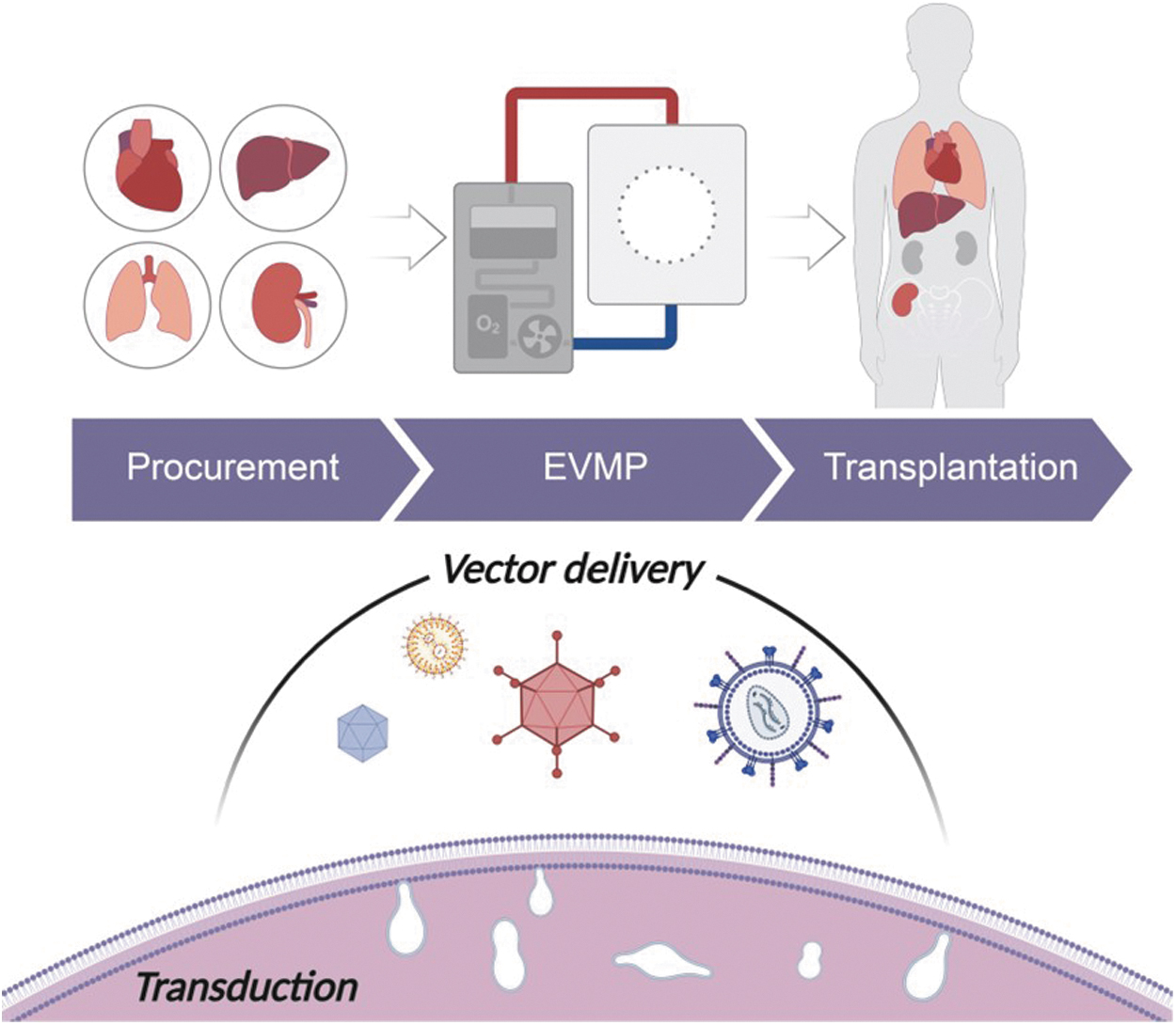
EVMP-mediated gene delivery for organ transplantation. Organs procured for transplantation can be preserved using EVMP while in transit from the donor to the recipient. While the organ undergoes perfusion, vectors, such as viral or nanoparticles, can be added to the perfusate to deliver therapeutic genes to the organ before transplantation. The vectors are endocytosed by cells from the perfusate. After transplantation, the organs will express the conferred transgenes, which can serve to prevent transplantation complications. EVMP, ex vivo machine perfusion.
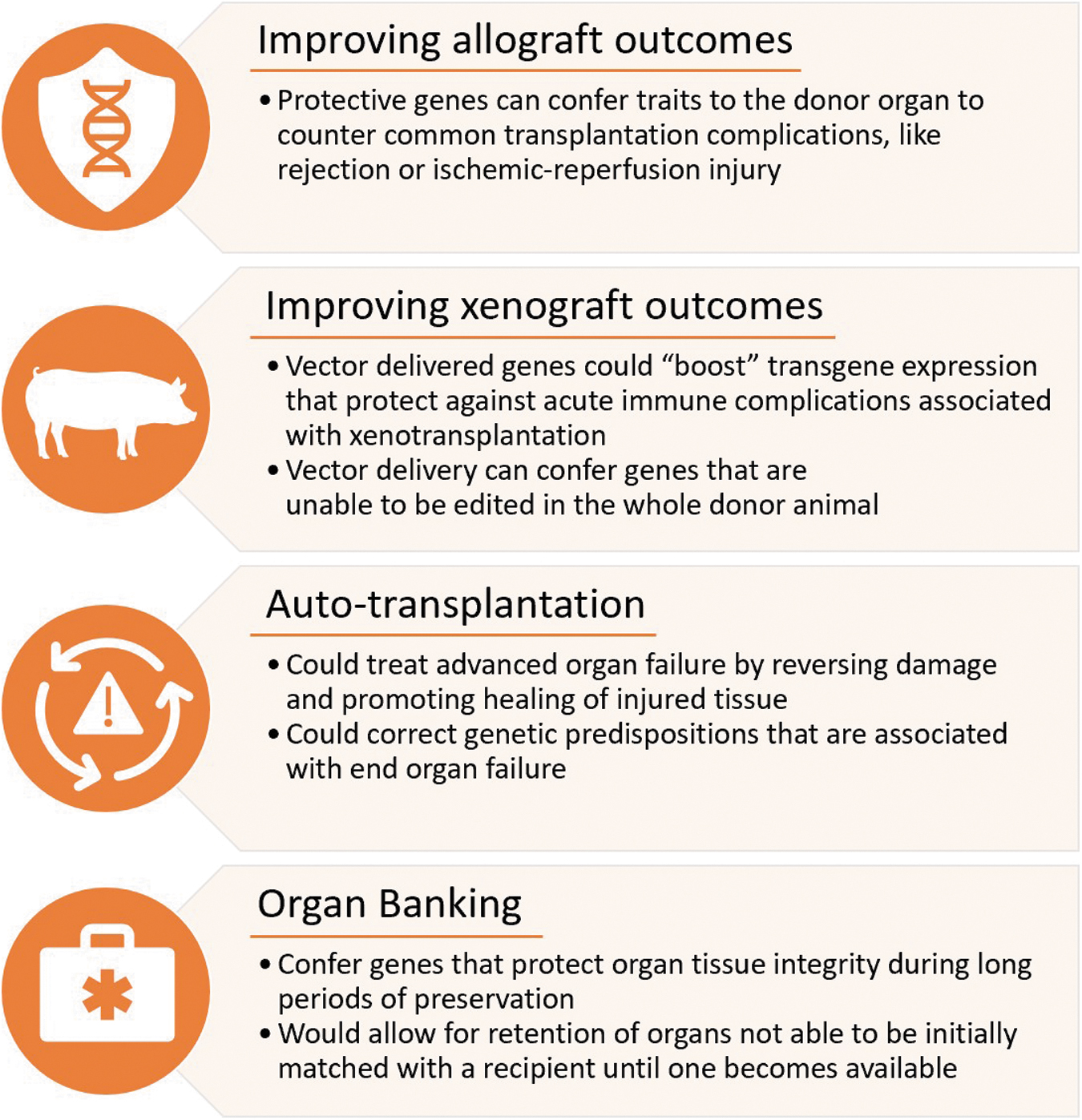
Gene therapy applications for organ transplantation. Organ transplantation is continually evolving to meet the need for more donor organs and to improve the lifetime of each transplant. These include improving allograft outcomes by conferring traits to organs to counter common complications, improving xenograft outcomes by boosting transgene expression that protect against acute immune complications, autotransplantation to treat advanced heart failure by reversing damage and promoting healing of injured tissue, or by engineering organs to be able to be preserved for long periods of time.
GENETIC MODIFICATIONS FOR ORGAN TRANSPLANTATION
Gene addition and silencing in the transplanted organ have been described through EVMP-mediated vector delivery. Gene addition introduces new genes into the cells to confer expression of a protein that would not usually be expressed at baseline by the treated cell. This technique can be used to confer gene expression in a cell that is lacking functional expression of the gene of interest. It can also be used to confer genes to cells that will protect the organ from damage caused by oxidative stress, humoral or cellular immune responses. 11
Alternatively, gene silencing holds great potential as a therapeutic approach in the context of pretreating the donor organ to silence expression by RNA interference using small interfering RNA (siRNA) or short hairpin RNA (shRNA). The targets mostly described are immunogenic genes or cytokines that elicit humoral and cellular immune responses in the context of transplantation. 12
Gene editing is another technique for gene modification that has demonstrated tremendous advances in the field of xenotransplantation, allowing for the first porcine heart transplant into a human. 13 Gene editing has not yet been described in the context of EVMP-mediated vector delivery; however, it holds potential in applications toward reconditioning discarded or poor quality organs to make them suitable for transplantation, as well as toward engineering organs to achieve tolerance after transplantation into the recipient. 14
Gene delivery vectors in EVMP-mediated delivery
To be able to achieve these techniques in genetic modification of donor organs, effective gene delivery is required. It is overall a particular challenge of gene therapy to be able to achieve global and robust gene expression throughout an entire target organ. Use of EVMP allows for direct administration of vectors to the perfusate that will percolate through the vasculature of the donor organ and recirculate several times until vector uptake by the organ is achieved.
Vectors that have demonstrated utility in this setting so far include viral and nonviral vectors. The most effective vehicles are viral vectors that deliver genetic cargo by transducing cells. The different types of viral vectors are each characterized by different potencies, duration of transgene expression, and amounts of transgene expression. The viral vectors that have been most utilized for EVMP-mediated gene delivery are adenoviral (Ad) vectors, adeno-associated viral vectors (AAVs), and lentiviral vectors (LVs).
Ad is ideal for obtaining peak gene expression quickly (within 1–3 days of administration). Gene expression is conferred to both dividing and resting cells. Ad vectors are very potent, being able to achieve high levels of gene expression at lower titers than AAV or LV. Ad vectors, however, are associated with high immunogenicity with gene expression lasting for only several days to weeks. 15
AAV is the least immunogenic of all viral vectors. It is especially appealing because it confers gene expression that can last for years after administration, although it does take several weeks for peak gene expression to occur. Also, AAVs are limited to carrying genetic loads of 4.7 kb. 15 LVs have not been as widely used to date in gene delivery applications in organ transplantation. Their main characteristic is that they are able to transduce dividing and nondividing cells with the genetic cargo they deliver being integrated into the host genome conferring long-term and stable expression.
There has been growing use of nonviral vectors for gene delivery. Nanoparticles can be composed of several different materials, such as lipids, polymers, peptides, and inorganic particles. 16 Their ability to deliver genes is mainly dependent on the particle composition, charge, and size. Secondarily, factors such as uptake and clearance of particles from the target organ also affect the success of gene delivery by nanoparticles. A technique known as active targeting can be implemented where receptor ligands are directly conjugated to the nanoparticles to target a cell type of interest. The main obstacle affecting the widespread utility of nanoparticles is their degradation by endonucleases, direct toxicity to cells, and by their potential to form aggregates in solution. 16
Notwithstanding, these are all promising vectors for utilization with EVMP-mediated delivery, and further investigation is needed to develop their utility in organ transplantation. For instance, the unique characteristics of gene expression conferred by each vector could be strategically implemented to best prevent post-transplantation complications. AAV or LV could be the ideal vectors to utilize for strategies looking to prevent acute rejection (AR), given the long-term gene expression they confer, whereas Ad or LNPs could be better suited for utilization in treatment strategies looking to prevent or mitigate damage caused by ischemia–reperfusion from storage conditions.
Clinical applications for genetic engineering of organs in transplantation
Donor organs are subject to substantial stress beginning at the time of procurement and extending well after transplantation into the recipient. The success of a transplant is ultimately dependent on the ability of the donor organ to withstand the harmful effects of these stressors. Donor organs, before and after placement on EVMP, are exposed to proinflammatory cytokines and injury caused by the presence of reactive oxygen species (ROS) formed from ischemia followed by reperfusion of the organ. The latter events portend to the development of IRI (see the Ex Vivo Machine Perfusion section). The incidence and extent of IRI are associated with the development of primary graft dysfunction (PGD) and AR. 5,17
PGD can manifest within the first 72 h after transplantation where the transplanted organ is unable to function. Depending on the severity of PGD, this condition can quickly lead to multiorgan dysfunction and even death. The exact pathophysiology of PGD from organ to organ is unknown; however, the presence of proinflammatory cytokines and damage-associated molecular patterns released from IRI and activation of endothelial cells leading to a coagulopathic state have been associated with its development. 18 –20
AR manifests within the first weeks to the first year after transplantation. Like PGD, AR is associated with a higher risk of morbidity and mortality for the patient. AR is primarily manifested by mismatched major histocompatibility complex (MHC) molecules resulting from specific recognition of these antigens by T cells. 21,22
The T cells can become activated by either having direct interaction through the T cell receptor with intact allogeneic MHC–peptide complexes presented by donor-derived antigen presenting cells (APCs) or by interacting with previously degraded donor MHC peptides presented by recipient APCs. Once a T cell is activated by antigen recognition, an immunologic synapse forms, which results in clustering of costimulatory, signaling, and adhesion proteins to form a supramolecular activation complex and thereby T cell activation. 11 The activated T cells go on to attack the foreign cells of the donor graft, eventually leading to fulminant organ failure if left unchecked.
CONSIDERATIONS FOR EVMP-MEDIATED VECTOR ADMINISTRATION
Effective gene delivery to target sites has been the biggest challenge for in vivo gene therapies to become successful therapeutics. 1 This is affected by two main components: (1) the ability of the vector to bind and enter the target cell; (2) the delivery of the vector to the target organ.
The ability of the vector to bind and enter specific cells is specific to the characteristics of the vector being used. Specifically, with viral vectors, this would be attributable to the capsid design at the molecular level conferring tropism for the target organ. At the macrolevel, delivery of the vector to the target is dependent upon route of administration. Most gene therapies are developed for either systemic intravenous (IV) delivery or by direct local injection into the desired target.
Systemic IV vector delivery is influenced by off-target gene delivery to other organs, given that viral vectors are generally able to interact with multiple types of receptors that are present on more than one organ. The main limitation of direct local injection to the target site is the ability of the vector to distribute throughout the region of interest as this route of administration does not allow for widespread distribution throughout the organ, hence making this route of vector delivery ideal for smaller or focal targets. 23 Both systemic and local routes of administration are challenged by capsid induced activation of recipient immune responses and by any circulating neutralizing antibodies. 24
The effects of these not only decrease the efficiency of gene delivery by the vectors, but also can elicit a severe inflammatory response that can be life threatening for the recipient. EVMP is emerging as a promising new method for administering vectors to organs during perfusion. It excels in comparison with administration by systemic and direct local injection in that the full vector dose is being administered to the organ while it is isolated from all other organs. The risk of off-target delivery is reduced and has yet to be observed in studies. 25,26 This method of vector administration also offers the advantage of circumventing the presence of neutralizing antibodies circulating in the recipient's blood and minimizing the stimulation of immune responses.
EVMP: normothermic versus hypothermic
EVMP systems have been developed to primarily function through hypothermic or normothermic temperature settings (Table 1). Both preservation strategies consist of similar perfusion circuit components. The circuit is equipped with a blood pressure gauge, flow meter, and oxygen saturation probe to be able to adjust and optimize the perfusion settings on the device. Analogous to how the organ receives blood flow in vivo, the perfusion devices deliver perfusate to the organ through an inflow cannula and perfusate flows out of the organ through an outflow cannula.
Ex vivo machine perfusion characteristics: normothermic versus hypothermic storage
OCS, Organ Care System; RBC, red blood cell.
In the case of the lung, mechanical ventilation is also provided to the organ. The perfusate from the outflow cannula then collects in a reservoir, which then flows through a gas exchanger where oxygenation occurs. The perfusate is then returned back to the organ through the inflow cannula. Currently, the devices predominantly being utilized clinically include the TransMedics Organ Care System (OCS) (heart—normothermic, liver—normothermic, lung—normothermic); the XVIVO XPS (lung—normothermic) and XPHS (heart—hypothermic), the OrganOx Metra (liver—normothermic), and the Organ Recovery Systems LifePort (kidney—hypothermic). Under normothermic machine perfusion (NMP) settings, the organ continues to function in a near-physiologic state as the temperature and nutrient supplementation mimic in vivo conditions.
NMP enables recovery of adenosine triphosphate production during preservation and induces protective stress responses while downregulating cell death and enhancing cellular proliferation. 27,28 Under NMP conditions, gene delivery is able to proceed similarly to how it would in vivo. As a result, robust gene expression has been reported in donor organs soon after organ transplantation. 25
Hypothermic machine perfusion (HMP) cools the organ to the point where organ metabolism is reduced to ∼10% of its metabolism at baseline. 29 As a result, the physiologic function of the organ is nearly ceased during the perfusion period, and cellular injury due to ischemia and hypoxia is attenuated. The advantage of HMP over SCS lies in HMP continually flushing debris, toxic metabolites, and free radicals produced by cells while providing supplementation of metabolic substances to sustain maintenance cellular metabolic functions to further prevent cellular injury. 29 –32 Because metabolic functions of the cells are significantly slowed, so is the ability of viral vectors to be efficiently taken up by cells for gene delivery.
In vitro studies have demonstrated that viral vectors, such as Ad and AAV, can still attach to their cell surface receptors, but that it is to a much lower degree compared with normothermic conditions. 33,34 Given more time, more vectors may attach to their receptors. However, cellular entry is inefficient until cellular conditions are returned to normothermic range. 33,34
Perfusate considerations
Viral vectors interact with components of the medium in which they reside, whether it be blood, the interstitial space between cells, or perfusate circulating through an EVMP device. These components can affect their efficiency to transduce cells and achieve transgene expression. For this reason, careful selection of perfusates for EVMP where gene therapy is planned to be administered is imperative. However, the current understanding of what additives enhance or diminish viral vector transduction during EVMP-mediated vector delivery is lacking and warrants further investigation.
The knowledge base for this phenomenon comes from in vitro studies where the addition of additives, ranging from inorganic molecules, small molecules, to lipids, can enhance transduction and yield higher transgene expression. 26,35 –39 A few of these studies were also able to demonstrate that the enhancement noted in vitro is associated with enhanced in vivo transgene expression. 35,36,38,39
Currently, the perfusates that are mostly utilized for EVMP were developed by the companies of the devices for which they are used. These perfusates were primarily designed to protect cells from ischemia and injury during long periods of preservation, and supplement nutrients that support cellular metabolic functions. Not much is known about how these perfusates and the additives that comprise the final formulation affect viral vector transduction efficiency and transgene expression after organ transplantation.
Two studies examined the different perfusate components of the TransMedics OCS using in vitro assays to assess whether gene delivery is affected. Bishawi et al. observed that blood components overall diminish Ad viral vector transduction; however, the remainder of the OCS perfusate with additives appeared to rescue the ability of the Ad to transduce cells and achieve robust transgene expression. 25 Mendiola Pla et al. subsequently assessed the individual components of the OCS perfusate across various cell lines using a panel of recombinant AAVs, and observed that methylprednisolone and calcium gluconate appeared to enhance transduction efficiency to varying degrees depending on the cell type. 26
While both of these findings are limited in that they were only observed in in vitro assays, both studies demonstrated that viral vector delivery by EVMP-mediated delivery achieved global and robust transgene expression in the transduced donor hearts.
The major perfusates being utilized for EVMP are blood based to effectively deliver oxygen to cells during preservation. As described above, different components of blood can adversely affect transduction efficacy. These include interactions with erythrocytes, monocytes, circulating proteins, and neutralizing antibodies. 40 –42 These could potentially negatively affect transduction efficacy during EVMP-mediated gene delivery. To address this potential adverse factor when delivering viral vectors using the TransMedics OCS, both Bishawi et al. and Mendiola Pla et al. implemented a blood washing step using a cell saver device to remove serum components. 25,26
Both studies reported robust, global transgene expression in the transduced hearts; however, neither study reported on transgene expression in hearts without addition of the blood washing step so it remains unclear whether this step substantially improves transduction efficiency. Regardless of its effectiveness, blood washing introduces a degree of complexity to the use of EVMP for organ preservation. This process takes 20–40 min to complete and affects the oncotic pressure of the blood collected from the donor by removing the majority of proteins from it. To counter this and prevent unwanted cellular edema in the organ, albumin had to be added to the perfusate to restore the desired oncotic pressure of the perfusate.
Dosing and toxicity considerations
There is growing experience with dosing strategies for IV and intramuscular injected gene therapies in terms of efficacy and safety. The same experience does not currently exist for EVMP-mediated gene delivery to organs. When gene therapies are dosed systemically, aspects such as vector clearance from the circulation, presence of circulating blood components, and off-target uptake of vector affect how much of the administered vector is able to reach the intended target to achieve the desired therapeutic effect. 43 Analogous considerations for dosing using EVMP-mediated vector delivery exist.
EVMP is advantageous for vector administration to whole organs since the target organ is completely isolated from other organs. Because of this isolation, EVMP-mediated vector delivery allows for the administered dose to be concentrated to the target organ, minimizing the amount of vector that needs to be given to achieve therapeutic transgene expression in the transduced organ. In addition, the potential for eliciting a severe immune response in the recipient is decreased, given that direct exposure of the viral vector to the recipient's immune system is largely avoided by this method of vector delivery.
In the context of organ transplantation, immune responses to the vector are further avoided since the organ recipients have already been administered immunosuppression medications in anticipation of organ transplantation. Use of immunosuppression medications in the immediate post-transplantation period could also prevent the induction of neutralizing antibody production, potentially allowing for viral vector redosing in the future. 43,44
Another form of toxicity that is associated with viral vector administration is the activation of cytotoxic T cells against transduced cells. This has been described with induction of hepatotoxicity in recipients of systemic viral vector administration. However, the effect appears to be threshold dependent, such that lower doses of vector administration will not elicit this cytotoxic T cell response. 45 As described above, EVMP-mediated gene delivery has the potential to administer lower doses of viral vector to organs, isolated from the recipient immune response, thus circumventing activation of a T cell-mediated immune response.
In the ex vivo setting, consideration toward how much viral vector can be safely administered is important. Gene therapies are typically dosed based on weight of the recipient, and as described earlier there are many factors that effectively lower the actual amount of vector that is able to reach the cells of the target organ. A safe dosing range is yet to be described for vector administration through ex vivo perfusion where the bulk of the vector that is administered will reach the organ directly.
It is unknown what effect exposure to a high dose of viral vector would have on the target cells, which could potentially be toxic due to high viral vector uptake into the cell. It is also unknown what effect high transgene expression from the organ would have on the normal function of the organ. Important consideration of these factors is also concerning in the context of the potential immune response that may be elicited within the organ recipient. This response could be in the context of stimulation of the immune response against components of the viral vector capsid or against the expression of high levels of the conferred transgene. Ultimately, these considerations may result being transgene dependent.
LITERATURE REVIEW OF EX VIVO GENE THERAPY IN ORGAN TRANSPLANTATION
Numerous studies have been described about ex vivo gene therapy applied to organ transplantation during EVMP (Table 2). The interventions described focus on preventing IRI or AR through modification of cytokines or antioxidant enzymes through genetic overexpression or gene silencing. Targets for mitigating tissue damage from IRI function by minimizing the hyperproduction of ROS or by minimizing the inflammatory responses they induce. Genes involved in the native antioxidant response to IRI are the transcription factors hypoxia-inducible factor, nuclear factor kappa-light-chain-enhancer of activated B cells, and nuclear factor erythroid 2-related factor 2. 46
Studies investigating ex vivo machine perfusion-mediated delivery of gene therapy
AAV, adeno-associated viral vector; Ad, adenoviral; ASO, antisense oligomer; BSA, bovine serum albumin; CTLA4Ig, cytotoxic T lymphocyte antigen 4 Ig; eNOS, endothelial nitric oxide synthase; EVMP, ex vivo machine perfusion; GFP, green fluorescent protein; HEPES, 4-(2-hydroxyethyl)-1-piperazineethanesulfonic acid; HMP, hypothermic machine perfusion; IHC, immunohistochemistry; IL, interleukin; IRI, ischemia–reperfusion injury; LV, lentiviral vector; LVDP, left ventricular developed pressure; MIP, macrophage inflammatory protein; MMP-2, matrix metalloproteinase-2; NMP, normothermic machine perfusion; PCR, polymerase chain reaction; pfu, plaque-forming units; pRBC, packed red blood cells; RT-PCR, real-time PCR; siRNA, small interfering RNA; SLA, swine leukocyte antigen; SOD, superoxide dismutase; TGF-β1, transforming growth factor-β1; UW, University of Wisconsin; VGC, viral genome copies; VP, viral particles; WME, William's medium E.
Other potential approaches could involve the genetic silencing of key oxidases involved in the propagation of ROS such as xanthine oxidase, nicotinamide adenine dinucleotide phosphate oxidase, and monoamine oxidase; or conversely through the overexpression of antioxidant enzymes such as superoxide dismutase (SOD), glutathione-S-transferases, thioredoxins, and peroxidoxins. 46,47 An indirect approach for mitigating IRI is through the overexpression of anti-inflammatory cytokines, such as interleukin (IL)-10 and transforming growth factor-β (TGF-β). 48,49
In AR, therapeutic mechanisms focus on prevention of effector T cell activation by preventing T cell receptor binding with MHC or inhibiting the activation of T cells. Silencing of the MHC expression on donor organs has been investigated through overexpression of β2-microglobulin and class II-transactivator. 50,51 Another method of achieving the same effect could be through stimulation of inhibitory checkpoint molecules on T cells, such as cytotoxic T lymphocyte antigen 4 (CTLA4) or PD-1. 52,53
Additional immune regulatory molecules of interest that inhibit T cell effector function include TIM-3, TIGIT, and VISTA. 54 These additional targets have been explored in the context of cancer immunotherapy but could potentially be exploited to induce graft tolerance in organ transplantation. The studies presented here employed EVMP to administer the therapeutic interventions by direct addition to the perfusate while the organ was undergoing perfusion before transplantation. Ad vectors are the most used in the literature to date; however, more recent studies have used AAV and LV vectors for gene delivery.
Heart
One of the earliest examples of ex vivo gene transfer to an organ was described by Brauner et al. 49 In this study, IL-10 and TGF-β1 were delivered to donor rabbit hearts using Ad vector through HMP to prevent incidence of AR. Donor hearts were perfused with the Ad vector for 20-min before transplanting the treated hearts in the cervical heterotopic position. Some treated hearts were explanted 4-days later for analysis of gene transfer and distribution.
An average vector absorption ratio of 81% was reported; however, transgene expression was unevenly distributed throughout the myocardium with most of the gene expression observed in the subepicardial layer and less gene expression noted in the subendocardial layers. For analysis of allogenicity, hearts were explanted when the cardiac allografts no longer had palpable contractile activity. A very small increase in survival (∼4-days) was seen in the hearts that were treated with IL-10 or TGF-β1 with the intervention.
Another early study described by Yang et al. investigated Ad-mediated CTLA4Ig gene delivery during HMP to rat hearts to induce allograft tolerance. 55 Viral vectors were administered by slow infusion over 10–15 min during the 1-h cold preservation of the heart. The hearts then underwent perfusion with cold 0.9% normal saline for 10-min before transplantation. To study the pattern of distribution within the myocardium, the first experiments they performed delivered β-galactosidase as a reporter gene.
There was predominant subepicardial expression with progressively diminishing expression in the subendocardial layers of the myocardium. The next experiments delivered CTLA4Ig to induce allograft tolerance. The intervention conferred indefinite allograft survival versus the control allografts that all rejected between 9 and 12 days after transplantation. On histology, all of the treated hearts demonstrated well-preserved myocardial architecture with no lymphocytic infiltration and no evidence of AR.
Abunasra et al. investigated the protective effect of Ad-mediated multigene transfer with SOD and endothelial nitric oxide synthase (eNOS) to prevent damage from IRI. 47 HMP was used to perfuse the hearts for 15-min during which these therapeutics were administered. After abdominal heterotopic transplantation, the hearts were explanted 4-days later and subjected to 6-h of ischemia followed by 1-h of reperfusion. There were noted improvements in left ventricular developed pressure in the groups that received either SOD or eNOS, as well as in the group that received both genes. The overall conclusion of this study was that delivery of these genes can attenuate IRI; however there is no additive therapeutic effect when they are delivered together.
One group has described gene delivery to hearts during NMP using the TransMedics OCS. Using this device, a luciferase reporter gene using either Ad or AAV was administered to the perfusate after the hearts had been reanimated on the device. The hearts underwent perfusion for 2-h before abdominal heterotopic transplantation. In the first study, Ad-mediated gene delivery was performed, and the hearts were explanted 5-days after transplantation. There was homogeneous distribution of luciferase expression observed throughout the hearts with high levels of expression. 25
In the second study, an AAV vector was utilized at increasing doses to assess for a dose-dependent pattern of distribution. The hearts were explanted 30–35 days after transplantation. Again, homogeneous distribution of luciferase expression was observed, and the level of expression was greater with increasing doses. 26 These experiments collectively demonstrated that homogeneous and robust transgene expression can be achieved after administration of viral vectors using a clinically utilized EVMP device.
Lung
In the lung, delivery of IL-10 has been extensively investigated in the prevention of lung inflammation during NMP. This strategy decreases donor lung damage caused by the release of proinflammatory cytokines. Overexpression of IL-10 promotes anti-inflammatory changes by decreasing expression of proinflammatory cytokines. Decreasing the damage caused by inflammation reduces the incidence of complications such as IRI and AR.
One group based out of Toronto has described use of the XVIVO XPS to deliver Ad-mediated IL-10 transgene during NMP to both porcine and human donor lungs using Ad. 48,56,57 The lungs treated with gene therapy had significantly improved lung oxygenation and reduced pulmonary vascular resistance during EVLP. They also observed decreases in IL-1β and IL-8 expression in lung tissues with concurrent restoration of tight junctions on histology indicating the reduced effect of inflammatory injury. 48
One study utilized RNAi to silence MHC expression in porcine lungs to reduce the risk of allograft rejection. shRNA delivered by LV were utilized, which targeted β2-microglobulin and class II-transactivator. The intervention during NMP on the TransMedics OCS demonstrated that all regions of the lungs successfully received the therapy, achieving a targeted silencing effect for swine leukocyte antigen (SLA) SLA I and II of 67% and 52%, respectively. It also demonstrated that delivery by LV vectors does not induce unintentional tissue injury. 51
Gao et al. investigated AAV-mediated gene delivery during NMP of rat lungs, and delineated the distribution and efficacy of gene delivery through intrabronchial or intra-arterial (pulmonary artery) administration. The lungs were perfused for 1-h with an AAV carrying either luciferase or green fluorescent protein (GFP) transgene. The lungs were then transplanted into a recipient rat and followed for 2-weeks. Intrabronchial AAV administration resulted in the highest level of transgene expression compared with the pulmonary artery delivery group. Transgene expression was noted to be highly variable in the pulmonary artery group, suggesting inconsistent and inefficient gene delivery. There was negligible off-target expression observed in the recipient animal's native tissues. 58
Liver and kidney
One group has been investigating the use of RNAi to silence the FAS signaling pathway to reduce tissue damage caused by IRI. The FAS receptor signals hepatocytes apoptosis, and when FAS receptor expression is reduced this potentially reduces the damage associated with IRI. The first experiments used LNP-mediated delivery of siRNA targeting FAS receptor expression on rat hepatocytes. Uptake of the siRNA by rat livers was compared when delivered under hypothermic versus normothermic conditions after 4-h of EVMP. There was reported diffuse uptake in the sinusoids and the surrounding central veins that was greater after HMP compared with NMP. 59
The follow-up study looked for a potential therapeutic effect from directly silencing FAS expression in rat livers initially preserved in SCS for 4-h before undergoing hypothermic EVMP for 1-h. 60 While there were increased IL-4 and IL-10 levels, differences in apoptotic or tissue necrosis levels on histology were not observed. There were also no differences in FAS transcript levels between the treated and control groups. The group concluded that better siRNA compounds and appropriate doses would be needed to prove siRNA therapy effectiveness.
The same group demonstrated the feasibility of AAV-mediated gene delivery during HMP to rat liver allografts using GFP as a reporter gene; the liver grafts were perfused for 2-h, and AAV was added to the perfusate at the beginning of the perfusion period. Afterward the livers were transplanted into a recipient. The livers were explanted 24-h later, and GFP was observed in the transduced livers. 61
Also utilizing an RNAi strategy, Moser et al. studied siRNA targeting matrix metalloproteinase-2 (MMP-2) during HMP in rat livers. MMPs play an important role in ischemic injury to the heart, and they hypothesized that inhibition of MMPs would prevent tissue damage from IRI. The livers were perfused for 22-h with the siRNA added directly to the perfusate. After the intervention, they analyzed the perfusate and kidney tissue for IRI. Observed were decreased levels of MMP-2, decreased injury markers lactate dehydrogenase and cytochrome-c, and decreased damage to outer mitochondrial membranes as seen by electron microscopy. 62
Another therapeutic RNAi strategy to prevent IRI was tested in porcine kidneys through the administration of miRNA-182-5p to perfusate to suppress damage caused by IRI. The kidneys were perfused for 6 h under NMP conditions, and the therapy was added 30-min after perfusion started. There was reported upregulation of Dpt, Fam129a, Kcnj10, Ppp11r1a, and TEK, which are targets normally suppressed by miRNA-182-5p. There were overall diminished levels of miRNA-182 expression, demonstrating its successful downregulation. 63
Yuzefovych et al. performed a study aiming to reduce the allogenicity of kidney allografts using subnormothermic EVMP. LV-mediated delivery of shRNA was used targeting rat β2-microglobulin and rat class II transactivator, which leads to silencing of rat MHC I and MHC II genes. Six-weeks post-transplantation, they observed increased levels of IL-10, macrophage inflammatory protein (MIP)-1a, MIP-2, epidermal growth factor, with concurrent decrease in IL-12, IL-17, monocyte chemoattractant protein, and interferon-γ, indicating a cytokine profile more consistent with tolerance relative to controls. 50
Gymnotic delivery, which entails the direct addition of naked RNA antagomir antisense oligonucleotide to the perfusate, was described by Thompson et al. to protect kidney grafts from IRI. 64 They used normothermic EVMP to deliver the therapy to human kidneys deemed unsuitable for transplantation. They underwent perfusion for 6-h with miRNA-24-3p antagomir. After perfusion, biopsies of the kidneys were collected for analysis. The investigators observed uptake into both endothelial and epithelial cells.
In comparison, they noted that antagomir delivered during HMP predominantly resulted in expression on the vascular endothelium but did not result in intracellular uptake. This suggested that uptake is an active process that is enabled by normothermic conditions. They noted significant increases in heme oxygenase-1 and sphingosine-1-phosphate receptor-1, which are two targets that are normally inhibited by miRNA-24-3p and are proteins believed to be protective against IRI.
FUTURE CONSIDERATIONS FOR EX VIVO GENE THERAPY IN ORGAN TRANSPLANTATION
Gene therapy for organ transplantation is currently at its earliest stages of development with increasingly more interest after the increasing use of EVMP during transplantation. Safe implementation of these therapies will require foresight for how the organs will be monitored after transplantation. For example, it is unknown what immune responses could be elicited after EVMP-mediated vector delivery. Stimulation of immunologic responses in the recipient should theoretically be minimal in comparison with systemically administered gene therapies since vector and gene delivery are isolated from the transduced organ.
Guidelines for postoperative monitoring and treatment strategies for adverse immunologic responses will be required for widespread clinical adoption of gene therapy administered during EVMP.
In the same vein, strategies to closely monitor transgene expression in the transplanted organs will need to be defined. In some therapeutic applications, such as inducing tolerance to prevent rejection, it will be important to monitor sustained expression of the therapeutic gene. For example, transplanted organs are currently monitored for rejection through regularly scheduled tissue biopsies that undergo assessment for lymphocytic infiltration consistent with rejection. Transgene expression in a transplanted organ could potentially be monitored in a similar way where tissue biopsies are assessed for transgene expression.
Another growing modality that has been gaining traction clinically for allograft monitoring is the assessment of cell-free DNA (cfDNA) isolated from the recipient's plasma. This technology could potentially be useful as well for monitoring transgene expression from the allograft based on the characteristics of the expressed protein or even by detection of transgene DNA from isolated cfDNA.
As experience grows with clinical monitoring of transduced organs, one possibility that may arise in the case of diminishing transgene expression is of repeated dosing of the therapy to the recipient to sustain therapeutic levels of transgene expression. It will also be critical to develop strategies to assess for off-target transgene expression within the native organs of the recipient to minimize unwanted effects and/or damage to them.
Clinical experience with xenotransplantation has recently grown with achievements in porcine-to-human cardiac and kidney transplantation surgeries that allowed for survival of xenografts post-transplantation for prolonged periods of time without evidence of hyperacute rejection. 13,65 These recent achievements were made possible due to extensively gene-edited pigs to minimize the antigenicity of their organs and “humanize” their organs. 65,66 Xenograft rejection is primarily the result of preformed antibodies against porcine antigens on endothelial cells leading to cell death and intravascular thrombosis. 67 Modifications required for these clinical interventions involved removing specific carbohydrate antigens and decreasing the propensity toward complement activation, which together led to systemic inflammation and coagulopathy.
While there has been tremendous success in extending the survival of the xenograft in the first 2 months after xenotransplantation, there is room for consideration of ex vivo gene therapy interventions administered during EVMP to bolster the expression of target genes before transplantation. EVMP-mediated delivery of genes could also potentially confer modifications to xenografts that are not readily tolerated in an entire animal and could be utilized as an adjunct to further modify gene-edited xenograft organs.
Ultimately, as clinical experience grows with gene therapy interventions to recondition organs for transplantation, applications using EVMP-mediated gene delivery could be extended toward pre-emptively treating organs of those with devastating genetic diseases to avoid development of end-organ failure in these patients. The possibilities are vast at this stage, and responsible development of this technology could lead toward unprecedented advances in how we approach treatment of diseases.
Footnotes
ACKNOWLEDGMENTS
We thank Lauren Halligan, CMI, for assisting with the creation of the illustrations included in this article.
AUTHORs' CONTRIBUTIONS
M.M.P. and D.E.B. conceptualized and contributed equally to the preparation and writing of this article.
AUTHOR DISCLOSURE
No competing financial interests exist.
FUNDING INFORMATION
Michelle Mendiola Pla was supported by NIH T32HL007101.