
Abstract
Choroideremia, an incurable, progressive retinal degeneration primarily affecting young men, leads to sight loss. GEMINI was a multicenter, open-label, prospective, two-period, interventional Phase II study assessing the safety of bilateral sequential administration of timrepigene emparvovec, a gene therapy, in adult males with genetically confirmed choroideremia (NCT03507686, ClinicalTrials.gov). Timrepigene emparvovec is an adeno-associated virus serotype 2 vector encoding the cDNA of Rab escort protein 1, augmented by a downstream woodchuck hepatitis virus post-transcriptional regulatory element. Up to 0.1 mL of timrepigene emparvovec, containing 1 × 1011 vector genomes, was administered by subretinal injection following vitrectomy and retinal detachment. The second eye was treated after an intrasurgery window of <6, 6–12, or >12 months. Each eye was followed at up to nine visits over 12 months. Overall, 66 participants received timrepigene emparvovec, and 53 completed the study. Visual acuity (VA) was generally maintained in both eyes, independent of intrasurgery window duration, even after bilateral retinal detachment and subretinal injection. Bilateral treatment was well tolerated, with predominantly mild or moderate treatment-emergent adverse events (TEAEs) and a low rate of serious surgical complications (7.6%). Retinal inflammation TEAEs were reported in 45.5% of participants, with similar rates in both eyes; post hoc analyses found that these were not associated with clinically significant vision loss at month 12 versus baseline. Two participants (3.0%) reported serious noninfective retinitis. Prior timrepigene emparvovec exposure did not increase the risk of serious TEAEs or serious ocular TEAEs upon injection of the second eye; furthermore, no systemic immune reaction or inoculation effect was observed. Presence of antivector neutralizing antibodies at baseline was potentially associated with a higher percentage of TEAEs related to ocular inflammation or reduced VA after injection of the first eye. The GEMINI study results may inform decisions regarding bilateral sequential administration of other gene therapies for retinal diseases.
INTRODUCTION
The eye is a target organ with several advantages for gene therapy. It is small, easily accessible, and compartmentalized with a physical blood–retina barrier. It is also relatively immune privileged (its immunological response to antigens is attenuated), and successful transduction requires relatively few vector/gene copies. The untreated fellow eye acts as a control. 1 –4 Gene replacement therefore offers a potential treatment strategy for inherited retinal degenerations, particularly for rare, recessive diseases in which the required transgene is small, such as choroideremia. 5,6
Choroideremia is caused by mutations in CHM, which encodes Rab escort protein 1 (REP1), a protein involved in retinal pigment epithelium (RPE) maintenance. 7 –9 The RPE separates the retina from the choroid, which provides oxygen and nutrients to the outer retinal layer. 10,11 In choroideremia, peripheral RPE degeneration and rod photoreceptor cell death cause childhood night blindness. 5,7,8 Progressive bilateral centripetal degeneration of the RPE, retina, and choroid typically results in legal blindness by the patient’s fourth decade, 6 –8,12,13 impairing quality of life. 14 –16
As an X-linked disease, choroideremia almost exclusively affects the male population; its prevalence is approximately 1:50,000. 7,17 –20 Female patients often have mild pigmentary changes and well-preserved visual acuity (VA), although X-chromosome inactivation may cause variable phenotypes. 6,7,17 In males, VA decline accelerates after around 40 years of age but remains slow compared with the typical interventional study duration of 1–2 years. 15,21 NIGHT, a noninterventional natural history study, demonstrated stable best-corrected visual acuity (BCVA) over 20 months in males with choroideremia and an average age of 47.1 years. 22
Choroideremia is currently untreatable. Several gene therapies are being investigated to address the significant unmet need for therapies to slow disease progression, 4,7,14 mostly using the adeno-associated virus serotype 2 (AAV2) vector. 4 A Phase III study evaluating the efficacy and safety of bilateral sequential subretinal injection of voretigene neparvovec, with the second eye injected 6–18 days after the first, demonstrated improved functional vision in participants with RPE65-mediated inherited retinal dystrophy; this AAV2-based treatment was the first ocular gene therapy approved by the Food and Drug Administration. 4,23
Timrepigene emparvovec (BIIB111/AAV2-REP1), described previously, 24 also uses the AAV2 vector. Its Phase I/II studies demonstrated improved or stable BCVA over 24 months in most participants with moderate vision loss at baseline (≥34 to <78 letters), compared with the untreated eye. 16,25 –29 However, the Phase III STAR study (NCT03496012, ClinicalTrials.gov), which evaluated efficacy and safety of unilateral timrepigene emparvovec administration, did not meet its primary end point (≥15-letter BCVA improvement at month 12 versus untreated control). 30
GEMINI was an open-label, Phase II study assessing the safety of bilateral sequential administration of timrepigene emparvovec (NCT03507686) focusing on inflammatory responses, conducted to satisfy the regulatory recommendation to clinically assess ocular gene therapies for bilateral treatment in both eyes. 31,32
METHODS
Study design
GEMINI was a multicenter, open-label, prospective, two-period, bilateral, interventional safety study conducted between November 29, 2017 and June 29, 2022. Surgical timrepigene emparvovec administration in each eye was separated by an observational intrasurgery window of variable duration (Fig. 1). Each eye was followed for ≤9 visits per treatment period (day 0/injection day, days 1, 3, 7, and 14, and months 1, 3, 6, and 12). After the second surgery (period 2, day 0), participants followed the period 2 visit schedule; period 2 ophthalmic assessments were performed on both eyes. With each participant’s collaboration, the investigator generally assigned the eye with lower baseline BCVA to be study eye 1.

Study design. Partially shaded bars indicate remapped data for period 1. Most participants began period 2 before completing period 1, so BCVA end points for study eye 1 (lower baseline BCVA) in period 2 were converted (remapped) to their equivalent period 1 time points to allow longitudinal analysis across the whole study. BCVA, best-corrected visual acuity.
The intrasurgery windows (short: <6 months, medium: 6–12 months, or long: >12 months) were not randomized; instead, anticipated windows were determined at screening by a Patient Eligibility Review Committee, aiming to reflect expected real-world timrepigene emparvovec use. GEMINI participants could enter a long-term follow-up study (SOLSTICE, NCT03584165). 33
Eligible participants were male, aged ≥18 years, with a genetically confirmed choroideremia diagnosis, active disease clinically visible within the macular region of both eyes, and a BCVA of ≥34 Early Treatment of Diabetic Retinopathy Study letters in both eyes, or in the untreated eye if the other had previously received timrepigene emparvovec (in which case, their untreated eye could be treated in GEMINI). Whereas the STAR study required a baseline BCVA of 34–73 letters, GEMINI had no upper limit. 30 Previous participation in the following studies was allowed: STAR (including control participants), investigator-sponsored trials (NCT02077361; NCT02671539; NCT02553135; NCT01461213), REGENERATE (NCT02407678), NIGHT (NCT03359551), or SOLSTICE (NCT03584165). 30,33 –39
Participants with a history of amblyopia or inflammatory disorder in either eye, or any other significant ocular or nonocular condition that could put the participant at risk in the study, were ineligible. Intraocular surgery within 3 months of screening, participation in another research study involving an investigational product in the past 12 weeks, or previous receipt of another gene- or cell-based therapy was not permitted.
Each site’s respective research ethics committees (independent ethics committee or institutional review board) approved the study, and all participants gave written informed consent. The study complied with all appropriate laws and regulations, including the International Council for Harmonization Guidelines for Good Clinical Practice and, where permissible, the Declaration of Helsinki. 40,41
Interventions
Timrepigene emparvovec comprises the wild-type CHM cDNA sequence encoding REP1, with the cytomegalovirus enhanced chicken β-actin hybrid promoter and a modified woodchuck hepatitis virus post-transcriptional regulatory element, packaged into the AAV2 vector. 24 In a two-step process, vitrectomy and retinal detachment with a balanced salt solution were performed first. 25 Secondly, timrepigene emparvovec was administered by subretinal injection of ≤0.1 mL of the study drug containing 1 × 1011 vector genomes at day 0 of period 1 (visit 1) for study eye 1 and day 0 of period 2 (visit 1) for study eye 2.
All participants received oral prednisone or prednisolone to minimize postsurgical inflammation (Supplementary Data S1); most also received prophylactic ocular steroid drops.
Primary and secondary end points
The primary end point was the safety of bilateral administration of timrepigene emparvovec, evaluated (through month 12, unless otherwise stated) by the following safety measures: BCVA; spectral domain optical coherence tomography (SD-OCT); autofluorescence (AF); microperimetry (MP); adverse event (AE) reporting; ophthalmic examination assessments (including intraocular pressure, slit lamp examination, lens opacity grading, and dilated ophthalmoscopy); fundus photography (screening and month 12); vital signs (screening, days 1 and 3, and month 12); post-treatment vector shedding (through month 3); and immunogenicity sampling post-treatment, with assessment of antidrug antibodies (ADAs) against the REP1 transgenic product, neutralizing antibodies (NAbs) against the AAV2 capsid, and enzyme-linked immunospot (ELISpot) assays. Vector shedding samples were considered positive if the measured vector DNA concentration was above the limit of detection; positive samples may have been below the limit of quantification. Supplementary Data S2 describes the immunogenicity assessments.
Treatment-emergent AEs (TEAEs) and serious AEs (SAEs), their relationship to study drug and/or procedures, and participants with SAEs leading to study discontinuation were summarized. Time to TEAE onset was calculated starting from the participant’s first surgery in GEMINI. The relationship between immunogenicity and TEAEs related to ocular inflammation, reduced VA, and hypersensitivity was assessed; the latter were defined by the standardized Medical Dictionary for Regulatory Activities (MedDRA) queries (broad and narrow) of hypersensitivity, v25.0. 42 AEs of interest were chosen using custom MedDRA queries to collate all preferred terms related to ocular inflammation or reduced VA.
The secondary end points were changes from baseline in BCVA, AF, SD-OCT, and MP at month 12.
Statistical methods
The planned enrollment was 60 participants. The all-treated participants population comprised all participants who had surgery in GEMINI. The immunogenicity population comprised participants with evaluable immunogenicity samples at baseline and at least one postsurgery visit.
No formal statistical analyses were planned or performed for the primary and secondary end points. Descriptive statistics summarized continuous variables. Counts and percentages summarized categorical and binary variables. Safety analyses and the main efficacy analysis used the observed case method. Supportive analyses for BCVA-related end points used the last observation carried forward method. Most participants began period 2 before completing period 1 (Fig. 1), so BCVA end points for study eye 1 in period 2 were converted (i.e., remapped) to their equivalent period 1 time points to allow longitudinal analysis across the whole study.
Selected baseline characteristics and retinal inflammation events were assessed post hoc in participants with ≥15-letter BCVA loss at month 12 (continuous variables: logistic regression model; categorical variables: Fisher’s exact test) (Supplementary Table S1). NAb status heatmaps were generated post hoc.
RESULTS
Participant disposition and baseline characteristics
Overall, 66 participants enrolled and received timrepigene emparvovec, and 53 completed the study; 13 participants discontinued, four of these because of SAEs (Supplementary Fig. S1). No participants withdrew because of nonserious TEAEs. All participants were male; baseline ocular characteristics were representative of adults with choroideremia and were well-balanced between study eyes (Table 1). The intrasurgery window ranged from 22 to 483 days.
Demographics and Participant Baseline Characteristics
The first surgery was performed on visit 1 (day 0) of period 1, and the second surgery was performed on visit 1 (day 0) of period 2.
Retinal sensitivity was measured by microperimetry.
AF, autofluorescence; BCVA, best-corrected visual acuity; dB, decibel; IQR, interquartile range; N/n, number of participants; SD, standard deviation.
Functional and anatomical end points
BCVA was generally maintained post-treatment, despite both eyes undergoing retinal detachment and subretinal injection. Small, but not clinically significant, mean decreases were seen at month 12 in both eyes; the largest mean decrease (−2.8 ± 16.0 letters) was for study eye 1, period 1 (Fig. 2). Post hoc analyses did not demonstrate a statistically significant correlation (nominal p > 0.05) between retinal inflammation events and BCVA reduction of ≥15 letters from baseline at month 12 (Supplementary Table S1). In period 1, after treatment of study eye 1, a few participants experienced sporadic ≥10- and ≥15-letter improvements in BCVA from baseline in their untreated study eye 2. The BCVA decrease observed up to 30 days after treatment was consistent with normal postprocedure recovery, when blurred vision may persist for several weeks. 43 –45 BCVA changes from baseline were comparable between study eyes and unaffected by intrasurgery window. Based on post hoc subgroup analyses, older baseline age for study eye 1 and lower baseline BCVA in study eye 2 were the only potential risk factors for a ≥15-letter BCVA reduction at month 12 (n = 7 eyes) (Supplementary Table S1). No adverse changes in SD-OCT, AF, or MP parameters were observed at month 12.
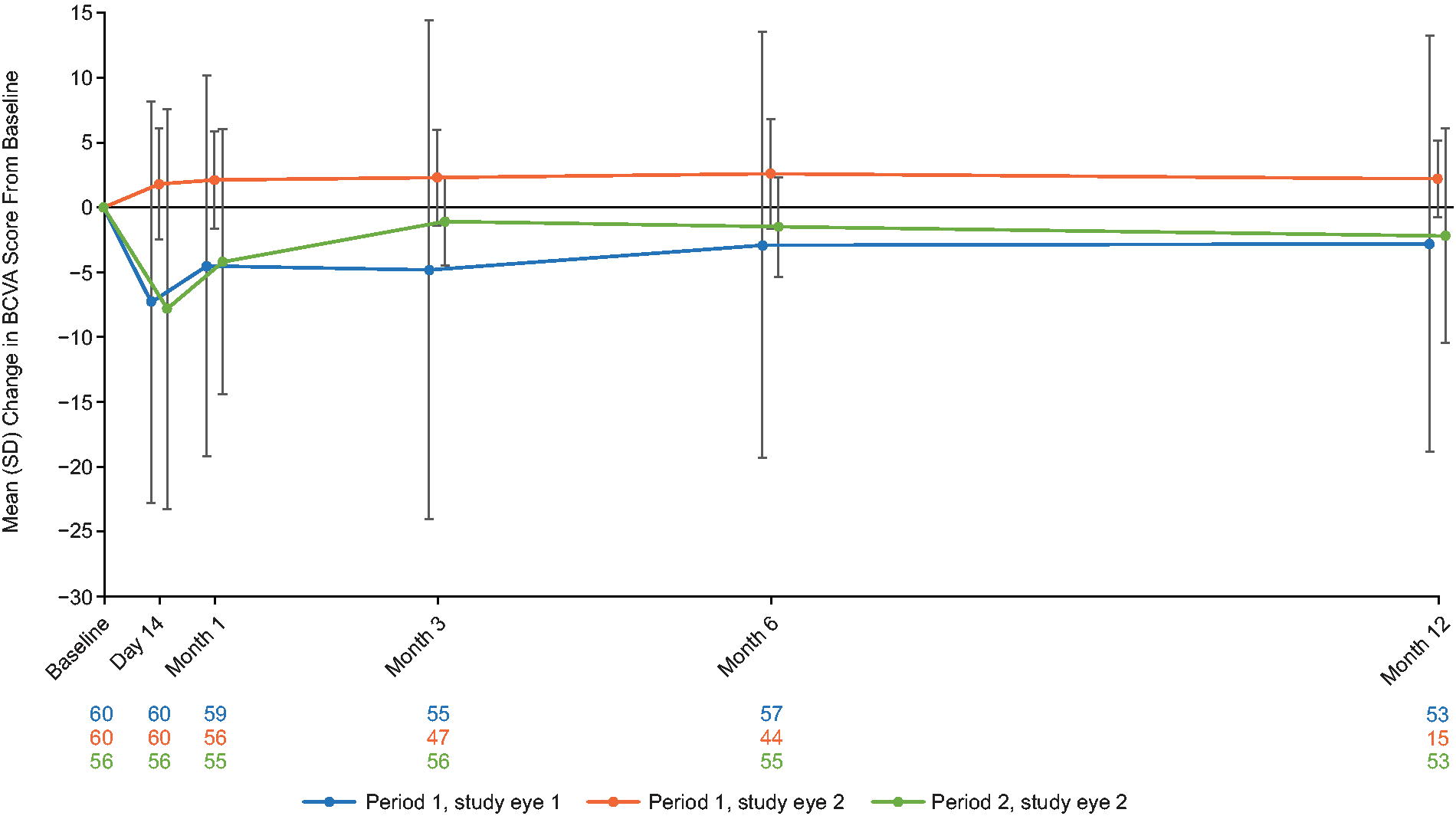
BCVA mean (SD) change from baseline over time (partial output). Data for days 1, 3, and 7 are not shown because these data are highly variable and are not predictive of final visual outcome. Data for period 2, study eye 1 (lower baseline BCVA) are not available for this figure because the data in this figure are the remapped observed case data (see Figure 1 legend for definition of remapped data). The blue, orange, and green numbers represent the n numbers for each time point. BCVA, best-corrected visual acuity; n, number of participants; SD, standard deviation.
Safety end points
In both periods, most participants experienced TEAEs, which were predominantly mild or moderate (Table 2; Supplementary Table S2). The most common ocular TEAEs were conjunctival hemorrhage, anterior chamber cell, VA reduced, eye pain, and foreign body sensation (Supplementary Table S3). Most ocular TEAEs were considered related to study procedure (502 events in 65/66 participants, 98.5%) rather than study drug (46 events in 19/66 participants, 28.8%); some were considered related to both. Five participants (7.6%) had SAEs potentially related to procedural complications with anatomical correlation (vitreous hemorrhage, macular hole, retinal detachment, tractional retinal detachment, and choroidal neovascularization). Supplementary Table S4 lists SAEs leading to study discontinuation, including noninfective retinitis. In period 1, more participants reported TEAEs in study eye 1 soon after surgery (≤30 days post-treatment, 95.0%) compared with later time points (28.3%). There was no meaningful difference across intrasurgery windows in TEAE incidence, onset time, outcome (recovered/resolved), or participants reporting at least one study-drug- or study-procedure-related SAE. One participant died from completed suicide, considered unrelated to study drug or study procedures. Supplementary Table S5 lists SAEs by study period.
Treatment-Emergent Adverse Events Reported by Treatment Period
Events with the following preferred terms were considered to be related to ocular inflammation: anterior chamber cell, anterior chamber fibrin, anterior chamber flare, anterior chamber inflammation, aqueous fibrin, autoimmune eye disorder, birdshot chorioretinopathy, chorioretinitis, choroiditis, cystoid macular edema, endophthalmitis, eye inflammation, hypopyon, immune-mediated uveitis, macular edema, necrotizing retinitis, noninfectious endophthalmitis, noninfective chorioretinitis, noninfective retinitis, ocular vasculitis, optic neuritis, panophthalmitis, retinal edema, retinal vasculitis, retinitis, sympathetic ophthalmia, toxic anterior segment syndrome, uveitis, uveitis-glaucoma-hyphema syndrome, and vitritis.
Events with the following preferred terms were considered to be related to reduction in VA: altered visual depth perception, amaurosis, amaurosis fugax, blindness, blindness day, blindness transient, blindness unilateral, central vision loss, Charles Bonnet syndrome, chloropsia, chromatopsia, color blindness, color blindness acquired, cyanopsia, delayed dark adaptation, delayed light adaptation, diplopia, eccentric fixation, erythropsia, foveal degeneration, glare, halo vision, loss of visual contrast sensitivity, low luminance BCVA decreased, metamorphopsia, night blindness, photopsia, sudden visual loss, tunnel vision, vision blurred, VA reduced, VA reduced transiently, visual brightness, visual field defect, visual impairment, and xanthopsia.
Events with the following preferred terms were considered to be related to retinal inflammation: chorioretinitis, choroiditis, cystoid macular edema, eye inflammation, noninfective chorioretinitis, noninfective retinitis, retinal edema, retinitis, vitreal cells, and vitritis.
BCVA, best-corrected visual acuity; E, number of events; N/n, number of participants; SAE, serious adverse event; TEAE, treatment-emergent adverse event; VA, visual acuity.
Incidences of ocular-inflammation-related (66.7%) and reduced-VA-related TEAEs (57.6%) were similar between study eyes, periods (Supplementary Tables S6 and S7), and intrasurgery windows. Retinal-inflammation-related TEAEs occurred in 45.5% of participants, with similar rates in both eyes; serious noninfective retinitis occurred in two participants (3.0%) (Supplementary Table S8).
No meaningful changes occurred in intraocular pressure, slit lamp examination assessments, lens opacity grades, dilated ophthalmoscopy, fundus photography, or vital signs. Figure 3 shows representative retinal images of participants. Baseline saliva, blood, urine, and bilateral tear samples were negative for vector shedding in both treatment periods. Urine samples remained negative. At day 1 in both periods, low proportions of saliva (≤25%), blood (≤25%), and bilateral tear samples (≤35%) were positive, most of which were below the limit of quantification; these generally reverted to baseline (negative) by either day 14 (tears and saliva) or month 1 (blood).

Representative retinal images from GEMINI participants with
Immunogenicity
Baseline ADA samples were available for all participants, and none was positive at any time point. Approximately one-third of participants with available NAbs data were baseline positive, consistent with the published NAb seroprevalence. 46 The highest percentage of treatment-emergent positive NAb responses was observed at month 1 (period 1: 10.5%, four participants; period 2: 14.3%, five participants) (Fig. 4). Of those with available ELISpot data (36 in period 1, 40 in period 2), most were negative at baseline (Fig. 5). The highest percentage of treatment-emergent positive ELISpot statuses against overall AAV2-REP1 was observed at month 3 in period 1 (5/17 participants, 29.4%) and at month 6 in period 2 (4/28 participants, 14.3%). In post hoc heatmap analyses, baseline NAbs positivity (19 in period 1, 21 in period 2) was not associated with post-treatment NAb response or occurrence of retinal inflammation TEAEs (Supplementary Fig. S2). ELISpot heatmaps are not included owing to the small sample size.
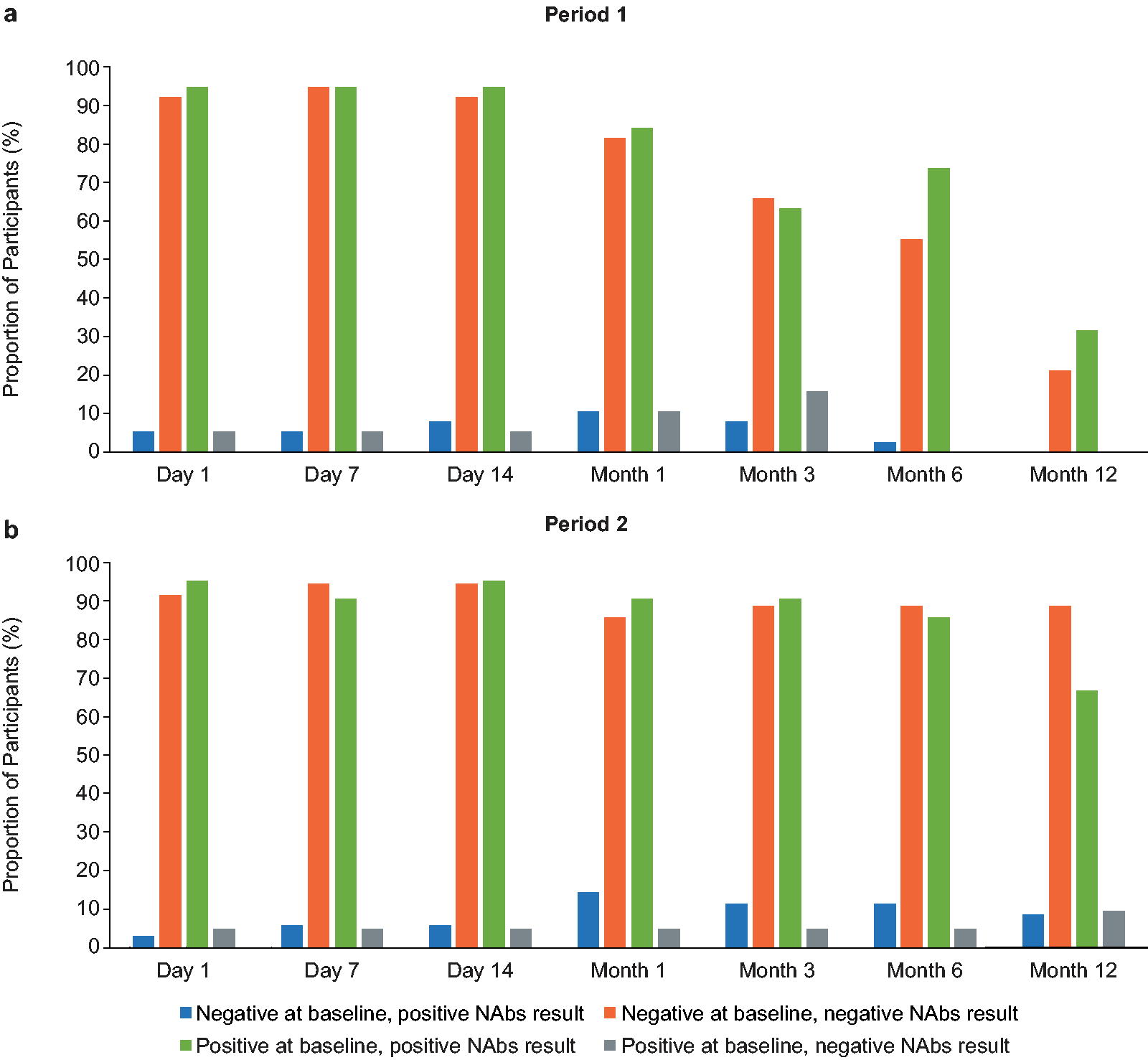
NAbs sampling over time during period 1

ELISpot sampling over time during period 1
In period 2, a ≥15-letter decrease from baseline in month 12 BCVA score was observed in four eyes in three participants (aged 33–57) with preexisting NAbs; no reasons were identified for this. No participants with baseline-positive ELISpot status experienced a ≥15-letter BCVA reduction. More participants with baseline-positive NAbs experienced a month 12 ≥15-letter decrease from baseline in BCVA in period 2 than in period 1. Baseline positivity for NAbs was potentially associated with a higher period 1 incidence of ocular-inflammation- or reduced-VA-related TEAEs.
DISCUSSION
The GEMINI study demonstrated an acceptable safety profile for bilateral sequential subretinal injection of timrepigene emparvovec in male participants with choroideremia, without significant immune response. GEMINI is the largest prospective bilateral ocular gene therapy clinical study conducted to date. 23
Contextualizing the study procedure’s low serious complications rate (7.6%) is challenging because data on subretinal injection complications are sparse, and injection techniques constantly evolve. 47,48 Prior exposure to timrepigene emparvovec did not increase the serious TEAE risk upon second surgery, potentially associated with a lower complication risk given surgeons’ greater procedural familiarity.
The intrasurgery windows did not meaningfully affect the safety profile. Except for the 1.7- to 4.6-year intrasurgery window in a follow-on Phase I safety study of contralateral voretigene neparvovec administration, 49 the GEMINI intrasurgery windows were longer than those for voretigene neparvovec: an approved minimum of 6 days, 43,50 6–18 days in a Phase III study, 23 and 7 days in a small, retrospective Danish study. 51 In the retrospective study, 9/23 eyes (6/12 patients) had vitritis, more frequently in the second eye. 51
Our immunological analyses suggested that bilateral sequential timrepigene emparvovec administration was not associated with a significant immune response: no post-treatment samples were positive for ADAs, and few participants developed treatment-emergent ELISpot positivity. Furthermore, there was no evidence of systemic immune reaction or an inoculation effect, as the reported inflammatory reaction profile was similar for both injections. Similar results were seen following sequential bilateral administration of AAV2 in nonhuman primates with baseline anti-AAV2 antibodies. 52 These findings have important implications for other AAV2-based ocular gene therapies. NAb positivity at baseline was potentially associated with increased rates of ocular-inflammation-related TEAEs and reduced-VA-related TEAEs during period 1. Subretinal inflammation was not specifically assessed in GEMINI, but could be related to NAb status and, for subretinally administered treatments, be more relevant than general ocular inflammation. Subretinal inflammation primarily relates to choroidal thickening and, in some cases, intraretinal fluid. 27
Although many participants experienced ocular inflammation (66.7%) or retinal inflammation (45.5%), these were generally manageable with steroid administration, and very few participants discontinued because of ocular-inflammation-related (1/44 participants, 2.3%) or retinal-inflammation-related (1/30 participants, 3.3%) TEAEs. The vast majority of these ocular/retinal inflammation events were nonserious (95.5%) and generally manageable. Retinal inflammation rates in the GEMINI study (45.5%) and the STAR study treatment groups (47–51%) were similar. 30 The rate was lower in a Phase I/II study of timrepigene emparvovec; 1/14 participants (7.1%) experienced significant retinal inflammation, but the postoperative steroid course duration was subsequently increased. 27 Initiation of steroids could be a useful proxy to monitor subretinal inflammation. Other potential immunosuppressive strategies include rituximab, protease inhibitors, hydroxychloroquine, and rapamycin. 53,54
As expected in a safety study of this duration, BCVA was generally maintained in both eyes over 12 months after a single subretinal treatment in each eye. The small overall decrease in BCVA was not clinically meaningful and some participants experienced sporadic ≥10- or ≥15-letter improvements from baseline. Many participants had high baseline BCVA, limiting their scope for VA improvements. Surprisingly, study eye 2 had a small apparent treatment effect during period 1. The recently published STAR study did not meet its primary end point, but there was a treatment effect for the number of participants with ≥15-letter BCVA gains for high-dose timrepigene emparvovec (1 × 1011 vector genomes) versus untreated control and with ≥10-letter gains for both high and low dose (1 × 1010 vector genomes) versus control. 30 BCVA loss after 12 months was less for both the high and low dose than the untreated control group. 30
GEMINI showed no meaningful changes from baseline in other secondary outcomes, suggesting that they may not be influenced by prior timrepigene emparvovec exposure; together with the post hoc analyses, the previously reported correlation between inflammation and BCVA reduction is not supported. Verifying this would require larger studies, as few participants lost ≥15 letters in GEMINI. Furthermore, baseline characteristics and retinal inflammation events were not assessed post hoc in participants with losses in MP measures, which can sometimes progress while BCVA remains stable. 22 Potential reasons for stable secondary outcomes include age-related effects, ceiling effects for improvement from a relatively high baseline VA, the short follow-up period relative to the time course of disease, and interindividual variation in natural history of disease. The maintenance of BCVA in the 20-month noninterventional NIGHT study suggests that GEMINI may have been too short to detect slowing of disease progression. 22 However, GEMINI achieved its primary goal of assessing inflammatory responses to bilateral retinal gene therapy with an AAV2 vector.
Additional limitations include the unique challenges of performing surgery on eyes with choroideremia, such as retinotomies close to the fovea, exposing it to high injection pressures and variable tolerance to induction of retinal detachment by bleb initiation. 25,55 –57 The lack of ADA-positive participants precluded assessment of the effect of ADAs on study end points. Exclusion of participants with incomplete immunogenicity data reduced the sample size to support immunogenicity conclusions. Participants transferring from earlier studies, involving treatment of only one eye, potentially had unintentionally long intrasurgery windows, up to 483 days. Finally, the definition of AE onset (calculated from the first surgery in GEMINI) potentially limited the ability to draw safety conclusions for study eye 2.
In conclusion, we demonstrated that bilateral sequential administration of timrepigene emparvovec was well tolerated in male participants with choroideremia, without significant immune responses and with BCVA maintained. Our findings may be applicable to bilateral administration of other ocular gene therapies for retinal diseases.
Footnotes
ACKNOWLEDGMENTS
The authors thank the staff, participants, and their families for their work and participation in the GEMINI study. Dr. Aniz Girach and Dr. Tuyen Ong (Nightstar Therapeutics) provided input into the study design. Medical writing support was provided by Jennifer Mitchell, PhD, of Selene Medical Communications, Cheshire, UK, which was funded by Biogen.
DATA SHARING STATEMENT
Individual participant data collected during the trial may be shared after anonymization and on approval of the research proposal. ![]() .
.
AUTHORS’ CONTRIBUTIONS
R.E.M.: conceptualization; data curation; funding acquisition; investigation; methodology; supervision; validation; writing—review and editing; visualization; and resources; I.A.: investigation; resources; project administration; supervision; validation; and writing—review and editing; M.D.F.: investigation; supervision; validation; and writing—review and editing; R.M.H.: investigation and writing—review and editing; B.L.L.: investigation and writing—review and editing; M.E.P.: investigation and writing—review and editing; R.S.: writing—review and editing; J.A.G.: data curation; formal analysis; supervision; visualization; and writing—review and editing; J.L.: formal analysis; methodology; and writing—review and editing; K.Z.: conceptualization; data curation; formal analysis; investigation; methodology; resources; validation; visualization; writing—original draft; and writing—review and editing; S.-F.T.: writing—original draft; writing—review and editing; conceptualization; and formal analysis.
GEMINI STUDY GROUP
Oxford Eye Hospital, Oxford University Hospitals NHS Foundation Trust, Oxford, UK: Robert MacLaren, Jasleen Kaur Jolly, Imran H Yusuf; Bascom Palmer Eye Institute, University of Miami Health System, Miami, Florida, USA: Byron Lam, Janet Davis, Ninel Gregori, Carlos Mendoza; Center Hospitalier National d’Ophtalmologie (CHNO) des Quinze-Vingts, Paris, France; Isabelle Audo, Raphael Atia, Stéphane Bertin, Saddek Mohand-Said, Jose-Alain Sahel; OHSU, Casey Eye Institute, Portland, Oregon, USA: Mark Pennesi, Cristy Ku, Paul Yang, Steven Bailey, Andreas Lauer; Universitätsklinikum Tübingen, Institute for Ophthalmic Research, Tübingen, Germany: M. Dominik Fischer, Felix Reichel, Caroline Gassel, Lasse Wolfram, Nora Fischer, Tobias Peters, Barbara Wilhelm, Immanuel Seitz, Fabian Wozar, Yousof Vaheb, Guy Ochakovski; Massachusetts Eye and Ear, Harvard Medical School, Boston, Massachusetts, USA: Rachel Huckfeldt, Brian Ballios, Sarah Chorfi, Jason Comander, Eric Pierce, Kevin T. Ferenchak; Cincinnati Eye Institute, Blue Ash, Ohio, USA: Robert Sisk, Robert Foster, Daniel Miller, James Osher, Lucas Lindsell.
AUTHOR DISCLOSURE
R.E.M. reports consulting fees (AGTC, Beacon Therapeutics, and
FUNDING INFORMATION
The study was funded by
SUPPLEMENTARY MATERIAL
Supplementary Data S1
Supplementary Data S2
Supplementary Figure S1
Supplementary Figure S2
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4
Supplementary Table S5
Supplementary Table S6
Supplementary Table S7
Supplementary Table S8
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.